A Rare Cause of Neck Swelling: A Case Report and Review of Primary Pyomyositis of the Sternocleidomastoid
Daniel J Shepherd, Katerina Bopota, Wanyun Su, Andrew Barrett, Farzad Borumandi

TL;DR
A rare case of neck swelling caused by a bacterial infection in the sternocleidomastoid muscle is reported, highlighting the need for early diagnosis and treatment to prevent complications.
Contribution
This paper presents a rare case of primary pyomyositis in the sternocleidomastoid muscle and reviews existing literature on the topic.
Findings
Primary pyomyositis of the sternocleidomastoid muscle is rare and can lead to serious complications if not diagnosed early.
Surgical drainage and antimicrobial therapy led to a full recovery in the reported case.
Diagnostic delays are common, emphasizing the importance of early imaging in similar presentations.
Abstract
Primary pyomyositis is a rare bacterial infection of skeletal muscle occurring without a contiguous source of infection. Involvement of the sternocleidomastoid muscle (SCM) is exceptionally uncommon in temperate regions and may result in serious complications if diagnosis is delayed. We report a case of primary pyomyositis of the left SCM in a previously healthy 19-year-old male who presented with rapidly progressive neck pain and swelling nine days after minor blunt neck trauma. Contrast-enhanced computed tomography demonstrated an intramuscular SCM abscess with marked muscle oedema. Due to worsening pain and concern for evolving compartment syndrome, urgent surgical drainage and fasciotomy were performed, followed by delayed primary closure using a vessel-loop technique. The patient made a full functional recovery following antimicrobial therapy. To place this presentation in the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
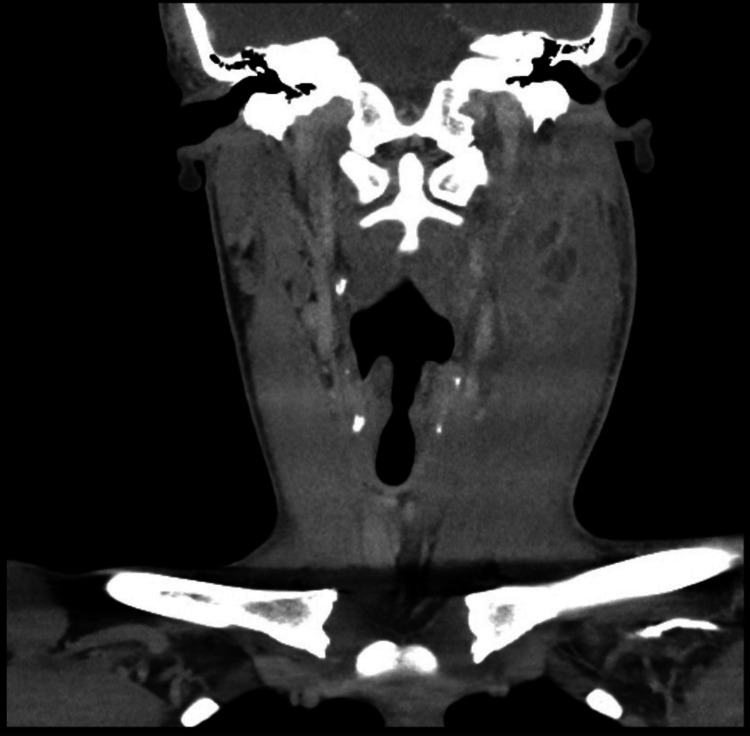 Figure 1
Figure 1 Figure 2
Figure 2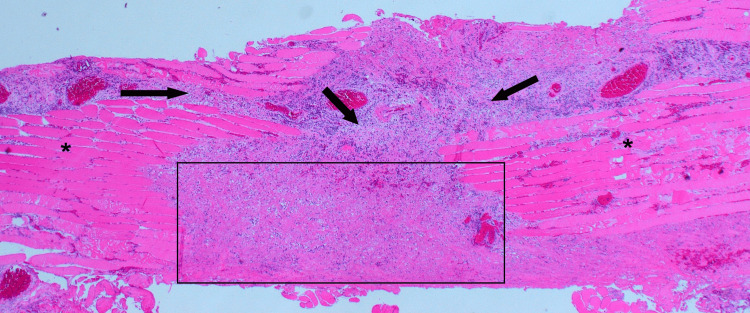 Figure 3
Figure 3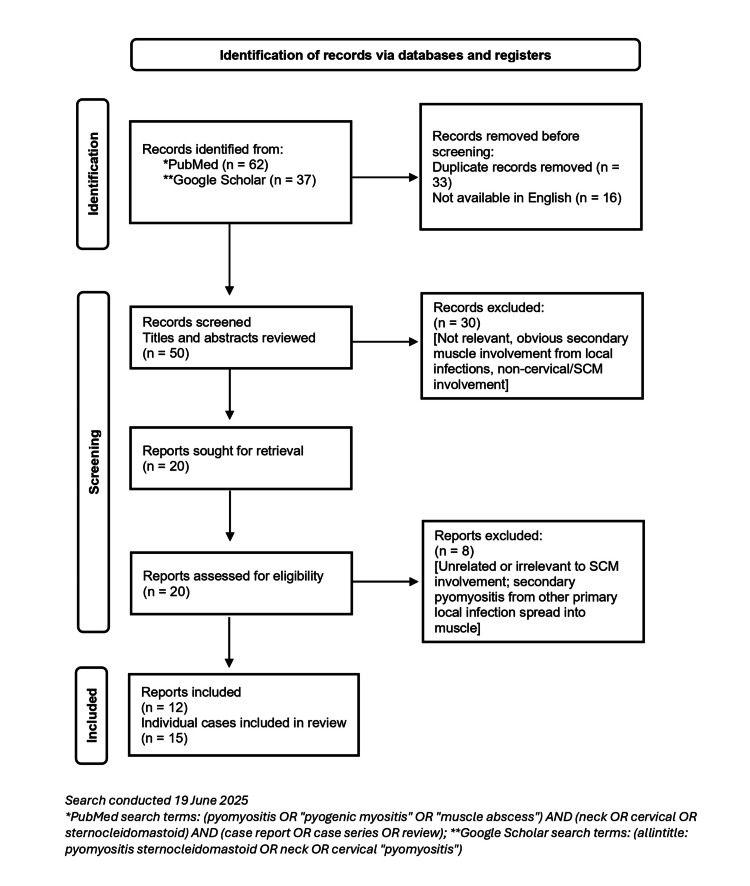 Figure 4
Figure 4| Day 0 (presentation) | Post-operative day 2 | Post-operative day 10 (discharge) | Six-week follow-up | Laboratory Reference Range | |
| C-Reactive Protein | 197 mg/L (H) | 50 mg/L (H) | 3 mg/L | <1 mg/L | < 5 mg/L |
| Total White Blood Cell Count | 15.5 × 10^9/L (H) | 20.3 × 10^9/L (H) | 9.9 × 10^9/L | 5.3 × 10^9/L | 4 – 10 × 10^9/L |
| Neutrophil Count | 12.2 × 10^9/L (H) | 18.6× 10^9/L (H) | 7.1 × 10^9/L | 2.4 × 10^9/L | 2 – 7 × 10^9/L |
| Age/Sex | Co-morbidities/Risk Factors | Clinical Presentation | Imaging | Microbiology | Management | Complications | Outcome | |
| *Gorospe et al., 2017 [ | 21 Male | None | Neck pain; tender mass; fever | CT: SCM abscess with descending mediastinitis | Group A Streptococcus | Surgical drainage of SCM & mediastinum; IV antibiotics | Mediastinitis | Full recovery |
| *Gosnell et al., 2016 [ | 48 Male | None | 1-week neck pain & swelling; fever; limited ROM | CT: abscess in SCM | Group A Streptococcus | Surgical drainage; IV co-amoxiclav (1.2g TDS) switched to benzylpenicillin (1.2g QDS x 4 days) then oral clindamycin (450mg QDS x 4 weeks) | None reported | Full recovery |
| **Soleh & Mohamad, 2010 [ | 72 Female | Poorly controlled type II DM | 1-week neck swelling, pain, fever | CT: abscess in SCM; parotid gland displaced | Klebsiella pneumoniae | Surgical drainage; IV co-amoxiclav and metronidazole | None reported | Full recovery; diabetes improved |
| *Collier et al., 2010 – Case 1 [ | Young adult Female | Recent travel to Africa (tropical region) | Fever, neck pain, no trauma | US/CT: diffuse SCM swelling, no abscess | No organism isolated | IV flucloxacillin + benzylpenicillin (2.4g QDS); no surgery (doubled dose of antibiotics) | None reported | Full recovery once the antibiotic dose increased |
| *Collier et al., 2010 – Case 2 [ | Young adult Female | Systemic Lupus Erythematosus (prednisolone); recent travel to Africa (tropical region) | Fever, neck pain, no trauma | US/CT: diffuse SCM inflammation, no abscess | Group A Streptococcus | IV flucloxacillin + benzylpenicillin; no surgery (doubled dose of antibiotics) | None reported | Full recovery once the antibiotic dose increased |
| **Snyder et al., 2018 [ | 22 Male | Blunt trauma to the neck 3 months prior | 3-month history of neck pain & swelling, weight loss, fevers, reduced ROM | MRI: SCM mass with medial spread to deep neck spaces | Staphylococcus epidermidis & Propionibacterium acnes | Surgical drainage, IV antibiotics, then oral (not specified) | None reported | Full recovery reported |
| *Rimell et al., 1992 [ | 43 Male | Rheumatoid Arthritis (prednisone + azathioprine); Type II DM | Neck pain & swelling following joint infection, progression to sepsis | CT: bilateral abscesses in SCM & mediastinal spread | Staphylococcus aureus | Multiple surgical debridements of neck & infected joints; IV vancomycin | Multiple arthrotomies of other infected joints | Recovered after a prolonged 12-week inpatient stay |
| *López-Rodríguez et al., 2008 [ | 46 Male | None | 7 days of difficulty elevating the arm, erythematous induration over the sternal manubrium | CT: abscesses in distal SCM & pectoralis major | Staphylococcus aureus | IV Cloxacillin (1 g QDS x 10 days) then oral Cloxacillin (1g QDS x 8 weeks) | None reported | Recovered (5 months of follow-up) |
| *Sakaida et al., 2016 [ | 62 Male | Poorly controlled type II diabetes mellitus (HbA1c 12.1%) | 1-week neck swelling, fever | US: swollen SCM with hypoechoic mass; CT: abscess in SCM | Streptococcus anginosus | US-guided aspiration + surgical drainage; IV antibiotics | None reported | Full recovery; discharged on day 16 |
| #Haroun et al., 2022 (Abstract only) [ | 55 Male | Liver cirrhosis; uncontrolled DM | 6-day neck swelling, no fever | CT: SCM abscess & early mediastinitis | Salmonella enterica | Surgical drainage; IV ceftriaxone changed to oral trimethoprim-sulfamethoxazole | Mediastinitis | Recovery; residual induration at 4 weeks |
| *Casillas et al., 2023 [ | 61 Male | Type II DM (HbA1c 8.5%) | 9 days of right neck pain/swelling, initially afebrile, later febrile | Initial CT: swelling only; repeat CT: abscess in SCM | Staphylococcus aureus | Initial oral doxycycline; later IV therapy + surgical drainage; 6-week daptomycin | None reported | Improved; discharged on antibiotics |
| *Fraser et al., 2024 (Abstract only) [ | Elderly Male | None | 7 days of worsening neck pain, swelling, fever | CT: collection within SCM | Not available | Surgical drainage & debridement; 14 days IV antibiotics | None reported | Recovery implied; followed up in clinic |
| **Neshat et al., 2024 – Case 3 [ | 41 Male | DM (unspecified) | Bilateral neck swelling, pain | CT: bilateral bulky SCM with peripheral enhancement and air foci | Klebsiella pneumoniae | Surgical drainage; cephalosporins, carbapenems (unclear dose/duration) | Delayed wound closure | Improved within 2 months |
| **Neshat et al., 2024 – Case 6 [ | 45 Male | DM (unspecified) | Bilateral neck swelling, dyspnea & dysphagia | CT: right SCM abscess, pectoralis major abscess, mediastinal spread | Bacteroides fragilis | Surgical drainage. Antibiotics (unclear antibiotic choice & dose/duration) | Mediastinitis | Recovery implied |
| **Neshat et al., 2024 – Case 7 [ | 48 Male | None | 1 week of neck pain, swelling, fever | CT: abscess in SCM; no mediastinal spread | Staphylococcus aureus | Surgical drainage; IV Co-amoxiclav (1.2g TDS) then benzylpenicillin (1.2g QDS x4 days), oral clindamycin (450mg QDS x 4 weeks) | None reported | Full recovery; no residual infection |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Osteomyelitis and Bone Disorders Research · Otolaryngology and Infectious Diseases
Introduction
Primary pyomyositis is a rare primary bacterial infection of skeletal muscle that arises in the absence of any contiguous skin, soft tissue, or bone infection [1]. Secondary pyomyositis is much more common and simply refers to muscle involvement as a direct extension from a nearby infected site [1,2]. Primary pyomyositis usually involves large muscle groups such as the quadriceps, iliopsoas, or gluteals. Involvement of a small cervical muscle, such as the sternocleidomastoid muscle (SCM), is exceedingly rare [1,2]. Awareness of this rare condition is important as, without any obvious regional source, diagnosis is often delayed. When occurring in the neck, severe complications can result, including descending mediastinitis, internal jugular vein thrombosis, compartment syndrome, and systemic sepsis [1-4].
The exact pathogenesis of primary pyomyositis is not fully understood, as healthy muscle is generally considered resistant to bacterial invasion [4,5]. It is hypothesised that transient bacteraemia allows seeding of bacteria to skeletal muscles where an intra-muscular infective process occurs, especially in the presence of local and systemic factors that allow for bacterial proliferation. Primary pyomyositis is well recognised in the tropics, typically affecting healthy individuals under the age of 20. It accounts for as much as 2% of all paediatric admissions in some regions, and up to 25% of cases occur in otherwise healthy individuals (often preceded by minor trauma or vigorous exercise [1,2,4,6]. In contrast, it is seldom encountered in temperate climates such as the United Kingdom (UK), where it is classically thought to occur in patients with underlying systemic immunosuppression such as diabetes, HIV, or chronic corticosteroid use [1,2,4].
Primary pyomyositis, if untreated, classically progresses through three distinct clinical stages: an initial local diffuse inflammatory stage; a local suppurative or abscess stage; and finally, to a systemic or septic stage [5,7]. Early recognition and intervention during the initial or suppurative stages are critical to prevent progression to life-threatening complications [1-4,6].
The most recent review of primary pyomyositis of this topic is limited in scope and predates several subsequent reports [2]. We therefore present a case of primary SCM pyomyositis in an immunocompetent young adult in the United Kingdom, highlighting the diagnostic challenges associated with this rare presentation. To place this case in context and better define the spectrum of disease, we also performed a review of all reported cases of primary SCM pyomyositis in the literature, characterising patient risk factors, clinical presentation, management strategies, and outcomes in accordance with PRISMA 2020 guidelines [8].
Case presentation
A 19-year-old previously healthy male rugby player presented with a two-day history of progressive left-sided neck pain and swelling, accompanied by rigors and malaise. Nine days prior to presentation, he had sustained minor blunt trauma to the left side of his neck while wrestling, with no immediate post-injury symptoms. He had no underlying medical conditions or relevant medical history.
On examination, the patient was febrile and tachycardic. The left side of the neck was markedly swollen, firm, and tender, extending from the mastoid region to approximately cervical levels II-III, with overlying erythema and severe restriction of neck movement. No alternative source of infection was identified on head and neck or systemic examination.
Laboratory investigations on presentation demonstrated a pronounced inflammatory response, with markedly elevated C-reactive protein, leukocytosis, and neutrophilia (Table 1), while muscle enzymes, including creatine kinase and lactate dehydrogenase, were within normal reference ranges. HIV testing and blood glucose screening were unremarkable. Contrast-enhanced computed tomography of the neck revealed a 3.9 × 2.7 cm rim-enhancing intramuscular collection within the medial aspect of the left sternocleidomastoid muscle at level II, with diffuse muscle oedema and associated reactive lymphadenopathy (Figure 1). No local or regional source for the intramuscular infection was identified.
Coronal view of contrast-enhanced CT of the neck of a 19-year-old male immunocompetent athlete, demonstrating intra-muscular collection within the left SCM in the absence of local or regional source.SCM: Sternocleidomastoid muscle
Empirical intravenous co-amoxiclav was commenced on admission. Despite 24 hours of antimicrobial therapy, the patient developed worsening neck pain and increasing pressure that was disproportionate to examination findings, while inflammatory markers remained elevated (Table 1), raising concern for evolving compartment syndrome. Urgent surgical drainage and fasciotomy were therefore undertaken via a linear cervical incision.
Intraoperatively, the SCM was firm and tense, with gross oedema. Fasciotomy along the lateral aspect revealed markedly inflamed muscle fibres that were visibly separated and friable, consistent with intramuscular necrosis. Copious purulent material was drained from a cleft cavity on the medial aspect of the muscle at level II. Pus and tissue samples were obtained for microbiological and histopathological analysis. The carotid sheath was mobilised from the medial SCM fascia, with both the internal jugular vein and carotid artery found to be patent.
Given the degree of muscle oedema and concern for sustained compartment pressure, delayed primary closure was performed using a vessel-loop “shoelace” technique to allow gradual approximation of the skin edges as swelling subsided (Figure 2), with definitive closure achieved on post-operative day five. Inflammatory markers improved rapidly following surgical intervention and normalised by the time of discharge on post-operative day 10, remaining within normal limits at six-week follow-up (Table 1).
Left neck wound closure using the vessel loop (“shoelace”) technique due to tense muscle oedema.
Histological examination confirmed features consistent with pyomyositis (Figure 3). Blood and intraoperative cultures were negative. The patient completed a 14-day course of co-amoxiclav. Follow-up ultrasound demonstrated complete resolution of the abscess, and at six-week review, the wound had healed fully with restoration of normal neck function.
Bundles of striated muscle (asterisks) disrupted by infiltrates of acute and chronic inflammatory cells (arrows) leading to localised muscle necrosis (rectangle). H&E, original magnification x 20.
Discussion
Primary pyomyositis of the SCM presenting in a young, immunocompetent patient is an exceptionally rare diagnosis in temperate regions such as the UK. In this case, minor blunt neck trauma was followed by rapidly progressive pain and swelling, highlighting the diagnostic and management challenges associated with this uncommon presentation. To place these findings in context, previously reported cases of primary SCM pyomyositis were identified through a structured review of the literature (strategy outlined in Figure 4). The key clinical features, management strategies, and outcomes from previously reported cases are summarised in Table 2, allowing direct comparison with the presentation and clinical course observed in our patient.
Flow diagram for review of the literature for sternocleidomastoid pyomyositis.
The literature review identified only 15 reported cases of primary SCM pyomyositis over the last 33 years, with just seven occurring in patients without identifiable immunosuppression (Table 2). This contrasts with the traditional perception of primary pyomyositis as a disease predominantly affecting immunocompromised individuals. Notably, only one previously reported case described primary SCM pyomyositis in an immunocompetent young adult following minor blunt neck trauma, mirroring the presentation observed in our patient [9].
Unlike primary pyomyositis affecting other muscle groups, diabetes mellitus, rather than haematological malignancy or HIV infection, appears to be the most frequently associated comorbidity. The condition also demonstrates a marked male predominance, with 12 of the 15 reported cases occurring in male patients, a finding that may relate to relative skeletal muscle mass. While SCM involvement remains rare in the literature, data from tropical regions suggest that healthy individuals with a history of trauma or strenuous physical activity represent a recognised subset of primary pyomyositis affecting other muscle groups [4-6].
Reported cases of primary SCM pyomyositis demonstrated a remarkably consistent clinical presentation, characterised by the rapid onset of painful lateral neck swelling, usually accompanied by fever and elevated inflammatory markers. Similar to our patient, several reports described pain that appeared disproportionate to early examination findings, which may represent an important diagnostic clue [1-4,6,7,14,16]. Nearly all cases presented in the suppurative stage, with an established intramuscular abscess within the SCM at the time of diagnosis. Early misdiagnosis was common, reflecting the unusual occurrence of an isolated intramuscular neck abscess in the absence of a local or regional source. Initial alternative diagnoses included parotid abscess, cellulitis, lymphadenitis, and neoplastic processes, with diagnostic delay in some cases resulting in serious complications, most notably descending mediastinitis [3,9].
Given the potentially life-threatening sequelae of deep neck infections, imaging was frequently guided by availability in the acute setting. Cross-sectional imaging played a central role in confirming the diagnosis and informing surgical planning. Contrast-enhanced CT was the most commonly utilised modality, consistently demonstrating rim-enhancing intramuscular collections with surrounding muscle oedema [1-3,12]. Although MRI is more sensitive for detecting early myositis, it was rarely used in reported cases of SCM pyomyositis, likely due to clinical urgency and resource constraints. Ultrasound was occasionally employed for initial assessment or image-guided aspiration but was insufficient as a sole imaging modality in cases with deep or extensive disease [12].
Once suppuration was confirmed, most patients underwent open surgical drainage, typically via transverse or longitudinal cervical incisions [1-3,7,9,10,12-16]. A small number of early cases without a discrete abscess were successfully managed with intravenous antibiotics alone [6,11]. Several cases were complicated by mediastinitis, reinforcing the importance of early diagnosis and timely intervention. In our patient, progressive pain, tense swelling, and concern for evolving compartment physiology prompted urgent surgical decompression. To our knowledge, compartment syndrome of the SCM has not previously been described. Decompression was achieved via longitudinal fasciotomy with delayed primary closure using a vessel-loop “shoelace” technique, a method commonly employed in limb fasciotomies but not previously reported in the management of SCM pyomyositis (Figure 2).
Microbiological findings across reported cases mirrored those seen in pyomyositis affecting other muscle groups, with staphylococcal and streptococcal species predominating [17-19]. Empirical antibiotic regimens generally targeted these organisms, most commonly using penicillin-based therapies, and several reports noted clinical improvement only after escalation or increased dosing [2,6,16]. Once culture results were available, antimicrobial therapy was adjusted and continued for a total duration of two to six weeks, depending on disease severity. Culture-negative cases, including ours, were not uncommon and likely reflect prior antibiotic exposure in the setting of a sensitive causative organism. The isolation of atypical pathogens in a minority of cases further emphasises the importance of microbiological sampling to guide targeted therapy.
When recognised and managed promptly, outcomes were favourable across all reported cases. In contrast, diagnostic delay was associated with significant morbidity, including descending mediastinitis, internal jugular vein thrombosis, and sepsis [1-6,10,13,16]. Despite these complications, no mortality has been reported. In our case, early imaging, timely surgical decompression, and appropriate antimicrobial therapy resulted in full functional recovery, consistent with outcomes reported in cases managed without delay.
Conclusions
Primary pyomyositis of the SCM, although rare, should be considered in the differential diagnosis of neck pain with swelling and fever, even in a young, immunocompetent patient. It is a common misconception that only immunocompromised patients are at risk for this condition, especially in temperate regions, such as the UK. This case and our literature review emphasise the diagnostic and therapeutic challenges of primary pyomyositis of the SCM. A high index of suspicion, early imaging and appropriate surgical and antimicrobial treatment are key to reducing morbidity and have been associated with favourable outcomes in these unusual and rare cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Descending necrotizing mediastinitis secondary to spontaneous sternocleidomastoid muscle abscess Arch Bronconeumol Gorospe Sarasúa L Valdebenito-Montecino AP Muñoz-Molina GM 1571585320172737428010.1016/j.arbres.2016.05.013 · doi ↗ · pubmed ↗
- 2Sternocleidomastoid pyomyositis Eur Ann Otorhinolaryngol Head Neck Dis Gosnell EJ Anwar B Varadarajan V Freeman S 27327513320162687958010.1016/j.anorl.2015.02.003 · doi ↗ · pubmed ↗
- 3Sternocleidomastoid pyomyositis mimicking parotid abscess Bangladesh J Med Sci Soleh MN Mohamad I 23824092010
- 4Primary pyomyositis J Bone Joint Surg Am Bickels J Ben-Sira L Kessler A Wientroub S 227722868420021247372110.2106/00004623-200212000-00024 · doi ↗ · pubmed ↗
- 5Tropical pyomyositis (myositis tropicans): current perspective Postgrad Med J Chauhan S Jain S Varma S Chauhan SS 2672708020041513831510.1136/pgmj.2003.009274 PMC 1743005 · doi ↗ · pubmed ↗
- 6Two cases of tropical pyomyositis of the sternocleidomastoid muscle occurring in the UK Br J Oral Maxillofac Surg Collier S Vig N Collier J 2162174820101996280010.1016/j.bjoms.2009.10.028 · doi ↗ · pubmed ↗
- 7A case confirming the progressive stages of pyomyositis J Pediatr Surg Flier S Dolgin SE Saphir RL Shlasko E Midulla P 155115533820031457708810.1016/s 0022-3468(03)00515-3 · doi ↗ · pubmed ↗
- 8PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews BMJ Page MJ Moher D Bossuyt PM 0372202110.1136/bmj.n 160PMC 800592533781993 · doi ↗ · pubmed ↗