Beyond codeine – the evidence landscape of conventional, natural, and emerging antitussive therapies: a systematic review and meta-analysis
Monika Marko, Rafał Pawliczak

TL;DR
This study compares the effectiveness and safety of traditional, natural, and new cough treatments, finding that new P2X3 receptor antagonists show the most promise.
Contribution
The study provides a systematic comparison of emerging antitussive therapies, highlighting P2X3 antagonists as a promising alternative to codeine.
Findings
P2X3 antagonists consistently reduced chronic cough frequency compared to placebo.
Conventional and natural antitussives showed inconsistent efficacy.
The observed effect of P2X3 antagonists appears to be a class-related response.
Abstract
For decades, cough treatment has relied on centrally acting agents like codeine despite inconsistent efficacy. Advances in cough neurobiology enabled targeted therapies. Natural remedies remain widely used, though evidence for their effectiveness and safety is limited. This study aimed to compare evidence on the efficacy and safety of conventional, natural, and novel antitussives. A systematic review and meta-analysis of randomized clinical trials assessed cough frequency, Visual Analogue Scale (VAS), Leicester Cough Questionnaire (LCQ) and adverse events versus placebo. Subgroup meta-analysis showed no significant differences between P2X3 antagonists, indicating a consistent class effect. All subgroups reduced chronic cough frequency [standardized mean difference (SMD) = −0.50, 95% confidence interval (CI) (−0.67–0.34), P = 0.0001], suggesting that the observed effect is a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
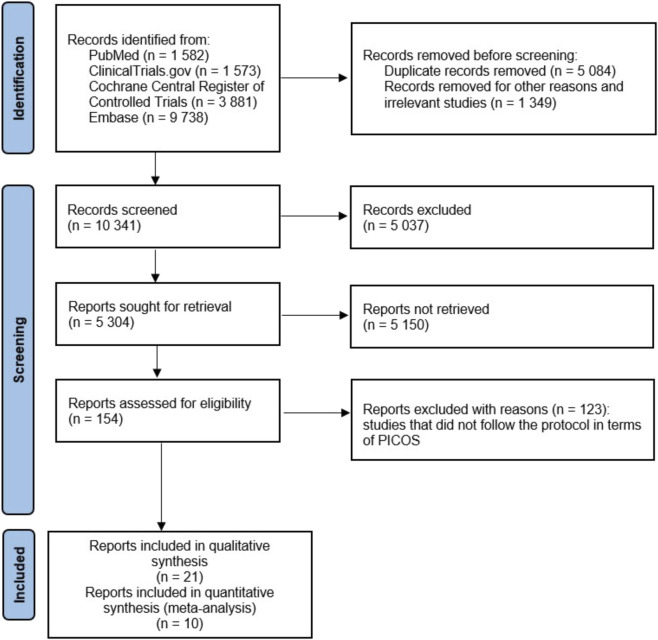 FIGURE 1
FIGURE 1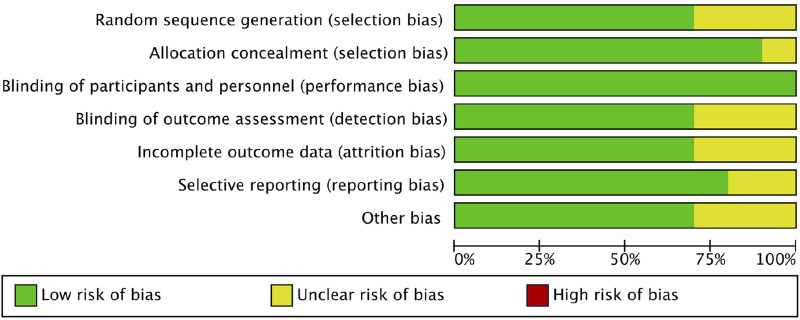 FIGURE 2
FIGURE 2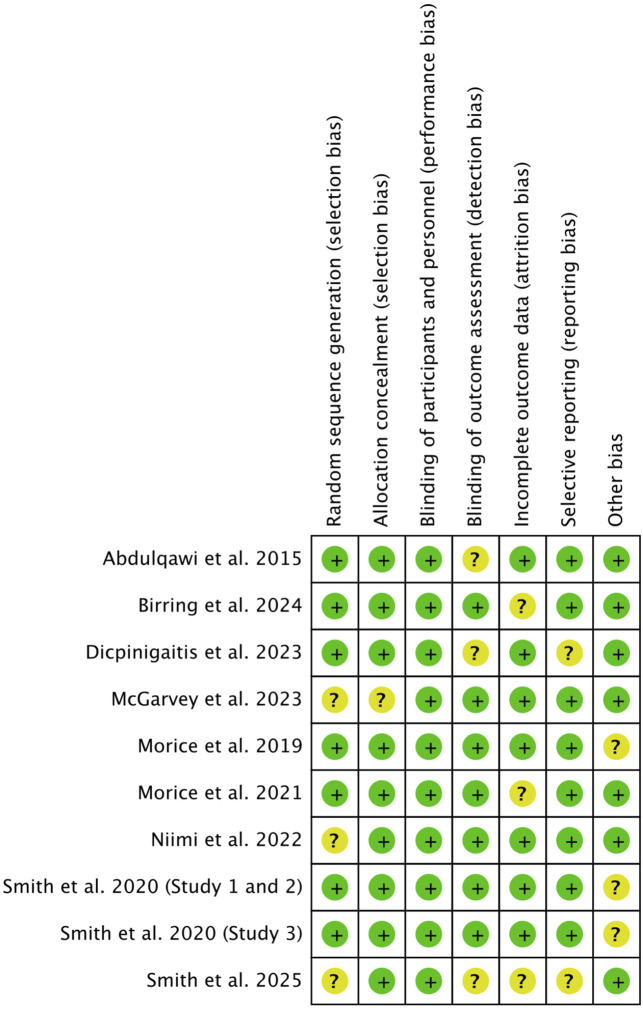 FIGURE 3
FIGURE 3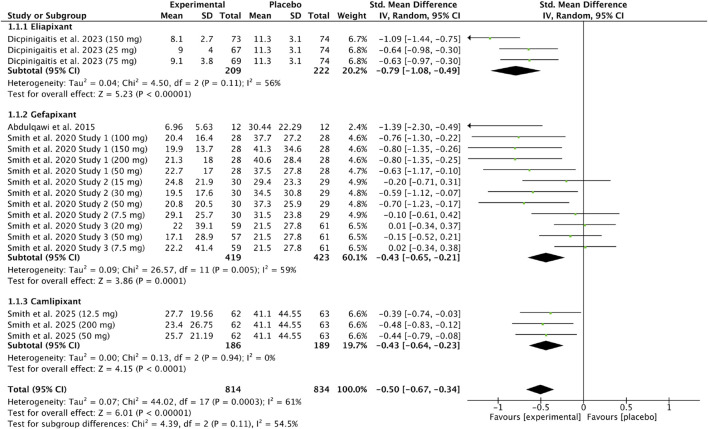 FIGURE 4
FIGURE 4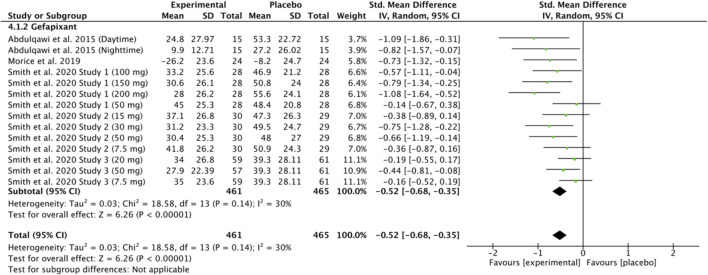 FIGURE 5
FIGURE 5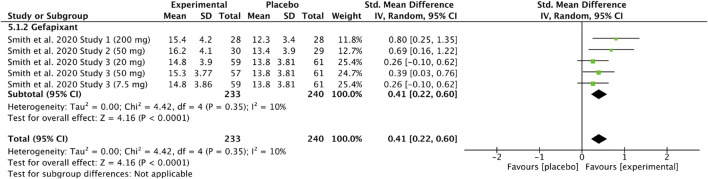 FIGURE 6
FIGURE 6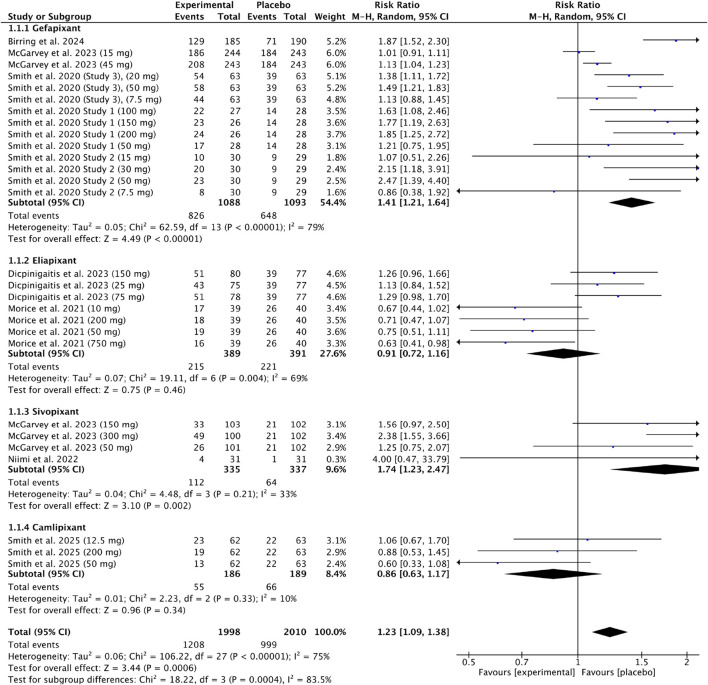 FIGURE 7
FIGURE 7| Database | Search strategy |
|---|---|
| PubMed | ((antitussive agents) OR (antitussive drugs) OR (cough treatment) AND ((efficacy)) AND ((safety) OR (adverse events) OR (side effects)) |
| Cochrane Central Register of Controlled Trials (CENTER) | Antitussive agents OR antitussive drugs OR cough treatment AND efficacy AND safety |
| ClinicalTrials.gov | (antitussive agents OR antitussive drugs OR cough treatment) AND (efficacy) AND (safety OR adverse events OR side effects) |
| Embase | (“antitussive agents”/exp OR “antitussive agents” OR “antitussive drugs” OR “cough treatment” OR “efficacy”/exp OR “efficacy” OR “safety”/exp OR “safety” OR “adverse events”/exp OR “adverse events” OR “side effects”) AND ([controlled clinical trial]/lim OR [randomized controlled trial]/lim) AND “coughing”/dm AND (“clinical trial”/de OR “controlled clinical trial”/de OR “controlled study”/de OR “double blind procedure”/de OR “human”/de OR “intervention study”/de OR “open study”/de OR “randomized controlled trial”/de OR “retrospective study”/de) AND (“article”/it OR “clinical trial”/it) |
| Google Scholar | ((antitussive agents) OR (antitussive drugs) OR (cough treatment) AND ((efficacy)) AND ((safety) OR (adverse events) OR (side effects)) |
| Studies included in a meta-analysis | ||||
|---|---|---|---|---|
| Study (author, year)/Design | Duration | Intervention | Participants N, age, condition | Main outcomes and measures |
| ( | 12 weeks | Twice daily: | N = 310, ≥18 refractory chronic cough (RCC) | PO: Change from baseline in 24-h cough count after 12 weeks of intervention |
| ( | 8 weeks (two 2-week treatment periods + 2-week washout + 2-week follow-up) | Twice daily: | N = 24 | PO: Daytime cough frequency, night-time and 24-h cough frequency assessed |
| ( | ∼5–8 weeks (two 16-day treatment periods + washout) | Gefapixant BID 7.5–200 mg; 4-day escalation placebo | N = 59 mean age 63 years (47–76) | PO: Awake cough freq. (VitaloJAK) |
| ( | 12-week | Gefapixant BID 7.5–50 mg placebo | N = 253 | PO: Change from baseline in awake objective cough frequency after 12 weeks (day 84) |
| ( | 4 weeks | camlipixant | N = 310 | PO: Change in 24-h cough frequency (Day 28, VitaloJAK) |
| ( | ∼3 weeks total (two 1-day periods, 48-h washout, 2-weeks follow-up) | single dose gefapixant | N = 24 | PO: Cough challenge thresholds C2 (≥2 coughs) and C5 (≥5 coughs) for each challenge agent, averaged across 1-, 3-, and 5-h post-exposure |
| ( | ≈16 weeks total (2-week run-in +12-week treatment + 2-week follow-up) | Gefapixant | N = 375 | PO: Percentage change from baseline in 7-day average of daily CSUI episodes at week 12 (recorded in incontinence diary) |
| ( | ≈16 weeks total (2-week screening +12-week treatment + 2-week follow-up) | gefapixant | N = 415 | PO: change from baseline at week 12 in LCQ total score |
| ( | Approximately 6–7 weeks (2 weeks of treatment, 2–3-week washout period, followed by another 2 weeks of treatment in the crossover phase) | oral sivopixant | N = 31 | PO: Ratio of daytime coughs per hour after 2 weeks vs. baseline |
| ( | ∼9–10 weeks (two 3-week periods + 3–4 weeks washout) | Period A: placebo 2 weeks: eliapixant 10 mg BID 1 week; Period B: eliapixant 50/200/750 mg BID (1 week each) | N = 40 | PO: Change in cough frequency per hour (24-h objective monitoring, VitaloJAK) at baseline (day 1) and end of each treatment week (days 7, 14, 21); awake and asleep cough frequencies also assessed |
| Studies included in a systematic review | ||||
| Study ID | Duration | Intervention | Participants | Main outcomes and measures |
| ( | Single-day sessions (3 h follow-up) | Dextromethorphan 30 mg | N = 44 | Not specifically reported |
| ( | 3-h laboratory assessment + 4-day home phase | Codeine 30 mg/10 mL q.d.s. (total 120 mg/day) placebo syrup | N = 91 | Not specifically reported |
| ( | 2 single-day periods, 1 week apart | Codeine phosphate 60 mg or matched placebo | N = 21 | PO: Time spent coughing (cough seconds, cs) during 10-h daytime and overnight recordings (objective cough frequency) |
| ( | 2 days | 50 mg codeine or matched placebo in capsule form | N = 83 | cough sound-pressure levels (CSPLs) measured on a sound meter; subjective scores of coughs seventy; and cough frequency recorded by means of a microphone connected to an ink-pen recorder |
| ( | dextromethorphan | 3 days | N = 120 median age: | Symptom scores |
| ( | 4 days | Dextromethorphan | N = 131 | PO: Total cough count during the first 24 h of treatment |
| ( | Approximately 7–13 days (two treatment sessions of 10 consecutive doses each, separated by a 3–7-day washout period) | Levodropropizine 60 mg (20 drops) or matching placebo, administered orally three times daily (t.i.d.) for 10 consecutive doses | N = 26 | Bronchodilator reversibility by FEV1 change after salbutamol 200 μg |
| ( | Approximately 6–9 days (three treatment sessions separated by 48–72-h washout periods) | 60 mg Levodropropizine, or 15 mg Dihydrocodeine or matching placebo | N = 24 | Ventilatory response to CO2 rebreathing |
| ( | 12 weeks (COUGH-1) and 24 weeks (COUGH-2) | gefapixant 15 mg twice per day, or gefapixant 45 mg twice per day or placebo | COUGH-1 | PO: Change from baseline in 24-h cough frequency (weeks 12/24) |
| ( | 5 days |
| N = 177 | PO: efficacy of treatment (Cough Relief Index), cough frequency |
| ( | 8 days | Grintuss | N = 102 | PO: The changes in the day- and night-time cough score |
| ( | 8 days | KalobaTUSS | N = 106 | PO: The change in the night-time cough score before treatment and nocturnal scores obtained after the first, fourth and eighth nights of treatment, and the change in the diurnal time cough score before treatment and scores obtained after the first, fourth and eighth days of treatment |
| ( | 15 months | Licorice pastilles | N = 70 | PO: a decrease in the daily cough scores during the 2-week treatment period |
| ( | 28-day follow-up | Suhuang Zhike capsules | N = 132 | PO: Change in ACT scores on day 42 relative to baseline, reflecting asthma control status |
| ( | 13 months | Agave nectar | N = 120 | The outcome of between-night change |
| ( | 7 months |
| N = 182 | Evaluation in terms of the duration until cough suppression was achieved |
| ( | 5 months | Thyme-ivy syrup 5.4 mL three times daily for 11 days (15 g thyme +1.5 g ivy extract/100 g); placebo identical in appearance and flavour | N = 363 | PO: Change in mean frequency of daytime coughing fits (Days 7–9 vs. Day 1) |
| ( | 5 months | Thyme–primrose tablets | N = 362 | PO: Change in mean frequency of daytime coughing fits (Days 7–9 vs. Day 1) |
| ( | 14-day study: 7-day treatment, and 7-day safety follow-up | Sediflu syrup 10 mL BID for 7 days | N = 56 | PO: Change in day- and night-time CCS. |
| ( | 4 weeks | purple passion fruit (PFP) peel extract | N = 43 | Asthma symptoms and spirometry (FVC, FEV1) at baseline and weekly |
| ( | 9 months | Pelargonium sidoides extract (EPs®7630, Kaloba®) | N = 132 average age: 56–59 years | Feasibility (recruitment, diary return/completion, antibiotic use, symptom duration/resolution, medication compliance), clinical (symptom duration, resolution at Day 7), and health-economic (EQ-5D-5L, NHS resource use, costs) |
| Continuous data | |||||
|---|---|---|---|---|---|
| Patients, interventions, comparators | Number of participants/studies | Intervention vs. comparator standardized mean difference (95% CI) | Comparator | Certainty of the evidence (GRADE) | |
| Eliapixant vs. placebo | 209 vs. 222/1 study (divided into three) | −0.79 [−1.08, −0.49] | The mean cough count (24 h frequency) | High | |
| Gefapixant vs. placebo | 419 vs. 423/4 studies (3 studies divided into several parts) | −0.43 [−0.65, −0.21] | The mean cough count (24 h frequency) | Moderate | |
| Camlipixant vs. placebo | 186 vs. 189/1 study (divided into three) | −0.43 [−0.64, −0.23] | The mean cough count (24 h frequency) | Moderate | |
| Gefapixant vs. placebo | 461 vs. 465/4 studies (3 of them divided into several parts) | −0.52 [−0.68, −0.35] | The mean VAS | High | |
| Gefapixant vs. placebo | 233 vs. 240/3 studies (1 of them divided into several parts) | 0.41 [0.22, 0.60] | The mean LCQ | High | |
| Dichotomous data | |||||
| Outcomes | Absolute Effect (95% CI) | Relative effect (95% CI) | Number of studies | Certainty of the evidence (GRADE) | |
| Risk with placebo | Risk with experimental | ||||
| Occurrence of adverts events | 648 per 1,000 | 914 (785-1,000) per 1,000 | RR 1.41 [1.21, 1.64] | 4 studies (3 of them divided into several parts) | Low |
| Absolute difference per 1,000: | |||||
| Occurrence of adverts events | 221 per 1,000 | 217 (190–245) per 1,000 | RR 0.98 [0.86, 1.11] | 3 studies divided into several parts | Low |
| Absolute difference per 1,000: | |||||
| Occurrence of adverts events | 64 per 1,000 | 113 (86–147) per 1,000 | RR 1.76 [1.35, 2.30] | 2 studies (1 of them divided into several parts) | Moderate |
| Absolute difference per 1,000: | |||||
| Occurrence of adverts events | 66 per 1,000 | 56 (42–75) per 1,000 | RR 0.85 [0.63, 1.14] | 1 study divided into several parts | Low |
| Absolute difference per 1,000: | |||||
- —Uniwersytet Medyczny w Lodzi10.13039/501100005888
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory and Cough-Related Research · Chronic Obstructive Pulmonary Disease (COPD) Research · Pediatric health and respiratory diseases
Introduction
1
Cough is a vital protective reflex whose primary function is to generate high-velocity airflow, thereby clearing the airways and maintaining respiratory function (Morice et al., 2020; Lee et al., 2021). When this response becomes excessive or uncontrolled, however, it may evolve into a chronic condition that markedly affects quality of life and increases the healthcare burden (Jakusova and Brozmanova, 2023; Weinberger and Hurvitz, 2020). Children are considered to have a chronic cough when symptoms persist for more than 4 weeks, whereas in adults the threshold is 8 weeks (Weinberger and Hurvitz, 2020). The leading causes of chronic cough include asthma, chronic obstructive pulmonary disease (COPD), pulmonary fibrosis, eosinophilic bronchitis, chronic bacterial bronchitis (Weinberger et al., 2025), as well as upper airway cough syndrome and gastroesophageal reflux disease (GERD).
Increasing attention has been given to cough hypersensitivity syndrome (CHS), which is now recognized as a significant clinical entity accounting for a substantial proportion of patients with chronic cough in whom no clear underlying cause can be identified (Khan et al., 2024; Chung et al., 2016). This condition is characterized by an exaggerated cough response to otherwise innocuous stimuli (thermal, mechanical, or chemical), resulting from enhanced excitability and plasticity of airway sensory nerves, particularly involving vagal afferent pathways (Khan et al., 2024). Importantly, evidence suggests that, in addition to maladaptive neural plasticity, other pathophysiological mechanisms underlying cough hypersensitivity have not been sufficiently characterized (Song and Morice, 2017).
Other contributing factors comprise the use of antihypertensive agents such as angiotensin-converting enzyme (ACE) inhibitors, smoking, habit cough, and systemic disorders (Morice et al., 2020; Jakusova and Brozmanova, 2023). A so-called habit cough, more frequently observed in children and adolescents, is considered a functional disorder characterized by repetitive coughing without an identifiable organic cause, often influenced by behavioral or psychogenic factors (Weinberger et al., 2023). Identification of the etiologies of chronic cough is essential for effective management. In adults, the most common etiologies include cough-variant asthma (CVA), upper airway cough syndrome (UACS), and eosinophilic bronchitis (EB). In contrast, the etiologies of chronic cough in children differ, with protracted bronchitis (PB) predominating and asthma or CVA representing frequent etiologies in school-aged children. However, data on pediatric etiologies remain limited due to the restricted feasibility of diagnostic investigations (Yu et al., 2019).
Cough is one of the most common symptoms encountered in clinical practice, and despite significant progress in understanding its mechanisms, treating it remains a challenge for clinicians (Jakusova and Brozmanova, 2023; Rouadi et al., 2025).
For decades, the management of cough has relied on centrally acting agents, including codeine (Smith et al., 2006), dextromethorphan (Meeves et al., 2023), butamirate (Faruqi et al., 2014; Charpin and Weibel, 1990), and levodropropizine (Lee et al., 2022; Mannini et al., 2017), despite their limited and inconsistent clinical efficacy. Recent advances in the neurobiology of cough have led to the development of mechanism-based therapies, such as P2X3 receptor antagonists, that directly target peripheral cough pathways (Rouadi et al., 2025). This paradigm shift from symptom suppression to pathway-specific modulation marks a pivotal moment in antitussive research.
Alongside these agents, a wide range of natural or herbal remedies continues to be promoted for cough relief, reflecting patient preference for “natural” options (Murgia et al., 2021). It is estimated that nearly four billion people worldwide still rely primarily on herbal medicines for their healthcare needs (Wardani et al., 2023).
Natural cough medicines, often perceived as safer, offer an alternative to conventional over the counter (OTC) cough medications. It should also be emphasized that the market for so-called “natural” cough medicines is rapidly expanding, offering a wide range of preparations with diverse compositions and claimed mechanisms of action (Murgia et al., 2021). Moreover, because medicinal plants contain a variety of bioactive molecules that can simultaneously exert expectorant and antitussive effects, the classification of herbal cough remedies is difficult (Pourova et al., 2023).
An important aspect is the difficult-to-assess chemical composition of plant extracts, which can vary significantly depending on cultivation, harvesting, storage, and processing conditions. As a result, products sold under the same name may differ in composition and pharmacological activity (Murgia et al., 2021). Due to growing interest in natural cough remedies and the lack of consistent, high-quality scientific evidence, a critical assessment of the current state of knowledge is necessary.
Our study aimed to go beyond codeine and examine the current scientific evidence on the effectiveness and safety of conventional, natural, and novel antitussive therapies for the treatment of chronic cough. Therefore, we conducted a systematic review and meta-analysis to assess and compare the effectiveness and safety of antitussives. By integrating data from randomized clinical trials (RCTs), we aimed to provide an updated and comprehensive evidence synthesis to aid clinical decision-making in cough management.
Methods
2
Search strategy
2.1
This systematic review and meta-analysis was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). The study protocol was described in PROSPERO (CRD420251172660).
A comprehensive search was carried out across PubMed, the Cochrane Central Register of Controlled Trials (CENTRAL), Embase, and ClinicalTrials.gov up to October 2025. In addition, gray literature sources–such as conference abstracts, official reports, preprints, datasets, white papers, and patents were explored via Google Scholar. The complete search strategy is provided in Table 1. To ensure completeness, updated searches were performed prior to the final synthesis.
The research question and selection criteria were formulated using the Population, Intervention, Comparison, Outcome, and Study design (PICOS) structure. The inclusion criteria were population: patients with cough, intervention: antitussive drugs, comparison: placebo, outcomes: cough count, change in cough frequency, Visual Analogue Scale (VAS), Leicester Cough Questionnaire (LCQ) and adverse events (AEs), and study design: randomized clinical trials (RCTs), non-randomized clinical trials, real-life trials, observational trials, open-label trials, and prospective trials.
The following exclusion criteria were formulated: review article, systematic reviews, meta-analysis, case series, case report, articles with insufficient information and data, articles published in languages other than English, original articles where specific data and outcomes could not be extracted, original articles that do not include outcomes of interest and retracted articles.
Study selection and data extraction
2.2
The study selection process was conducted independently by two reviewers in parallel. Titles and abstracts identified through database searches were first screened for relevance, and duplicate records were excluded. Full texts of potentially eligible studies were then assessed in detail to determine whether they met the predefined inclusion criteria. To minimize selection bias, eligibility was judged independently by both reviewers, and any discrepancies were resolved through discussion until consensus was achieved.
Data extraction was performed independently using standardized forms. Extracted information included study identifiers (title, authors, institutional affiliation, and registration number), study design, duration, year of publication, intervention details, sample size, participant age, underlying condition, and reported outcomes. The two sets of extracted data were subsequently compared for accuracy and consistency.
All included studies were further assessed for missing or unclear data. Where required, efforts were made to clarify information or standardize reporting. In accordance with Cochrane guidelines (Higgins et al., 2024), results expressed as confidence intervals (CIs) or standard errors of the mean (SEM) were converted to means and standard deviation (SD) to ensure comparability across studies.
Assessment of the risk of bias and methodological quality
2.3
Risk of bias was assessed independently by two reviewers using the Cochrane Risk of Bias tool in Review Manager 5.4. Seven domains were evaluated (sequence generation, allocation concealment, blinding, incomplete data, selective reporting, and other bias), with studies rated as low, unclear, or high risk. Potential conflicts of interest were also considered in relation to funding sources. Disagreements were resolved by consensus, and an attrition rate above 10% was regarded as potentially influencing study validity.
Statistical methods
2.4
All extracted data were analyzed using Review Manager (RevMan) version 5.4. Continuous outcomes were expressed as standardized mean difference (SMD) with 95% confidence intervals (CI), and dichotomous outcomes as risk ratios (RR) with CI. Given the expected heterogeneity, pooled analyses were performed using the Mantel–Haenszel random-effects model. Heterogeneity was assessed with Cochran’s Q test and the I^2^ statistic, with P < 0.05 considered significant. Results were presented as forest plots, and SMDs were interpreted according to Cohen’s thresholds (0.2 small, 0.5 moderate, ≥0.8 large).
Additional analyses
2.5
The certainty of evidence for the outcomes included in the quantitative synthesis was appraised using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach (Schünemann et al., 2023; Guyatt et al., 2013). This assessment considered potential limitations related to risk of bias, inconsistency, indirectness, imprecision, and publication bias. Evidence quality was classified as high, moderate, low, or very low, following the standard GRADE framework, and findings were summarized in a Summary of Findings (SoF) table (Guyatt et al., 2013). The potential for publication bias was further examined through visual inspection of funnel plots.
Results
3
Included studies
3.1
Figure 1 (Page et al., 2021) illustrates the study selection process. Table 2 summarizes the characteristics of the studies included in the meta-analysis (Dicpinigaitis et al., 2023; Abdulqawi et al., 2015; Smith et al., 2020a; Smith et al., 2020b; Smith et al., 2025; Birring et al., 2024; McGarvey et al., 2023; Niimi et al., 2022; Morice et al., 2021) and a systematic review (Smith et al., 2006; Meeves et al., 2023; Mannini et al., 2017; Canciani et al., 2014; Carnevali et al., 2021; Ghaemi et al., 2020; Pan et al., 2025; Paul et al., 2014; Qasemzadeh et al., 2015; Kemmerich et al., 2006; Kemmerich, 2007; Núñez et al., 2024; Watson et al., 2008; Willcox et al., 2021; Lee et al., 2000; Eccles et al., 1992; Freestone et al., 1996; Bhattacharya et al., 2013; Bruschi et al., 2003; McGarvey et al., 2022; Barth et al., 2015). Following study selection, quantitative synthesis was feasible exclusively for chronic cough, as no eligible studies investigating acute cough met the predefined inclusion criteria.
Flowchart of the screening procedure. PICOS: Population, Intervention, Comparison, Outcome and Study design.
No additional records were identified through the gray literature search (Google Scholar), and no duplicates were detected. The updated search yielded no further eligible studies for inclusion in the systematic review or meta-analysis.
The pooled risk of bias assessment (Figures 2, 3) confirmed that most studies were of low risk. Qualitative evaluation did not suggest substantial publication bias. Given the limited number of studies (n < 10), funnel plots were used for illustrative purposes only, as recommended by Cochrane guidelines (Higgins et al., 2024). Visual inspection of the plots (Supplementary Figures S1–S4) showed no marked asymmetry, though the small sample precludes definitive conclusions.
Risk of bias summary. Review authors’ judgements about each risk of bias item for each included study.
Risk of bias graph. Review authors’ judgements about each risk of bias item presented as percentages across studies.
P2X3: cough count (24 h frequency, chronic cough)
3.2
Five studies (Dicpinigaitis et al., 2023; Abdulqawi et al., 2015; Smith et al., 2020a; Smith et al., 2020b; Smith et al., 2025) were included in the subgroup meta-analysis of 24-h cough frequency after P2X3 antagonist administration versus placebo. Due to varying dosages and study stages, data were analyzed in three subgroups: eliapixant, gefapixant, and camlipixant. The pooled analysis (814 experimental vs. 834 placebo participants) showed a significant reduction in cough frequency [SMD = −0.50, 95% CI (–0.67, −0.34), P < 0.00001; I^2^ = 61%]. No significant subgroup differences were observed (P = 0.11; I^2^ = 54.5%), with eliapixant demonstrating the greatest effect [SMD = −0.79, 95% CI (–1.08, −0.49), P < 0.00001; I^2^ = 56%]. Results are presented in Figure 4.
Standardized mean difference in 24-h cough frequency following P2X3 antagonist treatment in patients with chronic cough compared with placebo.
Gefapixant: visual analogue scale (chronic cough)
3.3
Four studies (Dicpinigaitis et al., 2023; Abdulqawi et al., 2015; Smith et al., 2020a; Smith et al., 2020b) were included in the meta-analysis of Visual Analogue Scale (VAS) scores after gefapixant versus placebo. Data from 461 experimental and 465 placebo participants were analyzed, with some studies divided by dosage or observation period. The pooled analysis showed a significantly lower VAS score in the gefapixant group [SMD = −0.52, 95% CI (–0.68, −0.35), P < 0.00001; I^2^ = 30%]. Results are presented in Figure 5.
Standardized mean difference in Visual Analogue Scale (VAS) scores following gefapixant treatment in patients with chronic cough compared with placebo.
Gefapixant: leicester cough questionnaire (chronic cough)
3.4
Two studies (Smith et al., 2020a; Smith et al., 2020b) were included in the meta-analysis of Leicester Cough Questionnaire (LCQ) scores after gefapixant versus placebo. Data from 233 experimental and 240 placebo participants were analyzed, with study parts divided by dosage or design. The pooled analysis showed a significantly higher LCQ score in the gefapixant group [SMD = 0.41, 95% CI (0.22, 0.60), P < 0.0001; I^2^ = 10%]. Results are shown in Figure 6.
Standardized mean difference in Leicester Cough Questionnaire (LCQ) scores following gefapixant treatment in patients with chronic cough compared with placebo.
P2X3: adverse events (chronic cough)
3.5
Eight studies (Dicpinigaitis et al., 2023; Smith et al., 2020a; Smith et al., 2020b; Smith et al., 2025; Birring et al., 2024; McGarvey et al., 2023; Niimi et al., 2022; Morice et al., 2021) were included in the meta-analysis of adverse events (AEs) after P2X3 antagonist administration versus placebo. Data from 1998 experimental and 2010 placebo participants were analyzed across four subgroups (gefapixant, eliapixant, sivopixant, camlipixant). The pooled analysis showed a higher incidence of AEs in the experimental group [RR = 1.23, 95% CI (1.09, 1.38), P = 0.0006; I^2^ = 75%], with significant subgroup differences (P = 0.00004; I^2^ = 83.5%), indicating that AEs frequency varied by the type of P2X3. Results are presented in Figure 7.
Risk ratio of adverse events (AEs) following P2X3 antagonist treatment in patients with chronic cough compared with placebo.
Results of additional analyses
3.6
The certainty of evidence for all analyzed outcomes was evaluated according to the GRADE methodology (Guyatt et al., 2013). The summary of findings and corresponding GRADE ratings are presented in Table 3.
Discussion
4
This systematic review and meta-analysis included centrally, and peripherally acting medications commonly used to treat cough. The analysis aimed to assess their efficacy and safety based on the results of available RCTs. It should be emphasized that this study did not present quantitative data for codeine, butamirate, dextromethorphan, and levodropropizine. Only qualitative analysis was possible for these antitussives (Table 2). The inability to conduct a meta-analysis of the data from the included studies confirms previous observations that the available studies are characterized by significant heterogeneity. Furthermore, their conclusions are inconsistent. Consequently, it is impossible to draw clear conclusions about the efficacy of these medications in treating cough.
As shown in Table 2, the observed heterogeneity results from significant differences across studies, including drug doses used, therapy duration, methods of efficacy assessment, and heterogeneity in the patient population (age, cough etiology, and comorbidities). These factors contributed to the discrepancy in results and limited the comparability of data in this meta-analysis.
Eccles et al. (1992) in a study using a 30 mg codeine syrup, no significant differences in cough frequency or subjective cough severity were observed between the codeine and placebo groups, either in the laboratory or during home monitoring. These results suggest that cough mechanisms during viral infections may be poorly responsive to opioid antitussives, underscoring the need to explore alternative agents with distinct mechanisms of action.
Moreover, a study (Smith et al., 2006) in patients with stable COPD demonstrated that codeine, although considered a standard antitussive, did not significantly affect cough frequency or subjective cough severity compared with placebo. Despite a slight decrease in cough time after codeine administration compared to baseline, this difference was not statistically significant compared to the control group. These results suggest that cough mechanisms in COPD may be resistant to the effects of opioid antitussives, questioning the validity of using codeine as a reference point in studies of new antitussive agents.
Similarly, a clinical trial in children (Bhattacharya et al., 2013) with upper respiratory tract infection (URTI) found that neither dextromethorphan nor promethazine was more effective than placebo at reducing nocturnal cough or improving sleep quality. Analogously, a study of adults with URTI (Lee et al., 2000) showed no significant advantage over placebo in relieving cough.
These results emphasize that the routine use of antitussives in children and adults with acute upper respiratory tract infection is unjustified, and the effectiveness of both opioid and non-opioid antitussives remains limited. The antitussive effect of dextromethorphan in acute URTI is marginal at best, casting doubt on its routine use in treating viral cough.
Contrary results were obtained in a recent clinical trial in children aged 6–11 years with cough associated with colds (Meeves et al., 2023) Multiple doses of dextromethorphan hydrobromide resulted in statistically significant, although modest, reductions in cough frequency and severity compared with placebo. This effect was most pronounced during the day, but there were no differences between groups in nocturnal cough frequency or sleep quality. These results suggest that dextromethorphan may have some antitussive efficacy in children, particularly for daytime cough, although its effect remains limited. Furthermore, the study highlights the importance of using objective, validated cough assessment tools in the pediatric population to increase the sensitivity of analyses of antitussive efficacy.
Other observations were reported in a study evaluating the efficacy of codeine and levodropropizine in patients with chronic cough (Lee et al., 2022). Codeine was significantly more effective than levodropropizine in reducing cough severity, as confirmed by changes in the VAS, Cough Severity Scale (CSS), and LCQ. Adverse events such as drowsiness, constipation, and headache were more frequently observed in the codeine-treated group, although these did not lead to a higher number of treatment discontinuations. These results indicate that codeine may be more effective in relieving chronic cough, but its use is associated with the risk of side effects typical of opioid medications. In contrast, levodropropizine, despite being slightly less effective, has a more favorable safety profile, making it a potentially better choice for long-term therapy.
The present review also identified several studies evaluating natural antitussive agents that could not be included in the quantitative synthesis due to substantial heterogeneity in study design, methodology, outcome measures, endpoints, and study populations.
Similarly, studies assessing natural or plant-based preparations demonstrated encouraging yet inconsistent results. Barth et al. showed that a combination of aqueous ethanolic extracts of Justicia adhatoda L. leaf, Echinacea purpurea (L.) Moench root and Eleutherococcus senticosus Harms root have an antitussive effect in patients aged 18–65 years with non-complicated URTI (Barth et al., 2015). What is more, another study (Canciani et al., 2014) confirmed that the use of Grintuss® syrup containing resins, polysaccharides, saponins, flavonoids and sugars derived from Grindelia robusta, Plantago lanceolata, Helichrysum italicum and honey leads to an improvement in cough symptoms in children, especially nocturnal cough, after just 4 days of use. Carnevall et al. also demonstrated that KalobaTUSS® syrup (acacia honey in combination with Malva sylvestris, Inula helenium, Plantago major, and Helichrysum stoechas extracts) reduced the severity and duration of daytime and nighttime cough in children with acute cough. However, it should be noted that these two studies focused on entirely different ingredients, so there is considerable risk in interpreting the results comprehensively (Carnevali et al., 2021). Another new substance was investigated in a study conducted in Iran (Ghaemi et al., 2020), which showed that lozenges containing licorice root extract (Glycyrrhiza glabra L.) effectively relieved symptoms of chronic cough of unknown etiology. After 2 weeks of treatment and at a four-week follow-up, a significant reduction in cough severity was observed compared to placebo, while quality of life, as assessed by the LCQ, improved.
It is also worth mentioning a study combining conventional asthma therapy with a traditional Chinese medicine preparation (Pan et al., 2025). This study demonstrated that Suhuang Zhike capsules can be an effective and safe adjunct to therapy in patients with mild to moderate asthma whose symptoms were inadequately controlled despite inhaled corticosteroids (ICS) and long-acting beta_2_-agonists (LABA) therapy. Although no significant improvement in Asthma Control Test (ACT) scores was observed in the overall population, a subgroup analysis of patients on stable treatment prior to enrollment demonstrated significant clinical improvement and reduced cough severity.
Another study (Núñez et al., 2024) showed that Sediflù syrup, containing active plant ingredients, effectively relieved cough during both the day and the night in children with upper respiratory tract infections. Significant improvement in cough severity was observed after just 2 days of treatment, and this effect persisted and intensified in subsequent days.
It should be emphasized, however, that the studies discussed in this paper differed significantly in terms of design, population, intervention type, and endpoints, which prevented their direct comparison in a meta-analysis. Some studies included preparations with mechanical or protective effects (Grintuss®, KalobaTUSS®, Sediflù), while others involved herbal products with potential anti-inflammatory or immunomodulatory effects (licorice, Suhuang Zhike, Xiehuangjiejing). The patient populations also varied, from children with acute infectious cough to patients with chronic cough or asthma, as did the intervention duration and methods for assessing efficacy (symptom scales, LCQ, VAS). Despite favorable clinical outcomes and a good safety profile, these results should be interpreted with caution because they come from studies of varying methodological quality and often a limited number of participants.
While several trials reported modest symptomatic relief, particularly in cough frequency and sleep quality, methodological weaknesses and lack of standardized outcomes considerably limit the strength and generalizability of these findings. Together, these observations underscore the urgent need for more rigorous, harmonized clinical trials with standardized outcome measures, adequate sample sizes, and improved study designs to assess better the comparative efficacy of both pharmacological and natural antitussive therapies.
The meta-analysis revealed that among the available RTCs on antitussive medications, those on P2X3 receptor antagonists demonstrated the greatest methodological consistency, particularly in the outcome measures used. Therefore, statistical analyses could be performed primarily for this group of medications, yielding reliable, comparable results on their efficacy and safety. Other interventions, due to the heterogeneity of cough assessment methods and the limited number of studies, could not be included in the quantitative analysis. This represents a significant limitation but also highlights the methodological advances in research on P2X3 antagonists.
The subgroup analysis revealed no statistically significant differences between P2X3 antagonists, indicating a consistent treatment effect across compounds. All subgroups demonstrated a reduction in cough frequency, suggesting that the observed effect is a class-related response rather than compound-specific.
After gefapixant administration, we also observed a statistically significant lower VAS score and a higher LCQ score, with a moderate, potentially clinically relevant effect and high certainty of evidence compared to placebo. In addition, after gefapixant administration, we observed that the intervention increased the risk of AEs by 41% compared with the placebo group, with low certainty of evidence. Also, sivopixant increased the risk of AEs by approximately 76% compared to the placebo group with moderate certainty of evidence. In contrast, eliapixant and camlipixant administration resulted in reductions of AEs of 2% and 15%, respectively, with low certainty of evidence. Furthermore, we noted that the type of P2X3 receptor has a significant impact on AEs frequency.
The GRADE assessment showed varying levels of evidence certainty across outcomes. Low heterogeneity, consistent effects, and narrow confidence intervals characterized high-certainty results. Moderate and low certainty were mainly due to heterogeneity, wide intervals, or a limited number of studies. Despite these differences, the overall results consistently indicated a beneficial effect of the intervention, supporting its clinical relevance.
The obtained results are consistent with previous meta-analyses and systematic reviews (Ramadan et al., 2023; Yamamoto et al., 2024), which also indicated the high efficacy of P2X3 receptor antagonists in reducing cough frequency in patients with refractory chronic cough.
From a clinical perspective, recent findings, together with our results, support the potential role of P2X3 antagonists as a targeted therapeutic option primarily for patients with refractory or unexplained chronic cough. By directly modulating cough hypersensitivity at the level of peripheral sensory pathways, these agents offer a mechanism-based, symptom-oriented approach rather than a replacement for etiological treatment, which remains the cornerstone of chronic cough management. Based on available clinical evidence, P2X3 antagonists may be best positioned as add-on or later-line therapies for patients whose symptoms persist despite optimized standard care. This treatment strategy aligns with emerging views that modulation of sensory neural pathways represents a promising adjunct approach in the management of chronic cough.
Safety and tolerability are central to the clinical implementation of P2X3 antagonists, particularly given their intended use in long-term treatment of chronic cough. In clinical studies with gefapixant, a high incidence of taste-related adverse effects has been reported, attributed to inhibition of the heteromeric P2X2/3 receptor (Yamamoto et al., 2024; Francke et al., 2025). Consequently, the development of more selective P2X3 antagonists has been pursued to improve tolerability while maintaining efficacy (Francke et al., 2025). Morice et al. (2021) showed that taste-related adverse events following eliapixant administration were less frequent at therapeutic doses than with the less selective P2X3 antagonist gefapixant. Although generally reversible upon discontinuation of treatment, taste-related adverse effects may negatively affect treatment adherence, especially during prolonged therapy. Significantly, the development of next-generation P2X3 antagonists with increased receptor selectivity has been associated with a lower incidence and severity of taste disturbances, suggesting a more favorable tolerability profile and supporting the feasibility of chronic administration. On the other hand, Morice et al. (2021) hypothesized that filapixant would be associated with a lower incidence of taste-related adverse effects compared with the non-selective P2X3/P2X2/3 antagonist gefapixant and the less selective P2X3 antagonist eliapixant. However, the results of their study were unexpected. Although filapixant was generally well tolerated, the frequency of taste-related adverse events was higher than anticipated. Therefore, further studies are required to evaluate sustained tolerability, optimal dosing strategies that balance efficacy and adverse effects, and to identify patient subgroups most likely to benefit from therapy with minimal impact on quality of life. Such data will be essential for defining the role of P2X3 antagonists within future chronic cough management algorithms and for informing clinical decision-making in routine practice.
Limitations
5
This meta-analysis included only pharmacological agents classified as antitussive drugs, acting directly on the cough reflex through central or peripheral mechanisms. Medications that may indirectly reduce cough by treating underlying airway inflammation or hyperresponsiveness, such as inhaled corticosteroids, leukotriene receptor antagonists, or bronchodilators, were not included. Therefore, the results primarily reflect the efficacy of classical antitussive therapy rather than broader pharmacological strategies targeting disease-specific mechanisms. This may limit the generalizability of the findings to patients whose cough is secondary to inflammatory or allergic airway disorders, such as asthma or eosinophilic bronchitis.
The available evidence may be influenced by publication bias, as studies with positive outcomes are more likely to be published, potentially overestimating the therapeutic efficacy of novel antitussive agents. Second, substantial heterogeneity exists across studies in terms of outcome measures, including differences in cough frequency assessment, patient-reported endpoints, and study duration, which limits direct comparability and quantitative synthesis of results. Finally, while P2X3 receptor antagonists are supported by the most robust clinical data to date, the number of high-quality, randomized trials evaluating alternative mechanistic targets remains limited. This imbalance limits broader conclusions about the relative efficacy of non-P2X3 therapies and underscores the need for well-designed trials across diverse antitussive strategies.
Although the literature search included both acute and chronic cough, only studies focusing on chronic cough met the inclusion criteria for quantitative synthesis. As a result, the meta-analysis and forest plots reflect evidence exclusively related to chronic cough. The absence of eligible studies on acute cough highlights a gap in the current literature and limits the generalizability of the findings to chronic cough populations only. Consequently, conclusions regarding the efficacy of P2X3 antagonists should not be extrapolated to acute cough.
Another limitation of this work is the inclusion of only English-language publications, which may have introduced a language-related selection bias. As a result, relevant studies published in other languages, particularly those originating from regions with extensive research on traditional medicine, such as China, may not have been captured. Numerous studies have investigated traditional herbal remedies with potential antitussive effects, however, many were excluded due to language restrictions and classification difficulties. Consequently, the exclusion of non-English studies and traditional herbal formulations may limit the completeness of the evidence base and should be considered when interpreting the findings of this review.
Conslusions
6
Our study confirms that despite the long history of use of codeine and other antitussives, both centrally (butamirate, dextromethorphan) and peripherally (levodropropizine), evidence for their effectiveness remains limited, and the available data are scattered and inconsistent. In recent years, there has been growing interest in natural preparations as alternatives to traditional antitussives. However, their efficacy and safety remain inconsistent, highlighting the need for further, high-quality clinical trials. P2X3 receptor antagonists deserve particular attention, as they have shown potential to reduce cough frequency and severity in available studies. In addition, all P2X3 antagonists reduced cough frequency, with no significant differences between compounds. Accordingly, P2X3 represents a promising direction for the development of new therapies. In this context, the concept of “beyond codeine” takes on particular significance–it encompasses not only the search for more effective and safer synthetic drugs but also the development of therapies targeting new, peripheral molecular targets, such as P2X3 receptors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abdulqawi R. Dockry R. Holt K. Layton G. Mc Carthy B. G. Ford A. P. (2015). P 2X 3 receptor antagonist (AF-219) in refractory chronic cough: a randomised, double-blind, placebo-controlled phase 2 study. Lancet 385 (9974), 1198–1205. 10.1016/S 0140-6736(14)61255-1 25467586 · doi ↗ · pubmed ↗
- 2Barth A. Hovhannisyan A. Jamalyan K. Narimanyan M. (2015). Antitussive effect of a fixed combination of Justicia adhatoda, Echinacea purpurea and Eleutherococcus senticosus extracts in patients with acute upper respiratory tract infection: a comparative, randomized, double-blind, placebo-controlled study. Phytomedicine 22 (13), 1195–1200. 10.1016/j.phymed.2015.10.001 26598919 · doi ↗ · pubmed ↗
- 3Bhattacharya M. Joshi N. Yadav S. (2013). To compare the effect of dextromethorphan, promethazine and placebo on nocturnal cough in children aged 1-12 y with upper respiratory infections: a randomized controlled trial. Indian J. Pediatr. 80 (11), 891–895. 10.1007/s 12098-013-1002-2 23592248 · doi ↗ · pubmed ↗
- 4Birring S. S. Cardozo L. Dmochowski R. Dicpinigaitis P. Afzal A. La Rosa C. (2024). Efficacy and safety of gefapixant in women with chronic cough and cough-induced stress urinary incontinence: a phase 3b, randomised, multicentre, double-blind, placebo-controlled trial. Lancet Respir. Med. 12 (11), 855–864. 10.1016/S 2213-2600(24)00222-4 39222649 · doi ↗ · pubmed ↗
- 5Bruschi C. Crotti P. Dacosto E. Fanfulla F. Daffonchio L. Novellini R. (2003). Levodropropizine does not affect P 0.1 and breathing pattern in healthy volunteers and patients with chronic respiratory impairment. Pulm. Pharmacol. Ther. 16 (4), 231–236. 10.1016/S 1094-5539(03)00053-1 12850126 · doi ↗ · pubmed ↗
- 6Canciani M. Murgia V. Caimmi D. Anapurapu S. Licari A. Marseglia G. L. (2014). Efficacy of Grintuss® pediatric syrup in treating cough in children: a randomized, multicenter, double blind, placebo-controlled clinical trial. Ital. J. Pediatr. 10, 40–56. 10.1186/1824-7288-40-56 24917119 PMC 4066701 · doi ↗ · pubmed ↗
- 7Carnevali I. La Paglia R. Pauletto L. Raso F. Testa M. Mannucci C. (2021). Efficacy and safety of the syrup “Kaloba TUSS®” as a treatment for cough in children: a randomized, double blind, placebo-controlled clinical trial. BMC Pediatr. 21 (1), 29. 10.1186/s 12887-020-02490-2 33430841 PMC 7798282 · doi ↗ · pubmed ↗
- 8Charpin J. Weibel M. A. (1990). Comparative evaluation of the antitussive activity of butamirate citrate linctus versus clobutinol syrup. Respiration 57 (4), 275–279. 10.1159/000195855 2095610 · doi ↗ · pubmed ↗