Carrington’s Disease: A Case Report
Siham Bouali, Sara Gartini, Meriem Rhazari, Afaf Thouil, Hatim Kouismi

TL;DR
This paper presents a case of Carrington’s disease, a rare lung condition, in a 59-year-old man who improved with corticosteroid treatment.
Contribution
The contribution is a detailed clinical case report of Carrington’s disease with successful treatment and radiological improvement.
Findings
The patient showed bilateral peripheral ground-glass opacities and blood eosinophilia.
Corticosteroid treatment led to complete symptom resolution and radiological improvement.
Bronchoalveolar lavage confirmed eosinophilic alveolitis.
Abstract
Idiopathic chronic eosinophilic pneumonia (ICEP), also known as Carrington’s disease, is a rare eosinophilic lung disorder characterized by pulmonary infiltrates with no identifiable cause. We report the case of a 59-year-old man with no significant medical history who presented with an eight-month history of progressive exertional dyspnea and a non-productive cough. Chest imaging showed bilateral peripheral ground-glass opacities. Laboratory evaluation revealed peripheral blood eosinophilia (2,000/mm³), and bronchoalveolar lavage demonstrated eosinophilic alveolitis (30%). The patient was treated with oral corticosteroids, resulting in complete symptom resolution and marked radiological improvement.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
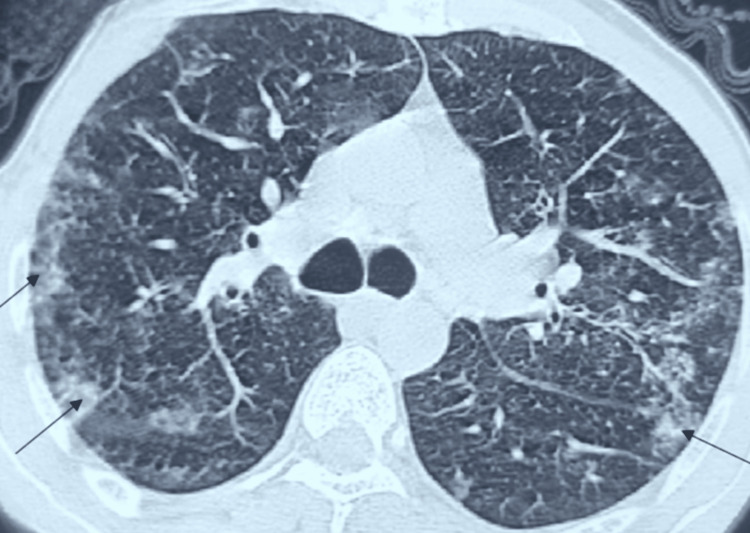 Figure 1
Figure 1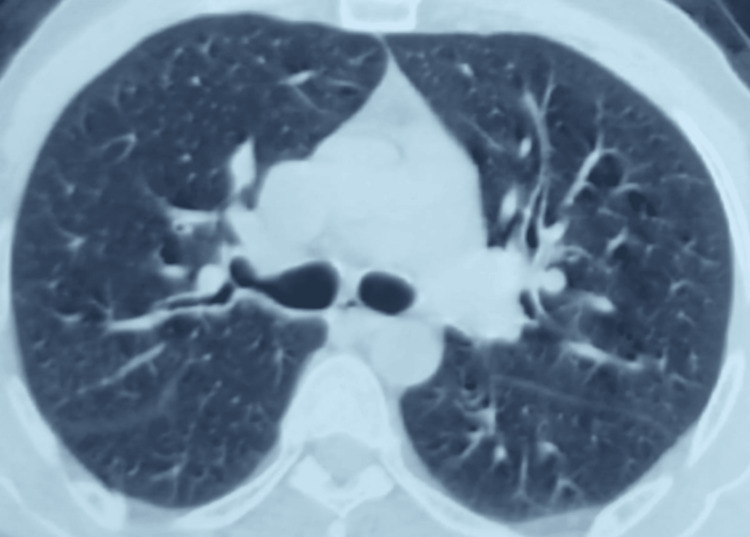 Figure 2
Figure 2| Test | Result | Reference range |
| Eosinophil count | 2,000/mm³ | 0–500/mm³ |
| C-reactive protein | 15 mg/L | <5.0 mg/L |
| Antinuclear antibody (ANA) | Negative | <80 |
| ANCA (p-ANCA/c-ANCA) | Negative | <20 |
| Total IgE | 50 IU/mL | 0–150 IU/mL |
|
| Negative | Titer < 1/320: non-significant reaction; titer = 1/320: doubtful reaction; titer ≥ 1/640: significant reaction in favor of deep aspergillosis |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInterstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Eosinophilic Disorders and Syndromes · Eosinophilic Esophagitis
Introduction
Idiopathic chronic eosinophilic pneumonia (ICEP) is a rare nosological entity among diffuse infiltrative lung diseases, with an estimated prevalence between 0% and 2.5% [1]. First described by Carrington et al. in 1969, this condition is characterized by an infiltration of the pulmonary parenchyma by inflammatory cellular elements with a predominant eosinophilic component, without an identifiable cause [2].
The pathogenesis of ICEP remains poorly understood, although it is often considered a localized pulmonary manifestation of an idiopathic hypereosinophilic syndrome (HES) [3]. Diagnosis relies on a combination of clinical, radiological, and biological findings, after the exclusion of other causes of eosinophilic pneumonias.
From a clinical standpoint, ICEP is particularly important to recognize in routine practice because of its potential for misdiagnosis. Its insidious presentation and frequent overlap with asthma or other eosinophilic lung diseases may lead to diagnostic delay. Early identification is essential, as ICEP typically demonstrates a rapid and dramatic response to systemic corticosteroid therapy, making timely diagnosis both prognostically and therapeutically significant. We present a typical case of ICEP in a middle-aged patient, illustrating the diagnostic and therapeutic specificities of this entity, and provide an updated review based on recent literature data.
Case presentation
A 59-year-old male patient with no significant past medical history, a non-smoker, without specific occupational exposures or recent medication use, presented for evaluation of grade II Modified Medical Research Council (MMRC) exertional dyspnea associated with a non-productive cough that had been progressing over eight months, and no evidence of extrapulmonary manifestations was noted at presentation. His general condition was preserved, with no reported weight loss or fever.
Upon admission, the patient was afebrile and hemodynamically and respiratorily stable (oxygen saturation 97% on room air). The clinical pleuropulmonary examination was unremarkable. Initial laboratory findings revealed peripheral blood hypereosinophilia at 2,000/mm³ (20% of the leukocyte differential), associated with a moderate inflammatory syndrome (C-reactive protein (CRP) 15 mg/L). Immunological workup (antinuclear antibodies, antineutrophil cytoplasmic antibodies (ANCA)) was negative.
An exhaustive etiological workup was performed to rule out the main secondary causes of pulmonary hypereosinophilia: parasitic and fungal serological testing (aspergillosis) returned negative; total immunoglobulin E (IgE) levels were within normal limits (Table 1).
Chest computed tomography revealed bilateral peripheral ground-glass opacities, predominantly in the upper lobes (Figure 1). Pulmonary function tests were within normal limits. Bronchoalveolar lavage (BAL) demonstrated increased total cellularity with an eosinophilic predominance of 25%, confirming the diagnosis of eosinophilic alveolitis.
Representative axial chest CT slices showing bilateral peripheral ground-glass opacities (black arrows)CT: computed tomography
Given this highly suggestive clinical, radiological, and biological presentation, a diagnosis of ICEP was established. Treatment with prednisolone at a dose of 1 mg/kg/day was initiated. Follow-up at three months showed complete resolution of respiratory symptoms and near-complete regression of the radiological lesions (Figure 2). A gradual tapering of the corticosteroid therapy was started, with regular clinical and radiological monitoring.
Representative axial chest CT images obtained after three months of corticosteroid therapy demonstrating near-complete radiological regression of the previously described lesionsCT: computed tomography
Discussion
ICEP, historically referred to as Carrington’s disease, is considered a distinct nosological entity characterized by pulmonary infiltration with a predominant eosinophilic component and no identifiable etiology. Although it has been interpreted as a localized manifestation of idiopathic HES [3], it is distinguished by its exclusive pulmonary tropism.
ICEP predominantly affects middle-aged adults, with peak incidence observed between 40 and 50 years of age. Pediatric cases remain exceptional but have been documented in the literature [4]. The clinical presentation typically follows a subacute or chronic course, combining respiratory manifestations (persistent cough, dyspnea-often wheezy and initially suggestive of asthma) with non-specific systemic symptoms (general malaise, low-grade fever). This non-specific nature accounts for the average diagnostic delay of four to six months reported in most case series [5].
The exclusively pulmonary nature of this condition is a crucial diagnostic feature, requiring the absence of extrapulmonary involvement to rule out differential diagnoses, particularly eosinophilic granulomatosis with polyangiitis (EGPA) (formerly Churg-Strauss syndrome) and other systemic vasculitis. The differential diagnosis can be organized into primary (indeterminate-origin) disorders, such as acute and chronic eosinophilic pneumonia, as well as systemic disease-associated entities like EGPA and chronic idiopathic HES, and secondary causes (determined-origin) including parasitic infections (e.g., ascariasis, tropical pulmonary eosinophilia, and strongyloidiasis), non-parasitic infections (e.g., coccidioidomycosis and tuberculosis), aspergillosis and allergic bronchopulmonary mycoses, and drug-, toxin-, or radiation-induced eosinophilic pneumonia. In addition, several other pulmonary conditions may involve the lungs with only occasional eosinophilia, including cryptogenic organizing pneumonia, pulmonary fibrosis, pulmonary Langerhans cell histiocytosis, sarcoidosis, granulomatosis with polyangiitis, malignancy-associated eosinophilia (e.g., eosinophilic leukemia and certain lymphomas), and transplant rejection [6].
Thoracic imaging, especially computed tomography, plays a central role in diagnosis. Typical findings include ground-glass opacities or alveolar consolidations with a peripheral and migratory distribution, predominantly affecting the upper and middle lobes [7]. The labile nature of these lesions under corticosteroid treatment is a hallmark feature.
Peripheral blood eosinophilia (>500/mm³), while highly suggestive, is not constant and may be absent in approximately 10% of cases [8]. BAL represents a key examination, consistently demonstrating eosinophilic alveolitis with an eosinophil percentage typically around 25%-40% [9].
Pulmonary function tests, while not essential for diagnosis, are of clear value for follow-up, particularly in patients with coexisting asthma. At initial evaluation, spirometry may reveal an obstructive or restrictive ventilatory defect [10]. The presence of early alveolar eosinophilia is frequently associated with bronchial obstruction [11]. Arterial blood gas analysis typically shows mild hypoxemia, in contrast to acute eosinophilic pneumonia, where acute respiratory failure is more common [5].
Histological confirmation by lung biopsy is not routinely required to establish the diagnosis [12]. When performed, biopsy typically shows infiltration of the interstitium and alveolar spaces by eosinophils and lymphocytes, without evidence of vasculitis or granuloma.
A positive diagnosis rests on the combination of four major criteria [13]: (1) the presence of subacute or chronic respiratory symptoms, often accompanied by systemic manifestations; (2) evidence of peripheral blood and/or alveolar eosinophilia; (3) pulmonary opacities that are predominantly alveolar on imaging; and (4) exclusion of other causes of eosinophilic pneumonia.
First-line therapy consists of systemic corticosteroids, with initial prednisone-equivalent doses typically in the range of 0.5 to 1 mg/kg/day [14]. Clinical response is usually rapid and dramatic and may even serve as a therapeutic diagnostic test. Complete radiological improvement is often observed as early as the second week of treatment [9].
However, the long-term course is frequently characterized by relapses during tapering of therapy (up to 50% of cases), necessitating prolonged treatment beyond one year in more than two-thirds of patients [5,14]. Rare cases of fibrosing progression have been described, justifying long-term surveillance [14]. It should be noted that spontaneous remission occurs in approximately 10% of cases [9].
Conclusions
ICEP remains a distinctive diagnostic and therapeutic entity within diffuse infiltrative lung diseases. Its diagnosis relies on a multidisciplinary approach that combines clinical features, characteristic imaging, and the presence of peripheral and/or alveolar eosinophilia. Corticosteroid therapy is the reference treatment, typically yielding an excellent initial response, but with a non-negligible risk of relapse, requiring a gradual taper and prolonged follow-up.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Eosinophilic pneumonias Allergy Cottin V Cordier JF 8418576020051593237210.1111/j.1398-9995.2005.00812.x · doi ↗ · pubmed ↗
- 2Chronic eosinophilic pneumonia N Engl J Med Carrington CB Addington WW Goff AM Madoff IM Marks A Schwaber JR Gaensler EA 7877982801969577363710.1056/NEJM 196904102801501 · doi ↗ · pubmed ↗
- 3Mepolizumab or placebo for eosinophilic granulomatosis with polyangiitis N Engl J Med Wechsler ME Akuthota P Jayne D 1921193237620172851460110.1056/NEJ Moa 1702079 PMC 5548295 · doi ↗ · pubmed ↗
- 4Pulmonary infiltrates with eosinophilia syndromes in children J Pediatr Oermann CM Panesar KS Langston C 35135813620001070069210.1067/mpd.2000.103350 · doi ↗ · pubmed ↗
- 5Eosinophilic lung diseases: a clinical, radiologic, and pathologic overview Radiographics Jeong YJ Kim KI Seo IJ 6176372720071749528210.1148/rg.273065051 · doi ↗ · pubmed ↗
- 6Guideline for the investigation and management of eosinophilia Br J Haematol Butt NM Lambert J Ali S 55357217620172811238810.1111/bjh.14488 · doi ↗ · pubmed ↗
- 7Eosinophilic lung diseases: diagnostic accuracy of thin-section CT in 111 patients Radiology Johkoh T Müller NL Akira M 77378021620001096671010.1148/radiology.216.3.r 00se 01773 · doi ↗ · pubmed ↗
- 8Eosinophilic lung diseases Am J Respir Crit Care Med Allen JN Davis WB 142314381501994795257110.1164/ajrccm.150.5.7952571 · doi ↗ · pubmed ↗