Established and emerging pharmacologic options and unmet needs in HFpEF and HFmrEF
Andrew J Sauer, Jozine M ter Maaten, Gianluigi Savarese

TL;DR
This paper reviews current and emerging treatments for heart failure with preserved or mildly reduced ejection fraction, highlighting the need for better therapies.
Contribution
The paper identifies new pharmacologic options and unmet needs in HFpEF and HFmrEF treatment.
Findings
Sodium–glucose cotransporter 2 inhibitors show promise for HFpEF and HFmrEF.
Finerenone reduced HF events and cardiovascular deaths in patients with ejection fraction ≥40%.
GLP-1 receptor agonists may benefit HFpEF patients with obesity.
Abstract
A decline in mortality due to heart failure (HF) with reduced ejection fraction (HFrEF) has been attributed to effective guideline-directed medical therapies. But few effective therapies are available for HF with preserved ejection fraction (HFpEF), despite a high burden of HF events, or for HF with mildly reduced ejection fraction (HFmrEF). Novel therapies are needed for these HF subtypes. Clinical trials have demonstrated the efficacy of sodium–glucose cotransporter 2 inhibitors for improving outcomes in HFpEF and HFmrEF. While renin–angiotensin system inhibitors, angiotensin receptor/neprilysin inhibitors, and steroidal mineralocorticoid receptor antagonists for HFpEF or HFmrEF have not demonstrated effects on primary trial outcomes, sub-analyses from large HF trials suggest they may reduce the risk of hospitalization for HF or mortality. Beta blockers may be beneficial for HFmrEF.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
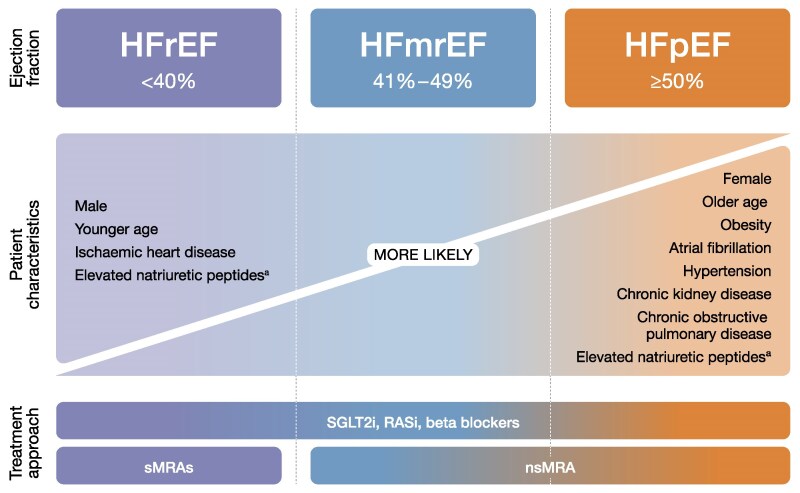 Figure 1
Figure 1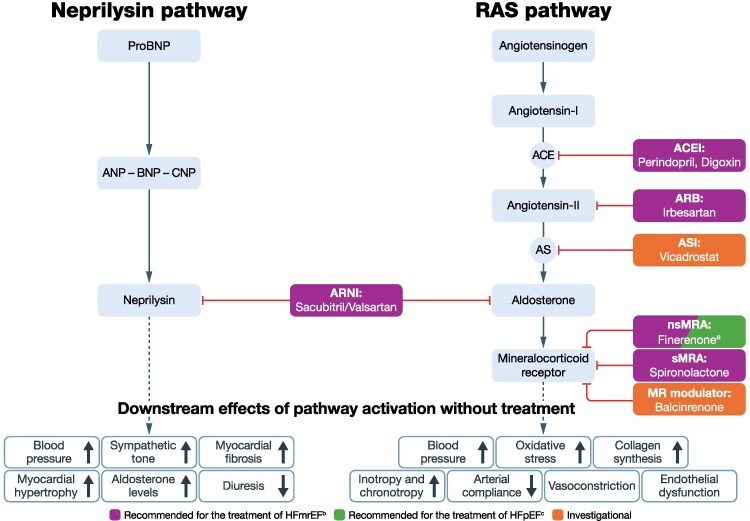 Figure 2
Figure 2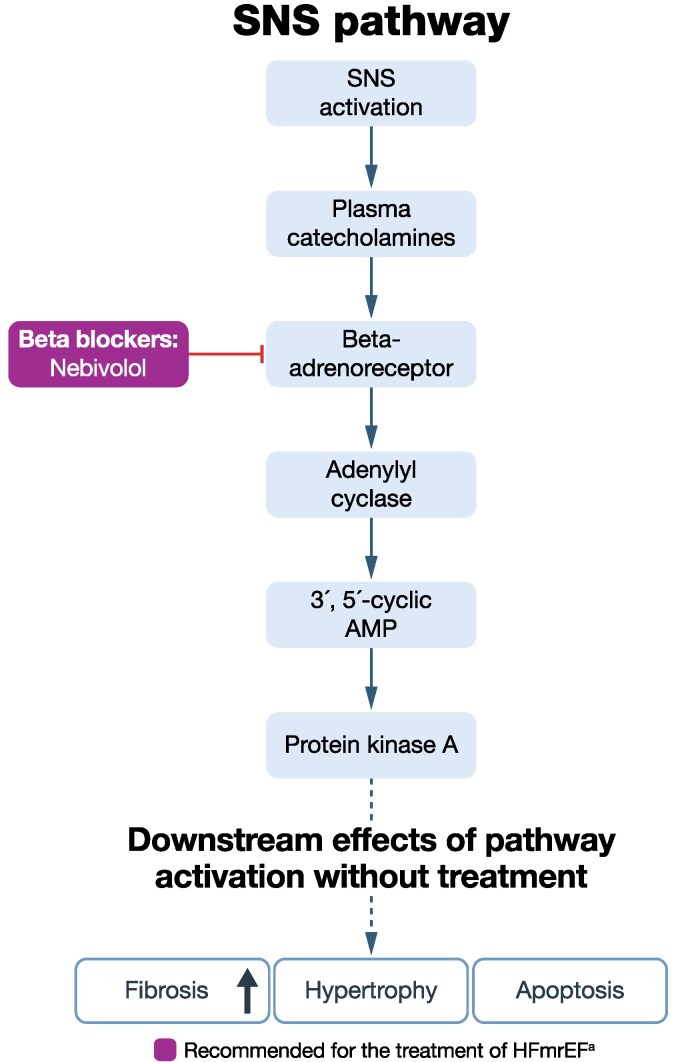 Figure 3
Figure 3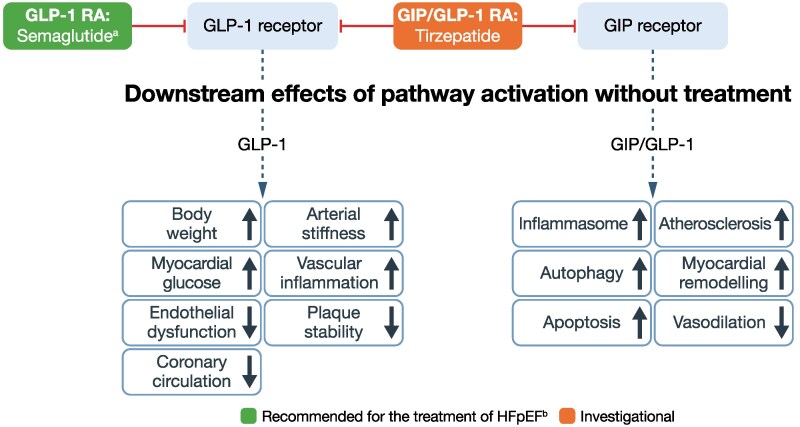 Figure 4
Figure 4 Figure 5
Figure 5| Therapy | Organization | Guidance | Class | Level |
|---|---|---|---|---|
| HFpEF | ||||
| RASi | ESC | No recommendation | — | — |
| AHA/ACC/HFSA | In selected people, an ARB may be considered to decrease hospitalizations, particularly among those with LVEF on the lower end of the spectrum | IIb | B-R | |
| JCS/JHFS | ARBs may be considered as an alternative to ARNI in symptomatic people with LVEF below normal to reduce the risk of HF hospitalizations | IIb | B-NR | |
| iCARDIO Alliance | Suggested to reduce the risk of HF hospitalization especially in people at the lower end of the LVEF spectrum | Suggested | — | |
| ARNI | ESC | No recommendation | — | — |
| AHA/ACC/HFSA | In selected people, it may be considered to decrease hospitalizations, particularly among those with LVEF on the lower end of the spectrum | IIb | B-R | |
| JCS/JHFS | May be considered in symptomatic people with LVEF below normal to reduce HF hospitalizations | IIa | B-NR | |
| iCARDIO Alliance | Recommended especially for people at the lower end of the LVEF spectrum. Particularly recommended in people with LVEF <58% and in women | Recommended | — | |
| Beta blocker | ESC | No recommendation | — | — |
| AHA/ACC/HFSA | No recommendation | — | — | |
| JCS/JHFS | No recommendation | — | — | |
| iCARDIO Alliance | No recommendation | — | — | |
| sMRA | ESC | No recommendation | — | — |
| AHA/ACC/HFSA | In selected people, it may be considered to decrease hospitalizations, particularly among those with LVEF on the lower end of the spectrum | IIb | B-R | |
| JCS/JHFS | Spironolactone or eplerenone may be considered in symptomatic people to reduce HF hospitalizations | IIb | B-NR | |
| iCARDIO Alliance | Spironolactone suggested to decrease HF hospitalization | Suggested | — | |
| nsMRA | ESC | No recommendation | — | — |
| AHA/ACC/HFSA | No recommendation | — | — | |
| JCS/JHFS | Finerenone may be considered in symptomatic people to reduce the risk of CV death or HF exacerbation events | IIa | B-R | |
| iCARDIO Alliance | Finerenone recommended to decrease HF hospitalization | Recommended | ||
| SGLT2i | ESC | Dapagliflozin or empagliflozin recommended to reduce the risk of HF hospitalization or CV death | I | A |
| AHA/ACC/HFSA | Can be beneficial for decreasing HF hospitalizations and CV mortality | IIa | B-R | |
| JCS/JHFS | Empagliflozin or dapagliflozin should be administered in symptomatic people to reduce the risk of HF hospitalization or CV death | I | A | |
| iCARDIO Alliance | Recommended to reduce the risk of HF hospitalization and CV death | Strongly recommended | — | |
| GLP-1 RA | ESC | No recommendation | — | — |
| AHA/ACC/HFSA | No recommendation | — | — | |
| JCS/JHFS | No recommendation | — | — | |
| iCARDIO Alliance | Tirzepatide or semaglutide recommended in people with obesity and HFpEF for weight loss and to improve symptoms and QoL | Strongly recommended | — | |
| Tirzepatide or semaglutide suggested in people with obesity and HFpEF to reduce the risk of HF hospitalization | Suggested | — | ||
| IV iron supplementation | ESC | No recommendation | — | — |
| AHA/ACC/HFSA | No recommendation | — | — | |
| JCS/JHFS | No recommendation | — | — | |
| iCARDIO Alliance | No recommendation | — | — | |
| HFmrEF | ||||
| RASi | ESC | May be considered to reduce the risk of HF hospitalization and death | IIb | C |
| AHA/ACC/HFSA | ARB may be considered to reduce the risk of HF hospitalization and CV mortality, particularly among people with LVEF on the lower end of the spectrum | IIb | B-NR | |
| JCS/JHFS | ARB may be considered in symptomatic people to reduce CV death or HF hospitalizations | IIb | B-NR | |
| ACEi may be considered in symptomatic people to reduce the risk of CV death or HF hospitalizations | IIb | C-LD | ||
| iCARDIO Alliance | Recommended for ambulatory people to reduce mortality and morbidity, if ARNI is contraindicated | Strongly recommended | — | |
| ARNI | ESC | May be considered to reduce the risk of HF hospitalization and death | IIb | C |
| AHA/ACC/HFSA | May be considered to reduce the risk of HF hospitalization and CV mortality, particularly among people with LVEF on the lower end of the spectrum | IIb | B-NR | |
| JCS/JHFS | May be considered in symptomatic people to reduce the risk of CV death or HF hospitalizations | IIa | B-NR | |
| iCARDIO Alliance | Recommended for ambulatory people to reduce mortality and morbidity | Strongly recommended | — | |
| Recommended as a replacement therapy to reduce mortality and morbidity in people with NYHA II and III class symptoms who can tolerate RASi | Strongly recommended | — | ||
| Beta blocker | ESC | May be considered to reduce the risk of HF hospitalization and death | IIb | C |
| AHA/ACC/HFSA | Evidence-based beta blockers for HFrEF may be considered to reduce the risk of HF hospitalization and CV mortality, particularly among people with LVEF on the lower end of the spectrum | IIb | B-NR | |
| JCS/JHFS | May be considered in symptomatic people to reduce the risk of CV death or HF hospitalizations | IIb | B-NR | |
| iCARDIO Alliance | Recommended (bisoprolol, carvedilol, nebivolol, or sustained-release metoprolol succinate) to reduce the risk of CV mortality and HF hospitalization | Strongly recommended | — | |
| sMRA | ESC | May be considered to reduce the risk of HF hospitalization and death | IIb | C |
| AHA/ACC/HFSA | May be considered to reduce the risk of HF hospitalization and CV mortality, particularly among people with LVEF on the lower end of the spectrum | IIb | B-NR | |
| JCS/JHFS | May be considered in symptomatic people to reduce risk of CV death or HF hospitalizations | IIb | B-NR | |
| iCARDIO Alliance | Recommended if eGFR >30 ml/min/1.73 m2 and potassium <5.0 mEq/L, to reduce morbidity and mortality | Strongly recommended | — | |
| nsMRA | ESC | No recommendation | — | — |
| AHA/ACC/HFSA | No recommendation | — | — | |
| JCS/JHFS | May be considered in symptomatic people to reduce the risk of CV death or HF exacerbation events | IIa | B-NR | |
| iCARDIO Alliance | Recommended if eGFR >30 ml/min/1.73 m2 and potassium <5.0 mEq/L, to reduce morbidity and mortality | Strongly recommended | — | |
| SGLT2i | ESC | Dapagliflozin or empagliflozin recommended to reduce the risk of HF hospitalization or CV death | I | A |
| AHA/ACC/HFSA | Can be beneficial for decreasing HF hospitalizations and CV mortality | IIa | B-R | |
| JCS/JHFS | Should be administered in symptomatic people to reduce the risk of HF hospitalization or CV death | I | A | |
| iCARDIO Alliance | Recommended to reduce the risk of HF hospitalization and CV death | Strongly recommended | ||
| GLP-1 RA | ESC | No recommendation | — | — |
| AHA/ACC/HFSA | No recommendation | — | — | |
| JCS/JHFS | No recommendation | — | — | |
| iCARDIO Alliance | No recommendation | — | — | |
| IV iron supplementation | ESC | Ferric carboxymaltose or ferric derisomaltose recommended in symptomatic people to reduce the risk of HF hospitalization | IIa | A |
| AHA/ACC/HFSA | No recommendation | — | — | |
| JCS/JHFS | No recommendation | — | — | |
| iCARDIO Alliance | IV ferric carboxymaltose or ferric derisomaltose recommended in iron deficiency to improve symptoms | Strongly recommended | — | |
| IV ferric carboxymaltose or ferric derisomaltose recommended in iron deficiency to reduce HF hospitalization and CV death | Recommended | — |
| Trial | Drug | Trial population and key inclusion criteria | Patient profile at baseline (mean, unless stated otherwise) | Key results (vs placebo unless stated otherwise) |
|---|---|---|---|---|
| RASi | ||||
| PEP-CHF | Perindopril | Diastolic HF | Age (median): 75.0 years | Primary outcome (composite of death or hospitalization) |
| CHARM-Preserved | Candesartan | HFpEF and HFmrEF | Age: 67.2 years | Primary outcome (composite of CV death or hospitalization for HF) during median follow-up of 36.6 months: |
| I-PRESERVE | Irbesartan | HFpEF | Age: 72.0 years | Primary outcome (composite of all-cause death or hospitalization for CV disease) during mean follow-up of 49.5 months: |
| DIG-Ancillary | Digoxin | HFpEF | Age: 66.8 years | Primary outcome (composite of HF mortality or hospitalization for HF) during mean follow-up of 37 months: |
| CHARM Programme | Candesartan | HFmrEF | Age: 65 years | Primary outcome (composite of CV death or hospitalization for HF) during mean follow-up of 2.9 years: |
| ARNI | ||||
| PARAGON-HF | Sacubitril/ | HFpEF | Age: 72.7 years | Primary outcome (composite of CV death or hospitalization for HF) during median follow up of 35 months: |
| PARAGON-HF and PARADIGM-HF pooled analysis | Sacubitril/ | HFpEF, HFmrEF, and HFrEF | Age: 68.0 years | Total hospitalization for HF and CV death by EF during median follow-up of 27 months and 35 months: |
| PARAGLIDE-HF | Sacubitril/ | HFpEF and HFpEF | Age: 71.5 years | Hierarchical composite endpoint (CV death, hospitalization for HF, urgent HF visits, change in NT-proBNP) during median follow-up of 5.9 months: |
| sMRA | ||||
| TOPCAT | Spironolactone | HFpEF | Age (median): 68.7 years | Primary outcome (death from CV causes, aborted cardiac arrest, or hospitalization for HF) during mean follow up of 3.3 years: |
| SPIRIT-HF | Spironolactone | HFpEF and HFmrEF | NA—trial terminated | Primary outcome: |
| SPIRRIT-HFpEF | Spironolactone/eplerenone | HFpEF and HFmrEF | NA—trial ongoing | Primary outcome: |
| Beta blocker | ||||
| Meta-analysis | Beta blockers | HFpEF, HFmrEF, and HFrEF | Age (median): | All-cause mortality by EF for 1.3 years median follow-up: |
| SGLT2i | ||||
| EMPEROR-Preserved | Empagliflozin | HFpEF and HFpEF | Age: 71.9 years | Primary outcome (composite of CV death or hospitalization for HF) for 26.2 months median follow-up: |
| DELIVER | Dapagliflozin | HFpEF and HFpEF | Age: 71.7 years | Primary outcome (composite of CV death or worsening HF [hospitalization or urgent visit]) for 2.3 years median follow-up: |
| PRESERVED-HF | Dapagliflozin | HFpEF | Age (median): 70.0 years | Improved KCCQ-CSS vs placebo at 12 weeks: |
| nsMRA | ||||
| FINEARTS-HF | Finerenone | HFpEF and HFmrEF | Age: 72.0 years | Primary outcome (composite of CV death or worsening HF [hospitalization or urgent visit]) for 32 months median follow-up: |
| REDEFINE-HF | Finerenone | HFpEF and HFpEF | NA—trial ongoing | Primary outcome: |
| CONFIRMATION-HF | Finerenone plus empagliflozin | HF | NA—trial ongoing | Primary outcome: |
| Trial | Drug | Trial population and key inclusion criteria | Patient profile at baseline (mean, unless stated otherwise) | Key outcomes or results (if available; vs placebo) |
|---|---|---|---|---|
| MR modulator | ||||
| MIRACLE | Balcinrenone plus dapagliflozin vs dapagliflozin | HF and CKD | Age: 72.3 years | Primary outcome—relative change in UACR from baseline to |
| BALANCED-HF | Balcinrenone plus dapagliflozin vs dapagliflozin | HF with recent HF event, | NA—trial ongoing | Primary outcome: |
| ASI | ||||
| EASi-HF | Vicadrostat plus empagliflozin vs empagliflozin | HFpEF and HFmrEF | NA—trial ongoing | Primary outcome: |
| GLP-1 RA | ||||
| STEP-HFpEF | Semaglutide | HFpEF and obesity | Age (median): 69.0 years | Primary outcome (mean change in KCCQ-CSS from baseline to Week 52): |
| STEP-HFpEF DM | Semaglutide | HFpEF, obesity, and T2D | Age (median): 69.0 years | Primary outcome (mean change in KCCQ-CSS from baseline to Week 52): |
| Pooled STEP-HFpEF and STEP-HFpEF DM analysis | Semaglutide | HFpEF and obesity | Age (median): 69.5 years | Secondary outcome (hierarchical composite including death, HF events, and differences in the change in KCCQ-CSS and 6MWD): |
| Dual GIP/GLP-1 RA | ||||
| SUMMIT | Tirzepatide | HFpEF and obesity | Age: 65.2 years | Primary outcome—composite of CV death or worsening HF: |
| Correction of iron deficiency | ||||
| FAIR-HFpEF | Ferric carboxymaltose | HFpEF iron deficiency | Age (median): 80 years | Difference vs placebo in change in 6MWD at Week 24: |
- —Bayer AG10.13039/100004326
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Treatment and Management · Heart Failure Treatment and Management · Cardiovascular Function and Risk Factors
Introduction
Heart failure (HF) is a complex clinical disease characterized by structural or functional impairment of ventricular filling or ejection of blood.^1^ Guidelines generally classify HF according to left ventricular ejection fraction (EF) into three subsets (phenotypes)^2–5^ that differ in terms of their characteristics and outcomes (Figure 1).^6–8^
Classification, characteristics, and treatment outcomes of HF by phenotype.2–4,6,7 HF, heart failure; HFmrEF, heart failure with mildly reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; nsMRA, non-steroidal mineralocorticoid receptor agonist; RASi, renin–angiotensin system inhibitor; SGLT2i, sodium–glucose cotransporter 2 inhibitor; sMRA, steroidal mineralocorticoid receptor antagonist. aElevated natriuretic peptides observed in HFrEF and HFpEF
HF is a significant global health concern that affects more than 64 million people worldwide, with a prevalence estimated at 1%–3% in the general population.^9,10^ In registry studies of hospitalized patients, approximately 15%–50% of the HF population have HF with preserved EF (HFpEF) and approximately 15%–25% have HF with mildly reduced EF (HFmrEF).^9^ However, the prevalence of HFpEF and HFmrEF may be much higher than that of HF with reduced EF (HFrEF) in the broader population. In addition, HFpEF and HFmrEF may be underdiagnosed because they have minimally reduced or preserved EF and milder symptoms than HFrEF.^7,11^ While the prevalence of HFrEF is stable and the incidence is falling because of better treatments for ischaemic heart disease, the prevalence of HFpEF is rising as a consequence of an ageing population, the increasing burden of comorbidities, and improved disease awareness, and may soon exceed that of HFrEF.^9,11–13^
HF is associated with high morbidity and mortality, poor quality of life, and a substantial burden to the healthcare system.^9^ In the SwedeHF registry of people with HF enrolled at hospital discharge or in an outpatient setting, the 5-year mortality rate was higher in participants with HFpEF (56%) compared with those with HFrEF (45%) or HFmrEF (46%).^14^ Cardiovascular (CV) causes accounted for most deaths (HFrEF, 65%; HFpEF, 59%; HFmrEF, 58%), with ischaemic heart disease being the leading cause of CV death in all HF phenotypes. Non-CV deaths accounted for a higher proportion of deaths in HFpEF (39%) and HFmrEF (41%) compared with HFrEF (33%; P < .001 for both comparisons), and cancer was the most common cause of non-CV death in all HF phenotypes.^14^
All-cause hospitalization rates and healthcare costs for HF are substantial and are generally higher for people with HFrEF than HFpEF.^15,16^ However, total healthcare costs associated with people with HFpEF may be higher than those with HFrEF due to the presence of comorbidities.^17^
HFrEF is well characterized, and since most prior HF trials have focused on this population, guideline-recommended therapies are now available.^2,4^ For people with HFpEF and HFmrEF, who face an equally high burden of HF events, there are limited available therapies and a substantial unmet need remains.^2–4,18^
The objective of this review is to evaluate the evidence base for the current pharmacologic treatment options for people with HFpEF and HFmrEF, discuss the unmet therapeutic needs in this population, and review emerging treatments and therapeutic approaches.
Evidence for current treatment options in people with HFpEF and HFmrEF (EF ≥40%)
Global guideline recommendations, as well as those for Europe, the USA, and Japan, describing current treatment options for people with HFpEF or HFmrEF are shown in Table 1, classified from I (strongest recommendation) to III (not recommended) based on the anticipated magnitude of treatment effect and benefit-to-risk ratio, with level of supporting evidence organized from A (highest) to C (lowest) based on scientific quality.^2–5,19^
Evidence from clinical trials supporting the effectiveness of current treatment options in people with HFpEF and HFmrEF is presented in Table 2.^20–45^ It should be noted that heterogeneity of trial populations regarding inclusion criteria (e.g. EF, age, hospitalization, and diuretic therapy), baseline characteristics, comorbidities, and background therapies limits comparisons between trials.
Renin–angiotensin system inhibitors (RASis), angiotensin receptor/neprilysin inhibitors (ARNIs), and steroidal mineralocorticoid receptor (MR) antagonists (sMRAs)
RASis target the neurohormonal activation that occurs in HF in response to a fall in cardiac output.^46^ Renin–angiotensin system activation is a key feature of HFrEF,^47^ is related to hypertension, which is prevalent in HFpEF,^48^ and is an important contributory factor in the development of CV disease in people with chronic kidney disease (CKD).^49^ Despite this, none of the large randomized controlled trials conducted with RASis, ARNIs, or sMRAs in people with HFpEF, including PEP-CHF (perindopril), CHARM-Preserved (candesartan), I-PRESERVE (irbesartan), TOPCAT (spironolactone), DIG-Ancillary (digoxin), and PARAGON-HF (sacubitril/valsartan), achieved their primary endpoint (Table 2).^20–22,24,26,29^ Heterogeneity of the trial populations increases complexity in evaluating the reasons for the failed primary endpoints when comparing the trials. However, perindopril reduced hospitalization for HF compared with placebo in PEP-CHF.^20^ A similar trend was shown in the PARAGON-HF trial, although no statistically significant difference was seen (Table 2).^26^ Subgroup analyses of I-PRESERVE and TOPCAT suggest that people with HFpEF and comorbidities, such as obesity and diabetes, may derive greater benefit from RASis or sMRA therapy than those with HFpEF without these comorbidities (Table 2).^23,32^
There have been no dedicated trials for RASis, ARNIs, and sMRAs in HFmrEF; however, sub-analyses from the CHARM, PARAGON-HF, and TOPCAT trials have suggested some benefit in this population.^25,26,29^
In CHARM, candesartan reduced the primary outcome (CV death or HF hospitalization) in participants with HFmrEF (17% of the CHARM programme population) as compared with placebo (Table 2).^25^
In PARAGON-HF, sacubitril/valsartan did not significantly reduce hospitalizations for HF and CV death compared with valsartan overall; however, a greater benefit was observed in people with an EF of 45%–57% compared with those with an EF of >57% (Table 2).^26^ A pooled analysis of PARAGON-HF (EF eligibility, ≥45%) and PARADIGM-HF (EF eligibility, ≤40%) suggested some benefit of sacubitril/valsartan in people with HFmrEF in terms of first hospitalization for HF or CV death (HR: 0.81, 95% CI 0.64–1.03; P = .09).^27^ In the PARAGLIDE-HF study, although no significant clinical benefit was seen in the overall cohort of participants with EF >40%, when limiting the analysis to those with EF ≤60% a notable benefit was observed (Table 2).^28^
In TOPCAT, spironolactone did not significantly reduce the risk of the primary composite outcome of CV death, aborted cardiac arrest, or hospitalization for HF compared with placebo in people with an EF ≥45% (15% with EF ≥45 to <50%), over a mean follow-up of 3 years.^29^ However, people with an EF at the lower end of the spectrum (<50%) were more likely to benefit from spironolactone with respect to the primary composite outcome and hospitalization for HF (Table 2).^30^
Post-hoc analyses of data from TOPCAT demonstrated variations in baseline characteristics, response to spironolactone, and spironolactone metabolite concentrations between the two regions (Russia and Georgia compared with the Americas [the USA, Canada, Brazil, and Argentina]).^31,50^ Taken together, these findings called into question the study’s conduct at some sites, and suggested that a significant proportion of participants in Russia/Georgia randomized to spironolactone may not have had HF or taken randomized treatment.^50^ In contrast with the finding in the study population overall, the rate of the primary outcome was nominally significantly reduced by spironolactone compared with placebo in the Americas (HR: 0.82, 95% CI 0.69–0.98; P = .026).^31^
An individual patient-level meta-analysis of four randomized controlled trials, including TOPCAT, demonstrated that sMRAs reduced the risk of HF hospitalization or CV death compared with placebo in people with HF across the EF spectrum (HR: 0.77, 95% CI 0.72–0.83).^51^
The SPIRIT-HF and SPIRRIT-HFpEF studies were designed to assess whether the initiation of spironolactone or eplerenone improves outcomes in people with HFpEF and HFmrEF (Table 2). SPIRIT-HF, a double-blind, randomized, placebo-controlled interventional Phase 3 study, enrolled 743 participants but was terminated.^33^ SPIRRIT-HFpEF is a registry-randomized trial evaluating data from 2400 participants; both studies have a primary composite endpoint of hospitalization for HF or CV death.^34^ A positive finding in SPIRRIT-HFpEF would provide additional support for the use of sMRAs in people with HFpEF and HFmrEF.
Most sMRAs are associated with hyperkalaemia due to the role of aldosterone in controlling potassium homeostasis.^52^ In TOPCAT, spironolactone was associated with a doubling of the incidence of hyperkalaemia (potassium ≥5.5 mmol/L 18.7 vs 9.1% in the placebo group) in people with HFpEF or HFmrEF.^29^ The incidence of hypokalaemia (potassium <3.5 mmol/L), which is also associated with increased risk of mortality,^53^ was reduced by spironolactone compared with placebo (16.2 vs 22.9%, respectively).^29^ Serum potassium should be monitored within 1 week of treatment initiation and during treatment with these agents.^54,55^ Hyperkalaemia mitigation strategies might include combining an sMRA with an SGLT2i, use of potassium binders, and use of loop or thiazide diuretics.^56^
Based on the findings of the studies described above, global guidelines and those in the USA and Japan recommend that angiotensin receptor blockers, ARNIs, or sMRAs may be considered for specific groups of people with HFpEF, whereas there is no such recommendation in Europe (Table 1).^2–5,19^ For people with HFmrEF, guidelines state that treatment with RASis, ARNIs, or sMRAs may be considered to reduce the risk of hospitalization or death (Table 1).^2–5,19^
Beta blockers
A meta-analysis of 11 studies demonstrated no significant improvement in all-cause and CV mortality with beta blockers compared with placebo in people with HF and EF ≥50% (Table 2).^35^ In addition, beta blockers did not improve prognosis in people with HFpEF and atrial fibrillation, a frequent comorbidity of HFpEF.^35^ Observational data from a large, real-world cohort of outpatients ≥65 years of age found that beta blocker use was associated with an increased risk of hospitalization in people with HFpEF, notably when EF exceeded 60%.^57^ The lack of supporting data means that guidelines do not include recommendations for the use of beta blockers in people with HFpEF (Table 1).^2,4,5,19^
The meta-analysis of studies of beta blockers in HF demonstrated a significant reduction in all-cause and CV mortality compared with placebo in those with an EF of 40%–49% (Table 2).^35^ As many people with HFmrEF may have another CV indication, HF guidelines state that use of a beta blocker may be considered to reduce the risk of hospitalization for HF or death in people with HFmrEF (Table 1).^2,4,19^
Sodium–glucose cotransporter 2 inhibitors (SGLT2is)
Of the currently approved HF therapies, only SGLT2is have convincingly shown a benefit in people with EF >40%.^36,38,58^ In the EMPEROR-Preserved trial in people with HF and an EF >40% (33.1% with EF 40%–49%), empagliflozin was associated with a 21% reduction in the primary composite endpoint of hospitalization for HF or CV death compared with placebo (P < .001; Table 2), an effect that was consistent in people with HFpEF and HFmrEF.^36,59^ DELIVER assessed the efficacy and safety of dapagliflozin in people with HFpEF and HFmrEF (33.8% with EF 40% to ≤49%).^38^ Dapagliflozin was associated with an 18% reduction (P < .001) for the primary composite endpoint of worsening HF or CV death compared with placebo, this effect was consistent regardless of EF at baseline (Table 2).^38^
SGLT2is have also been reported to improve patient-reported outcomes. The PRESERVED-HF study showed that dapagliflozin improved the Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CSS; ≥5 points is clinically meaningful) and 6-minute walk distance compared with placebo in participants with HFpEF (Table 2).^39,60^
Analysis of data from eight studies that evaluated the effect of SGLT2is on adverse events (AEs) in people with HFmrEF or HFpEF showed that rates of volume depletion, kidney injury, drug discontinuation, ketoacidosis, hypoglycaemia, amputation, and urinary tract infections were similar compared with placebo.^58^ Furthermore, the risk of serious AEs was significantly lower in those receiving SGLT2is vs placebo (risk ratio: 0.94, 95% CI 0.91–0.98; P = .07).^58^
Supported by the findings of the EMPA-REG OUTCOME,^61^ EMPA-KIDNEY,^62^ DECLARE-TIMI 58,^63^ DAPA-CKD,^64^ CANVAS,^65^ and CREDENCE^66^ studies, SGLT2is are also recommended by the American Diabetes Association and the Kidney Disease: Improving Global Outcomes CKD Work Group for reducing CV risk and progression of CKD in people with type 2 diabetes (T2D) and CKD,^67–69^ conditions that frequently coexist with HFpEF and HFmrEF.^70–72^
Non-steroidal MR antagonists (nsMRA)
Finerenone is an nsMRA with distinct physiochemical properties from sMRAs. Compared with spironolactone and eplerenone, it exhibits higher selectivity for the MR, a shorter half-life, lacks active metabolites, achieves equal distribution between the heart and kidneys, and utilizes distinct transcriptional coactivators.^73,74^ Finerenone acts as an inverse agonist ligand, reducing MR cofactor recruitment even in the absence of aldosterone.^73^ Additionally, finerenone may offer more potent anti-inflammatory and anti-fibrotic effects related to cardiac MR activation due to its more balanced distribution between the heart and kidneys.^73,74^ Finerenone's shorter plasma half-life compared to sMRAs may help lower the risk of hyperkalaemia.^73^ Finerenone is indicated to reduce CV risk and CKD progression in people with CKD associated with T2D^75^ following the results of the FIDELIO-DKD and FIGARO-DKD studies.^76,77^ It has recently been approved for patients with HF and left ventricular EF ≥40% (i.e. HFpEF and HFmrEF) in the USA;^75^ approval for patients with HF in Europe has not yet been granted.
In FINEARTS-HF, finerenone was associated with a 16% reduction (P = .007) in the primary composite endpoint of total (first and recurrent) HF events and CV death in participants with HFpEF and HFmrEF (36.2% with EF <50%); this effect was consistent in people with an EF of <60% and ≥60% (Table 2).^40^ Hyperkalaemia (potassium >5.5 mmol/L) occurred more frequently in the finerenone group (14.3 vs 6.9% with placebo). Similarly, investigator-reported cases of hyperkalaemia were higher with finerenone (9.7 vs 4.2% with placebo). Hospitalizations due to hyperkalaemia were rare in both groups (0.5% in the finerenone group vs 0.2% in the placebo group), with no events leading to death.^40^
A prespecified analysis of FINEARTS-HF demonstrated that the benefit of finerenone was similar in participants treated or not treated with SGLT2is, including in participants randomized to finerenone who were newly initiated on an SGLT2i during the trial.^43^ A separate prespecified secondary analysis of the 817 participants receiving finerenone and a SGLT2i showed a lifetime gain in event-free survival observed for a 65-year-old participant receiving finerenone plus a SGLT2i (3.1 years [95% CI 0.1–6.0, P = .04] vs 1.8 years [95% CI 0.5–3.1; P = .009] in a participant not taking a SGLT2i at baseline).^78^ In an analysis of three clinical trials, including FINEARTS-HF, combined use of finerenone and a SGLT2i reduced the risk of CV death or first worsening HF event by 31% (HR 0.69; 95% CI 0.59–0.81).^79^ For a 65-year-old patient, this translated to an additional 3.6 years (95% CI 2.0–5.2) free from an HF event or CV death.^79^
Ongoing trials^44,45,80^ will explore the efficacy and safety of finerenone in people hospitalized with acute decompensated HF and an EF ≥40% (REDEFINE-HF)^44^ and in combination with empagliflozin in people hospitalized (or recently discharged) for HF across the EF spectrum (CONFIRMATION-HF).^45^
The iCARDIO Alliance guidelines recommend finerenone to reduce HF hospitalizations in people with HFpEF, and in people with HFmrEF, estimated glomerular filtration rate >30 ml/min/1.73 m^2^, and potassium <5.0 mEq/L to reduce morbidity and mortality (Table 1).^19^ Guidelines in Japan recommend finerenone in people with symptomatic HF (Class IIa recommendation) to reduce the risk of CV death (HFpEF and HFmrEF) and HF hospitalization (HFpEF) or HF exacerbation events (HFmrEF).^5^ The European Society of Cardiology (ESC) and American College of Cardiology American Heart Association Heart Failure Society of America do not yet give a formal recommendation.
Intravenous iron supplementation
Iron deficiency affects up to 50% of people with HF.^81^ ESC and iCardio Alliance guidelines recommend the use of intravenous iron supplementation with ferric carboxymaltose or ferric derisomaltose to correct iron deficiency in HFmrEF,^3,19^ while no recommendations are made for iron supplementation in HFpEF (Table 1).
Unmet need in people with HFmrEF and HFpEF (with EF ≥40%)
Even with guideline-recommended therapy, residual risk for people with HFpEF and HFmrEF remains high.^36,38^ Several factors may contribute to the slower therapeutic development in individuals with HFpEF and HFmrEF.^18,82^ First, design choices in historical clinical trials regarding event rates and sample sizes have led most trials in HF to focus on people with HFrEF.^18^ It should also be noted that although EF is a continuum, ‘digit bias’, where clinicians report EF to numbers ending in ‘0’ or ‘5’, is common and may lead to misclassification of HF phenotypes.^83^
Second, people with HFpEF and HFmrEF represent a highly heterogeneous group with varying comorbidities/clinical profiles and a high risk of competing events that challenges trial design.^82^ There is also variability across clinical trials in terms of the inclusion criteria, leading to added heterogeneity across the different trial populations. Thus, HFpEF and HFmrEF may be considered a population comprising multiple ‘phenogroups’ and tailoring therapy to each individual's clinical profile may improve clinical outcomes in people with HFpEF and HFmrEF.^82^
Myocardial dysfunction in people with HFpEF could be a consequence of various comorbidities, including CV, obesity, kidney, metabolic, pulmonary, and geriatric conditions, and affects 5%–80% of this population.^82^ CV and kidney disease share similar pathophysiology and often coexist, making these conditions more difficult to manage. Cardio-kidney-metabolic disease is a complex disorder affecting the heart and kidneys that occurs in 40%–50% of people with HF, and CKD is frequently underdiagnosed in people with HF.^84,85^ The early assessment of kidney function in people presenting with HF is required to determine whether cardio-kidney disease is present and to inform appropriate management strategies to target both the heart and kidneys.^86,87^
New classes of therapies that target novel pathways implicated in the complex pathophysiology of HFpEF and HFmrEF and the comorbidities that contribute to their clinical presentation remain an unmet need. Dedicated trials are needed to fill key evidence gaps for existing and emerging HF therapies in people with HFpEF and HFmrEF.
Finally, non-pharmacologic factors are also important for optimizing the management of HFpEF and HFmrEF, but these are beyond the scope of this review. Briefly, age and sex are important demographic factors when assessing people with HFpEF, and may influence the burden associated with comorbidities of HF.^82,88^ Further establishing the clinical profiles of people with HFpEF and HFmrEF will help to provide timely diagnosis and appropriate treatment.^82^ The REVOLUTION-HF study found that 70% of people presenting to outpatient care with a combination of HF signs and/or symptoms and elevated N-terminal pro–B-type natriuretic peptide (NT-proBNP) levels were not diagnosed within the first year due to a lack of resources, resulting in a high risk of adverse outcomes.^89^
People with HFpEF or HFmrEF can also present with skeletal muscle dysfunction, which may contribute to exercise intolerance. Exercise training is an effective intervention for HFpEF; however, its effects on skeletal muscle function are poorly understood. Additional studies are needed to identify targeted therapies for people with HF presenting with skeletal muscle dysfunction.^90^ While beta blockers may have a potential benefit in HFpEF, they also induce chronotropic incompetence—an inability to increase heart rate during exercise—that is frequently observed in people with HFpEF and contributes to reduced exercise capacity,^91,92^ and improves following beta blocker withdrawal.^93^
Other cardiomyopathies, such as hypertrophic cardiomyopathy, Fabry disease, or cardiac amyloidosis, can present with a HFpEF-like phenotype.
Emerging treatment options for people with EF ≥40%
Due to the residual risk in people with HFpEF and HFmrEF driven by the heterogeneity of these conditions, the burden of comorbidities, and the persistent risk of adverse outcomes, several emerging treatments are being investigated for their potential benefits in this population. Treatment targets of emerging therapies relative to current therapies are presented in Figures 2–5.^19,75,94-101^
Pathway/receptor targets for current treatments and emerging therapies for HFpEF and HFmrEF: RAS and neprilysin pathways.94–96 ACC, American College of Cardiology; ACE, angiotensin-converting enzyme; ACEI, angiotensin-converting enzyme inhibitor; AHA, American Heart Association; ANP, atrial natriuretic peptide; ARB, angiotensin receptor blocker; ARNI, angiotensin receptor/neprilysin inhibitor; AS, aldosterone synthase; ASI, aldosterone synthase inhibitor; BNP, B-type natriuretic peptide; CNP, C-type natriuretic peptide; ESC, European Society of Cardiology; HFmrEF, heart failure with mildly reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFSA, Heart Failure Society of America; JCS, Japanese Circulation Society; JHFS, Japanese Heart Failure Society; MR, mineralocorticoid receptor; nsMRA, non-steroidal mineralocorticoid receptor antagonist; proBNP, pro–B-type natriuretic peptide; RAS, renin–angiotensin system; sMRA, steroidal mineralocorticoid receptor antagonist. aFinerenone was approved for patients with HF and left ventricular EF ≥40% (i.e. HFpEF and HFmrEF) in the USA in July 2025;75 approval for patients with HF in Europe has not yet been granted. bBased on ESC, AHA/ACC/HFSA or JCS/JHFS Class I or IIa recommendation, or iCARDIO Alliance ‘recommended’ or ‘strongly recommended’; ACEI or ARB recommended by iCARDIO Alliance; ARNI recommended by JCS/JHFS, and iCARDIO Alliance; finerenone (nsMRA) recommended by JCS/JHFS and iCARDIO Alliance; sMRA recommended by iCARDIO Alliance (see Table 1 for details). cBased on ESC, AHA/ACC/HFSA or JCS/JHFS Class I or Class IIa recommendation, or iCARDIO Alliance ‘recommended’ or ‘strongly recommended’; ARNI recommended for selected patients by JCS/JHFS and iCARDIO Alliance; finerenone (nsMRA) recommended by JCS/JHFS and iCARDIO Alliance (see Table 1 for details)
Pathway/receptor targets for current treatments and emerging therapies for HFpEF and HFmrEF: SNS pathway.97,98 ACC, American College of Cardiology; AHA, American Heart Association; AMP, adenosine 3′,5′-monophosphate; ESC, European Society of Cardiology; HFmrEF, heart failure with mildly reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFSA, Heart Failure Society of America; JCS, Japanese Circulation Society; JHFS, Japanese Heart Failure Society; SNS, sympathetic nervous system. aBased on ESC, AHA/ACC/HFSA or JCS/JHFS Class I or Class IIa recommendation, or iCARDIO Alliance ‘recommended’ or ‘strongly recommended’; recommended by iCARDIO Alliance (see Table 1 for details)
Pathway/receptor targets for current treatments and emerging therapies for HFpEF and HFmrEF: GLP-1 and GIP receptors.99,100 ACC, American College of Cardiology; AHA, American Heart Association; ESC, European Society of Cardiology; GIP, glucose-dependent insulinotropic polypeptide; GLP-1, glucagon-like peptide 1; GLP-1 RA, glucagon-like peptide 1 receptor antagonist; HFmrEF, heart failure with mildly reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFSA, Heart Failure Society of America; JCS, Japanese Circulation Society; JHFS, Japanese Heart Failure Society. aPrescribing information for semaglutide does not include HFpEF as an indication;101 however, global guidelines recommend its use in people with HFpEF and obesity.19 aBased on ESC, AHA/ACC/HFSA or JCS/JHFS Class I or Class IIa recommendation or above, or iCARDIO Alliance ‘recommended’ or ‘strongly recommended’: recommended by iCARDIO Alliance for people with obesity and HFpEF (see Table 1 for details)
Pathway/receptor targets for current treatments and emerging therapies for HFpEF and HFmrEF: SGLT2 receptor.99 ACC, American College of Cardiology; AHA, American Heart Association; ESC, European Society of Cardiology; HFmrEF, heart failure with mildly reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFSA, Heart Failure Society of America; JCS, Japanese Circulation Society; JHFS, Japanese Heart Failure Society; SGLT2, sodium–glucose cotransporter 2; SGLT2i, sodium–glucose cotransporter 2 inhibitor. aBased on ESC, AHA/ACC/HFSA or JCS/JHFS Class I or Class IIa recommendation or higher, or iCARDIO Alliance ‘recommended’ or ‘strongly recommended’: recommended by ESC, AHA/ACC/HFSA, JCS/JHFS, and iCARDIO Alliance (see Table 1 for details). bBased on ESC, AHA/ACC/HFSA or JCS/JHFS Class I or Class IIa recommendation, or iCARDIO Alliance ‘recommended’ or ‘strongly recommended’; recommended by ESC, AHA/ACC/HFSA, JCS/JHFS, and iCARDIO Alliance (see Table 1 for details)
MR modulators
Balcinrenone, a selective MR modulator, is being investigated for its efficacy and safety in people with HF (Table 3).^102,103,110^ In the Phase 2b study MIRACLE, balcinrenone in combination with dapagliflozin in people with HF (EF <60%, mean EF 46%) and CKD did not improve the primary endpoint of geometric mean percentage change in urine albumin-to-creatinine ratio from baseline to Week 12 compared with dapagliflozin alone.^102^ The ongoing BALANCED-HF Phase 3 trial will further evaluate the role of balcinrenone in combination with dapagliflozin in people with HF with a recent HF event and impaired kidney function, and is recruiting people with HF across the EF spectrum.^103^ A positive effect of balcinrenone, irrespective of EF and with an acceptable safety profile, will support the use of balcinrenone in people with HFpEF and HFmrEF.
Aldosterone synthase inhibitors (ASIs)
ASIs are an emerging treatment class that may provide an alternative method to target the effects of excess aldosterone observed in CV disease pathophysiology,^94^ and eliminate off-target effects of excess aldosterone frequently observed with sMRA and nsMRAs.^111^ EASI-HFpEF will evaluate the efficacy and safety of the ASI vicadrostat plus empagliflozin compared with placebo and empagliflozin in approximately 6000 participants with symptomatic HFpEF and HFmrEF not on sMRAs or an nsMRA (Table 3).^104^ A positive finding in this study will support the use of ASIs in people with HFpEF or HFmrEF.
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and glucose-dependent insulinotropic polypeptide receptor agonists (GIP RAs)
The effects of GLP-1 RAs on atherosclerotic CV disease in T2D, kidney outcomes, and obesity are well established.^112–114^ In addition, a meta-analysis indicated that treatment with a GLP-1 RA may prevent new-onset HF and mortality in people with T2D without HF.^115^
Two recently published trials have demonstrated the benefit of the GLP-1 RA semaglutide in people with obesity-related HF and an EF ≥45%. In the STEP-HFpEF trial, semaglutide reduced the secondary hierarchical composite endpoint, which included death and HF events, and improved KCCQ-CSS and 6-min walking distance compared with placebo (Table 3).^105^ The STEP-HFpEF DM study demonstrated similar effects on the same hierarchical composite endpoint in people with obesity-related HF (EF ≥45%) and T2D (Table 3).^106^ A prespecified analysis of pooled data from STEP-HFpEF and STEP-HFpEF DM confirmed the results of the individual studies with regard to the hierarchical endpoint (Table 3).^107^ Semaglutide reduced NT-proBNP at 52 weeks compared with placebo (Table 3)^108^ and was also associated with a reduction in loop diuretic use and dose compared with placebo.^116^ Although these trials were double-blind studies, the side effects and the body weight loss associated with GLP-1 RAs may undermine the blinded nature of the study, and the results should be interpreted with caution.
Safety results from the pooled analysis demonstrated that semaglutide was well tolerated in people with obesity-related HFpEF with or without T2D.^107^ Although gastrointestinal events leading to discontinuation were higher with semaglutide than placebo, the overall frequencies of gastrointestinal serious AEs were similar in both groups.^107^ Current treatment recommendations for GLP-1 RAs based on findings of studies with semaglutide are limited to people with obesity.
Tirzepatide is a long-acting dual agonist of GIP and GLP-1 (Figure 2), with a greater affinity towards the GIP receptor. This imbalance in agonism is considered important for its efficacy as dose escalation of GLP-1 RA can be limited due to gastrointestinal AEs. In SUMMIT, treatment with tirzepatide reduced the risk of the two co-primary endpoints, the composite of CV death or worsening HF (Table 3), and improved health status (KCCQ-CSS between-group difference: 6.9, P < .001).^109^ This benefit was observed irrespective of MRA use at baseline (Table 3).^109^ Although gastrointestinal symptoms were common with tirzepatide, they tended to dissipate over time and led to treatment discontinuation in only 4% of participants; the frequencies of serious AEs were similar between the tirzepatide and placebo groups.^109^ A cardiac magnetic resonance substudy of SUMMIT (n = 106) demonstrated that tirzepatide decreased left ventricular mass compared with placebo, and that the change in left ventricular mass was correlated with body weight loss.^117^ These findings suggest that changes in cardiac structure and a reduction in pro-inflammatory paracardiac adipose tissue may contribute to the decrease in HF events observed with tirzepatide in the main SUMMIT trial.^117^
The studies described above provide support for further evaluation of the efficacy of GLP-1 RAs and GIP/GLP-1 RAs in these populations.
Intravenous iron supplementation
While not currently recommended in the guidelines for HFpEF, results from the FAIR-HFpEF study suggest there may be potential benefits of ferric carboxymaltose treatment in participants with HFpEF and iron deficiency.^81^
New treatment approaches: combination therapy and precision medicine
Expert opinion increasingly supports the benefits of simultaneous or rapid sequence initiation of combination therapy for people with HFpEF and HFmrEF.^118,119^ To this end, recently, a three-pillared approach to treatment of HFpEF and HFmrEF was proposed, incorporating simultaneous/rapid sequence initiation of SGLT2is, an nsMRA, and GLP-1 RAs in combination.^119^ However, evidence to support this approach is currently lacking. Another potential three-pronged therapeutic strategy involves the use of an SGLT2i, an nsMRA, and an ARNI. In a recent analysis of data from three clinical trials in people with HFmrHF and HFpEF (DELIVER, FINEARTS HF, and PARAGON-HF), this combination reduced the risk of cardiovascular death or first worsening HF event by 39% in those with left ventricular EF <60% (HR 0.61; 95% CI 0.48–0.77).^79^
Furthermore, the heterogenous nature of HFpEF and HFmrEF due to the variable pathologic drivers, risk factors, and underlying aetiologies suggests that a shift toward phenotype-specific treatment strategies is warranted.^120,121^ Despite the heterogeneity between patients, the variability of clinical trial inclusion criteria, and a limited understanding of risk factors and predictors of HFpEF and HFmrEF, recent studies have proposed three broadly similar phenotypic clusters for HFpEF based on demographic and clinical characteristics.^120–122^ Specifically, the HFpEF phenotype clusters are based on age, comorbidity type, and burden of comorbid disease.^122^ Patients in phenotype 1 tend to be younger and have fewer comorbidities, those in phenotype 2 are older and are more likely to have comorbid atrial fibrillation and cardiorenal disease, while patients in phenotype 3 are of intermediate age with high comorbid disease burden including higher rates of T2D and obesity.^122^
Personalized approaches to treatment of certain subgroups of people based on comorbidities may be considered.^118,119^ For example, in patients with comorbid CKD, RASis or ARNIs for HFpEF and HFmrEF can be initiated as well as SGLT2is and an nsMRA.^118^ In addition, in a phenotype-guided treatment approach, GLP-1 RAs should be initiated in combination with SGLT2is and an nsMRA in patients with HFpEF or HFmrEF and comorbid CKD and T2D or obesity.^118^
Although new research is needed to further understand HFpEF and HFmrEF, especially given their complexity and associated comorbidities, continuing to explore optimal treatment sequencing and precision medication approaches will help with addressing the unmet medical needs and therapeutic gaps for patients with EF >40%.
Additional combination treatment considerations
As effective treatment options for patients with HFpEF and HFmrEF expand, guideline-directed treatments will likely evolve to include simultaneous initiation of combinations of drugs, similar to the current treatment approach for HFrEF. Polypharmacy will necessitate increased monitoring for electrolytes, blood pressure, and kidney function, and additional considerations related to the safety, access, and cost-effectiveness of combination therapy must be taken into account. The safety and tolerability of combination regimens for HFpEF and HFmrEF will need to be considered based on clinical trial findings alongside individual patient factors based on their comorbidities. Such an approach is fundamental to precision medicine. Polypharmacy costs may be a barrier for some patient populations; however, costs for healthcare systems may be lower if the number of HF hospitalizations is reduced, as has been observed with combination treatment in HFrEF.^118^
Conclusion
Despite guideline-directed therapy,^18,59,82^ an unmet need for effective pharmacologic treatment options remains for people with HFpEF and HFmrEF. Moreover, treatment is further complicated by the heterogeneity of comorbidities and clinical profiles in these populations, as also seen across clinical trials, which can significantly influence outcomes.
SGLT2is and the nsMRA finerenone have shown efficacy in improving outcomes for individuals with HFpEF and HFmrEF and are currently being further investigated in ongoing studies. Additionally, multiple trials are underway to explore new classes of treatments for HFpEF and HFmrEF, aiming to expand available therapeutic options.^44,45,80,103,104^ Further improvement in outcomes may also be achieved by tailoring treatment to specific phenotypes, such as obesity and CKD.^118,119^
Ongoing studies addressing key knowledge gaps in the management of HFpEF and HFmrEF, along with the integration of emerging and existing therapies into clinical guidelines, are essential for advancing treatment strategies, improving outcomes, and addressing the unmet therapeutic needs for people with HFpEF and HFmrEF.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bozkurt B, Coats AJS, Tsutsui H, Abdelhamid CM, Adamopoulos S, Albert N, et al Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese · doi ↗ · pubmed ↗
- 2Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022;145:e 895–1032. 10.1161/CIR.000000000000106335363499 · doi ↗ · pubmed ↗
- 3Mc Donagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al 2023 focused update of the 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2023;44:3627–39. 10.1093/eurheartj/ehad 19537622666 · doi ↗ · pubmed ↗
- 4Mc Donagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2021;42:3599–726. 10.1093/eurheartj/ehab 36834447992 · doi ↗ · pubmed ↗
- 5Kitai T, Kohsaka S, Kato T, Kato E, Sato K, Teramoto K, et al JCS/JHFS 2025 guideline on diagnosis and treatment of heart failure. Circ J 2025;89:1278–444. 10.1253/circj.CJ-25-000240159241 · doi ↗ · pubmed ↗
- 6Tan C, Dinh D, Brennan A, Hare DL, Kaye D, Lefkovits J, et al Characteristics and clinical outcomes in patients with heart failure with preserved ejection fraction compared to heart failure with reduced ejection fraction: insights from the VCOR heart failure snapshot. Heart Lung Circ 2022;31:623–8. 10.1016/j.hlc.2021.09.01934742643 · doi ↗ · pubmed ↗
- 7Savarese G, Stolfo D, Sinagra G, Lund LH. Heart failure with mid-range or mildly reduced ejection fraction. Nat Rev Cardiol 2022;19:100–16. 10.1038/s 41569-021-00605-534489589 PMC 8420965 · doi ↗ · pubmed ↗
- 8Palazzuoli A, Beltrami M. Are H Fp EF and H Fmr EF so different? The need to understand distinct phenotypes. Front Cardiovasc Med 2021;8:676658. 10.3389/fcvm.2021.67665834095263 PMC 8175976 · doi ↗ · pubmed ↗