Diagnostic accuracy of teledermatology for skin diseases: a systematic review and meta-analysis
Katalin Martyin, Fanni Adél Meznerics, Laura Anna Bokor, Bence Szabó, Péter Hegyi, Norbert Kiss, András Bánvölgyi

TL;DR
Teledermatology is a reliable method for diagnosing skin diseases and can be a good alternative to in-person visits, especially for skin cancer screening.
Contribution
This study provides a comprehensive meta-analysis of teledermatology's diagnostic accuracy across various skin conditions and platforms.
Findings
Diagnostic concordance was 76% for all skin conditions and 73% for skin cancers.
Dermoscopy significantly improved diagnostic accuracy for skin cancers.
Patient satisfaction with teledermatology was high at 82%.
Abstract
Skin diseases affect nearly one-third of the global population, yet limited access to dermatological care remains an unmet challenge. Teledermatology offers a promising solution, however, concerns about technological and workforce demands have limited its broader adoption. Furthermore, its diagnostic reliability across communication platforms and types, and different skin conditions remains unclear. We aimed to evaluate the diagnostic accuracy of teledermatology compared to in-person consultations. We searched PubMed, Embase, and CENTRAL on November 19, 2023, for observational and experimental studies, without date or language restrictions. Primary outcomes included diagnostic concordance, Cohen’s kappa, sensitivity, specificity, and predictive values; secondary outcomes were diagnostic time, teledermatology provider and patient satisfaction and interrater agreement. A random…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
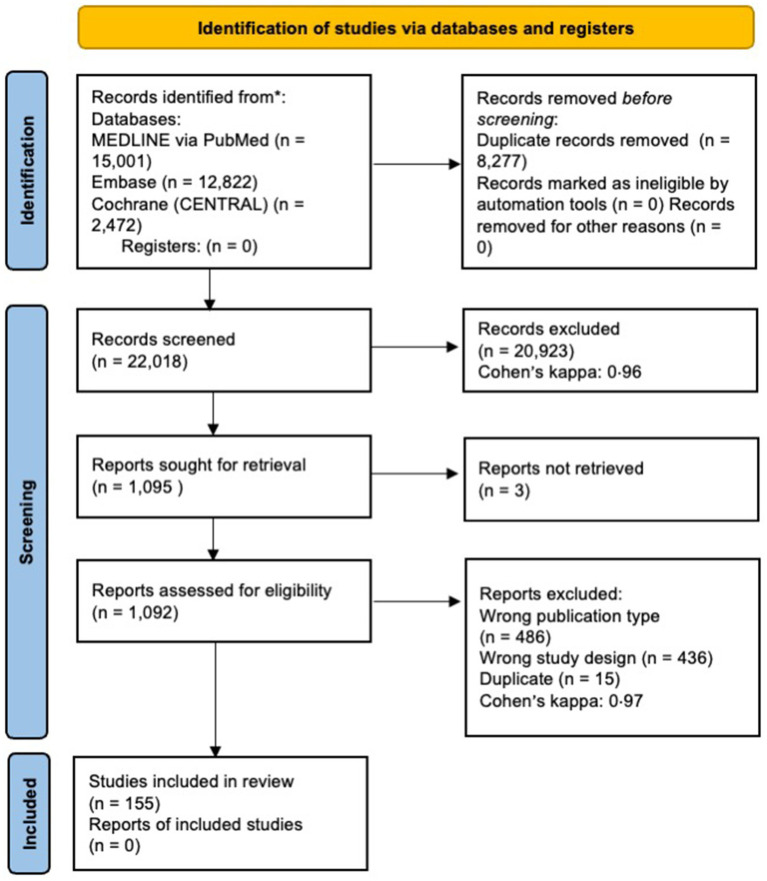 Figure 1
Figure 1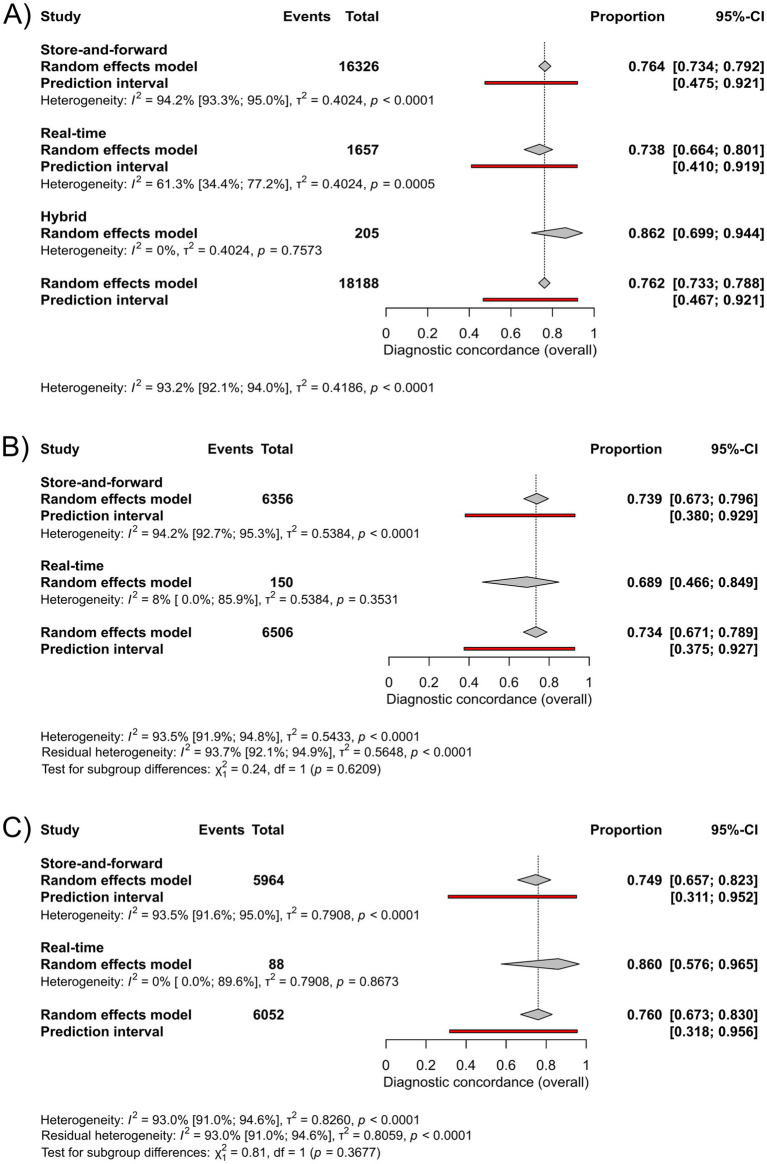 Figure 2
Figure 2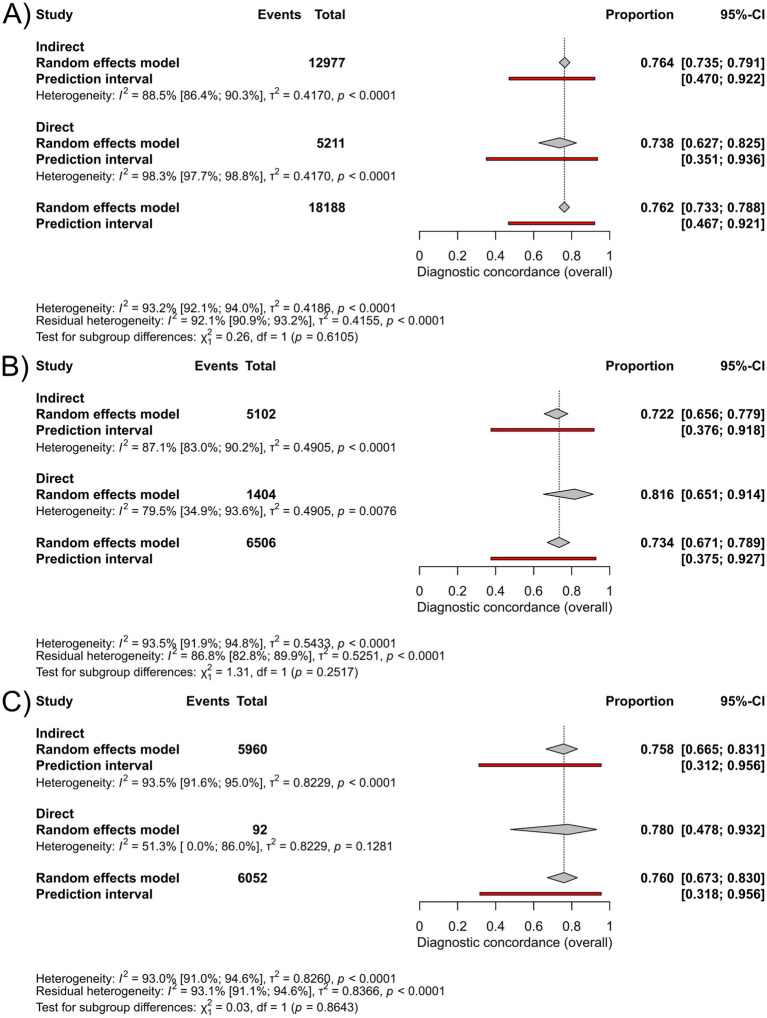 Figure 3
Figure 3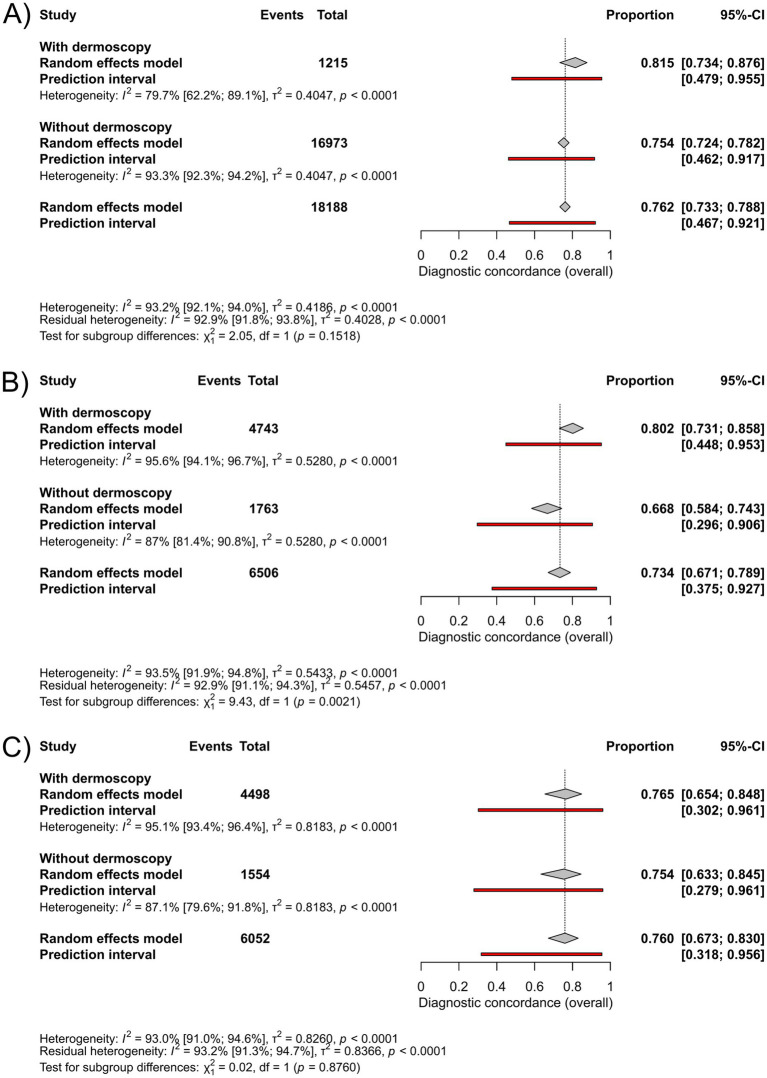 Figure 4
Figure 4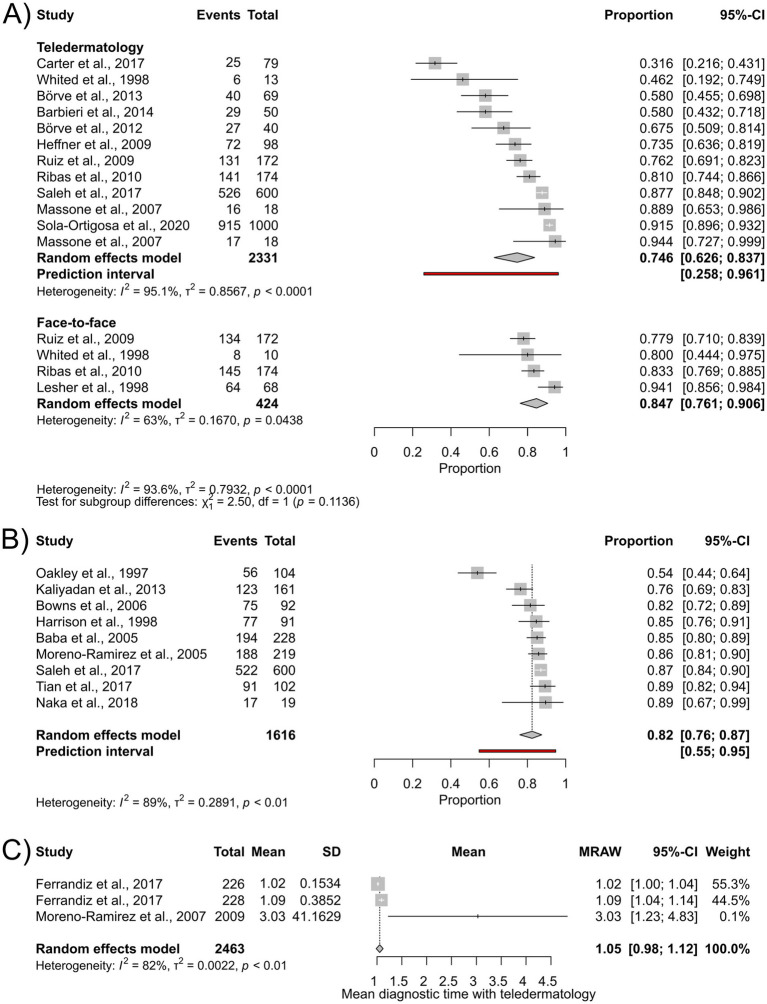 Figure 5
Figure 5| First author and year of publication | Study design | Study period | Country | Population | Communication method | Communication type | Photography device | Use of dermoscopy or other imaging method | Comparator | Reported outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| Articles included in the meta-analysis | ||||||||||
| Altieri, 2017 ( | Observational (prospective) | February 2007–June 2007 | USA | All skin conditions | SAF | ID | DC | no | FTF | DgC, CK |
| Baba, 2005 ( | Observational (prospective) | May 2003–July 2003 | Turkey | All skin conditions | SAF / HY | ID | DC / VC | no | FTF ± HP | DgC, CK, IA-TD, P-SAT |
| Barbieri, 2014 ( | Observational (prospective) | September 1, 2012 - April 31, 2013 | USA | Hospitalized patients, all skin conditions | SAF | ID | SP | no | FTF | DgC, CK, IA-TD |
| Barcaui, 2018 ( | Observational (prospective) | April 2017–June 2017 | USA | Pigmented lesions | SAF | ID | SP | DS | FTF ± HP | DgC, CK |
| Barnard, 2000 ( | Observational (prospective) | NA | USA | All skin conditions | SAF | ID | DC | no | FTF ± HP, HP | DgC, CK |
| Batalla, 2016/1 ( | Observational (retrospective) | May 2011–January 2015 | Spain | All skin conditions | SAF | ID | NA | no | FTF | DgC |
| Batalla, 2016/2 ( | Observational (cross-sectional) | May 2011–April 2014 | Spain | All skin conditions | SAF | ID | NA | no | FTF | DgC |
| Borve, 2012 ( | Observational (prospective) | NA | Sweden | All skin conditions | SAF | ID | SP | no | FTF | DgC, CK, IA-TD |
| Borve, 2013 ( | Observational (prospective) | NA | Sweden | Suspected skin cancer | SAF | ID | SP | DS | HP | DgC, CK, IA-TD |
| Bowns, 2006 ( | RCT | NA | UK | All skin conditions | SAF | ID | DC | no | FTF ± HP | DgC, CK, P-SAT |
| Observational (prospective) | NA | UK | Suspected skin cancer | SAF | ID | DC | DS | FTF | CKa | |
| Braun, 2000 ( | Observational (prospective) | NA | Switzerland | Pigmented lesions suspicious of skin cancer | SAF | ID | DC | DS | HP | DgC, CK |
| Carter, 2017 ( | Observational (prospective cohort, retrospective review) | May 2013–December 2014 | USA | All skin conditions | SAF | ID | DC | no | FTF | DgC, CK, IA-TD |
| Castillo, 2022 ( | Observational (retrospective) | March 2020–December 2020 | USA | All skin conditions | SAF / RT | D | NA | no | HP | DgC, CK |
| Cazzaniga, 2016 ( | Observational (retrospective) | July 1, 2015 -December 31, 2015 | Italy | Suspected skin cancer | SAF | D | NA | no | HP | DgC |
| Chan, 2000 ( | Observational (prospective) | NA | Hong Kong, China | All skin conditions | RT | ID | VC | no | FTF | DgC, CK |
| Chao, 2003 ( | Observational (prospective) | April 2002–August 2002 | Brazil | All skin conditions | SAF | ID | NA | no | FTF | DgC, CK, Time |
| Chen, 2010 ( | Observational (retrospective) | January 1, 2002 - May 1, 2006 | USA | All skin conditions | SAF | ID | NA | no | FTF | CKa |
| Cheung, 2018 ( | Observational (retrospective) | September 2014–March 2016 | UK | Solitary skin lesions | SAF | ID | DC | DS | FTF, HP | CKa |
| Chung, 2007 ( | Observational (prospective) | NA | USA | Hospitalized patients, all skin conditions | SAF | ID | DC | no | FTF | DgC |
| Clarke, 2023 ( | Observational (prospective) | October 2019–February 2020 | USA | All skin conditions | SAF | ID | DC | no | FTF ± HP, HP | DgC, CK, IA-TD |
| Congalton, 2015 ( | Observational (prospective) | April 1, 2012 - March 31. 2014 | New Zealand | Suspected melanoma | SAF | ID | DC | DS | HP | DgC, CK, Sens, Spec, PPV, NPV |
| Coras, 2003 ( | Observational (prospective) | NA | Germany | Pigmented skin lesions | SAF | ID | DC | DS | FTF ± HP | CKa |
| D’elia, 2007 ( | Observational (prospective) | NA | Brazil | All skin conditions | SAF | ID | DC | no | FTF | DgC, IA-TD |
| de Giorgi, 2016 ( | Observational (prospective) | NA | Italy | Pigmented lesions | SAF | ID | DC | DS | HP | DgC, CK |
| Dobry, 2021 ( | Observational (retrospective) | March 2014–December 2017 | USA | All skin conditions | SAF | ID | NA | no | FTF | DgC, CK |
| Du Moulin, 2003 ( | Observational (prospective) | June 2000–May 2001 | The Netherlands | All skin conditions | SAF | ID | DC | no | FTF ± HP | DgC, CK |
| Edison, 2008 ( | Observational (prospective) | NA | USA | All skin conditions | SAF, RT | ID | NA | no | FTF | DgC, CK |
| Eminovic, 2003 ( | Observational (prospective) | NA | The Netherlands | All skin conditions | SAF | ID | NA | no | FTF | CKa, Timea |
| Fabbrocini, 2008 ( | Observational (prospective) | NA | Italy | Melanocytic and non-melanocytic “pink” lesions (poor/absent pigmentation) | SAF | ID | DC | DS | HP | CK, IA-TD |
| Faucon, 2022 ( | Observational (prospective) | November 2016–January 2020 | France | All skin conditions | SAF | ID | NA | no | FTF ± HP | CKa |
| Ferrandiz, 2017 ( | RCT | January 1, 2015 - December 31, 2015 | Spain | Suspected skin cancer | SAF | ID | DC | DS | FTF | DgC, CK, Sens, Spec, PPV, NPV, Time |
| Gabel, 2021 ( | Observational (retrospective) | July 2023–August 2013 | USA | All skin conditions | SAF | ID | DC / tablet | no | FTF | DgC, CK |
| Gao, 2023 ( | Observational (retrospective) | July 1, 2017 - December 31, 2017 | New Zealand | Suspected skin cancer | SAF | ID | NA | DS | HP | DgC, CK, Time |
| Gatica, 2015 ( | Observational (prospective) | NA | Chile | All skin conditions | SAF | ID | DC | no | FTF | DgC |
| Gemelas, 2019 ( | Observational (retrospective) | February 1, 2015 - January 31, 2016 | USA | Suspected or confirmed melanoma | SAF | ID | DC | DS | FTF ± HP | DgC, CK, Sens |
| Gerhardt, 2021 ( | Observational (retrospective) | January 2017–December 2017 | USA | All skin conditions | SAF | D | NA | no | FTF | DgC, CK |
| Giavina-Bianchi, 2020/1 ( | Observational (retrospective) | July 2017–July 2018 | Brazil | Skin neoplasms | SAF | ID | SP | no | FTF, HP | CKa |
| Gilmour, 1998 ( | Observational (prospective, multicenter) | September 1995–September 1996 | UK | All skin conditions | RT | ID | VC | no | FTF | DgC |
| Gyllencreutz, 2017 ( | Observational (retrospective) | NA | Sweden | Suspected skin cancer | SAF | ID | SP / NA | DS / no | FTF ± HP | DgC, CK, IA-TD |
| Gyllencreutz, 2018 ( | Observational (retrospective) | NA | Sweden | All skin conditions | SAF | ID | SP | DS | FTF ± HP | DgC, CK |
| Harrison, 1998 ( | Observational (prospective) | NA | UK | Pigmented lesions | SAF | DC | DC | no | HP | DgC, Sens, P-SAT |
| Heffner, 2009 ( | Observational (prospective) | July 2006–August 2007 | USA | Rashes | SAF | ID | DC | no | FTF | DgC, CK, IA-TD |
| Herrmann, 2005 ( | Observational (prospective) | February 2003–April 2003 | Germany | All skin conditions | SAF | ID | DC | no | FTF | DgC |
| High, 2000 ( | Observational (prospective) | September 4, 1997 - October 15, 1997 | USA | All skin conditions | SAF | ID | DC | no | FTF | DgC, CK |
| Hines, 2021 ( | Observational (retrospective) | January 1, 2015 - December 31, 2019 | USA | Emergency department patients, all skin conditions | SAF | ID | SP | no | FTF | DgC, CK |
| Hue, 2015 ( | Observational (prospective) | January 2015–December 2015 | France | Suspected melanoma | SAF | ID | SP | DS | FTF ± HP | DgC, CK |
| Ilie, 2022 ( | Observational (prospective) | March 2020–April 2020 | UK | All skin conditions | SAF | D | SP | no | FTF | DgC, Time |
| Ishioka, 2009 ( | Observational (retrospective) | 2005–2007 | Brazil | Pigmented skin lesions | SAF | ID | DC | DS | HP | DgC, CK, Sens, Spec, PPV, NPV |
| Fazil Jaber, 2023 ( | Observational (retrospective cross-sectional) | January 1, 2020 - June 30, 2020 | Sweden | Atypical, pigmented lesions | SAF | ID | DC | DS | HP | CKa |
| Janda, 2020 ( | RCT (open-label) | March 6, 2017 - June 7, 2018 | Australia | Suspected skin cancer | SAF | D | SP | DS | FTF | DgC, IA-TD, IA-FTF |
| Jang, 2002 ( | Observational (prospective) | NA | South Korea | All skin conditions | SAF | ID | DC | no | FTF | DgC |
| Jobbagy, 2022 ( | Observational (retrospective) | March 2020–July 2020 | Hungary | All skin conditions | SAF | D | NA | no | FTF ± HP | DgC, CK, Sens, Spec, PPV, NPV |
| Jolliffe, 2001 ( | Observational (prospective) | NA | UK | Pigmented skin lesions | SAF | ID | VC | no | HP | DgC |
| Jones, 2021 ( | Observational (retrospective) | July 1, 2016 - December 31, 2020 | New Zealand | Suspected skin cancer | SAF | ID | SP | DS | HP | DgC |
| Josendal, 1991 ( | Observational (prospective) | NA | Norway | All skin conditions | RT | ID | DC | no | FTF | DgC, CK |
| Kaliyadan, 2013 ( | Observational (prospective) | NA | Saudi Arabia | All skin conditions | SAF | ID | SP | no | FTF | DgC, CK, P-SAT, TD-SAT |
| Keller, 2020 ( | Observational (prospective) | November 2017–August 2018 | USA | All skin conditions | SAF | ID | SP / tablet | no | FTF | DgC, CK |
| Koop, 2023 ( | Observational (retrospective) | October 16, 2017 - August 30, 2019 | Estonia | Suspected melanoma | SAF | ID | NA | DS | HP | DgC, CK, Sens, Spec, PPV, NPV |
| Kravets, 2018 ( | Observational (prospective) | 2013–2016 | Ukraine | Skin neoplasms | SAF | ID | DC | DS | HP, FTF | DgC, CK |
| Kroemer, 2011 ( | Observational (prospective) | NA | Austria | Skin neoplasms | SAF | ID | SP | DS | FTF ± HP | CKa |
| Krupinski, 1999 ( | Observational (prospective) | NA | USA | All skin conditions | SAF | ID | DC | no | FTF, HP | DgC, CK, Time |
| Kvedar, 1997 ( | Observational (prospective) | March 1995–April 1995 | USA | All skin conditions | SAF | ID | DC | no | FTF | DgC, CK |
| Lamel, 2012 ( | Observational (prospective) | NA | USA | Skin cancer screening | SAF | ID | SP | no | FTF | DgC, CK |
| Lasierra, 2012 ( | Observational (prospective) | April 2008–July 2010 | Spain | All skin conditions | SAF | ID | DC | no | FTF | DgC, Time |
| Lepe, 2004 ( | Observational (prospective) | NA | Mexico | All skin conditions | SAF | ID | VC | no | FTF | DgC, CK |
| Lesher, 1998 ( | Observational (prospective) | NA | USA | All skin conditions | RT | ID | VC | no | FTF | DgC, CK, IA-FTF |
| Lim, 2001 ( | Observational (prospective) | NA | Australia | All skin conditions | SAF | ID | DC | no | FTF | DgC, CK |
| Loane, 1997 ( | Observational (prospective) | NA | UK | All skin conditions | RT | ID | VC | no | FTF | DgC |
| Loane, 1998 ( | Observational (prospective) | NA | UK | All skin conditions | RT | ID | VC | no | FTF | DgC |
| Lowitt, 1998 ( | Observational (prospective) | NA | USA | All skin conditions | RT | ID | VC | no | FTF | DgC, CK, Sens, Spec TD-SAT |
| Lyon, 1997 ( | Observational (prospective) | NA | UK | All skin conditions | SAF | ID | DC | no | FTF, HP | DgC, CK |
| Maclellan, 2021 ( | Observational (prospective) | NA | Canada | Pigmented lesions | SAF | ID | DC | DS | HP | DgC, CK, Sens, Spec |
| Mahendran, 2005 ( | Observational (prospective) | NA | UK | Suspected skin cancer | SAF | ID | DC | no | FTF | DgC, CK |
| Mallett, 2003 ( | Observational (retrospective) | October 1998–January 2003 | UK | All skin conditions | SAF | ID | DC | no | FTF | DgC, CK |
| Manahan, 2015 ( | Observational (prospective) | May 2013–November 2013 | Australia | Pigmented lesions | SAF | D | SP | DS | FTF | CKa |
| Marchell, 2017 ( | Quasi-randomized controlled trial | NA | USA | All skin conditions | SAF | ID | DC | no | FTF | DgC, CK |
| Markun, 2017 ( | Observational (prospective) | May 2013–June 2016 | Switzerland | Suspected skin cancer | SAF | ID | SP | DS | FTF ± HP | CKa |
| Massone, 2007 ( | Observational (prospective) | NA | Austria | Pigmented lesions | SAF | ID | DC | DS | FTF | CK, IA-TD |
| Massone, 2013 ( | Observational (prospective) | February 2008–February 2010 | Austria | Suspected skin cancer | SAF | ID | DC | DS | FTF ± HP | DgC, CK, Sens, Spec |
| Montejano, 2022 ( | Observational (retrospective) | September 2018–March 2019 | USA | All skin conditions | SAF | ID | NA | DS | HP | DgC, CK |
| Moreno-Ramirez, 2005 ( | Observational (prospective) | January 2004–April 2004 | Spain | Pigmented lesions | SAF | ID | DC | no | FTF | DgC, CK, P-SAT |
| Moreno-Ramirez, 2006 ( | Observational (prospective pilot) | September 2004–January 2005 | Spain | Pigmented lesions | SAF | ID | DC | DS | HP | CK, Sens, Spec |
| Moreno-Ramirez, 2007 ( | Observational (longitudinal) | March 2004–July 2005 | Spain | Suspected skin cancer | SAF | ID | DC | no | FTF ± HP | DgC, CK, Sens, Spec, PPV, NPV |
| Muir, 2011 ( | Observational (prospective pilot) | August 2008–August 2009 | Australia | Emergency department patients, acute/subacute skin conditions | SAF | ID | DC | no | FTF | CK, Time |
| Naka, 2018 ( | Observational (retrospective) | June 2014–November 2015 | USA | All skin conditions | SAF | ID | DC | DS | FTF ± HP | CK, P-SAT |
| Nami, 2015 ( | Observational (prospective) | October 2011–October 2012 | Italy, Austria | All skin conditions, except pigmented lesions | SAF | ID | SP | no | FTF | CK, Time |
| Ng, 2011 ( | Observational (retrospective) | October 2007–April 2008 | UK | Suspected skin cancer | SAF | ID | NA | no | FTF ± HP | DgC, CK, PPV, NPV |
| Nordal, 2001 ( | Observational (prospective) | 1994–1995 | Norway | All skin conditions | RT | ID | DC | no | FTF | CK |
| Norton, 1997 ( | Observational (prospective) | NA | USA | All skin conditions | RT | ID | NA | no | HP | DgC, CK |
| O’Connor, 2017 ( | RCT, observational (prospective) | March 1, 2016 - September 30, 2016 | USA | All skin conditions | SAF | D | SP | no | FTF | CK |
| Oakley, 1997 ( | Observational (prospective) | NA | New Zealand | All skin conditions | RT | ID | DC | no | FTF | DgC, P-SAT |
| Oakley, 1998 ( | Observational (prospective) | NA | New Zealand | All skin conditions | RT | ID | DC | no | FTF, HP | DgC, CK |
| Oakley, 2006 ( | Observational (prospective) | NA | New Zealand | All skin conditions | SAF | ID | DC | no | HP | CK |
| Okita, 2016 ( | Observational (prospective) | January 2015–April 2015 | Brazil | Hospitalized patients, all skin conditions | SAF | ID | SP | no | FTF | CK |
| Oztas, 2004 ( | Observational (prospective) | NA | Turkey | All skin conditions | SAF | ID | DC | no | FTF | CK |
| Pak, 2003 ( | Observational (prospective) | October 1, 1999 - January 30, 2000 | USA | All skin conditions | SAF | ID | DC | no | FTF | CK |
| Paradela-De-La-Morena, 2015 ( | Observational (retrospective) | 2011–2013 | Spain | All skin conditions | SAF | ID | DC | no | FTF | CK |
| Phillips, 1997 ( | Observational (prospective) | NA | USA | All skin conditions | RT | ID | DC | DS | FTF | CK |
| Phillips, 1998 ( | Observational (retrospective) | NA | USA | Skin cancer screening | RT | ID | DC | DS | FTF | CK |
| Preclaro, 2022 ( | Observational (cross sectional) | August 1, 2018 - September 30, 2018 | Philippines | All skin conditions | SAF | ID | DC | no | FTF, HP | CK, IA-TD |
| Rajagopal, 2009 ( | Observational (retrospective) | March 6, 2009 - March 8, 2009 | India | All skin conditions | SAF, RT | ID | VC | n.a. | FTF | CK |
| Rashid, 2003 ( | Observational (prospective) | NA | Pakistan | All skin conditions | SAF | ID | DC | no | FTF | DgC, CK |
| Ribas, 2010 ( | Observational (cross sectional) | NA | Brazil | All skin conditions | SAF | ID | DC | no | FTF | DgC, CK, IA-TD, IA-FTF |
| Rios, 2012 ( | Quasi-experimental, randomized, open-label | April 1, 2009 - April 30, 2009 | Spain | All skin conditions | SAF | ID | DC | no | FTF ± HP, FTF, HP | DgC |
| Romero, 2006 ( | RCT | June 2004–December 2005 | Spain | All skin conditions | SAF | ID | DC | no | FTF | DgC |
| Romero, 2010 ( | Observational (prospective pilot) | August 2003–February 2004 | Spain | All skin conditions | SAF /HY | ID | DC | no | FTF | DgC |
| Romero Aguilera, 2014 ( | RCT | June 2004–December 2005 | Spain | All skin conditions | SAF / HY | ID | DC | no | FTF | DgC |
| Rubegni, 2011 ( | Observational (prospective) | January 2009–December 2009 | Italy | All skin conditions | SAF | ID | DC | DS | FTF | DgC, CK |
| Ruiz, 2009 ( | Observational (prospective) | NA | Colombia | All skin conditions | SAF | ID | DC | no | FTF | DgC, IA-TD, IA-FTF |
| Saleh, 2017 ( | Observational (prospective) | February 2015–June 2015 | Egypt | All skin conditions | SAF | ID | DC | no | FTF | DgC, CK, IA-TD, P-SAT |
| Santosa, 2023 ( | Observational (retrospective) | June 2015–December 2015 | Singapore | Emergency department patients, all skin conditions | SAF | ID | DC | no | FTF | DgC |
| Schiener, 2001 ( | Observational (prospective pilot) | NA | Germany | All skin conditions | SAF | ID | DC | no | FTF | DgC |
| Senel, 2014 ( | Observational (retrospective) | NA | Turkey | benign and malignant skin lesions | SAF | ID | DC | DS | FTF ± HP, HP | DgC, CK |
| Shin, 2014 ( | Observational (prospective) | NA | South Korea | All skin conditions (military setting) | SAF | ID | SP | no | FTF | DgC, CK |
| Silva, 2009 ( | Observational (prospective) | January 2007–April 2007 | Brazil | All skin conditions | SAF | ID | DC | no | FTF | DgC |
| Silveira, 2019 ( | Observational (prospective) | NA | Brazil | Suspected skin cancer | SAF | ID | DP | no | FTF | CKa |
| Sola-Ortigosa, 2020 ( | Observational (prospective) | February 2016–March 2017 | Spain | Suspected actinic keratosis | SAF | ID | DC | DS | FTF ± HP | DgC, PPV, NPV, IA-TD |
| Taberner Ferrer, 2009 ( | Observational (prospective) | December 15, 2005 - July 4, 2008 | Spain | All skin conditions | SAF | ID | DC | DS | FTF ± HP | DgC |
| Tait, 1999 ( | Observational (prospective) | NA | Australia | All skin conditions | SAF | ID | DC | no | FTF | DgC |
| Tan, 2010 ( | Observational (prospective) | March 2008–September 2008 | New Zealand | All skin conditions | SAF | ID | DC | DS | FTF ± HP, FTF, HP | DgC, CK, Sens, Spec |
| Taslidere, 2022 ( | Observational (prospective) | September 1, 2020 - December 1, 2020 | Turkey | All skin conditions | SAF | ID | SP | no | FTF | DgC |
| Taslidere, 2023 ( | Observational (prospective) | April 15, 2022 - November 1, 2022 | Turkey | All skin conditions | SAF | ID | SP | no | FTF | DgC, CK |
| Taylor, 2001 ( | Observational (prospective) | February 4, 1997 - May 2, 1997 | UK | All skin conditions | SAF | ID | VC | no | FTF | DgC |
| Teague, 2022 ( | Observational (retrospective) | January 1, 2012 - December 31, 2016 | New Zealand | Suspected melanoma | SAF | ID | DC | DS | HP | DgC, CK, PPV |
| Teoh, 2022 ( | Observational (retrospective) | January 1, 2010 - May 31, 2019 | New Zealand | Suspected skin cancer | SAF | ID | DC | DS | HP | DgC, Sens |
| Tian, 2017 ( | Observational (prospective) | NA | Singapore | Esthetic conditions | SAF | D | SP | no | FTF | DgC, P-SAT |
| Tucker, 2005 ( | Observational (retrospective) | NA | UK | All skin conditions | SAF | ID | DC | no | FTF | DgC, CK |
| Vano-Galvan, 2011 ( | Observational (cross sectional, repeated measures study) | January 2009–April 2009 | Spain | All skin conditions | SAF | ID | DC | no | FTF | DgC, CK, Time |
| Villa, 2020 ( | Observational (prospective) | March 2017–July 2017 | Germany | Emergency department patients, all skin conditions | SAF | ID | tablet | no | FTF | DgC, CK |
| Wang, 2017 ( | Observational (retrospective) | July 1, 2009 - December 31, 2011 | USA | Suspected melanoma | SAF | ID | NA | DS | HP | DgC, CK |
| Warshaw, 2009/1 ( | Observational (cross sectional, repeated measures study) | November 2002–August 2005 | USA | Pigmented neoplasms | SAF | ID | DC | DS | HP | DgC, CK |
| Warshaw, 2015 ( | Observational (cross sectional, repeated measures study) | NA | USA | Skin neoplasms | SAF | ID | DC | DS | FTF ± HP, FTF, HP | DgC, CK |
| Weingast, 2013 ( | Observational (prospective) | NA | Austria | All skin conditions | SAF | D | SP | no | FTF | DgC, CK |
| Whited, 1998 ( | Observational (prospective) | NA | USA | Suspected skin cancer | SAF | ID | DC | no | FTF | DgC, CK, IA-TD, IA-FTF |
| Whited, 1999 ( | Observational (prospective) | NA | USA | All skin conditions | SAF | ID | DC | no | FTF | DgC, CK, IA-TD, IA-FTF |
| Yamazaki, 2003 ( | Observational (prospective) | September 1999–August 2002 | Japan | All skin conditions | RT | ID | SP | DS | FTF | DgC, CK |
| Zanini, 2013 ( | Observational (prospective) | NA | Portugal | All skin conditions | SAF | ID | DC | no | FTF | DgC |
| Zelickson, 1997 ( | Observational (prospective) | NA | USA | All skin conditions (nursing home patients) | SAF | ID | VC | no | FTF | DgC |
| Zink, 2017/1 ( | Observational (prospective) | NA | Germany | All skin conditions | SAF | ID | SP | no | FTF | DgC |
| Zink, 2017/2 ( | Observational (prospective) | NA | Germany | All skin conditions (in need of dermoscopic evaluation) | SAF | ID | SP | DS | FTF, HP | DgC |
| Articles only included in the systematic review | ||||||||||
| Alfageme, 2021 ( | Observational (prospective, multicenter) | June 2018–January 2019 | Spain | Palpable nodular skin lesions | SAF | ID | US | US | FTF | DgCa, Sensa, Speca, PPVa, NPVa |
| Creadore, 2023 ( | Observational (cross sectional) | NA | USA | Cellulitis/pseudocellulitis | SAF | ID | NA | Thermal imaging | FTF | DgC |
| Giavina-Bianchi, 2020/2 ( | Observational (retrospective) | July 2017–July 2018 | Brazil | Atopic dermatitis | SAF | ID | SP | no | FTF | CKa |
| Giavina-Bianchi, 2020/3 ( | Observational (retrospective) | July 2017–July 2018 | Brazil | Inflammatory dermatoses | SAF | ID | SP | no | FTF | CKa |
| Lozzi, 2007 ( | Observational (prospective) | September 2004–February 2005 | Italy, Austria | Neoplastic and inflammatory dermatoses | SAF | ID | DC | no | HP | DgC |
| Ludzik, 2016/1 ( | Observational (retrospective) | January 2015–May 2015 | Poland, Italy | Suspected melanoma | SAF | ID | NA | DS, RCM | HP | DgC, Sens, Spec |
| Ludzik, 2016/2 ( | Observational (retrospective) | January 2009–January 2012 | Italy | Pink cutaneous lesions | SAF | ID | NA | DS, RCM | HP | DgC, Sens, Spec |
| Rao, 2013 ( | Observational (retrospective) | June 2010–September 2011 | USA | Lesions that had been selected for removal for either cosmetic or medical reasons | SAF | ID | NA | DS, RCM | HP | DgC, Sens, Spec |
| Senel, 2013 ( | Observational (prospective) | April 2009–September 2009 | Turkey | Non-melanocytic skin tumors | SAF | ID | DC | DS | FTF ± HP | DgC, CK |
| Shah, 2023 ( | Observational (retrospective) | April 2020–October 2021 | USA | Dermatitis | SAF | D | NA | no | FTF | DgC, CK |
| Tognetti, 2021 ( | Observational (retrospective) | January 2018–March 2019 | Italy | Atypical melanocytic lesions | SAF | ID | NA | DS | HP | AUROC |
| Trindade, 2008 ( | Observational (prospective) | August 2005–April 2006 | Brazil | Suspicious for leprosy | SAF | ID | DC | no | FTF | DgC, Sens, Spec |
| Tugrul, 2022 ( | Observational (prospective) | April 2008–March 2019 | Turkey | Non-melanocytic skin lesions | SAF | ID | SP | DS | FTF | DgC |
| Van der Heijden, 2013 ( | Observational (prospective) | February 2010–May 2011 | The Netherlands | Pigmented lesions | SAF | ID | DC | DS | FTF ± HP | CK, IA-TD |
| Warshaw, 2009/2 ( | Observational (cross sectional) | NA | USA | Non-pigmented neoplasms | SAF | ID | DC | DS | HP | DgC |
| Witkowski, 2017 ( | Observational (retrospective) | January 2010–August 2011 | Italy, Poland, Spain | Suspected melanoma | SAF | ID | NA | DS, RCM | HP | Sens, Spec |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous Melanoma Detection and Management · Nonmelanoma Skin Cancer Studies · Psoriasis: Treatment and Pathogenesis
Introduction
1
Skin diseases are a major public health concern, affecting nearly one-third of the world population, and ranking among the leading causes of nonfatal burden globally (1, 2). Moreover, the incidence of skin diseases is rising, with a total demand projected to rise by 12.45% from 2021 to 2036 (3). However, the growing demand for dermatological care remains largely unmet worldwide, with some countries having less than one dermatologist per one million people (4). Although this issue weighs the heaviest on low-income countries, middle- and high-income countries also experience a maldistribution of dermatologists (5). Recognizing this gap, the World Health Organization (WHO) urged to integrate telemedicine platforms into clinical practice, especially in remote areas (6).
Teledermatology provides dermatological care between two distant locations through telecommunication technologies (7). It may offer a solution by reducing waiting times and making patient care more accessible in rural and low-resource areas (8). Although it has been shown to be effective during the COVID-19 pandemic in reducing the need for in-person visits, there is a lack of evidence for its applicability in daily practice (9).
Teledermatology can be categorized by communication platform and type. According to communication platform, there are three main forms: store-and-forward, real-time, and hybrid methods (10). In the case of the store-and-forward method, the connection between the patient and healthcare provider is separated in both time and space. Clinical images may also be complemented by historical and/or clinical information (10). The real-time method uses video conferencing technology for live interactions, while the hybrid method combines the features of both approaches (10). The two types of communication are direct and indirect forms. In the direct form, the patient contacts the dermatologist directly, while in indirect teledermatology, the interaction is mediated by the referring healthcare provider, usually a general practitioner (11). The indirect form can be enhanced by the use of dermoscopy (12).
In light of these factors, teledermatology stands out as a promising tool for facilitating timely and affordable dermatological care worldwide. However, its wider implementation has been constrained by technological and human resource limitations. In addition, its diagnostic reliability across communication platforms and types, as well as its efficacy for evaluating different skin conditions remains uncertain (13). We aimed to comprehensively evaluate the diagnostic accuracy of teledermatology compared to in-person dermatological examinations.
Materials and methods
2
Search strategy and selection criteria
2.1
We report our systematic review and meta-analysis following the recommendations of the PRISMA 2020 guidelines and the Cochrane Handbook (Version 6.4) (14, 15). The review protocol was registered in PROSPERO [registration number: CRD42023484476, available at https://www.crd.york.ac.uk/PROSPERO/view/CRD42023484476].
A systematic search was conducted in three databases: MEDLINE (via PubMed), Embase, and Cochrane Central Register of Controlled Trials (CENTRAL) on November 19, 2023, without any filters or language restrictions. The detailed search strategy is available in the Supplementary material.
Peer-reviewed observational (cohort, cross-sectional, and case–control) studies and experimental studies (randomized clinical trials, and non-randomized controlled trials) were included if they met the following Population-Intervention-Comparator-Outcome (PICO) framework: (P) patients with dermatological diseases, (I) diagnosis made via teledermatology, (C) diagnosis made during face-to-face visit or histopathology, (O) primary: diagnostic concordance, Cohen’s kappa, sensitivity, specificity, and predictive values, secondary: diagnostic time, teledermatology provider and patient satisfaction, interrater agreement between teledermatology providers, and between face-to-face dermatologists.
Articles were included if both teledermatology and face-to-face evaluation were performed by a dermatology specialist or resident.
After a reference library was created, Endnote 20 (Clarivate Analytics, Philadelphia, PA, USA) was used for automatic and manual removal of duplicates. Title and abstract selection, as well as full-text selection were performed using the Rayyan Systems (Qatar Computing Research Institute, Cambridge, MA, USA/ Doha, Qatar) software. The selection was independently performed by two reviewers (KM, LAB), and a third reviewer (FAM) resolved disagreements.
Two authors (KM, LAB) independently extracted data from eligible articles into a standardized data collection table. The following data were collected: title, first author, year of publication, country, study type, study period, study setting, patient characteristics, intervention details, comparator, primary and secondary outcomes. If available, both summary estimates and individual patient-level data were extracted. Disagreements were resolved by a third reviewer (FAM).
Data analysis
2.2
A random-effects model was used to pool effect sizes, as considerable between-study heterogeneity was assumed in all cases.
Proportions were considered as an effect size measure with 95% confidence intervals (CI), for the following outcomes: diagnostic concordance, Cohen’s kappa, sensitivity, specificity, predictive values, interrater agreement, and satisfaction. The number of all patients and the number of matching diagnoses were extracted to calculate study proportions and pooled proportions. If raw numbers were not reported, the point and interval estimates (95% CI, standard error) of the above-mentioned two ratios were extracted. A random intercept logistic regression model was used for pooling outcomes (16, 17). The maximum likelihood method was used to estimate the heterogeneity variance measure (τ^2^). The Clopper-Pearson method was used for the calculation of CIs of proportions of the individual studies (18). For the continuous outcome (diagnostic time), the difference between the mean (MD) was used for the effect size measure with a 95% CI.
Articles were grouped by disease category. Multilevel modeling with study ID as a random effect was used to account for repeated entries from the same article within analyses. Studies were classified and analyzed separately according to whether undiagnosed cases were treated as diagnostic disagreements or excluded from the analysis. Studies reporting both approaches were included in both analyses.
Subgroup analyses were performed in each disease group based on communication platform (store-and-forward, real-time, hybrid), communication type (direct, indirect), the use of dermoscopy, photography device (smartphone or tablet, photo or video camera), training for image acquisition, and comparator (face-to-face examination, histopathology).
The results of all analyses were visualized in forest plots. To perform all calculations, we used the R version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria) software, supplemented with the meta and metafor packages.
I^2^ and χ^2^ tests were used to assess the statistical heterogeneity, with a p-value <0.1 as a threshold for statistically significant difference. Egger’s test and funnel plots were applied to report and visualize publication bias if there were at least ten studies involved in the analysis (19).
The risk of bias was independently assessed by two reviewers (KM, LAB), using the QUADAS-2 tool (University of Bristol, Bristol, UK). Disagreements were resolved by a third reviewer (FAM).
Results
3
Study selection
3.1
A total of 30,412 records were identified through the systematic search. After duplicate removal and selection, 155 articles were included (20–175), most of which were observational studies. Quantitative analysis was performed on 139 studies (20–159), while 16 articles were only qualitatively assessed (160–175). The flowchart of the selection and screening process is summarized in Figure 1.
PRISMA 2020 flow diagram of the selection and screening process.
Characteristics of studies
3.2
The main characteristics of the included articles are presented in Table 1. Additional study and patient characteristics are shown in Supplementary Table S2.
Quantitative analysis
3.3
The included articles were assigned to three main groups based on disease categories. The articles on all types of skin conditions, without any major exclusions, were pooled together in the group “all skin conditions”. Articles on all types of skin malignancies, including actinic keratosis, squamous cell carcinoma, basal cell carcinoma, and melanoma, were pooled together in the “skin cancer” group. Articles on benign and malignant melanocytic lesions, including nevus, lentigo maligna, and melanoma, formed the group “pigmented lesions”. Within these disease categories, subgroup analyses were conducted based on communication platform, use of dermoscopic images, consultation type, tool used to acquire images, training received for image acquisition, and comparator.
Primary outcomes
3.3.1
All results presented refer to overall results, i.e., undiagnosed cases were included in the analysis. For results calculated excluding undiagnosed cases, see Supplementary Figures S1–S42.
Diagnostic concordance, Cohen’s kappa
3.3.1.1
In the group “all skin conditions”, subgroup analysis by communication platform showed a pooled diagnostic concordance of 76% (95%-CI: 73–79%; I^2^ = 94%) for store-and-forward (n = 16,326), and 73% (95%-CI: 66–80%; I^2^ = 61%) for the real-time method (n = 1,657) (Figure 2A). In the group “skin cancer”, pooled diagnostic concordance was found to be 74% (95%-CI: 67–79.6%; I2 = 94%) for store-and-forward (n = 6,356), and 69% (95%-CI: 47–85%; I^2^ = 8%) for real-time method (n = 150) (Figure 2B). For “pigmented lesions” the store-and-forward method (n = 5,964) showed a pooled diagnostic concordance of 75% (95%-CI, 66–82%; I^2^ = 94%), whereas for the real-time method (n = 88), the pooled diagnostic concordance was 86% (95%-CI, 58–97%; I^2^ = 0%) (Figure 2C). There was no statistically significant difference between communication platforms in any disease category. Data on the hybrid method were not sufficient for pooling. Forest plots displaying individual studies can be seen in Supplementary Figures S43–S45.
Forest plots for subgrouping based on communication platform: (A) Forest plot comparing diagnostic concordance between teledermatological and in-person dermatological diagnosis in the group “all skin conditions”, (B) Forest plot comparing diagnostic concordance between teledermatological and in-person dermatological diagnosis in the group “skin cancer”, (C) Forest plot comparing diagnostic concordance between teledermatological and in-person dermatological diagnosis in the group “pigmented lesions”.
Subgroup analyses based on communication type showed a pooled diagnostic concordance of 76% (95%-CI: 63–83%; I^2^ = 98%), for direct (n = 5,211), and 76% (95%-CI: 74–79%; I^2^ = 89%), for indirect (n = 12,977) types in the group “all skin conditions” (Figure 3A). In the group “skin cancer,” pooled diagnostic concordance was found to be 82% (95%-CI: 65–91%; I^2^ = 80%), for direct (n = 1,404), compared to 72% (95%-CI: 66–78%; I^2^ = 87%), for indirect (n = 5,102) type (Figure 3B). The pooled diagnostic concordance in the group “pigmented lesions” was 78% (95%-CI: 48–93%; I^2^ = 51%), for the direct (n = 92), and 76% (95%-CI: 67–83%; I^2^ = 93%), for the indirect (n = 5,960) method (Figure 3C). No statistically significant difference was found in any disease category. Forest plots with individual studies listed can be seen in Supplementary Figures S46–S48.
Forest plots for subgrouping based on communication type [direct/indirect]: (A) Forest plot comparing diagnostic concordance between teledermatological and in-person dermatological diagnosis in the group “all skin conditions”, (B) Forest plot comparing diagnostic concordance between teledermatological and in-person dermatological diagnosis in the group “skin cancer” group, (C) Forest plot comparing the diagnostic concordance between teledermatological and in-person dermatological diagnosis in the group “pigmented lesions”.
Subgroup analyses based on the use of dermoscopy in the group “all skin conditions” showed a pooled diagnostic concordance of 82% (95%-CI: 73–88%; I^2^ = 80%) with dermoscopy (n = 1,215), compared to 75% (95%-CI: 72–78%; I^2^ = 93%) without dermoscopy (n = 16,973), the difference was not statistically significant (Figure 4A). In the group “skin cancer,” the use of dermoscopy (n = 4,743) yielded a significantly higher concordance of 80% (95%-CI: 73–86%; I^2^ = 96%), compared to 67% (95%-CI: 58–74%; I^2^ = 87%) without dermoscopy (n = 1,763) (Figure 4B). In the group “pigmented lesions” the use of dermoscopy (n = 4,498) resulted in a pooled diagnostic concordance of 77% (95%-CI: 65–85%; I^2^ = 95%), compared to 75% (95%-CI: 63–85%; I^2^ = 87%) in cases assessed without dermoscopy (n = 1,554), a difference that was not statistically significant (Figure 4C). For forest plots showing individual studies, see Supplementary Figures S49–S52.
Forest plots for subgrouping based on the use of dermoscopy: (A) Forest plot comparing the diagnostic concordance between teledermatological and in-person dermatological diagnosis in the group “all skin conditions”, (B) Forest plot comparing diagnostic concordance between teledermatological and in-person dermatological diagnosis in the group “skin cancer”, (C) Forest plot comparing diagnostic concordance between teledermatological and in-person dermatological diagnosis in the group “pigmented lesions”.
No statistically significant subgroup differences were identified based on the photography device (Supplementary Figures S52-S54), or the training received for the image acquisition in any patient population (Supplementary Figures S55–S57). Subgroup differences based on comparator yielded inconclusive results (Supplementary Figures S58–S60).
Results for kappa concordance are presented in Supplementary Figures S61–S79.
Sensitivity, specificity
3.3.1.2
Sensitivity and specificity of teledermatology were found to be 94% (95%-CI: 87–100%; I^2^ = 92%) and 82% (95%-CI: 65–99%; I^2^ = 98%) in the group “skin cancer,” respectively. In the group “pigmented lesions,” sensitivity and specificity were found to be 87% (95%-CI: 80–93%; I^2^ = 0%) and 84% (95%-CI: 74–95%; I^2^ = 87%), respectively (Supplementary Figures S80–S83).
Secondary outcomes
3.3.2
Secondary outcomes were assessed by pooling data across all disease categories. Interrater agreement was 75% (95%-CI: 63–84%; I^2^ = 95%) for teledermatology evaluations (n = 2,331), and 85% (95%-CI: 76–91%; I^2^ = 63%) for face-to-face assessments (n = 424), with no statistically significant difference between the groups (Figure 5A). Results for kappa concordance are presented in Supplementary Figure S83.
Forest plots for secondary outcomes: (A) Forest plot for comparing interrater agreement between teledermatological and in-person dermatological diagnosis; (B) forest plot for patient satisfaction; (C) forest plot for mean diagnostic time with teledermatology.
The pooled proportion of patients satisfied with teledermatological care was 82% (95%-CI: 76–87%; I^2^ = 89%) (n = 1,616)(Figure 5B). There were insufficient data to perform a statistical analysis of teledermatology provider satisfaction (Supplementary Table S3).
The mean diagnostic time during teledermatology consultations was 1.05 min (95%-CI: 0.98–1.12; I^2^ = 82.2%) (n = 2,463) (Figure 5C); data were not sufficient on the duration of face-to-face consultations to perform statistical analysis (Supplementary Table S4).
Qualitative analysis
3.4
For results on only qualitatively assessed studies and outcomes not possible to pool, see Supplementary Tables S3-S9.
Risk of bias assessment and publication bias
3.5
Most studies demonstrated moderate or serious risk of bias in certain domains, possibly due to their observational design (Supplementary Table S10; Supplementary Figure S85). Funnel plots of the main analyses evaluating publication bias are shown in Supplementary Figures S86–S96.
Discussion
4
The findings of our systematic review and meta-analysis provide the most comprehensive overview to date, with 155 studies comparing the diagnostic concordance of teledermatology and in-person dermatological examination in the diagnosis of skin diseases.
Our findings support that teledermatology provides diagnostic accuracy comparable to in-person care, with high concordance across all disease categories. This aligns with previous analyses by Kanthraj et al. (176) and Bourkas et al. (177), which also reported strong agreement between teledermatology and face-to-face diagnoses. In contrast, Bastola et al. (178) found teledermatology to be less reliable than in-person assessment, likely due to the small number of included studies and strict inclusion criteria. Our study applied a broader inclusion criteria; however, the analysis was restricted to studies in which diagnoses were established by dermatologists, thereby providing a clinically more relevant assessment (177). Moreover, our study uniquely highlights that the direct store-and-forward method, beside requiring fewer resources, achieves diagnostic performance on par with more complex modalities, indicating scalability across varying resource levels.
Our analyses found no significant differences in diagnostic concordance based on the communication platforms and types, regardless of disease category. This suggests that direct store-and-forward, the most convenient approach, is as effective as more complex and resource-heavy methods. Store-and-forward was the most commonly used platform in the included studies, likely due to its cost-effectiveness and minimal resource requirements (10). Previous studies have already urged its implementation in daily practice in resource-poor areas (176). The indirect method was used by most of the included studies, suggesting the low number and inaccessibility of direct teledermatology platforms. Our results suggest that the direct, patient-initiated method is reliable, and feasible for broad implementation.
Additional dermoscopic images did not significantly enhance diagnostic concordance in the group “pigmented lesions,” which involved only nevus and melanoma, suggesting its added importance in diagnosing non-melanoma skin cancers. A prior meta-analysis by Bourkas et al., which combined different types of skin lesions into a single analysis, suggested the limited additional value of dermoscopic images (177). In contrast, the meta-analysis of Chen et al. reported a substantially larger improvement in diagnostic accuracy for melanocytic lesions when dermoscopy was utilized in addition to clinical examination. This discrepancy, however, is likely attributable to methodological and contextual differences, as their study evaluated in-person, as well as remote clinical and dermoscopic examinations, whereas our present study focused solely on remote diagnostic agreement. They found that the diagnostic benefit of dermoscopy was more pronounced in purely in-person examinations and reduced when remote image assessment was included. These results suggest that the diagnostic gain of dermoscopy is attenuated in remote settings, consistent with our observations (179).
Although our results showed no significant benefit in the groups “all skin conditions” and “pigmented lesions,” we found that dermoscopy improves diagnostic accuracy for skin cancers. Our results, further supported by high sensitivity and specificity values, demonstrate that teledermatology has great potential as a screening tool for malignant skin diseases, including melanoma. As melanoma has the highest mortality among skin cancers, particularly when diagnosis is delayed, early detection is crucial to promote public health, reduce economic costs of health care, and improve patient outcomes (180, 181). However, analyses stratified by individual non-melanoma skin cancer subtypes were precluded by the lack of consistently reported, subtype-specific diagnostic outcomes in the included studies.
Further strengthening the easy applicability of teledermatology, we found no statistically significant difference based on the photography device and the training received for image acquisition. Contrary to previous findings, our results showed that images taken by patients with smartphones, without previous training for image acquisition, are not associated with lower diagnostic concordance, possibly due to the larger number of studies included in our analysis (177, 178, 182). This reinforces the feasibility of implementing the direct method more easily in daily practice.
Time efficiency is crucial to the widespread use of teledermatology. In our analysis, the mean diagnostic time was 1.05 min per case, which can be explained by the fact that all studies included in the analysis used the store-and-forward method, which is recognized in the literature as the fastest method (11). Although a direct comparison with face-to-face visits was not possible, prior studies suggest that traditional face-to-face visits can last up to 15–25 min (183), implying that significantly more patients can be managed through teledermatology in the same time frame. Patient satisfaction was also high, with 82% of patients expressing satisfaction with their teledermatology experience, suggesting that real-time interaction is not essential, since most included studies used the store-and-forward method.
The high concordance rates observed across all disease categories support the broad applicability of teledermatology for a wide range of skin conditions. Notably, our results indicate that teledermatological care remains reliable even without the use of dermoscopy, both for general skin conditions and for melanoma screening. This may be especially relevant in low-resource settings, where access to dermoscopic equipment and training may be limited (184). Given its efficiency, diagnostic accuracy, and high user satisfaction, teledermatology, particularly the direct store-and-forward approach, offers a scalable solution that can be effectively integrated into routine clinical workflows, however further tailoring for low-income settings should be implemented. These findings, in line with the WHO’s call to improve primary care for skin conditions, underscore the potential of teledermatology to alleviate the burden on dermatology services by enabling timely access to specialist care without compromising diagnostic reliability (6).
Strengths and limitations
4.1
Our study has multiple strengths. By rigorously following our pre-registered protocol and adhering to the guidelines of the Cochrane Collaboration, we ensured high standards of quality, transparency, and replicability. To our knowledge, this study represents the most comprehensive meta-analysis to date, incorporating diverse methodologies, disease categories, and imaging technologies.
This meta-analysis was based on a large, international dataset comprising studies from 33 countries, the majority of which were conducted in middle- and high-income countries. However, the underrepresentation of low-income countries may restrict the generalizability of our results to lower-resource settings.
A key limitation is pooling different skin cancer types into a single analytical category, as subtype-specyfic analyses were constrained by the existing evidence base, as most studies reported outcomes under broad categories, without providing stratified data by individual skin cancer subtype.
Substantial heterogeneity was also observed across analyses. Despite extensive subgroup analyses, heterogeneity remained high, likely reflecting diverse study settings, and predominantly observational designs.
Additional limitations include the presence of moderate and high risk of bias in several studies, evidence of publication bias, and the inability to pool predictive values due to the inconsistent disease prevalence reporting.
Implications for practice
4.2
We emphasize that improving access to dermatological care requires translating scientific findings into practice. We therefore support the integration of teledermatology into daily clinical workflows (185, 186). Our findings underscore the importance for policy engagement and strategic investment in telehealth infrastructure to facilitate its broader implementation.
Implications for research
4.3
To facilitate appropriate adoption across heterogenous resource settings, future studies specifically designed to low-income countries are required, focusing on technical feasibility, integration within existing health care infrastructures, diagnostic performance when implemented by non-specialist personnel, long-term sustainability in settings with limited specialist availability, and patient-centered outcomes. To further elucidate the reliability of teledermatology, future studies should focus on reporting outcomes separately for individual disease subtypes, especially for non-melanoma skin cancers, as well as on standardized outcome reporting, in particular true positives, true negatives, false positives, and false negatives, which are needed to determine sensitivity and specificity. Conducting future research on technology-enhancing modalities, such as complementary imaging techniques and artificial intelligence, is necessary to further improve the diagnostic concordance in more complex cases.
Conclusion
5
In conclusion, our study suggests that teledermatology is an effective tool for the remote diagnosis of a wide range of skin conditions. The high efficiency of the direct store-and-forward method, as the most easily applicable approach, indicates potential suitability in resource-limited settings, however, further research is needed to ensure its adaptability in low-resource environments.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ferrari AJ Santomauro DF Aali A Abate YH Abbafati C Abbastabar H . Global incidence, prevalence, years lived with disability [YL Ds], disability-adjusted life-years [DAL Ys], and healthy life expectancy [HALE] for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2024) 403:2133–61. doi: 10.1016/S 0140-6736(24)00757-838642570 PMC 11122111 · doi ↗ · pubmed ↗
- 2Flohr C Hay R. Putting the burden of skin diseases on the global map. Br J Dermatol. (2021) 184:189–90. doi: 10.1111/bjd.19704, 33544440 · doi ↗ · pubmed ↗
- 3Balboul S Gronbeck C Feng H. Dermatology workforce projections in the United States, 2021 to 2036. Arch Dermatol Res. (2024) 316:192. doi: 10.1007/s 00403-024-02924-2, 38775980 · doi ↗ · pubmed ↗
- 4Gaffney R Rao B. Global teledermatology. Glob Dermatol. (2015) 2:209–14. doi: 10.15761/GOD.1000156 · doi ↗
- 5Yoo JY Rigel DS. Trends in dermatology: geographic density of US dermatologists. Arch Dermatol. (2010) 146:779. doi: 10.1001/archdermatol.2010.127, 20644040 · doi ↗ · pubmed ↗
- 6WHO. Skin diseases as a global public health priority. (2025) February 10, 2025. Report No.: EB 156/24. Geneva, Switzerland: WHO.
- 7Perednia DA Brown NA. Teledermatology: one application of telemedicine. Bull Med Libr Assoc. (1995) 83:42–7. 7703938 PMC 225996 · pubmed ↗
- 8López-Liria R Valverde-Martínez MA López-Villegas A Bautista-Mesa RJ Vega-Ramírez FA PeiróS . Teledermatology versus face-to-face dermatology: an analysis of cost-effectiveness from eight studies from Europe and the United States. Int J Environ Res Public Health. (2022) 19:2534. doi: 10.3390/ijerph 19052534, 35270227 PMC 8909884 · doi ↗ · pubmed ↗