A Comparison of Serum Lipase Levels and Clinical Outcome Trends in Hospitalized Pediatric Patients With Acute Pancreatitis: A Single-Center Retrospective Study
Sandeep K Puri, Amreen Masthan, David J Freestone, Andrew S Huang-Pacheco, Ruben E Quiros-Tejeira

TL;DR
This study found that tracking serum lipase levels in hospitalized children with pancreatitis does not improve outcomes and increases hospital costs.
Contribution
The study is the first to show that serial lipase monitoring in pediatric pancreatitis lacks prognostic value and increases healthcare costs.
Findings
Serial lipase levels did not correlate with symptom improvement in children with acute pancreatitis.
Patients with serial lipase testing had longer hospital stays and higher lab costs.
No significant difference in symptom resolution was found between groups.
Abstract
Background Serum lipase is widely used for the diagnosis of acute pancreatitis (AP) in pediatric patients; however, its prognostic value remains unclear. Despite limited evidence supporting serial monitoring, lipase levels are frequently trended during hospitalization. This study aimed to evaluate whether trending serum lipase levels are associated with improved clinical outcomes in children hospitalized with AP. Methodology We conducted a single-center retrospective chart review of pediatric patients (0-19 years) admitted with AP at Children’s Hospital & Medical Center between January 1, 2021, and December 31, 2022. Diagnosis was based on the INSPPIRE criteria. Patients were categorized into the following two groups: those who had serum lipase levels trended after diagnosis and those who did not. Clinical outcomes, including persistence of abdominal pain, nausea, and/or vomiting at…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
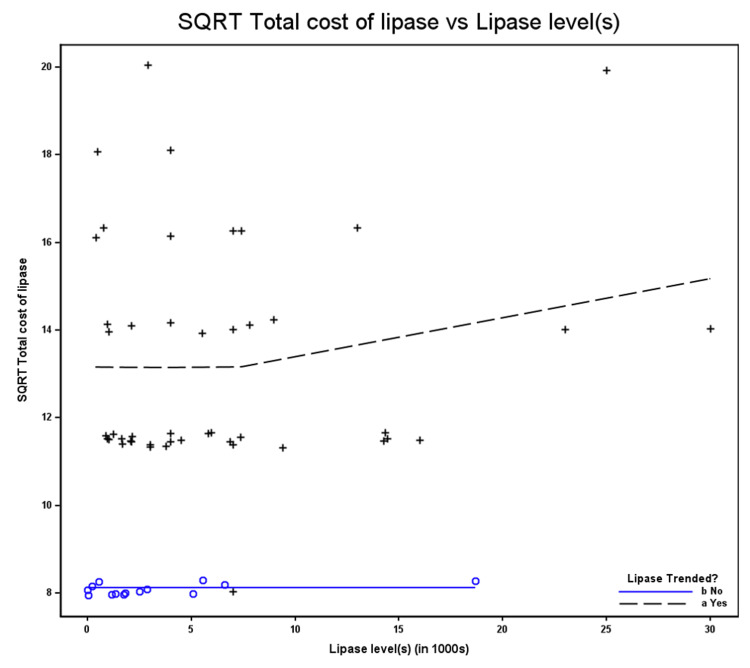 Figure 1
Figure 1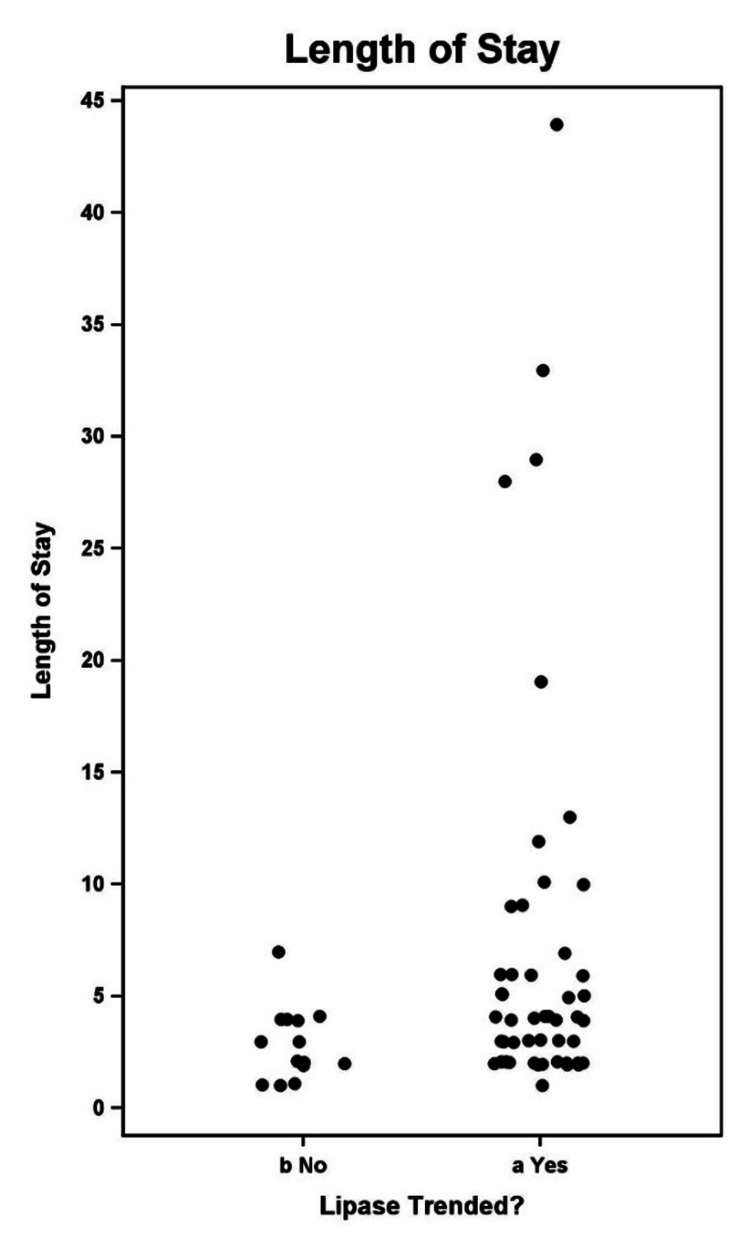 Figure 2
Figure 2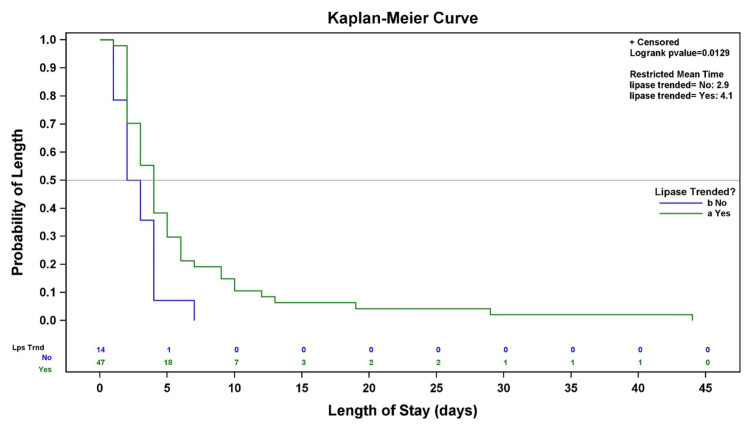 Figure 3
Figure 3| Patient demographics | n (%) | |
| Ethnicity | Hispanic | 9 (14.8) |
| Non-Hispanic | 52 (85.2) | |
| Sex | Female | 35 (57.4) |
| Male | 26 (42.6) | |
| Lipase trended? | No | 14 (23) |
| Yes | 47 (77) | |
| Pain management | Non-narcotics | 33 (54.1) |
| Narcotics | 28 (45.9) | |
| Type of IV fluids | Non LR | 25 (41) |
| LR | 36 (59) | |
| Risk factors/Complications | Yes | 47 (79.7) |
| No | 12 (20.3) | |
| Missing | 2 (0.03) | |
| Readmitted within 7 days? | No | 57 (93.4) |
| Yes | 4 (6.6) | |
| Clinical outcomes | Lipase trended | Lipase not trended | χ² (df) | P-value |
| Present, n (%) | 30 (63.8) | 11 (78.6) | 0.87 (1) | 0.35 |
| Absent, n (%) | 17 (36.2) | 3 (21.4) |
| Clinical outcomes | Lipase trended | Lipase not trended | χ² (df) | P-value |
| Yes, n (%) | 29 (82.9) | 5(100) | 0.30 (1) | 0.58 |
| No, n (%) | 6 (17.1) | 0 (0) |
| Clinical outcomes | Lipase trended | Lipase not trended | χ² (df) | P-value |
| Yes, n (%) | 25 (92.6) | 4 (100) | 0.12 (1) | 1.00 |
| No, n (%) | 2 (7.4) | 0 (0) |
| Clinical outcome | n | Median SQRT lipase level | Mean SQRT lipase level | Minimum SQRT lipase level | Maximum SQRT lipase level |
| Present | 40 | 63.2 | 63.5 | 4.1 | 173.2 |
| Absent | 20 | 62.4 | 72.2 | 6.2 | 158.1 |
| Clinical outcome | n | Median SQRT lipase level | Mean SQRT lipase level | Minimum SQRT lipase level | Maximum SQRT lipase level |
| Present | 33 | 63.2 | 73.1 | 6.2 | 173.2 |
| Absent | 6 | 54.3 | 55.7 | 27.5 | 83.7 |
| Clinical outcome | n | Median SQRT lipase level | Mean SQRT lipase level | Minimum SQRT lipase level | Maximum SQRT lipase level |
| Present | 29 | 63.2 | 74.5 | 6.2 | 173.2 |
| Absent | 2 | 87 | 87 | 53.9 | 120.1 |
| Clinical outcome at 48 hours | LR IV fluids | Non-LR IV fluids | χ² (df) | P-value |
| Present, n (%) | 28 (77.8) | 13 (52) | 3.78 (1) | 0.052 |
| Absent, n (%) | 8 (22.2) | 12 (48) |
| Clinical outcome at 96 hours | LR IV fluids | Non-LR IV fluids | χ² (df) | P-value |
| Present, n (%) | 23 (95.8) | 11 (68.8) | 4.78 (1) | 0.029 |
| Absent, n (%) | 1 (4.2) | 5 (31.3) |
| Clinical outcome at > 96 h | LR IV fluids | Non LR IV fluids | χ² (df) | P-value |
| Present, n (%) | 17 (100) | 12 (85.7) | 1.67 | 0.20 |
| Absent, n (%) | 0 (0) | 2 (14.3) |
| Outcomes at 48 hours | Narcotic pain management | Non-narcotic pain management | χ² (df) | P-value |
| Present, n (%) | 16 (57.1) | 25 (75.8) | 2.38 (1) | 0.17 |
| Absent, n (%) | 12 (42.9) | 8 (24.2) |
| Outcomes at 96 hours | Narcotic pain management | Non-narcotic pain management | χ² (df) | P-value |
| Present, n (%) | 18 (85.7) | 16 (84.2) | 0.01 (1) | 1.00 |
| Absent, n (%) | 3 (14.3) | 3 (15.8) |
| Outcomes at > 96 hours | Narcotic pain management | Non-narcotic pain management | χ² (df) | P-value |
| Present, n (%) | 16 (88.9) | 13 (100) | 1.33 (1) | 0.50 |
| Absent, n (%) | 2 (11.1) | 0 (0) |
| Lipase trended? | Mean |
| Yes | 182.4 |
| No | 66 |
| Difference | -116.4 |
| Lipase trended? | n | Mean |
| Yes | 47 | 184.0 |
| No | 14 | 66.0 |
| t-test summary for risk factors for AP | n | Nms | Median | Mean difference | Standard error | Lower limit | Upper limit | t | df | P-value (t-test) | P-value (Wilcoxon) |
| No risk | 12 | 0 | 59 | 63.53 | 7.54 | 46.94 | 80.12 | -0.13 | 56 | 0.9 | 0.85 |
| Yes | 46 | 1 | 62.4 | 65.04 | 5.75 | 53.45 | 76.62 | ||||
| Difference (row 1–row 2) | – | – | – | -1.51 | 11.94 | -25.43 | 22.41 |
| Risk factors for AP | Lipase trended, n (%) | Lipase not trended, n (%) | χ² (df) | P-value |
| Yes | 37 (78.7) | 10 (21.3) | 0.57 (1) | 0.45 |
| No | 8 (66.7) | 4 (33.3) |
| Complications | Frequency |
| Gallstones | 9 |
| IBD | 4 |
| DM | 5 |
| Biliary cyst | 3 |
| Multiple | 2 |
| Multiple comorbidities | 2 |
| Gallstone | Lipase trended, n (%) | Lipase not trended, n (%) | χ² (df) | P-value |
| Yes | 7 (77.8) | 2 (22.2) | 0.57 (1) | 1.00 |
| No | 29 (78.4) | 8 (21.6) |
| Lipase trended | N | Median | Mean |
| No | 14 | 2.50 | 2.86 |
| Yes | 47 | 4.00 | 6.09 |
| Test | χ² (df) | P-value |
| Log-rank | 6.1771 (1) | 0.0129 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatitis Pathology and Treatment · Dermatological and COVID-19 studies · COVID-19 Clinical Research Studies
Introduction
Acute pancreatitis (AP) is an increasingly recognized cause of hospitalizations in children and is associated with significant morbidity and healthcare utilization. The incidence of AP in children is rising. Etiologies include structural/anatomic, obstructive/biliary, trauma, infections, toxins, metabolic, systemic illnesses, inborn errors of metabolism, and genetic predispositions. The estimated incidence is approximately 1-3 cases per 10,000 children [1,2].
The diagnosis of pediatric AP is established using standardized criteria, most commonly the International Study Group of Pediatric Pancreatitis: In Search for a Cure (INSPPIRE) definition, which relies on a combination of characteristic abdominal pain, elevated pancreatic enzymes, and/or imaging findings. Once the diagnosis is made, management is largely supportive and guided by clinical status rather than biochemical normalization [3].
Serum lipase is a sensitive and specific marker for the diagnosis of AP and is routinely obtained at presentation. However, lipase levels may remain elevated for several days after symptom onset and do not reliably correlate with disease severity, clinical improvement, or resolution of symptoms. Despite this, repeat measurement of serum lipase after diagnosis remains common in hospitalized children, often driven by practice patterns rather than evidence. This practice may contribute to unnecessary laboratory testing, increased costs, and potential misalignment between laboratory trends and clinical decision‑making [2].
Existing adult and pediatric literature suggests that serial monitoring of pancreatic enzymes does not provide prognostic value once AP is diagnosed and should not guide clinical management. Nonetheless, data evaluating the association between lipase trending and symptom‑based clinical outcomes in pediatric AP remain limited, particularly in real‑world inpatient settings.
It is not uncommon for many institutions to trend serum lipase levels in hospitalized patients. Trending the serum lipase levels in hospitalized pediatric patients may put unnecessary financial and emotional burden on families, insurance companies, and institutions [4,5].
The primary objective of this study was to evaluate the association between serial serum lipase trending and short-term clinical outcomes in children hospitalized with AP. Clinical outcomes were defined as the presence of ongoing abdominal pain, nausea, and/or vomiting at 48 and 96 hours after admission. Secondary objectives included examining the association between lipase trending and hospital length of stay (LOS), opioid use, intravenous fluid type, and hospitalization costs. By focusing on clinically meaningful outcomes rather than biochemical normalization, this study aims to assess the utility of serial lipase testing in routine pediatric AP management.
Materials and methods
We identified 65 inpatient encounters at Children’s Nebraska (CHMC) from January 1, 2021, to December 31, 2022. The inclusion criteria were (1) patients aged 0-19 years hospitalized with AP; (2) patients seen by the PI, SI, or Pediatric GI team at CHMC; and (3) patients seen by other inpatient services at CHMC. The exclusion criteria were (1) patients aged 20 years or older and (2) patients who did not meet the inclusion criteria. A total of 61 patients met the inclusion criteria. Clinical outcomes were defined as the presence of ongoing abdominal pain, nausea, and/or vomiting at 48 and 96 hours after admission.
Data collection
The data collected were serum lipase levels, frequency of serum lipase testing during the same inpatient encounter, imaging studies, if performed, risk factors, complications, and body mass index (BMI) (Centers for Disease Control and Prevention guidelines for children ≥2 years; weight-for-age percentile for children <2 years). We also reviewed and compared the type of fluids (lactated Ringer’s vs. non-lactated Ringer’s), choice of pain medications (opioids vs. non-opioids), and correlation between serum lipase levels and risk factors. For this study, lipase trending was defined as more than one serum lipase measurement obtained after diagnosis. Patients with only a single lipase measurement were classified as not trended. One patient with a single repeat measurement obtained within the diagnostic window was categorized as trended based on the clinical context.
Statistical methods
All categorical data were summarized in two-way tables with counts and proportions. As a few cell counts were relatively small, to test statistical independence, Fisher’s exact test was applied. Continuous predictors with binary outcomes were evaluated with logistic regression. Continuous data, such as cost and lipase levels, were right-skewed, and a square root transformation was applied to improve distributional properties. The transformed continuous outcomes were evaluated with either a t-test or one-way analysis of variance. LOS was evaluated using a Kaplan-Meier analysis, including a graphical display. Statistical analyses were generated with the FREQ, LOGISTIC, and NPAR1WAY procedures from SAS/STAT software. Graphs were produced with the SGPLOT procedure from SAS/Base software, Version 9.4 (© 2016) of the SAS System for Windows (Cary, NC). For all inferential analyses, the corresponding test statistic (t, χ², or log-rank χ²) and degrees of freedom were reported alongside p-values.
Given the retrospective design, analyses were exploratory and intended to assess associations rather than causation. No multivariable adjustment was performed, and potential confounding by indication is addressed qualitatively in the Discussion.
Results
A total of 61 patient encounters met the study criteria. In 77% of patients (47/61), serum lipase level was trended. The number of patients available for outcome assessment decreased over time due to discharge before the 48- and 96-hour time points; therefore, analyses at each time point include only patients still hospitalized at that interval. Patient demographics and serum lipase measurement frequency are presented in Table 1.
Association between serial serum lipase trending and short‑term clinical outcomes
To assess the association between serial serum lipase trending and clinical outcomes, categorical outcomes at 48 and 96 hours were compared between groups using Fisher’s exact test, given small cell counts. At both time points, there was no statistically significant association between lipase trending and the presence of ongoing abdominal pain, nausea, and/or vomiting.
Although a higher percentage of patients without lipase trending had persistent clinical symptoms at both 48 and 96 hours compared to those with lipase trending, these differences were not statistically significant, as reflected by the corresponding p-values. These findings indicate that serial lipase trending was not associated with improved short‑term clinical outcomes in this cohort (Tables 2-4).
Association between serum lipase levels and short‑term clinical outcomes
Due to marked right skewness in serum lipase values, a square‑root transformation was applied before analysis to reduce the influence of extreme values. In the model evaluating clinical outcomes at 48 hours, the parameter estimate for transformed lipase level was negative, corresponding to an odds ratio of less than 1. This indicates a directional association in which higher lipase values were associated with a lower probability of persistent clinical symptoms; however, this association was not statistically significant (p = 0.397).
Model discrimination was assessed using the area under the receiver operating characteristic curve (AUC). The AUC was 0.539, indicating poor discriminatory ability and suggesting that serum lipase level alone had limited value in distinguishing between patients with and without persistent clinical outcomes in this cohort (Table 5).
At 96 hours, the interpretation was similar to that at 48 hours. The positive coefficient (0.0118) and an odds ratio greater than 1 (1.012) suggested a trend toward increased probability; however, this was not statistically significant (p = 0.352) (Table 6).
For the results >96 hours, interpretation was not performed due to the extremely small number of “absent” responses (n = 2) (Table 7).
Association between intravenous fluid type and short‑term clinical outcomes
Clinical outcomes at 48 and 96 hours were compared between patients receiving lactated Ringer’s and non-lactated Ringer’s intravenous fluids using Fisher’s exact test, given the presence of small cell counts in both tables. At both time points, the exact test p-values were relatively small, indicating a statistical association between fluid type and the presence of clinical outcomes.
At 48 hours, clinical outcomes were present in 77.8% (28/36) of patients who received lactated Ringer’s fluids compared with 52.0% (13/25) of those who received non-lactated Ringer’s fluids. Similarly, at 96 hours, clinical outcomes were present in 95.8% (23/24) of patients receiving lactated Ringer’s fluids compared with 68.8% (11/16) of those receiving non-lactated Ringer’s fluids.
These findings demonstrate an association between intravenous fluid type and short‑term clinical outcomes; however, given the retrospective design, small sample size, and potential confounding by indication, these results should be interpreted cautiously and not as evidence of a causal relationship (Tables 8-10).
Association between opioid use and short‑term clinical outcomes
Clinical outcomes at 48 and 96 hours were compared between patients receiving opioid versus non‑opioid analgesia using Fisher’s exact test, given small cell counts in both tables. At both time points, the exact test p-values were relatively large, indicating no statistically significant differences in clinical outcomes between the two analgesic groups.
At 48 hours, clinical outcomes were present in 57.1% (16/28) of patients who received opioids compared with 75.8% (25/33) of those who received non‑opioid analgesia. Although a similar pattern was observed at 96 hours, these differences did not reach statistical significance. Overall, opioid use was not statistically associated with short‑term clinical outcomes in this cohort (Tables 11-13).
Healthcare cost implications of guideline‑based management without serial serum lipase measurements
Figure 1 compares hospitalization costs between groups. In the figure, the solid blue line represents patients in whom serum lipase was not trended (n = 14), corresponding to a constant cost of $66, plotted on the square‑root scale (√66 ≈ 8.1). The dashed line represents the estimated trend in cost among patients whose serum lipase levels were trended (n = 47). Beyond a lipase level of 100 U/L (√lipase = 10), the curve demonstrates an upward pattern; however, this segment is based on a small number of observations and should be interpreted cautiously, as it may not reflect a true increase in cost with higher lipase levels.
Hospitalization costs between groups.
Because the cost data were right‑skewed, comparisons were performed on the square root-transformed cost scale. The group in which serum lipase was not trended exhibited no variability in cost (all values = $66), necessitating the use of an unequal‑variance model with variance for this group constrained near zero. Under these conditions, a conventional test statistic and corresponding p-value could not be calculated; therefore, the comparison is descriptive and reported as a mean difference on the transformed scale. Estimated means were subsequently back‑transformed to the original cost scale, and Table 14 presents the mean costs for the two lipase management groups.
In this sample, the estimated cost savings for the 47 patients who underwent serum lipase trending were calculated as 5,471. Because the non‑trended group exhibited no variability in cost (all values = $66), a formal test statistic and corresponding p-value could not be calculated; accordingly, all comparisons are descriptive.
The mean cost among the 47 patients with serum lipase trending was therefore descriptively compared with $66, representing the cost that would have been incurred had only a single serum lipase measurement been obtained. Mean costs are summarized in Table 15, along with the corresponding estimated cost savings under a single‑test strategy.
Based on the means of the data (not using a statistical model), the difference in the means is 118. Total cost savings is the difference, 118 x 47 = $5,546.
Association between serum lipase levels and the presence of one or more risk factors
The p-values in both the t-test and the Wilcoxon test are large (>0.85), indicating the means/medians are not different from each other (Table 16).
Table 16: Association between serum lipase levels and acute pancreatitis risk factors.Data are presented as mean ± SD or median (interquartile range), as appropriate. Group comparisons were performed using a two-sample t-test and a Wilcoxon rank-sum test. The t-test yielded t = −0.13 with 56 degrees of freedom (p = 0.90). Statistical significance was defined as p < 0.05.AP: acute pancreatitis
Gallstones were the most prevalent AP risk factor in the cohort. Both the two-sample t-test and the Wilcoxon rank-sum test demonstrated a statistically significant difference in square root-transformed serum lipase levels between patients with and without gallstones. The t-test yielded t = −3.62 with 44 degrees of freedom (p < 0.001), with concordant results from the Wilcoxon rank-sum test (p = 0.004).
Association between serum lipase trending and identified risk factors
Table 17 presents the association between serum lipase trending and risk factors. There was no statistical difference with a p-value of 0.45.
Table 18 presents the largest frequencies of risk factors and complications. Frequencies of these items are too small to consider. Table 19 presents the association between gallstones and serum lipase trending.
Association between hospital length of stay and frequency of serum lipase testing
Figure 2 illustrates the hospital LOS by lipase trending status.
Hospital length of stay by lipase trending status.
Length of hospital stay was longer in the lipase‑trended group, with a median of 4.0 days compared with 2.5 days and a mean of 6.09 days compared with 2.86 days. Due to the absence of analyzable individual‑level time‑to‑event data, no formal statistical hypothesis testing was performed (Table 20). Table 21 presents a comparison between the two groups.
Table 21: Comparison between two groups.Statistical significance was defined as p < 0.05.
Restricted mean survival time (RMST) estimates the average LOS within a specified follow‑up period using survival analysis methods and is related to, but distinct from, the median LOS. The RMST for patients with lipase trending was notably lower than the arithmetic mean LOS reported previously. This difference reflects the methodological distinction between RMST and the standard mean and is expected in this context, as LOS values are right‑skewed with a small number of prolonged hospitalizations, as illustrated in Figure 3.
Kaplan–Meier curve of hospital length of stay by serum lipase trending.Kaplan–Meier curves depict the probability of remaining hospitalized over time. Censoring is indicated by tick marks. Group comparisons were performed using the log‑rank test (χ² = 6.18, df = 1, p = 0.0129), demonstrating a statistically significant difference between groups. Restricted mean survival time (RMST) is also shown (lipase not trended: 2.9 days; lipase trended: 4.1 days). Statistical significance was defined as p < 0.05.
Discussion
This study evaluated the clinical utility of serial serum lipase measurement in hospitalized pediatric patients with AP. Consistent with existing literature, routine lipase trending after diagnosis was not associated with improvement in short‑term clinical outcomes [4].
Serum lipase elevation reflects pancreatic injury and is one of three diagnostic criteria for AP, along with characteristic abdominal pain and supportive imaging findings. Although lipase is often preferred over amylase because of greater specificity and, in some cases, diagnostic utility compared with imaging modalities, its role is primarily diagnostic. Lipase is present in several non‑pancreatic tissues [6] but is markedly more concentrated in pancreatic tissue [7]. Due to renal tubular reabsorption, serum lipase levels may remain elevated for prolonged periods, even after clinical recovery, limiting the usefulness of serial measurements in monitoring disease activity or severity [7].
In this retrospective cohort, serial lipase trending was not associated with symptom resolution at 48 or 96 hours. Although patients who underwent lipase trending had a longer hospital LOS, this finding represents an association rather than a causal relationship and is likely influenced by confounding by indication. Patients with more severe or persistent symptoms may have been more likely to undergo repeat testing and prolonged hospitalization, consistent with the survival and RMST analyses.
Clinical outcomes were based on symptom documentation in daily progress notes, which may introduce subjectivity and inter‑provider variability. Additionally, variability in patient availability at later time points reflects real‑world discharge practices and may limit outcome ascertainment.
Overall, these findings support limiting serum lipase testing to diagnostic purposes in pediatric AP and emphasize the importance of clinical assessment over biochemical monitoring. Future studies should focus on identifying more reliable clinical markers of disease progression, including standardized assessment of abdominal pain, as the absence of objective pain measures may contribute to continued reliance on laboratory trends [8].
This study is limited by its retrospective design, which restricts causal inference and is subject to documentation bias. The single‑center setting and relatively small sample size may limit generalizability. Decisions to trend serum lipase were based on individual clinician practice rather than a standardized protocol, introducing potential selection bias and confounding by clinical context. Variation in testing frequency precluded dose-response analyses, and some subgroup analyses were underpowered, particularly beyond 96 hours. Cost analyses were descriptive due to zero variance in the non‑trended group. Despite these limitations, the findings are consistent with existing literature and support guideline‑concordant management of pediatric AP.
Conclusions
In this single‑center retrospective study, serial serum lipase measurement after diagnosis of pediatric AP was not associated with improved short‑term clinical outcomes. These findings support limiting lipase testing to diagnostic purposes and emphasize the importance of clinical assessment over biochemical monitoring.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Serum lipase as an early predictor of severity in pediatric acute pancreatitis J Pediatr Gastroenterol Nutr Coffey MJ Nightingale S Ooi CY 602608562013 https://doi.org/10.1097/MPG.0b 013e 31828 b 36d 82340344110.1097/MPG.0b 013e 31828 b 36d 8 · doi ↗ · pubmed ↗
- 2Acute pancreatitis in children Am J Gastroenterol De Banto JR Goday PS Pedroso MR 172617319720021213502610.1111/j.1572-0241.2002.05833.x · doi ↗ · pubmed ↗
- 3Definitions of pediatric pancreatitis and survey of present clinical practices J Pediatr Gastroenterol Nutr Morinville VD Husain SZ Bai H 2612655520122235711710.1097/MPG.0b 013e 31824 f 1516 PMC 3626452 · doi ↗ · pubmed ↗
- 4An overused lab test? Evaluating repeat lipase in the management of acute pancreatitis and its impact on patient outcomes Am Gastroenterol Datta SK Husain SZ Bai H 01142019
- 5Cost of unnecessary amylase and lipase testing at multiple academic health systems Am J Clin Pathol Ritter JP Ghirimoldi FM Manuel LS 3463521532020 https://doi.org/10.1093/ajcp/aqz 1703167901110.1093/ajcp/aqz 170PMC 7315000 · doi ↗ · pubmed ↗
- 6Biochemistry, Lipase Pirahanchi Y Sharma S Treasure Island, FL Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 537346/30726031 · pubmed ↗
- 7Blood tests for acute pancreatitis Aust Prescr Basnayake C Ratnam D 1281303820152664864110.18773/austprescr.2015.043PMC 4653980 · doi ↗ · pubmed ↗
- 8The characteristics and prognostic role of acute abdominal on-admission pain in acute pancreatitis: a prospective cohort analysis of 1432 cases Eur J Pain Földi M Gede N Kiss S 6106232620223475817410.1002/ejp.1885 PMC 9299627 · doi ↗ · pubmed ↗