The Small Bowel's Big Secret: A Case of Hidden Adenocarcinoma Unmasked by Capsule Endoscopy
Shagufta K Kiran, Rafique Hussain, Ali Raza, Hira Gul, Pardeep Maheshwari

TL;DR
A rare case of small bowel adenocarcinoma was diagnosed using capsule endoscopy after other tests failed, emphasizing its importance in diagnosing hard-to-detect gastrointestinal cancers.
Contribution
This case report highlights the underutilized role of capsule endoscopy in diagnosing small bowel adenocarcinoma and advocates for broader access to this diagnostic tool.
Findings
Capsule endoscopy identified a small bowel mass in a patient with unexplained symptoms after standard tests failed.
Surgical resection confirmed adenocarcinoma with no nodal involvement, leading to the patient's recovery and symptom-free status.
The case underscores the need for earlier use of capsule endoscopy in diagnosing elusive gastrointestinal malignancies.
Abstract
Small bowel adenocarcinoma (SBA) is an uncommon gastrointestinal malignancy that frequently presents with vague or nonspecific symptoms, leading to delayed diagnosis and poor outcomes. Because the small bowel is largely inaccessible to standard endoscopy, many patients endure prolonged abdominal pain, iron deficiency anemia, and weight loss before the underlying pathology is identified. Capsule endoscopy can reveal lesions that are often missed on upper or lower endoscopy and cross-sectional imaging, but its use remains limited in many centers due to issues of availability, cost, or delayed clinical consideration. We report the case of a 79-year-old man with a history of ischemic heart disease and paroxysmal atrial fibrillation who presented with one year of post-prandial abdominal pain, vomiting, and significant weight loss. Initial investigations, including gastroscopy, colonoscopy,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
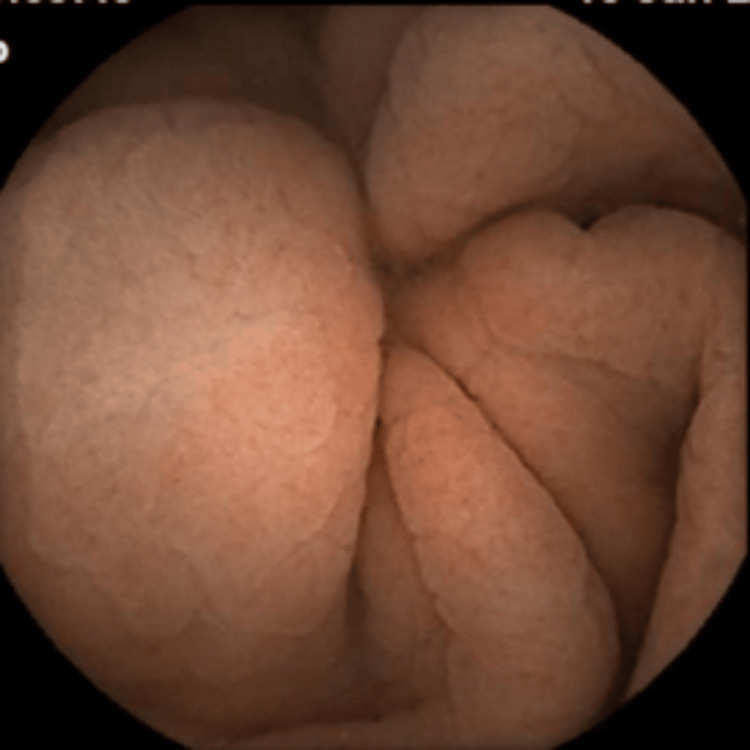 Figure 1
Figure 1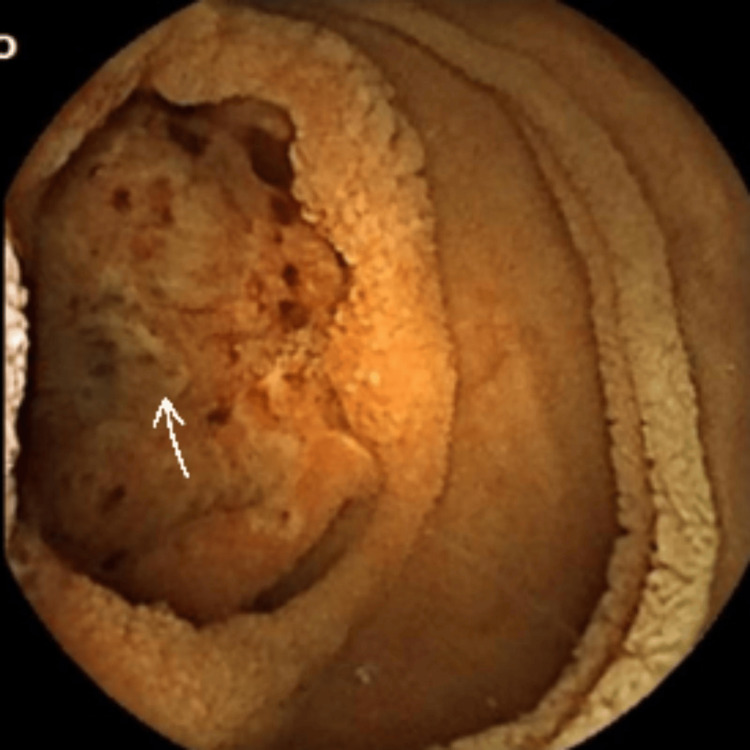 Figure 2
Figure 2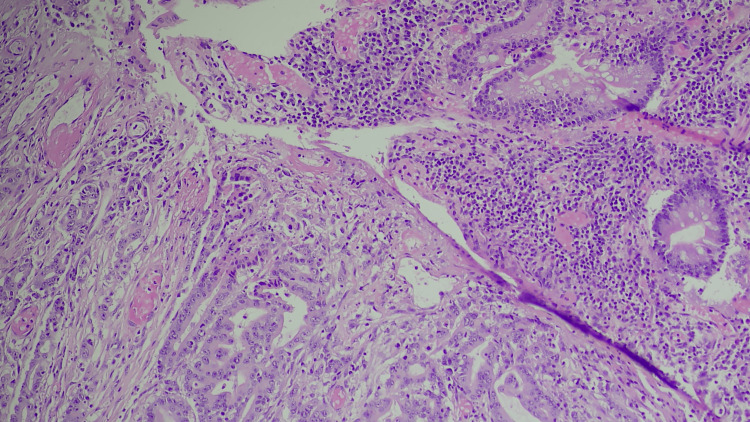 Figure 3
Figure 3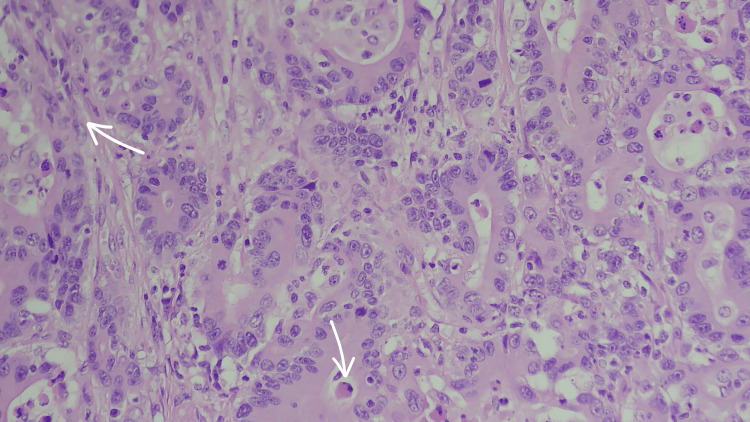 Figure 4
Figure 4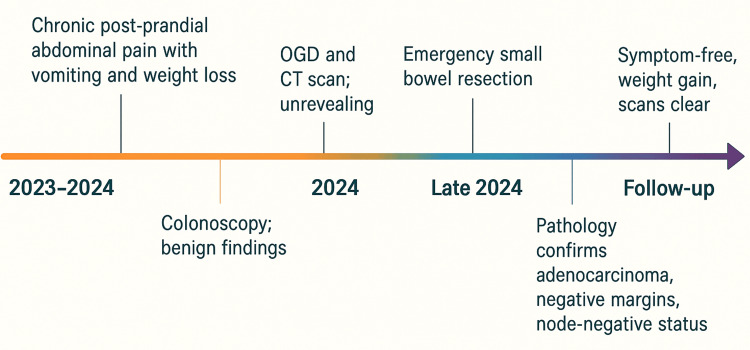 Figure 5
Figure 5| Test | Result | Reference Range | Interpretation |
| Hemoglobin | 9.1 g/dL | 13.5-16.5 g/dL | Low |
| Transferrin Saturation | 5% | 15-45% | Low |
| Alanine Amino Transferase | 9 U/L | 10-39 U/L | Normal |
| Gamma Glutamyl Transferase | 14 U/L | 10-71 U/L | Normal |
| Alkaline Phosphatase | 117 U/L | 40-129 U/L | Normal |
| Amylase | 33 U/L | 28-100 U/L | Normal |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Bleeding Diagnosis and Treatment · Gastrointestinal Tumor Research and Treatment · Colorectal Cancer Screening and Detection
Introduction
Small bowel adenocarcinoma (SBA) is a rare malignancy, representing only 1-3% of all gastrointestinal cancers [1,2]. Diagnosis is often delayed due to its vague presentation, typically intermittent abdominal pain, anemia, or weight loss, and the limited reach of standard endoscopy [3]. Consequently, patients may experience prolonged morbidity before diagnosis, with a significant proportion presenting at advanced stages. Studies have shown that 21-27% of patients have regional lymph node involvement and 32-37% present with distant metastases at the time of diagnosis [4].
These diagnostic challenges are exacerbated in settings where capsule endoscopy, an invaluable tool for evaluating the mid/small bowel, is unavailable, unaffordable, or underutilized. Early consideration of capsule endoscopy in cases of unexplained gastrointestinal bleeding or chronic abdominal pain may improve early detection and survival outcomes [5,6].
Case presentation
A 79-year-old man with ischemic heart disease (status post percutaneous coronary intervention) and paroxysmal atrial fibrillation on a non-vitamin K antagonist oral anticoagulant presented with a year-long history of post-prandial abdominal pain, occasional vomiting, and significant weight loss.
Laboratory findings revealed iron deficiency anemia with normal rest of the baseline investigations (Table 1).
An upper gastrointestinal endoscopy demonstrated mild Esophagitis, while a colonoscopy showed benign colonic polyps and a lipoma. A contrast-enhanced CT scan of the abdomen and pelvis revealed no evidence of malignancy. Prior investigations for bacterial overgrowth and celiac disease were negative. Despite proton pump inhibitors and antispasmodic therapy, his symptoms persisted. Capsule endoscopy revealed a 3 cm small bowel mass, prompting urgent surgical referral (Figures 1-2).
Capsule endoscopy image showing normal small bowel mucosa.
Capsule endoscopy image showing a mass in bowel mucosa with ulceration as denoted by the arrow.
Before the elective surgery could be performed, clinical deterioration due to intestinal obstruction necessitated emergency resection. Histopathology confirmed a moderately to poorly differentiated adenocarcinoma of the small bowel, measuring 3 cm, with negative resection margins, no lymphovascular invasion, and 24 lymph nodes negative for metastasis (Figures 3-4).
(H&E ×10) Histological examination of the mass showing irregular infiltration of glands/tubules invading through the bowel wall. In the upper right portion of the image, the cells that form more uniform and organized structures, such as the clear glandular lumen, represent normal or non-malignant tissue. These cells have more consistent nuclei and a more regular arrangement compared to the malignant cells. The clusters of cells forming irregular, crowded glands in the lower-left and central parts of the image are consistent with cancer cells, where cells are arranged in a disorderly fashion, the nuclei within these cells are varied in size and shape (pleomorphism), and often appear darker than the surrounding cells (hyperchromatism), which is a result of increased DNA content.
(H&E ×400) This magnified Image from histological examination of the mass shows presence of disorganized structures, irregular placement of nuclei (loss of polarity), cells are not forming the uniform, well-ordered glandular structures typical of healthy tissue as shown by the arrow in top left, presence of signet ring cells as denoted by the central bottom arrow, and the pinkish, fibrous connective tissue surrounding the abnormal glands is known as desmoplasia, a common stromal response to invasive cancer.
Given the absence of high-risk pathological features, surveillance was recommended. Follow-up at multidisciplinary discussion (MDM) confirmed concordant radiological findings and no recurrence. At his latest follow-up, the patient remains symptom-free, has regained weight, and demonstrates no evidence of disease on imaging (Figure 5).
Patient's progress.
Discussion
SBA is rare and often diagnosed late due to nonspecific symptoms and limited accessibility of the small bowel to conventional endoscopy [1,2,6]. Iron deficiency anemia and vague abdominal pain may persist despite normal upper and lower endoscopies, reflecting the low sensitivity of standard CT, which detects only about half of small bowel tumors (≈55.8%) with a sensitivity of around 40% for subtle intraluminal lesions [7]. Capsule endoscopy markedly improves diagnostic yield, identifying 79-83% of small bowel tumors, while CT enterography detects 93-94% of tumors when performed with dedicated protocols, demonstrating higher sensitivity for structural lesions but continued value of endoscopy for mucosal evaluation [7,8].
Despite its utility, capsule endoscopy remains underutilized in many settings, contributing to delayed diagnosis and poorer outcomes [9,10]. Prognosis is strongly stage-dependent, with five-year survival exceeding 80% in localized disease compared to ~30-35% overall [2,11]. The absence of standardized post-resection surveillance protocols highlights ongoing uncertainty in long-term management [12].
What this case adds
This case illustrates how SBA can remain undetected despite normal endoscopy and CT imaging and emphasizes the pivotal role of capsule endoscopy in reducing diagnostic delay and facilitating potentially curative intervention.
Patient perspective
The patient reports significant improvement in overall health and quality of life, weight gain, and complete resolution of symptoms. He expressed gratitude for the persistence shown in pursuing a definitive diagnosis after multiple inconclusive investigations.
Conclusions
Early use of capsule endoscopy is crucial for patients with persistent, unexplained gastrointestinal symptoms, particularly iron deficiency anemia, as it can significantly reduce diagnostic delays and improve outcomes. Expanding access to capsule endoscopy, including in resource-limited settings, remains a key priority.
There is also an unmet need for research to establish standardized post-resection surveillance, as current guidelines are limited. Timely diagnosis, appropriate surgical intervention, and structured follow-up remain essential for optimizing prognosis in SBA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Incidence, clinical management and prognosis of patients with small intestinal adenocarcinomas from 1999 through 2019: a nationwide Dutch cohort study Eur J Cancer de Back TR Linssen JD van Erning FN 1131241992024 http://www.ejcancer.com/article/S 0959-8049(24)00005-4/fulltext 10.1016/j.ejca.2024.11352938232410 · doi ↗ · pubmed ↗
- 2Endoscopic diagnosis of small bowel tumor Cancers (Basel) Yano T Yamamoto H 416202410.3390/cancers 16091704 PMC 1108395138730658 · doi ↗ · pubmed ↗
- 3The role of capsule endoscopy in the diagnosis and management of small bowel tumors: a narrative review Cancers (Basel) Fantasia S Cortegoso Valdivia P Kayali S Koulaouzidis G Pennazio M Koulaouzidis A 216202410.3390/cancers 16020262 PMC 1081347138254753 · doi ↗ · pubmed ↗
- 4Does age matter in the selection of treatment for men with early-stage prostate cancer?Cancer Konski A Eisenberg D Horwitz E Hanlon A Pollack A Hanks G 259826021062006 http://onlinelibrary.wiley.com/doi/10.1002/cncr.219231668322410.1002/cncr.21923 · doi ↗ · pubmed ↗
- 5Epidemiology of cancers of the small intestine: trends, risk factors, and prevention Med Sci (Basel) Barsouk A Rawla P Barsouk A Thandra KC 6720193088491510.3390/medsci 7030046 PMC 6473503 · doi ↗ · pubmed ↗
- 6Small bowel cancer in the United States: changes in epidemiology, treatment, and survival over the last 20 years Ann Surg Bilimoria KY Bentrem DJ Wayne JD Ko CY Bennett CL Talamonti MS 637124920091910667710.1097/SLA.0b 013e 31818 e 4641 · doi ↗ · pubmed ↗
- 7CT-enterography may identify small bowel tumors not detected by capsule endoscopy: eight years experience at Mayo Clinic Rochester Dig Dis Sci Hakim FA Alexander JA Huprich JE Grover M Enders FT 291429195620112173508510.1007/s 10620-011-1773-0 · doi ↗ · pubmed ↗
- 8Small bowel adenocarcinoma: an overview World J Gastrointest Oncol Khosla D Dey T Madan R Gupta R Goyal S Kumar N Kapoor R 4134221420223531732210.4251/wjgo.v 14.i 2.413PMC 8918997 · doi ↗ · pubmed ↗