Comparative efficacy and safety of three internal fixation strategies for femoral neck fractures: a network meta-analysis
Min Liu, Liyan Mao, Chongyang Zhao, Huan Li, Tao Chen, Jialei Chen, Xiaobing Pu

TL;DR
This study compares three surgical methods for femoral neck fractures and finds that one method may heal faster and reduce complications, though more research is needed.
Contribution
A network meta-analysis comparing the clinical efficacy and safety of three femoral neck fracture fixation methods.
Findings
FNS showed better Harris Hip Scores and faster healing than CCS.
FNS and CCS had lower femoral head necrosis rates than DHS.
CCS resulted in less intraoperative blood loss compared to FNS and DHS.
Abstract
Currently, the most common internal fixation devices for femoral neck fractures are cannulated compression screws (CCS), dynamic hip screws (DHS), and femoral neck systems (FNS). However, no clear consensus exists regarding which device offers superior clinical efficacy and safety. We systematically searched three databases (PubMed, Embase, and Cochrane Library) for clinical studies published from their inception until March 12, 2025. We included studies that directly compared the three internal fixation methods: FNS, DHS, and CCS. Outcomes of interest were analyzed using pairwise and network meta-analyses. This network meta-analysis included 23 studies comprising 55,910 patients. FNS demonstrated a statistically significant higher Harris Hip Score (MD 3.79, 95% CI 1.44–6.13) and a shorter fracture healing time (MD −1.00 months, 95% CI −1.53 to −0.48) compared to CCS. Both FNS and CCS…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
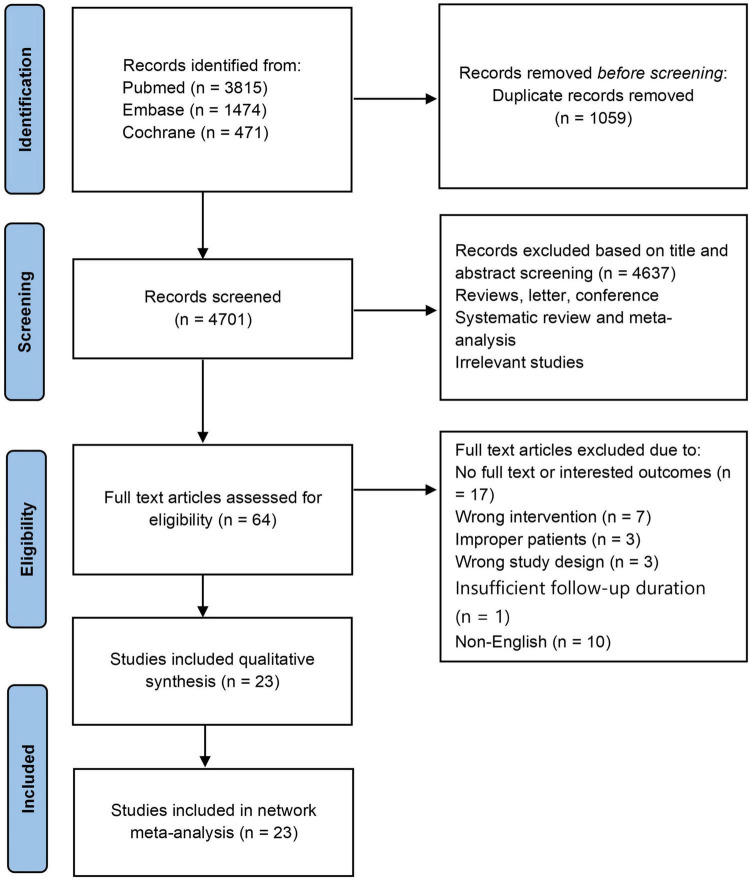 FIGURE 1
FIGURE 1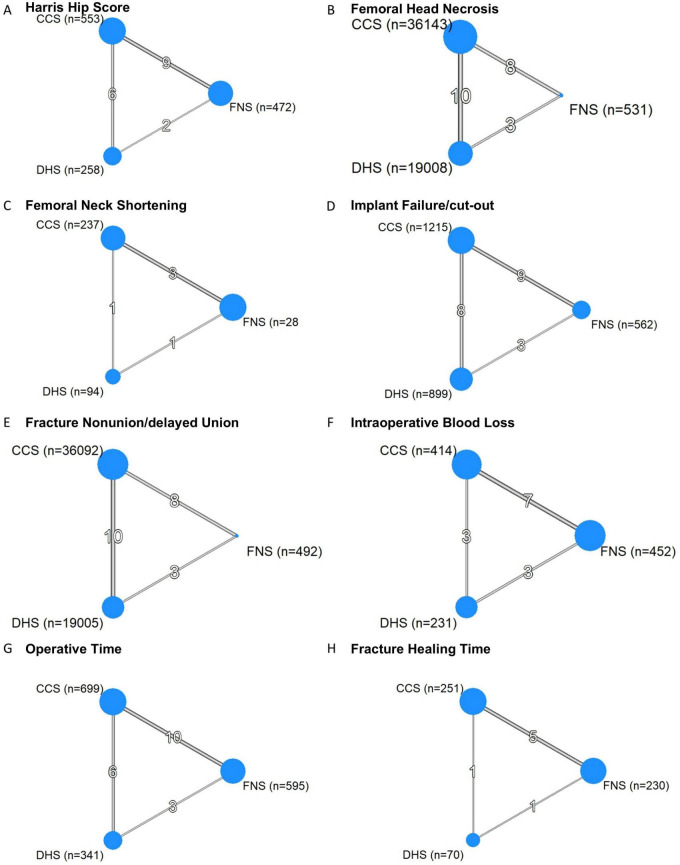 FIGURE 2
FIGURE 2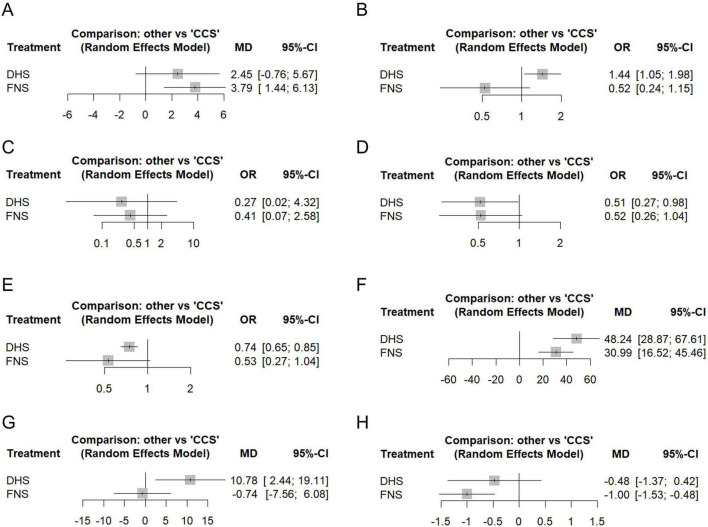 FIGURE 3
FIGURE 3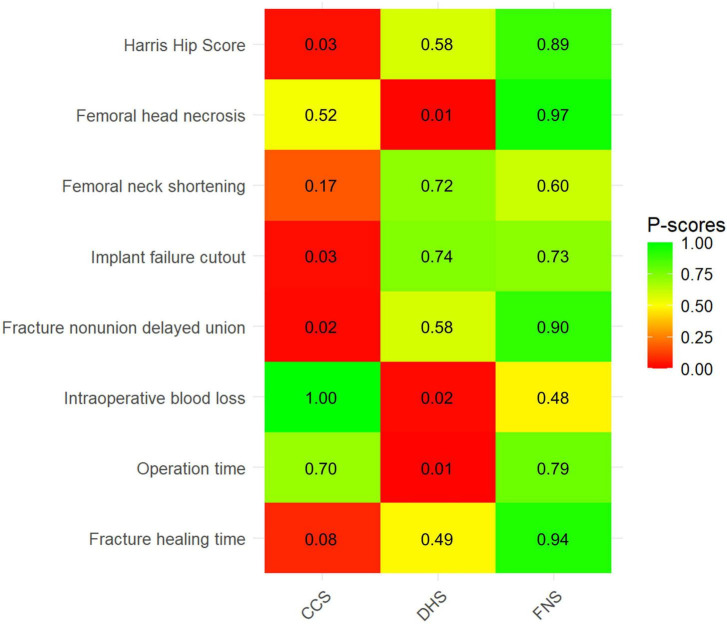 FIGURE 4
FIGURE 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip and Femur Fractures · Orthopaedic implants and arthroplasty · Bone fractures and treatments
Introduction
Femoral neck fractures account for 3.6% of all fractures and 53% of hip fractures (1). With population aging, the incidence of hip fractures in older adults is projected to rise significantly (2). By 2050, the age-standardized incidence rate is expected to reach 1,055.30 cases per 100,000 person-years, imposing substantial socioeconomic and healthcare system burdens (3, 4). Moreover, femoral neck fractures in the elderly are predominantly osteoporotic fragility fractures, where intrinsically compromised bone quality and abnormal bone metabolism substantially increase the complexity of internal fixation and present an ongoing challenge for clinical decision-making (5).
Current surgical treatments for femoral neck fractures primarily involve internal fixation and hip arthroplasty (6). Among internal fixation methods, cannulated compression screws (CCS) and dynamic hip screws (DHS) are commonly used devices (7). The established CCS technique employs three screws arranged in an inverted triangular configuration, offering advantages such as minimal invasiveness, fracture compression, and rotational stability (8). This approach is particularly suitable for non-displaced fractures in elderly patients (9). However, CCS demonstrates limited shear resistance and provides only static compression, which may lead to micromotion at the fracture site during weight-bearing (10). This can hinder healing and increase risks of complications, such as screw cut-out and fixation failure. In contrast, DHS provides angular stability with enhanced lateral cortical support (11, 12). Its sliding compression mechanism promotes fracture healing, but the bulky design requires more extensive surgical exposure (13, 14). Consequently, the use of DHS may be restricted in patients with compromised overall health.
The femoral neck system (FNS; DePuy Synthes, Zuchwil, Switzerland), introduced in 2017, was designed to optimize minimally invasive techniques and enhance biomechanical stability (15, 16). The biomechanical study by Stoffel et al. demonstrated that the stability of FNS is superior to CCS and comparable to DHS (17). However, a clinical consensus is lacking regarding the comparative safety and efficacy of these three internal fixation techniques. Existing research remains confined to pairwise comparisons with limited sample sizes, resulting in reduced statistical power and imprecise effect estimates (18–21). To address this evidence gap, we conducted the first network meta-analysis integrating both direct and indirect evidence across all three fixation methods. This approach allows simultaneous comparison among multiple interventions, overcoming the limitations of previous pairwise analyses. By synthesizing a broader range of studies than previously available, we have strengthened the robustness of the pooled estimates and, through the unique advantages of network meta-analysis, provided a preliminary, probability-based ranking of treatments based on the current body of evidence.
This network meta-analysis was conducted to evaluate the comparative effectiveness and safety of the three fixation methods—FNS, CCS, and DHS. Our primary research question was: In patients with femoral neck fractures, which internal fixation method demonstrates superior clinical efficacy (as measured by the Harris Hip Score) and a more favorable safety profile, particularly regarding the risks of femoral neck shortening, femoral head necrosis, implant failure/cut-out, and fracture nonunion/delayed union?
The article is organized into the following sections. The Methods section describes the search strategy, study selection criteria, data extraction, risk-of-bias assessment, and statistical synthesis. The Results section reports the characteristics of the included studies, the pooled results, and the treatment rankings. The Discussion section interprets the key findings in a clinical context and discusses the limitations of the evidence. Finally, the Conclusion section summarizes the principal conclusions and suggests directions for future research.
Methods
This study followed a registered protocol with PROSPERO (registration number: CRD420251014243), with one amendment implemented during the screening phase (rationale documented in the registry), and adheres to the Preferred Reporting Items for meta-analysis (PRISMA) guidelines (22).
Search strategy
We systematically searched PubMed, Embase, and Cochrane Library databases from inception through March 12, 2025, for relevant clinical studies. The search strategy incorporated key subject headings, including femoral neck fractures, femoral neck system, cannulated screws, and dynamic hip screws. Detailed search terms are provided in Supplementary Information 1.
Eligibility criteria
We developed the inclusion criteria according to the PICOS principle. (1) Population: Adults > 18 years diagnosed with unilateral femoral neck fractures. (2) Intervention: patients were treated with FNS. (3) Comparison: Fixation using either three CCS or DHS. (4) Outcome: Studies reporting at least one of the following primary outcomes: Harris Hip Score (HHS) and postoperative complications [e.g., femoral head necrosis (FHN), femoral neck shortening, implant failure/cut-out (IFC), fracture nonunion/delayed union (FNDU)], with a minimum 6-month follow-up for data completeness. (5) Study Design: Randomized controlled trials (RCTs) and cohort studies. Exclusion Criteria: (1) Patients with polytrauma, pathological fractures, open fractures, or revision surgeries. (2) Studies without full-text availability, duplicate datasets, or non-English publications. (3) biomechanics or animal research, finite element analysis, meta-analysis, review articles, case reports, conference abstracts, comments, and letters to editors.
Definition of interventions
Each internal fixation device was explicitly defined to ensure comparability: CCS: Three parallel cannulated screws placed in an inverted triangular configuration. DHS: A sliding hip screw system consisting of a lag screw and a side plate fixed to the lateral femoral cortex. This category includes DHS with or without an additional anti-rotation screw. FNS: The dedicated femoral neck fixation system (DePuy Synthes) comprising an intramedullary nail, a locking bolt, and anti-rotation screw. Studies employing hybrid techniques or non-standard variants were excluded.
Data extraction and quality assessment
Two reviewers independently extracted data using a predefined form and cross-verified for consistency. Discrepancies were resolved through discussion with a third reviewer. Extracted parameters included: first author, country, publication year, study design, intervention, sample size, patient age, gender, follow-up duration, fracture classification, and outcome measures. Primary outcomes comprised HHS and postoperative complications (e.g., FHN, femoral neck shortening, IFC, and FNDU). Secondary outcomes included intraoperative blood loss (IBL), operative time (OT), and fracture healing time (FHT). For each outcome within a study, data from the longest available follow-up time were extracted are reported in months. In addition, when studies reported outcomes as medians with ranges or interquartile ranges instead of means and standard deviations, we converted these summary statistics using the validated “Mean and Standard Deviation Calculator” developed by Tong et al. (23), which applies methods described by Luo et al. (24) and Wan et al. (25).
We employed the Cochrane Tool to assess the risk of bias for the included randomized controlled trials (RCTs) (26). Furthermore, for cohort studies, we used the Risk of Bias in Non-randomized Studies—of Interventions (ROBINS-I) tool to evaluate bias across seven domains: Bias due to confounding, participant selection, intervention classification, departures from intended interventions, missing data, outcome measurement, and selection of the reported result (27).
Data analysis
Data were analyzed using frequentist network meta-analysis with evidence network visualization, applying the random effects model (package netmeta, version 3.2–0) described by Rücker (28) and Rücker and Schwarzer (29), within the R 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria). Tau-squared (τ^2^) statistic calculated via the DerSimonian-Laird random-effects model was used to estimate the variance in heterogeneity between studies. We used the I^2^ statistic and Cochran’s Q statistic to assess heterogeneity across the entire network, within-design heterogeneity, and between-design inconsistency. I^2^ values < 25% indicated low heterogeneity; I^2^ values > 50% denoted substantial heterogeneity. Statistical significance was defined as p < 0.05. For multi-arm trials (studies with more than two treatment groups), we accounted for within-study correlation by appropriately splitting the shared control group sample size, preventing double-counting and ensuring valid standard error estimation. Missing outcome data were handled using complete-case analysis, including only participants with available data. For dichotomous outcomes with rare events (zero cells in contingency tables), we applied a continuity correction of 0.5.
We assessed local inconsistency within the network meta-analysis with the node-splitting method and quantified the contributions of direct and indirect evidence. Potential publication bias was evaluated using comparison-adjusted funnel plots symmetry and Egger’s test (30, 31). Pairwise meta-analyses were performed for all direct comparisons of primary and secondary outcomes. Treatments were ranked using P-scores (29). For the primary outcomes, absolute effects were calculated based on a baseline risk estimated from the pooled event rate in the CCS control groups. Furthermore, we conducted a leave-one-out sensitivity analysis by iteratively excluding individual studies to evaluate the robustness of the pooled effect estimates. Finally, to explore potential sources of heterogeneity, we pre-specified the following factors as potential effect modifiers for transitivity assessment and clinical heterogeneity prior to analysis: fracture displacement (Garden classification), reduction quality, osteoporosis status, age, and follow-up duration. Based on these, subgroup analyses and a meta-regression were performed for highly heterogeneous outcomes, using the gemtc package (version 1.1-0). A CINeMA (Confidence in Network Meta-Analysis) assessment was performed to evaluate the certainty of evidence for all outcomes (32, 33), and overall confidence was rated as High, Moderate, Low, or Very low.
Results
Included study
A comprehensive database search up to March 12, 2025, yielded 5,760 records. After removing 1,059 duplicates, 4,701 records underwent title and abstract screening. Of these, 4,637 records were excluded. Full-text assessment of the remaining 64 articles against predefined eligibility criteria resulted in the exclusion of 41 studies. Reasons for exclusion at the full-text stage are provided in Supplementary Table 1. Ultimately, 23 studies qualified for inclusion in the systematic review and network meta-analysis (Figure 1).
PRISMA flow diagram.
Study characteristics and quality assessment
The analysis included 5 RCTs (34–38) and 18 cohort studies (39–56), encompassing 55,910 patients. Detailed study characteristics are provided in Supplementary Information 2. Figure 2 presents network evidence diagrams for all outcome measures. Regarding quality assessment, Supplementary Figure 1 illustrates the risk of bias for included RCTs. Notably, all RCTs showed limitations in blinding procedures. For cohort studies, ROBINS-I assessment revealed that most studies were judged to be at “Moderate” overall risk of bias, predominantly due to residual confounding, outcome assessment, and potential selective reporting inherent to retrospective designs. One study (40) was rated at “Serious” overall risk due to critical unmeasured confounding (e.g., fracture displacement not controlled). The full ROBINS-I assessment is summarized in Supplementary Table 2.
Network graphs of primary and secondary outcomes. Panels show network evidence diagrams for each outcome, with node size proportional to the number of participants receiving each treatment and edge thickness proportional to the number of studies informing each direct comparison. (A) Harris hip score. (B) Femoral head necrosis. (C) Femoral neck shortening. (D) Implant failure/cut-out. (E) Fracture nonunion/delayed union. (F) Intraoperative blood loss. (G) Operative time. (H) Fracture healing time. CCS, cannulated compression screw; DHS, dynamic hip screw; FNS, femoral neck system.
Primary outcomes
Harris hip score
The Harris Hip Score (HHS), a validated instrument assessing pain, function, deformity, and range of motion, served as a key indicator of hip joint function, with higher scores indicating better outcomes (57). HHS was reported by 15 studies comprising 1,283 patients (Supplementary Figure 2). Compared with CCS, FNS demonstrated significantly higher HHS scores (MD 3.79, 95% CI 1.44–6.13). No statistically significant differences were observed between DHS and CCS (MD 2.45, 95% CI −0.76 to 5.67) or between DHS and FNS (MD −1.33, 95% CI −4.86 to 2.19) (Figure 3 and Supplementary Figure 3). Substantial network heterogeneity was detected for this outcome (I^2^ = 90.1%).
Forest plots for all outcomes from the network meta-analysis. Mean difference (MD) or odds ratio (OR) with 95% confidence intervals (CI) was used to measure the relative efficacy of different treatments compared to CCS. (A) Harris hip score. (B) Femoral head necrosis. (C) Femoral neck shortening. (D) Implant failure/cut-out. (E) Fracture nonunion/delayed union. (F) Intraoperative blood loss. (G) Operative time. (H) Fracture healing time. CCS, Cannulated compression screw; DHS, Dynamic hip screw; FNS, Femoral neck system.
Femoral head necrosis
FHN incidence was evaluated across 21 studies involving 55,682 patients (Supplementary Figure 4). The DHS group demonstrated significantly higher FHN risk than both the CCS group (OR 1.44, 95% CI 1.05–1.98) and the FNS group (OR 2.74, 95% CI 1.22–6.16), with no observed heterogeneity (I^2^ = 0%). Based on the CCS baseline risk of 5.45%, the absolute risk increase with DHS versus CCS was 2.21% (95% CI 0.26– 4.80%). No statistically significant difference emerged between FNS and CCS groups (OR 0.52, 95% CI 0.24–1.15) (Figure 3 and Supplementary Figure 5).
Femoral neck shortening
Femoral neck shortening, a common complication after internal fixation, was evaluated with a focus on clinically severe shortening (typically defined as > 10 mm), which is associated with impaired hip mechanics and function (58). It was evaluated in 5 studies comprising 612 patients (Supplementary Figure 6). Compared to CCS, neither DHS (OR 0.27, 95% CI 0.02–4.32) nor FNS (OR 0.41, 95% CI 0.07–2.58) showed significant differences in femoral neck shortening risk. Similarly, no significant difference emerged between DHS and FNS groups (OR 0.65, 95% CI 0.04–10.25) (Figure 3 and Supplementary Figure 7). Based on the CCS baseline risk of 12.86%, DHS and FNS were associated with absolute risk reductions (ARR) compared with CCS: −9.03% (95% CI −12.56 to 26.07) and −7.15% (95% CI −11.84 to 14.71), respectively. Substantial network heterogeneity was detected for this outcome (I^2^ = 82.2%).
Implant failure/cut-out
IFC was evaluated in 18 studies comprising 2,676 patients (Supplementary Figure 8). Compared with CCS, DHS significantly reduced the risk of IFC (OR 0.51, 95% CI 0.27–0.98), yielding an ARR of 3.40% (95% CI 0.13–5.15) based on the 7.21% baseline risk. While no significant difference was observed for FNS versus CCS (OR 0.52, 95% CI 0.26–1.04). DHS and FNS showed comparable IFC risk (OR 0.99, 95% CI 0.42–2.30) (Figure 3 and Supplementary Figure 9). All comparisons exhibited low heterogeneity (I^2^ = 23%).
Fracture nonunion/delayed union
FNDU was evaluated in 19 studies comprising 55,589 patients (Figure 3 and Supplementary Figure 10). Compared to CCS, DHS demonstrated significantly lower FNDU risk (OR 0.74, 95% CI 0.65–0.85). Based on the CCS baseline risk of 5.81%, this corresponds to an ARR of 1.44% (95% CI 0.83–1.95) for DHS. In contrast, no statistically significant difference was observed between FNS and CCS (OR 0.53, 95% CI 0.27–1.04) or between DHS and FNS (OR 1.41, 95% CI 0.71–2.77) (Figure 3 and Supplementary Figure 11). All comparisons exhibited minimal heterogeneity (I^2^ = 0%).
Secondary outcomes
Intraoperative blood loss
IBL was recorded in 11 studies comprising 1,097 patients (Figure 3 and Supplementary Figure 12). Both DHS (MD 48.24 mL, 95% CI 28.87–67.61) and FNS (MD 30.99 mL, 95% CI 16.52–45.46) demonstrated significantly greater blood loss than CCS. No significant difference was observed between DHS and FNS (MD 17.25 mL, 95% CI −1.80 to 36.30) (Figure 3 and Supplementary Figure 13). All comparisons exhibited substantial heterogeneity (I^2^ = 96.8%).
Operative time
OT was recorded in 17 studies comprising 1,635 patients (Supplementary Figure 14). DHS procedures were significantly longer than both CCS (MD 10.78 min, 95% CI 2.44–19.11) and FNS (MD 11.52 min, 95% CI 2.34–20.70). No significant difference emerged between FNS and CCS (MD −0.74 min, 95% CI −7.56 to 6.08) (Figure 3 and Supplementary Figure 15). All comparisons exhibited substantial heterogeneity (I^2^ = 94.5%).
Fracture healing time
FHT was evaluated across 7 studies involving 551 patients (Supplementary Figure 16). FNS demonstrated significantly shorter healing time than CCS (MD −1.00 months, 95% CI −1.53 to −0.48). No significant differences were observed between DHS and FNS (MD 0.53 months, 95% CI −0.38 to 1.43) or between DHS and CCS (MD −0.48 months, 95% CI −1.37 to 0.42) (Figure 3 and Supplementary Figure 17). All comparisons exhibited substantial heterogeneity (I^2^ = 94.2%).
Ranking of treatments
Figure 4 presents the P-score rankings for the three fixation technologies. FNS ranked first for HHS, FHN, FNDU, OT, and FHT, while securing second position across all remaining outcomes. CCS demonstrated a superior ranking only for IBL. DHS showed marginally higher P-scores than FNS in femoral neck shortening and IFC, earning first rank for these outcomes.
P-score ranking for primary and secondary outcomes. Color intensity corresponds to P-Score values (darker green = higher rank probability). P-score quantifies the probability of a treatment being ranked first (range: 0–1). Numeric values indicate P-scores. CCS, Cannulated compression screw; DHS, Dynamic hip screw; FNS, Femoral neck system.
Publication bias and inconsistency
Comparison-adjusted funnel plots for all outcomes demonstrated symmetrical distributions (Supplementary Figure 18), with Egger’s test p-values > 0.05 for outcomes with ≥ 10 studies, suggesting no significant publication bias. Egger’s test was not performed for femoral neck shortening and FHT due to limited studies ( < 10). Global inconsistency, assessed via the design-by-treatment interaction model, was statistically significant for HHS (Q = 11.31, p = 0.010), IBL (Q = 91.03, p < 0.001), OT (Q = 60.99, p < 0.001), and FHT (Q = 13.64, p = 0.0002), but not for other outcomes (all p > 0.05, see Supplementary Information 1 for details). Local inconsistency testing using the node-splitting approach revealed significant disagreement between direct and indirect evidence for IBL in the FNS vs. CCS (p = 0.002) and DHS vs. FNS (p = 0.014) comparisons. For all other outcomes, no significant local inconsistency was detected (all p > 0.05; see Supplementary Figures 19–26 for full results).
Sensitivity and exploratory analyses
Sensitivity analyses demonstrated robust findings for most outcomes upon sequential exclusion of individual studies (Supplementary Figures 27–32). For femoral head necrosis, exclusion of the study by Jetto et al. (40)—the largest retrospective registry study contributing substantial weight—resulted in a slight attenuation of the effect estimate for DHS versus CCS, with the confidence interval crossing unity (from OR 1.44, 95% CI 1.05–1.98 to OR 1.39, 95% CI 0.96–2.02). However, the direction of effect remained consistent, and the estimates for other comparisons (FNS vs. CCS and DHS vs. FNS) were largely unchanged. For fracture nonunion/delayed union, exclusion of the same study rendered the DHS versus CCS comparison non-significant, with substantially widened confidence intervals (OR changed from 0.74, 95% CI 0.65–0.85 to 0.72, 95% CI 0.49–1.06), while other comparisons remained stable, indicating its notable influence on outcome stability. Sensitivity analysis was not feasible for femoral neck shortening and FHT due to the limited included studies, where the removal of any single trial disrupted network connectivity.
Subgroup analyses revealed that in the fracture type subgroup, the DHS versus CCS comparison became statistically significant, unlike in the overall analysis, and heterogeneity decreased from I^2^ = 90.1–70.9% (detailed in Supplementary Table 3). In contrast, no significant differences from the primary treatment effects or substantial reductions in heterogeneity were observed in the subgroups based on study design or follow-up duration. For femoral head necrosis, the subgroup analysis by DHS design showed an OR of 1.46 (95% CI 0.84–2.54) for standard DHS vs. CCS, and an OR of 0.96 (95% CI 0.38–2.39) for DHS with an anti-rotation screw vs. CCS.
Network meta-regression revealed that age had a consistent negative moderating effect across all outcomes. However, this effect was statistically significant only for intraoperative blood loss (as shown in Supplementary Table 4). The relative treatment effects and their statistical significance for all comparisons remained consistent with the primary analysis.
Assessment of the certainty of evidence
The certainty of evidence, assessed using the CINeMA framework, was low or very low for the majority of comparisons across outcomes. The most common reasons for downgrading were within-study bias, imprecision, or heterogeneity. Detailed ratings for each outcome are presented in Supplementary Table 5.
Discussion
This network meta-analysis was conducted to evaluate the comparative effectiveness and safety of FNS, CCS, and DHS for femoral neck fractures, with the aim of determining the optimal fixation strategy. Our findings, within the constraints of the available data, indicate that no single method was universally superior across all outcomes, but each demonstrated distinct strengths: FNS significantly outperformed CCS in HHS and fracture healing time, while also significantly surpassing DHS in operative time and femoral head necrosis. DHS showed significantly lower risks of implant failure/cut-out and fracture nonunion/delayed union compared to CCS, with comparable performance to FNS. CCS demonstrated significant superiority over DHS in femoral head necrosis and operative time, while also showing a significant reduction in intraoperative blood loss compared to both DHS and FNS. However, given that the CINeMA assessment indicated generally low or very low certainty of evidence for most comparisons, the P-score rankings which offer a probability-based hierarchy of relative treatment performance should not be equated with definitive clinical superiority, especially for outcomes with small, non-significant, or highly heterogeneous between-treatment differences. Therefore, clinical decision-making should prioritize specific effect estimates, confidence intervals, and patient-centered goals over the rank order itself.
Our network meta-analysis found that FNS yielded significantly higher HHS compared to CCS, aligning with findings from Jiang et al. and Patel et al. (18, 59). The superior HHS observed with the FNS may be attributed to its capacity to prevent femoral neck shortening while mitigating complications, including femoral head necrosis and implant failure/cut-out. Substantial evidence indicates that femoral neck shortening markedly compromises hip function and quality of life. Mechanistically, this results from reduced moment arms of hip abductor muscles, causing limping and weakened abduction strength that collectively impair hip function (60). Furthermore, femoral head necrosis and fixation failure induce hip pain and restricted motion at varying severity levels, thereby directly diminishing HHS outcomes (61, 62). While the FNS showed a statistically significant improvement in HHS over CCS (mean difference 3.79), this change remains below the reported Minimal Clinically Important Difference (MCID) of 6–10 points for HHS in this population (63–65). Although the result suggests a positive trend, its clinical relevance at the individual level is likely modest. Therefore, when choosing a treatment, this potential functional benefit of FNS should be weighed against its complication risks, cost, and technical demands. The considerable heterogeneity observed in HHS outcomes underscores the potential role of fracture type as an effect modifier, as suggested by our subgroup analysis of mixed populations (Garden I-IV/II-IV). Unfortunately, the available literature’s lack of outcome stratification by fracture subtype prevented a more granular analysis. Consequently, our findings should be interpreted with caution. Future high-quality research focusing on specific fracture types is essential to definitively elucidate the comparative effectiveness of these three fixation devices on HHS, providing tailored guidance for clinical implant selection.
For femoral neck shortening, although no statistically significant differences were observed among the three fixation techniques, the odds ratios suggested a potential hierarchy: DHS demonstrated marginally superior outcomes relative to FNS, with CCS showing the least favorable results. It is important to note that the considerable heterogeneity and the sparse, inconsistent high-quality evidence necessitate a cautious interpretation of these results. Evidence suggests that fracture type (Garden III–IV) and reduction quality (III–IV) are key predictors of postoperative femoral neck shortening, potentially explaining the significant heterogeneity in our findings (66–68). Demographic variations may represent another source of heterogeneity. Older patients with osteoporosis frequently demonstrate compromised bone quality, prolonged fracture healing, and poorer implant stability. These factors increase susceptibility to deformation during weight-bearing, consequently leading to femoral neck shortening (69, 70). Unfortunately, the limited number of available studies precluded meaningful subgroup analysis. Further studies are necessary.
The significantly higher incidence of femoral head necrosis observed with DHS compared to CCS and FNS stems from its larger bolt diameter. This design characteristic generates greater surgical trauma, necessitates more bone removal, and induces rotational displacement during insertion—all factors contributing to impaired femoral head perfusion (13, 71, 72). In contrast, FNS’s smooth nail design and minimally invasive approach preserve blood supply. Furthermore, DHS demonstrated superior outcomes versus CCS for both implant failure/cut-out and fracture nonunion/delayed union. DHS converts vertical loads into axial compression at the fracture site via a sliding compression mechanism, enhancing interfragmentary compression and promoting fracture healing (73). Additionally, its larger lag screw diameter also increases bone-implant contact area and friction, reducing the risks of implant failure/cut-out and fracture nonunion/delayed union. FNS exhibited mechanical stability comparable to DHS with similar compression advantages (74, 75). Consequently, no significant differences were observed between FNS and DHS regarding implant failure/cut-out, fracture nonunion/delayed union, and fracture healing time. It should be noted that the pooled estimates for femoral head necrosis and fracture nonunion/delayed union were influenced by a single large retrospective registry study (Jetto et al.), which contributed substantial weight to these analyses. Sensitivity analysis excluding this study attenuated the DHS versus CCS comparisons for both outcomes to non-significance. However, the direction of effect remained consistent across both outcomes, and comparisons involving FNS were largely unchanged. These findings suggest that while the precision and statistical significance of the DHS versus CCS comparisons may be overestimated by the inclusion of this large study, the overall trends remain mechanistically plausible. Nevertheless, confirmation in future high-quality studies is warranted.
CCS demonstrated the lowest intraoperative blood loss, followed by FNS, with DHS exhibiting the highest volumes. Operative time was the longest for DHS, while FNS procedures were non-significantly shorter than CCS. Notably, FNS achieved this efficiency despite surgeons’ relative inexperience with this newer system, suggesting that it may offer greater ease of use compared to the established CCS and DHS techniques. The substantial heterogeneity observed likely stems from variations in patient age, which our meta-regression indicated was a significant moderator for blood loss, with the differences between treatments diminishing in older patients.
Notably, caution is required when extrapolating our findings to older adults. Although our study included adults across the age spectrum, subgroup analyses by age or osteoporosis status were not feasible. Since femoral neck fractures in the elderly are predominantly osteoporotic, their distinct bone-healing biology—such as impaired osteoblast function, aberrant stem cell activity, and a pro-resorptive microenvironment—may alter the healing response to different fixation devices (76, 77). Simultaneously, the degraded biomechanical environment, characterized by reduced bone mineral density and loss of trabecular connectivity, can directly compromise implant stability (78–80). Consequently, in osteoporotic bone, implant fixation strength, cut-out resistance, and control of micro-motion become paramount. Therefore, our primary findings may not directly inform decision-making for older osteoporotic patients, underscoring the urgent need for high-quality, targeted studies in this population. Moreover, the interpretation of these pooled estimates requires caution due to substantial statistical heterogeneity. Several outcomes in this analysis, including HHS, intraoperative blood loss, and fracture healing time, exhibited substantial statistical heterogeneity (I^2^ > 90%). As noted in the preceding discussions, potential sources are multifaceted and may include clinical diversity (e.g., variations in patient age, displacement, osteoporosis status, and rehabilitation protocols) and methodological diversity (e.g., differences in surgical technique, follow-up duration, and study design). Notably, the predominance of retrospective cohort studies in our analysis (18 of 23, mostly moderate risk of bias) introduces residual confounding from unmeasured factors—such as fracture displacement and surgeon selection bias—that could not be fully accounted for. These methodological limitations likely contribute substantially to the observed heterogeneity. While random-effects models were employed to incorporate this between-study variance, the high heterogeneity fundamentally suggests that the pooled effect estimates should be interpreted as an average across a diverse set of clinical scenarios rather than a precise predictor for all individuals. This underscores the need for caution when generalizing these findings and highlights that clinical decision-making should remain tailored to specific patient and contextual factors.
While the FNS has shown promising results for femoral neck fractures, several concerns require urgent resolution, such as the potential for subtrochanteric fracture, unclear cost-effectiveness, and a substantial lack of long-term evidence. Firstly, clinical case reports have suggested a potential risk of subtrochanteric fractures with the FNS (81, 82). This hypothesis is further corroborated by several biomechanical studies. Fan et al. demonstrated that the peak von Mises stress on the distal locking screw of the FNS in the lesser trochanteric region reaches approximately 80 MPa—higher than that observed with three CCS (83). Similarly, Jung et al. found that a longer lateral plate length and a valgus bolt position elevate cortical bone strain around the distal-most locking screw in FNS, consequently increasing the risk of subtrochanteric fracture (84). However, as the available evidence on FNS-related subtrochanteric fractures is largely confined to biomechanics and lacks clinical data, high-quality clinical studies are required to clarify the incidence and influencing factors of this complication. Secondly, cost-effectiveness plays an important role in clinical decisions. However, there is currently no cost-effectiveness analysis evidence demonstrating that the significantly higher price of FNS over three CCS can be offset by commensurate benefits (85). Finally, as a relatively new technology, FNS has a limited history of clinical application, and its optimal clinical indications-such as appropriate patient age and specific fracture types-remain undefined. A study initiated by the AO Foundation found that in younger patients under 58 years, HHS were uniformly good to excellent. In contrast, the distribution of HHS in patients aged 58–80 years was similar to that in those over 80 years, ranging widely from 25 to 100 (86). This indicates that postoperative functional recovery with FNS is superior in younger populations compared to older adults. This observation is consistent with the results of our meta-regression analysis, which demonstrated that the difference in postoperative functional outcomes between FNS and the other two internal fixation devices diminishes with increasing patient age. This attenuated benefit may be attributed to a reduction in the biomechanical stability provided by FNS in older patients particularly those with osteoporosis, which is even inferior to that of CCS (87). Consequently, the clinical application of FNS in elderly or osteoporotic patients should be cautious until high-quality RCTs are conducted to definitively establish its safety and efficacy in these specific populations. Furthermore, most existing studies are retrospective cohort analyses with relatively short follow-up periods, making it difficult to accurately assess the long-term incidence of complications such as femoral head necrosis and implant failure. Therefore, further high-quality, long-term studies are essential to evaluate the safety and efficacy of FNS and to define its optimal clinical applications.
Given the current evidence, clinical implant selection must be individualized based on their distinct efficacy-safety profiles. The FNS demonstrates advantages in promoting early function and healing, particularly for younger patients or those with displaced fractures where its biomechanical stability is most beneficial. Caution is advised for elderly or osteoporotic patients pending long-term safety data. The DHS provides reliable mechanical stability with a lower risk of implant failure and nonunion compared to CCS, making it a robust choice for unstable fracture patterns. However, its greater risk of femoral head necrosis necessitates careful consideration, especially in subcapital or transcervical fractures. The CCS remains the standard for minimally invasive fixation of non-displaced fractures, particularly when minimizing surgical trauma and blood loss is paramount. These recommendations are tempered by critical evidence gaps that must be addressed in future research: (1) long-term comparative safety, especially regarding subtrochanteric fracture risk with FNS and avascular necrosis across all implants; (2) stratified efficacy data for key but poorly reported modifiers, including precise osteoporosis status, fracture reduction quality, age, and specific displacement patterns; and (3) formal cost-effectiveness analyses. Until such high-quality, granular evidence emerges, a cautious and patient-tailored approach to implant selection, guided by surgeon expertise, remains prudent.
Limitations
This study has several limitations. First, despite a comprehensive literature screening, the final sample size remains limited, particularly regarding high-quality RCTs comparing FNS with the other two interventions. Future analyses should incorporate more robust evidence to enhance the reliability of conclusions. Second, broad inclusion criteria for age and fracture classification (Garden/Pauwels) were employed due to evidence constraints, which inevitably introduced confounding variables. Third, significant heterogeneity in certain outcomes precluded subgroup analysis of clinical modifiers (e.g., age, fracture type, reduction quality) due to insufficiently stratified primary data. Future research should prioritize larger RCTs with refined inclusion criteria and conduct stratified analyses to evaluate procedure efficacy across patient subgroups, thereby facilitating personalized clinical decision-making. Last, given that the CINeMA assessment indicated generally low or very low certainty of evidence for many comparisons, our findings should be interpreted cautiously, underscoring the need for larger, well-designed trials to strengthen the evidence base.
Conclusion
This network meta-analysis demonstrates that FNS shows potential benefits over CCS and DHS in terms of fracture healing time and reduced risk of femoral head necrosis. Regarding HHS, FNS was statistically superior to CCS, but the magnitude of improvement did not reach the minimal clinically important difference, suggesting limited clinical meaningfulness. Several limitations remain, such as uncertain clinical indications, an unclear risk of subtrochanteric fracture, and the absence of high-quality, long-term follow-up studies. Therefore, until more high-level and robust evidence becomes available, clinicians should adopt a selective and judicious approach to its use. Future large-scale, prospective studies are essential to definitively determine its clinical superiority and establish guidelines for its optimal use.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lu H Shen H Zhou S Ni W Jiang D. Biomechanical analysis of the computer-assisted internal fixation of a femoral neck fracture. Genes Dis. (2019) 7:448–55. 10.1016/j.gendis.2019.04.006 32884999 PMC 7452504 · doi ↗ · pubmed ↗
- 2Harris E Clement N Mac Lullich A Farrow L. The impact of an ageing population on future increases in hip fracture burden. Bone Joint J. (2024) 106-B:62–8. 10.1302/0301-620X.106B 1.BJJ-2023-0740.R 1 38160690 · doi ↗ · pubmed ↗
- 3Tian C Shi L Wang J Zhou J Rui C Yin Y Global, regional, and national burdens of hip fractures in elderly individuals from 1990 to 2021 and predictions up to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Arch Gerontol Geriatr. (2025) 133:105832. 10.1016/j.archger.2025.105832 40112671 · doi ↗ · pubmed ↗
- 4Bhandari M Swiontkowski M. Management of acute hip fracture. N Engl J Med. (2017) 377:2053–62. 10.1056/NEJ Mcp 1611090 29166235 · doi ↗ · pubmed ↗
- 5Mukhopadhaya J Bhadani JS. Fixation failure in osteoporotic bone: a review of complications and outcomes. Indian J Orthop. (2025) 59:389–404. 10.1007/s 43465-024-01316-y 40201917 PMC 11973034 · doi ↗ · pubmed ↗
- 6Zelle BA Salazar LM Howard SL Parikh K Pape HC. Surgical treatment options for femoral neck fractures in the elderly. Int Orthop. (2022) 46:1111–22. 10.1007/s 00264-022-05314-3 35187589 · doi ↗ · pubmed ↗
- 7Liang C Cao Y Lin Z Liu G Zhang C Hu Y. Open reduction and internal fixation of irreducible displaced femoral neck fracture with femoral Neck System: a preliminary study. BMC Musculoskelet Disord. (2023) 24:826. 10.1186/s 12891-023-06839-3 37858123 PMC 10585802 · doi ↗ · pubmed ↗
- 8Yang JJ Lin LC Chao KH Chuang SY Wu CC Yeh TT Risk factors for nonunion in patients with intracapsular femoral neck fractures treated with three cannulated screws placed in either a triangle or an inverted triangle configuration. J Bone Joint Surg Am. (2013) 95:61–9. 10.2106/JBJS.K.01081 23283374 · doi ↗ · pubmed ↗