A Systematic Mapping Review of Core Outcome Reporting in Surgical Research for Oesophageal Cancer
Nadia Matias, Anie Naqvi, Jack Thomson, Roukia Techache, Kerry Avery, Natalie Blencowe, Rhiannon Macefield, Bilal Alkhaffaf

TL;DR
This study reviews how well surgical research on oesophageal cancer reports key outcomes, finding that most studies do not fully adopt a recommended set of core outcomes.
Contribution
The paper evaluates the adoption of a core outcome set in oesophageal cancer surgery research, revealing low compliance and no improvement over time.
Findings
No study reported all 10 core outcomes, with a median of 4 outcomes reported.
In-hospital mortality and conduit necrosis/leak were most frequently reported (86% and 81%, respectively).
Overall survival and quality of life were reported in only 30% and 26% of studies, respectively.
Abstract
Oesophageal carcinoma is a rising global health burden, with surgical resection and perioperative chemotherapy forming the cornerstone of curative treatment. However, uncertainty persists regarding the optimal surgical approach, partly due to heterogeneity in outcome reporting, which hinders data synthesis and evidence‐based decision‐making. To address this, a core outcome set (COS) for oesophageal cancer surgery was developed through international consensus among clinicians and patients. This study systematically evaluates the uptake of these core outcomes in contemporary surgical research. A systematic review was conducted of randomised controlled trials and prospective cohort studies investigating oesophagectomy for oesophageal cancer, published between 2010 and 2024. The reporting of ten COS‐recommended outcomes was assessed across eligible studies. Fifty‐eight studies involving 22…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
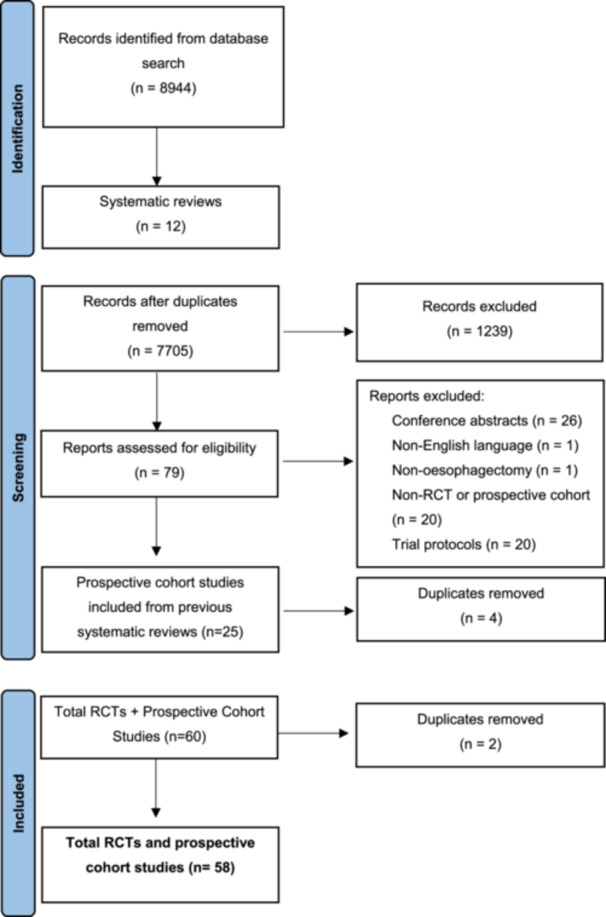 Figure 1
Figure 1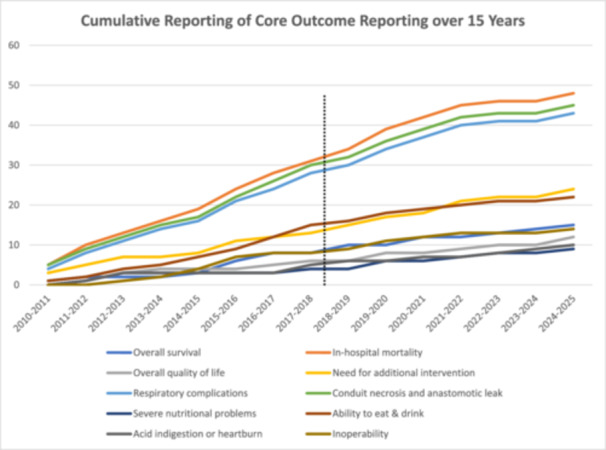 Figure 2
Figure 2| Inclusion | Exclusion | |
|---|---|---|
| Type of studies |
RCTs Prospective cohort studies or cohort studies with prospectively maintained databases English language studies |
Surgical RCTs, systematic reviews and cohort studies involving combination of surgical and non‐surgical interventions Retrospective cohort studies Trial protocols Non‐English language studies |
| Population |
Patients aged 18 years and over |
Patients below the age of 18 |
| Intervention |
Partial or total oesophagectomy Surgery with curative intent Oesophagectomy for gastro‐oesophageal junctional tumours |
Surgery with non‐curative intent (i.e., in stage 4 cancer, expected R1/R2 resection), for example for relief of symptoms Salvage surgery Endoscopic interventions Partial or total gastrectomy |
| Conditions |
Invasive localised cancer of oesophagus and gastro‐oesophageal junction Surgically resectable tumours |
Barret′s dysplasia or non‐invasive oesophageal neoplasms Metastatic/advanced disease Sarcomas Lymphomas |
| Randomised controlled trials | |||||||
|---|---|---|---|---|---|---|---|
| Study | Author | Publication year | Countries | Recruiting centres | Randomised patients | Interventions | Type of Study |
| PRE‐ COS | |||||||
| 1 | YC Yuan et al. [ | 2011 | China | 1 | 68 |
Modified thoracoscopic oesophagectomy Minimally invasive oesophagectomy | RCT |
| 2 | Biere et al. [ | 2012 | Netherlands, Spain, Italy | 3 | 105 |
Minimally invasive oesophagectomy Open oesophagectomy | RCT |
| 3 | Van der Sluis et al. [ | 2012 | Netherlands | 1 | 112 |
Robot‐assisted thoraco‐laparoscopic oesophagectomy Open three‐stage transthoracic esophagectomy | RCT |
| 4 | Guo et al. [ | 2013 | China | 1 | 221 |
Video‐assisted thoracoscopic radical esophagectomy (VATS) combined with laparoscopy Right open transthoracic oesophagectomy | RCT |
| 5 | Maas et al. [ | 2014 | Netherlands | 1 | 27 |
Minimally invasive oesophagectomy Open oesophagectomy | RCT |
| 6 | Li et al. [ | 2015 | China | 1 | 300 |
Ivor Lewis oesophagectomy Sweet oesophagectomy | RCT |
| 7 | Luketich et al. [ | 2015 | USA | 1 | 95 |
3 stage minimally invasive oesophagectomy 2 stage minimally invasive oesophagectomy | RCT |
| 8 | Nozaki et al. [ | 2015 | Japan | 37 | 379 |
Open oesophagectomy Thoracoscopic oesophagectomy | RCT and Prospective Cohort |
| 9 | Straatman et al. [ | 2017 | Netherlands, Spain, Italy | 3 | 115 |
Minimally invasive oesophagectomy Open oesophagectomy | RCT |
| POST COS | |||||||
| 10 | Ma et al. [ | 2018 | China | 1 | 144 |
Minimally invasive oesophagectomy Open oesophagectomy | RCT |
| 11 | Paireder et al. [ | 2018 | Austria | 1 | 29 |
Open oesophagectomy Hybrid minimally invasive oesophagectomy | RCT |
| 12 | Mariette et al. [ | 2019 | France | 13 | 207 |
Open oesophagectomy Hybrid minimally invasive oesophagectomy | RCT |
| 13 | Van der Sluis et al. [ | 2019 | Netherlands | 1 | 112 |
Robot‐assisted thoraco‐laparoscopic esophagectomy Open three‐stage transthoracic esophagectomy | RCT |
| 14 | Yang et al. [ | 2019 | China | Multiple | 360 |
Robot‐assisted esophagectomy Minimally invasive esophagectomy | RCT |
| 15 | Chao et al. [ | 2019 | Taiwan, China | 2 | 212 |
Robot‐assisted esophagectomy Video‐assisted thoracoscopic esophagectomy | RCT |
| 16 | Tagkalos et al [ | 2021 | Germany, Netherlands, Switzerland | 3 | 218 |
Robot assisted minimally invasive oesophagectomy Minimally invasive oesophagectomy | RCT |
| 17 | Li et al. [ | 2021 | China | 1 | 400 |
Oesophagectomy with Two‐Field lymphadenectomy Oesophagectomy with Three‐Field lymphadenectomy | RCT |
| 18 | Nuytens et al. [ | 2021 | France | 13 | 207 |
Open oesophagectomy Hybrid minimally invasive oesophagectomy | RCT |
| 19 | ROMIO Study Group [ | 2024 | UK | Multiple | 606 |
Hybrid (laparoscopic/thoracotomic) Open esophagectomy | RCT |
| RCT's | Prospective studies | |||||
|---|---|---|---|---|---|---|
| Pre‐publication of COS in 2018 | Post‐publication of COS in 2018 |
| Pre‐publication of COS in 2018 | Post‐publication of COS in 2018 |
| |
|
| 2 (10.5% of RCT's) | 6 (31.6% of RCTs) | 0.18 | 7 (17.9% of Prospective studies) | 0 (0% of Prospective studies) | 0.31 |
|
| 9 (47.4%) | 9 (47.4%) | 0.42 | 23 (58.9%) | 7 (17.9%) | 1.00 |
|
| 3 (15.8%) | 5 (26.3%) | 0.18 | 3 (7.7%) | 1 (2.6%) | 1.00 |
|
| 1 (5.2%) | 2 (10.5%) | 0.55 | 5 (12.8%) | 2 (5.1%) | 0.64 |
|
| 8 (42.1%) | 9 (47.4%) | 1.00 | 20 (51.3%) | 6 (15.4%) | 1.00 |
|
| 8 (42.1%) | 8 (42.1%) | 0.57 | 22 (56.4%) | 6 (15.4%) | 1.00 |
|
| 3 (15.8%) | 4 (21.1%) | 0.37 | 1(2.6%) | 1(2.6%) | 0.36 |
|
| 5 (26.3%) | 5 (26.3%) | 1.00 | 10 (25.6%) | 2 (5.1%) | 0.69 |
|
| 3 (15.8%) | 4 (21.1%) | 0.38 | 3 (7.7%) | 0 (0%) | 1.00 |
|
| 2 (10.5%) | 5 (26.3%) | 0.38 | 6 (15.4%) | 1(2.6%) | 1.00 |
| Studies Reporting outcome ( | Studies providing definitions ( | Measurement Tool | Timeframe | |
|---|---|---|---|---|
|
| 17 (29.8%) | 6 (10.3%) | ‐‐‐ | 2/3/5 years post‐operatively |
|
| 49 (85.9%) | 8 (13.8%) | ‐‐‐ | 30/60/90 days post‐operatively |
|
| 13 (22.8%) | 3 (5.17%) | ‐‐‐ | ‐‐‐ |
|
| 15 (26.3%) | ‐‐‐ | (Patient reported Outcome Measures questionnaire) SF‐36, CAT EORTC QLQ‐C30, CAT EORTC QLQ‐OES18, VAS, FACT‐E, HAD′s score, Fatigue score (MFI‐20), Modified Katz and the Lawton and Brody Scale | — |
|
| 11 (19.3%) | 8 (13.8%) | OES 18 | |
|
| 25 (43.9%) | 8 (13.8%) | OES 18 | |
|
| 12 (21.05%) | 8 (13.8%) | OES 18 | |
|
| 45 (78.9%) | 14 (24.1) | Esophagectomy Complications Consensus Group (‘ECCG′) classification ( | |
|
| 46 (80.7%) | ‐‐‐ | Esophagectomy Complications Consensus Group (‘ECCG′) classification ( | ‐‐‐ |
|
| 9 (15.8%) | ‐‐‐ | ‐‐‐ | 30 days post‐operatively |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDelphi Technique in Research · Esophageal Cancer Research and Treatment · Colorectal and Anal Carcinomas
Introduction
1
Oesophageal cancer remains a significant health burden as the eighth most common malignancy worldwide, with an increasing incidence in the Western world [1].
Although there has been significant improvement in the survival of localised oesophageal cancer [2], surgery post neoadjuvant therapy remains the cornerstone of curative treatment in locally advanced tumours [3]. Minimally invasive surgery for oesophageal cancer was first introduced in 1992. The long‐term results of the first randomised controlled trial (RCT) comparing hybrid techniques (laparoscopic abdominal phase and open thoracic phase) to open surgery were published in 2019 [3]. There have been few comprehensive RCTs comparing resection techniques based on postoperative outcomes. This may be due to the complexities of designing and delivering a surgical RCT, not least due to lack of standardisation in surgical expertise among various centres and strong surgeon preferences, which makes recruitment challenging [4].
Patients and clinicians have differing priorities on outcomes and what should be reported in the literature [5]. This heterogeneity poses a challenge to the systematic assessment of surgical approaches, contributing to significant research waste [6].
A core outcome set (COS) [6] was developed following a rigorous consensus process based on the COMET guidelines [7]. This was primarily undertaken to guide the development and application of a “minimum set of outcomes that should be measured and reported in all clinical trials of a specific disease or trial population” [7]. In the case of oesophageal cancer resection, the following 10 core outcomes were classed as essential: overall survival, in‐hospital mortality, inoperability, need for additional intervention, respiratory complications, conduit necrosis and anastomotic leak, severe nutritional problems, the ability to eat and drink, problems with acid indigestion or heartburn, and overall quality of life.
This study aims to map the reporting of core outcomes included in the previously described COS and establish the heterogeneity in more recent studies evaluating surgical treatments for oesophageal cancer. This would highlight the degree of uptake of the COS and identify areas requiring future work to improve the status quo.
Methods
2
This review was registered on the PROSPERO database and reported in line with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta‐Analyses) guidance [8].
Definitions
2.1
This review focuses on surgical studies comparing two or more therapeutic surgical interventions [9]. We define ‘therapeutic surgical intervention′, in the context of oesophageal malignancy, as a potentially curative intervention aiming to excise the oesophageal neoplasm, resulting in partial or total organ loss. Therefore, non‐surgical (e.g., endoscopic) therapies were excluded from this study.
Search Strategy
2.2
An initial systematic review included studies published from January 2006 to May 2011 [6] in conjunction with the development of the COS. This was used to aid the identification of trials for inclusion in the present study. An updated search strategy was generated between January 2010 and October 2024. The strategy is described in the supplementary appendix 1. The following databases were searched for studies that met the inclusion criteria
- Evidence Based Medicine Reviews via OVID (1 January 2010 to 1 October 2024)
- Cochrane Database of Systematic Reviews
- ACP Journal Club
- Database of Abstracts of Reviews of Effects
- Cochrane Central Register of Controlled Trials
- Health Technology Assessment
- NHS Economic Evaluation Database
- MEDLINE via OVID, EMBASE via OVID, CINAHL via EBSCO (1 January 2010 to 1 October 2024)
Eligibility Criteria
2.3
The inclusion and exclusion criteria are summarised in Table 1. Systematic reviews were included to identify relevant RCTs from the reference list. Non‐English language studies were excluded, as were conference abstracts, as word count limitations would likely restrict reporting of all outcomes measured in a study.
Data Analysis
2.4
Our group has previously described the heterogeneity of outcome reporting in the present published literature [6]. A meta‐analysis is beyond the scope of this review, as it primarily looks at the quality of ‘what′ and ‘how′ outcomes are reported. Descriptive statistical analysis was performed using Microsoft Excel. Statistical analysis using two‐tailed Fisher's Exact Test was performed on the cumulative core outcomes, offering a comparison pre and post‐publication of the COS.
Results
3
Study Selection
3.1
There were 8944 studies identified from the initial database search, which included primary studies and systematic reviews. After resolving discrepancies, 79 articles were included for analysis. These included 12 systematic reviews to source studies that may have been missed in the initial search (Figure 1). 58 individual studies were included for analysis. Articles reporting the same study were analysed together for ease of reference and to avoid duplication.
Preferred reporting items for systematic reviews and meta‐analyses (PRISMA) flowchart summarising study selection process.
Study Characteristics
3.2
The 58 studies that met the inclusion criteria included 19 RCTs and 39 prospective cohort studies (Table 2‐ Appendix). The majority of studies were undertaken in Europe and North America (64%) and the rest in Asia (33%), with one study in Australia. A total of 22 260 patients undergoing oesophageal resections for cancer were recruited. The smallest number of patients in a single study was 13, and the largest was 5822. The largest number of studies on oesophageal cancer resections was published in 2019. Most (24.6%) studies, published between 2010 and 2012, compared the outcomes of variations of minimally invasive and hybrid techniques with open surgery, after which the results of the first trial of robot‐assisted oesophagectomy were published in 2012 [12]. Four studies primarily evaluated the effect of lymphadenectomy on outcomes.
There were 42 (72.4%) studies comparing minimally invasive surgery with open approaches over 15 years. These included robotic, laparoscopic, and hybrid (e.g., a combination of laparoscopic abdominal and open thoracic) procedures. Surgical approaches (e.g., transthoracic vs. transhiatal) were the next most commonly studied (18.9%).
Core Outcome Reporting
3.3
There were 9 RCTs and 27 prospective cohort studies pre‐publication of the COS. The number of RCTs and prospective cohort studies post‐publication was 10 and 12, respectively. No study reported all core outcomes of the COS. The average number of outcomes reported was 4 (interquartile range 3–5).
In addition to the COS, study outcomes included postoperative morbidity, fatigue, lung collapse, bile leak, chylothorax, multiorgan dysfunction syndrome and cerebrovascular events. Five studies reported single or no outcomes from the COS. These prioritised oncological outcomes such as 5‐year survival, disease‐free survival rates, R0 resection rate, number of resected lymph nodes (LNs) and patterns of recurrence.
Table 3 demonstrates the reporting ratio of outcomes of included studies pre and post‐publication of the COS. There were no outcomes of statistical significance in either group (Table 4).
Core Outcome Reporting Trends
3.4
No discernible trends were identified over the past 15 years. (Figure 2). The most consistently reported outcomes were surgery‐related death (86%), conduit necrosis and leak (81%) and respiratory complications (79%).
Cumulative trends in outcome reporting over the past 15 years demarcated by publication of COS in 2018.
Defining and Measuring Outcomes
3.5
Thirty studies allocated a time period post‐operatively to report ‘in‐hospital mortality′. Three studies defined ‘inoperability′ as irresectability due to advanced disease found intra‐operatively. Twelve studies provided descriptions of the questionnaires given to patients to ascertain ‘overall quality of life′. These included a combination of several quality‐of‐life surveys, e.g. SF‐36, CAT EORTC QLQ‐C30, CAT EORTC QLQ‐OES18, VAS, FACT‐E and HAD′s score. Definitions for ‘respiratory complications varied from broad terminology such as ‘pneumonia,′ ‘atelectasis,′ and ‘pulmonary embolism′ to specific ones such as Computed Tomography (CT) and sputum culture‐proven pneumonia. The second most reported outcome was ‘conduit necrosis and leak′ (79%/n = 46), with two studies utilising the ECCG classification to define it. ‘Severe nutritional problems′ and ‘acid reflux and indigestion′ were the two least reported patient‐centred outcomes. Both were assessed via the OES 18 questionnaire, which included questions, such as, “Have you had trouble swallowing your own saliva?” and “Have you choked while swallowing?”. The ‘ability to eat and drink′ was recorded in 41.4% (n = 24) of studies. Nine studies used the EORTC QLQ‐OES18 questionnaire. The need for additional intervention, such as a return to theatre, was the lowest recorded surgical outcome.
Serious Adverse Events
3.6
Although not part of the COS, the majority (n = 54) of studies reported serious adverse outcomes. These were inconsistently defined. Twenty‐six studies used broad terms such as ‘complications′, ‘post‐operative complications′, or ‘intraoperative complications′. Four used terminology such as ‘morbidity′ or ‘general morbidity′. Some commented on individual outcomes (n = 12), while eight studies pooled complications based on severity or peri‐operative timing. Several studies (n = 27) reported adverse events as a combination of both.
Twenty‐three studies (39.7%) utilised grading systems such as Clavien‐Dindo, Common Terminology Criteria for Adverse Events, Comprehensive Complication Index, or criteria set by Low et al. [66].
Discussion
4
This review mapped the outcomes, described in a COS, for oesophageal cancer resection studies over the past 15 years and demonstrates the need for further standardisation of reporting in the literature. Overall, our study shows that there has been no significant improvement in the reporting of core outcomes since the COS was published in 2018.
Results show considerable variation in the priorities of oesophageal cancer resection studies globally.
Some studies have clearly defined objectives from the outset, focusing solely on oncological outcomes such as the extent of lymphadenectomy and resection margins. However, most studies reported outcomes related to short‐term complications. Similar findings were observed in the COMPAC (Core Outcome Measures for Perioperative and Anaesthetic Care) study, which aimed to establish core outcome sets in perioperative care and anaesthesia [67]. Patient‐reported outcomes were consistently poorly prioritised compared to clinical.
Selective reporting of certain outcomes leads to bias and an erosion of public trust in clinical studies. A significant proportion of planned study outcomes are not being reported as they may be subjectively deemed unimportant by researchers [68]. Preventing reporting bias and ensuring the representation of all stakeholders are compelling reasons for implementing a COS in the reporting of all research examining oesophagectomy practice.
The COS referenced in our study does not encompass serious adverse events and oncological outcomes. Calls for standardisation in the reporting of serious adverse events have been made by Low et al., [66] who formulated guidelines through a collaborative effort across 21 international centres. There is a rationale for developing distinct COS′ for oesophagectomies to categorise surgical, oncological, and patient‐centred outcomes. There is significant ambiguity in outcome definition across various studies, with endpoints and time periods being either undefined or unclear. The COMET (Core Outcome Measures in Effectiveness Trials) initiative launched in 2010 and the Standardising Endpoints for Perioperative Medicine (StEP) initiative in various medical disciplines aims to tackle the problem of loosely defined endpoints in surgical and oncological literature. It would complement the creation and implementation of a COS [9]. The reporting of a minimum number of core outcomes is critical to ensuring transparency in evaluating comparable trial data globally. It is a key factor in promoting equitable evidence synthesis and reducing research waste [69].
Finally, international consensus and the regular updating of a COS to guide future trials will be central to its utilisation. A UK‐based guideline may not be generalisable to the surgical or oncological needs in other demographic settings [69]. However, analysis of the GASTROS (COS for gastric cancer surgery) trial for gastric cancer demonstrated little disparity in the prioritisation of outcomes among international stakeholders, suggesting that core outcomes could similarly present a baseline for reporting expectations in oesophagectomy trials, except for a few that might be specific to region or country [70].
Ongoing and future RCTs may also provide scope for more up‐to‐date information to be disclosed, but we anticipate that improvement in the quality of reporting can be made only if there is concurrent uptake in the use of a COS. With a rise in the incidence of oesophageal carcinomas globally, the need to develop an international consensus on the outcomes of surgery to reliably share and analyse information in future studies becomes ever more crucial [71].
Strengths and Limitations
4.1
This review is the first of its kind comparing surgical studies in the field of oesophageal cancer treatment in the context of core outcome reporting. Its strength lies in the use of a consensus‐driven core outcome set together with a comparison of studies past and present, providing a comprehensive overview of this field.
The COS was primarily created to support the reporting of outcomes of RCTs. However, the inclusion of non‐randomised studies provides the breadth necessary for accurate representation of ongoing studies in this discipline. The first comprehensive multicentre RCT for oesophageal carcinoma resections was performed only 6 years ago [1]. The bulk of our review generally consisted of prospective cohort studies. This posed a challenge to sourcing high‐quality evidence from which to interpret results. Due to the high risk of morbidity and mortality, multicentre RCTs on oesophageal cancer resections face several ethical barriers to successful completion, especially when newer techniques and surgical modalities are being trialled. This is in addition to the investment of considerable time and resources. For this reason, we would not expect to see an immediate uptake of core outcome reporting in the period following its publication. Therefore our analysis of studies pre and post publication is merely indicative.
However, prospective studies can provide a snapshot of everyday clinical practice [63]. By improving the quality of non‐RCT comparative studies through standardisation, non‐randomised studies can still be beneficial in supplementing the results from RCTs to guide clinical practice [69].
The inclusion of English language studies alone may represent a limitation due to the high incidence and mortality associated with oesophageal cancer in Central and East Asia, with 90% incidence of the squamous cell type in these regions [72].
Finally, our review did not include multimodal treatment as the COS pertains primarily to surgical interventions undertaken. Surgical trials contain considerable heterogeneity in themselves and, therefore, were the focus of this study. Future work will endeavour to address both surgical and non‐surgical interventions.
Conclusion
5
Core outcomes following oesophagectomy that are of critical importance to healthcare professionals and patients are poorly reported in the literature. This picture has not improved over time. Further investment is required to increase the uptake of COS in oesophageal cancer research.
Author Contributions
Bilal Alkhaffaf conceptualised this review. Kerry Avery, Natalie Blencowe, and Rhiannon Macefield provided the search strategy and studies included in previous reviews on the topic. Nadia Matias conducted search, abstract and full paper screening, data acquisition and analysis and wrote the first draft of the manuscript. Anie Naqvi, Jack Thomson and Roukia Techache assisted as second reviewers in abstract screening, full paper review and data acquisition. All authors provided critical comments and approved the final version of the manuscript.
Funding
The authors received no specific funding for this work.
Conflicts of Interest
The authors declare no conflicts of interest.
Synopsis
This systematic review evaluates the extent to which core outcomes are reported in surgical trials and prospective studies of oesophageal cancer surgery. Among 58 eligible studies, no trial reported all 10 agreed‐upon core outcomes, with minimal improvement over time. These findings highlight the need for standardised outcome reporting to improve the quality and comparability of surgical research in oesophageal cancer.
Supporting information
PRISMA 2020 checklist complete.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1C. Mariette , S. R. Markar , T. S. Dabakuyo‐Yonli , et al., “Hybrid Minimally Invasive Esophagectomy For Esophageal Cancer,” New England Journal of Medicine 380, no. 2 (2019): 152–162, 10.1056/NEJ Moa 1805101.30625052 · doi ↗ · pubmed ↗
- 2A. Dubecz , I. Gall , N. Solymosi , et al., “Temporal Trends in long‐term survival and cure rates in esophageal cancer: a SEER database analysis,” Journal of Thoracic Oncology 7, no. 2 (2012): 443–447, 10.1097/JTO.0b 013e 3182397751.22173700 · doi ↗ · pubmed ↗
- 3A. W. Phillips , S. M. Lagarde , M. Navidi , B. Disep , and S. M. Griffin , “Impact of Extent of Lymphadenectomy On Survival, Post Neoadjuvant Chemotherapy and Transthoracic Esophagectomy,” Annals of Surgery 265, no. 4 (2017): 750–756, 10.1097/sla.0000000000001737.27467444 · doi ↗ · pubmed ↗
- 4L. Uttley , F. Campbell , M. Rhodes , A. Cantrell , H. Stegenga , and M. Lloyd‐Jones , “Minimally Invasive Oesophagectomy Versus Open Surgery: Is there An Advantage?,” Surgical Endoscopy 27, no. 3 (2013): 724–731, 10.1007/s 00464-012-2546-3.23052523 · doi ↗ · pubmed ↗
- 5B. Alkhaffaf , J. M. Blazeby , I. A. Bruce , and R. L. Morris , “Patient Priorities in Relation to Surgery for Gastric Cancer: Qualitative Interviews With Gastric Cancer Surgery Patients to Inform the Development of a Core Outcome Set,” BMJ Open 10, no. 2 (2020): e 034782, 10.1136/bmjopen-2019-034782.PMC 704496132051319 · doi ↗ · pubmed ↗
- 6K. N. L. Avery , K. A. Chalmers , S. T. Brookes , et al., “Development of a Core Outcome Set for Clinical Effectiveness Trials in Esophageal Cancer Resection Surgery,” Annals of Surgery 267, no. 4 (2018): 700–710, 10.1097/SLA.0000000000002204.28288055 PMC 5865486 · doi ↗ · pubmed ↗
- 7C. A. C. Prinsen , S. Vohra , M. R. Rose , et al., “Core Outcome Measures in Effectiveness Trials (COMET) Initiative: Protocol for an International Delphi Study to Achieve Consensus on how to Select Outcome Measurement Instruments for Outcomes Included in a “Core Outcome Set,” Trials 15, no. 1 (2014): 247, 10.1186/1745-6215-15-247.24962012 PMC 4082295 · doi ↗ · pubmed ↗
- 8M. J. Page , J. E. Mc Kenzie , P. M. Bossuyt , et al., “The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews,” BMJ 372 (2021): n 71. https://www.bmj.com/content/372/bmj.n 71.33782057 10.1136/bmj.n 71PMC 8005924 · doi ↗ · pubmed ↗