Surgical Outcomes and Prognostic Impact of Lung Cancer Associated with Cystic Airspaces: A Retrospective Analysis of 75 Cases
Yuichiro Machida, Kento Suzuki, Mitsunobu Ino, Takumi Sonokawa, Norihito Kawasaki, Jitsuo Usuda

TL;DR
This study examines lung cancer cases with cystic airspaces and finds they have worse outcomes compared to other cases.
Contribution
The study identifies LCCA as a prognostic factor and classifies it into four types with distinct cancer types.
Findings
LCCA cases had worse survival outcomes compared to non-LCCA lung cancer cases.
Stage and LCCA were significant prognostic factors in multivariate analysis.
LCCA types I and III were associated with adenocarcinoma, while Type IV was linked to squamous cell carcinoma.
Abstract
The present study reviewed surgical cases of lung cancer associated with cystic airspace (LCCA) and examined the imaging and clinicopathological features of these cases. A total of 75 patients with lung cancer associated with cystic airspace, who underwent lung cancer surgery in our hospital between January 2017 and December 2020, were included. We retrospectively analyzed the association between postoperative recurrence of lung cancer and lung cancer associated with the cystic airspace using the Cox proportional hazards model. Patients with LCCA had a worse prognosis than those with non-LCCA. Furthermore, a univariate analysis showed a significant difference between sex, smoking, differentiation, tumor size, Stage, and LCCA, while a multivariate analysis showed a significant difference between Stage and LCCA. LCCA cases were classified into four categories, as reported in a previous…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
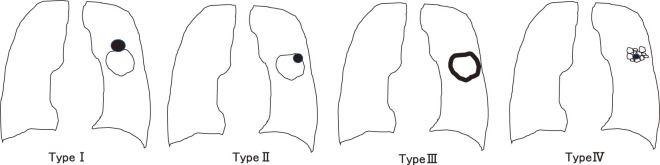 Fig. 1
Fig. 1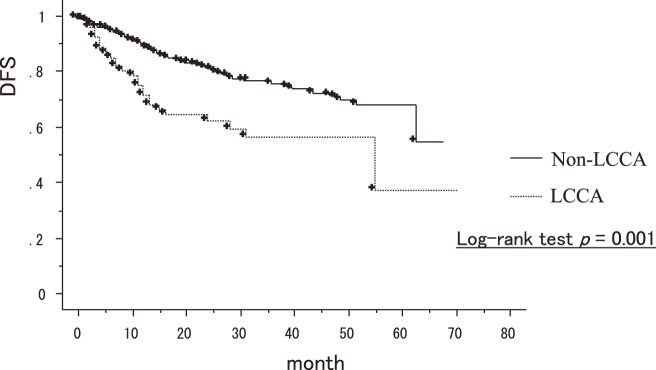 Fig. 2
Fig. 2| LCCA (N = 75) | Non-LCCA (N = 518) | p value | |
|---|---|---|---|
| Age | 68.6 (28–85) | 71.1 (32–91) | 0.007 |
| Sex | |||
| Male | 59 (79.7%) | 290 (56%) | 0.003 |
| Female | 16 (20.3%) | 228 (40%) | |
| Smoking history | |||
| Ever | 70 (93.3%) | 351 (67.8%) | <0.001 |
| Never, unknown | 5 (6.7%) | 167 (32.2%) | |
| Pathological stage | |||
| Ⅰ | 39 (52%) | 386 (74.5%) | 0.289 |
| II–III | 36 (48%) | 132 (25.5%) | |
| Tumor size (invasive diameter) | 3.6 (0.8–13.5) | 2.4 (0–13.5) | <0.001 |
| FDG-PET | |||
| SUV-Max | 8.0 ± 11.2 | 6.3 ± 6.0 | 0.478 |
| Differentiation | |||
| G1/G2 | 46 | 374 | 0.072 |
| G3/G4 | 29 | 144 | |
| Pathology | |||
| Adenocarcinoma | 40 (53.3%) | 379 (73.2%) | 0.003 |
| Squamous | 23 (30.1%) | 95 (18.3%) | |
| Others | 12 (16.6%) | 44 (8.5%) | |
| Surgery | |||
| Lobectomy | 65 (86.7%) | 431 (83.2%) | 0.578 |
| Segmentectomy | 1 (1.3%) | 16 (3.1%) | |
| Wide wedge resection | 9 (12.0%) | 71 (13.7%) |
| Parameter | HR | 95% CI | p value |
|---|---|---|---|
| Gender | 0.514 | 0.338–0.780 | 0.0017 |
| Age (<75) | 1.187 | 0.811–1.739 | 0.3778 |
| Smoking | 1.758 | 1.108–2.789 | 0.0165 |
| Differentiation | 0.398 | 0.199–0.793 | 0.0088 |
| Tumor size (invasive diameter) | 3.961 | 2.703–5.805 | <0.001 |
| Stage | 7.502 | 4.752–10.464 | <0.001 |
| LCCA | 2.156 | 1.337–3.478 | 0.0016 |
| Parameter | HR | 95% CI | p value |
|---|---|---|---|
| Gender | 1.44 | 0.843–2.460 | 0.182 |
| Smoking | 1.277 | 0.281–2.265 | 0.404 |
| Differentiation | 1.942 | 0.968–3.897 | 0.062 |
| Tumor size (>3 cm) | 0.721 | 0.443–1.174 | 0.188 |
| Stage | 0.176 | 0.106–0.290 | <0.001 |
| LCCA | 0.507 | 0.281–0.915 | 0.024 |
| I (N = 24) | II (N = 2) | III (N = 23) | IV (N = 26) | |
|---|---|---|---|---|
| Age | 66.9 (46–78) | 64 (55–73) | 67.7 (28–80) | 71.2 (48–85) |
| Sex | ||||
| Male | 20 | 1 | 16 | 22 |
| Female | 4 | 1 | 7 | 4 |
| Smoking history | ||||
| Ever | 20 | 2 | 19 | 25 |
| Never, unknown | 4 | 0 | 4 | 1 |
| Stage | ||||
| I | 17 | 0 | 11 | 11 |
| II–III | 7 | 2 | 12 | 15 |
| Tumor size | 2.96 (1.1–11.8) | 7.25 (4.5–10) | 3.69 (0.8–13.5) | 3.38 (1.2–8) |
| Pathology | ||||
| Adenocarcinoma | 14 | 1 | 19 | 6 |
| Squamous | 5 | 0 | 3 | 15 |
| Others | 5 | 1 | 1 | 5 |
| Surgery | ||||
| Lobectomy | 23 | 2 | 21 | 17 |
| Sublobectomy | 0 | 0 | 0 | 1 |
| Wide wedge | 1 | 0 | 1 | 7 |
| Others | 0 | 0 | 1 | 1 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Diagnosis and Treatment · Pleural and Pulmonary Diseases · Tracheal and airway disorders
Introduction
Lung cancer is one of the most well-known malignant tumors and the leading cause of cancer-related death worldwide.^1)^ The widespread use of computed tomography (CT) in lung cancer screening and the evolution of lung cancer screening programs have led to relatively early detection of lung cancer.^2)^ With the widespread use of radiological screening, the detection of cystic air spaces is increasing.^3)^ Lung cancer associated with cystic airspace (LCCA) is often misinterpreted as inflammation or infection,^4)^ and there are few reports of surgery for LCCA.
The present study reviewed surgical cases of LCCA and examined the imaging and clinicopathological features of the disease.
Materials and Methods
Patients
We retrospectively reviewed a database of 75 patients diagnosed with LCCA from among 593 patients who underwent surgery for primary lung cancer at Nippon Medical School Hospital between 2017 and 2020. Tumors were classified according to TNM classification (8th edition).^5)^ No benign lesions were found in the resected lesions. This study was approved by the Institutional Review Board of Nippon Medical School, Tokyo, Japan (B-2023-664).
LCCA classification
Drawings of the four morphological patterns of LCCA were reported by Mascalchi et al. (Fig. 1).^6)^
Four classifications of LCCA by Mascalchi et al.6) LCCA: lung cancer associated with cystic airspace
•Type I: nodule or mass extruded from the wall of the cystic airspace.•Type II: nodule or mass confined within the cystic airspace.•Type III: soft tissue density extending along the wall of the cystic air space.•Type IV: soft tissue density intermixed within clusters of cystic air spaces.
These cases were classified by second thoracic surgeons (YM, TS).
Statistical analyses
All statistical analyses were performed using the StatView software program (SAS Institute Inc., Cary, NC, USA). Differences between the groups were analyzed using the Pearson x^2^ test for categorical variables and an unpaired Student’s t-test. Prognostic factors were examined using univariate and multivariate analyses. Disease-free survival (DFS) rates were calculated using the Kaplan-Meier method and compared using the log-rank test. Hazard ratios and confidence intervals (CIs) were estimated using a stratified Cox proportional hazards model. Statistical significance was set at P <0.05.
Results
A comparison of LCCA and non-LCCA
The relationship between LCCA and clinicopathological characteristics of patients is shown in Table 1. LCCA patients accounted for 10.8% of all who underwent surgery for lung cancer. The median age of patient age was 70.8 (range: 28–91) years old. The LCCA status among the study patients was as follows: LCCA (n = 75, 10.8%) and non-LCCA (n = 518, 89.2%). On fluorodeoxyglucose-positron emission tomography (FDG-PET), the maximum standardized uptake value (SUV_max_) values of LCCA were higher than those of non-LCCA.
Prognostic analyses of all cases
Kaplan–Meier method of disease-free survival showed a significant association between LCCA and non-LCCA (p = 0.001) (Fig. 2). Sex (p = 0.0017), smoking (p = 0.016), differentiation (G3/4) (p = 0.0088), tumor size (p <0.001), stage (p <0.001), and LCCA (p = 0.0016) were significantly associated with the DFS in a univariate analysis (Table 2). A multivariate analysis of these significant variables showed that LCCA (p = 0.024) and stage (p <0.001) were independently associated with the DFS (Table 3).
The disease-free survival for LCCA and non-LCCA.
Consideration of classified LCCAs
The LCCA group was divided according to the classification established by Mascalchi et al. (Table 4).^6)^ Types I and III were mostly adenocarcinomas, while Type IV was mostly squamous cell carcinoma.
Discussion
In 1951, the first report of lung cancer associated with bullous lung disease was published by Bass and Singer.^7)^ In 1968, Goldstein et al. described the incidence of bulla-associated carcinoma as 3.8%.^8)^ Hanaoka et al. described the incidence of bulla-associated carcinoma as 3.4%.^9)^ Kaneda et al. reported the incidence of LCCA as 3.5%.^10)^ In our study, LCCA accounted for 10.8% of all cases. We suspect that the rate of LCCA has increased owing to the widespread use of CT in lung cancer screening and increased awareness of LCCA. We believe that the number of LCCA cases will continue to increase even further in the future.
While the pathogenesis of LCCA remains unknown, the check valve mechanism is the most popular theory.^11,12)^ Tan et al.^11)^ observed two types of “check valves”; one type arises from the alveolar wall and consists of tumors producing abundant fibrous tissue, which they reported causes local extrinsic compression of adjacent bronchi that communicate with the cystic vacuole. In the other type, however, tumor cells infiltrate directly into the bronchus or bronchial luminal wall, causing obstruction. The authors explained that these were important inciting events in LCCA. In summary, restricted airflow within the cyst allows microorganisms and carcinogens to deposit on the cyst wall, resulting in recurrent inflammation and formation of a microenvironment for carcinogenesis. Although much remains to be clarified, it is necessary to investigate the pathogenesis of LCCA from a molecular and biological perspective.
There are no clear conclusions regarding the prognosis of LCCA because of the small number of reports. However, based on our results, the prognosis of LCCA is poor, as reported by Jung^3)^ and Kaneda et al.^10)^ By contrast, Hanaoka et al.^9)^ reported that the postoperative survival rate of patients with LCCA is comparable to that of lung cancer patients without LCCA when the disease is resected early. Watanabe et al.^13)^ reported that the thickness of the cavity wall was an independent prognostic factor. Furthermore, Shinohara et al.^14)^ reported that patients with LCCA have a better overall survival rate than those without LCCA. Although the prognosis of LCCA is still under debate, it is necessary to study the prognosis adjusted for the clinicopathologic and imaging features of LCCA in the future.
The LCCA classification was first reported by Meskariki et al.^6)^ They classified lung cancers associated with cystic vacuoles into four morphological patterns, as shown in Fig. 1. Types I and II are reported to be associated with a higher frequency of intermediate or poorly differentiated adenocarcinomas than other morphological features on imaging.^6)^ In our study, adenocarcinoma was more common in Types I and III than in other types. This could be a clue to the formation of nodular carcinomas in the cyst wall. Shen et al.^15)^ and Fintelmann et al.^12)^ reported the classification of LCCA, and Shen et al. classified these lesions into four types: Type I, mean wall thickness <2 mm; Type II, mean wall thickness >2 mm; Type III, cystic vacuoles with mural cell nodules; and Type IV, mixed tissue within the cystic vacuole group. A multivariate analysis showed that lung adenocarcinoma with a Type III morphologic pattern was an independent risk factor for high pathologic invasiveness; patients with Type III LCCA had significantly worse survival than those with Type I LCCA. Type III tumors had the highest epidermal growth factor receptor mutation rate.^16)^ Although various classifications have been reported, no classification method has been established. We suggest that it is necessary to create a simpler classification of LCCA in the future.
Several limitations associated with the present study are worth mentioning. The sample size of this study was very small, and the study period duration was a single institution. This was a retrospective study with a relatively short duration. When conducting such a study, it would be desirable to conduct it at multiple institutions with a larger sample size.
Conclusion
LCCA, especially lung cancers with thick walls or intraluminal nodules, has a poor prognosis. In fact, it is difficult to measure the maximum diameter of a tumor using CT. In addition, it is often difficult to determine which of the T factors of the TNM classification are applied. Therefore, further studies are needed to accumulate more LCCA cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin 2011; 61: 69–90.21296855 10.3322/caac.20107 · doi ↗ · pubmed ↗
- 2Pan X, Wang H, Yu H, et al. Lung cancer associated with cystic airspaces: CT and pathological features. Transl Cancer Res 2020; 9: 3960–4.35117762 10.21037/tcr-20-1926 PMC 8797737 · doi ↗ · pubmed ↗
- 3Jung W, Cho S, Yum S, et al. Stepwise disease progression model of subsolid lung adenocarcinoma with cystic airspaces. Ann Surg Oncol 2020; 27: 4394–403.32363512 10.1245/s 10434-020-08508-4 · doi ↗ · pubmed ↗
- 4Sheard S, Moser J, Sayer C, et al. Lung cancers associated with cystic airspaces: underrecognized features of early disease. Radiographics 2018; 38: 704–17.29652577 10.1148/rg.2018170099 · doi ↗ · pubmed ↗
- 5Goldstraw P, Chansky K, Crowley J, et al. The IASLC lung cancer staging project: proposals for revision of the TNM stage groupings in the forthcoming (Eighth) Edition of the TNM Classification for lung cancer. J Thorac Oncol 2016; 11: 39–51.26762738 10.1016/j.jtho.2015.09.009 · doi ↗ · pubmed ↗
- 6Mascalchi M, Attinà D, Bertelli E, et al. Lung cancer associated with cystic airspaces. J Comput Assist Tomogr 2015; 39: 102–8.25279848 10.1097/RCT.0000000000000154 · doi ↗ · pubmed ↗
- 7Bass HE, Singer E. Co-existing lobar adenocarcinoma and cystic disease of the lung. Ann Intern Med 1951; 34: 498–507.14800221 10.7326/0003-4819-34-2-498 · doi ↗ · pubmed ↗
- 8Goldstein MJ, Snider GL, Liberson M, et al. Bronchogenic carcinoma and giant bullous disease. Am Rev Respir Dis 1968; 97: 1062–70.5658877 10.1164/arrd.1968.97.6P 1.1062 · doi ↗ · pubmed ↗