Efficacy of skeletally anchored modified leaf expander versus modified conventional Hyrax in maxillary molar distalization: a randomized clinical trial
Mohamed Elsaharty, Mahmoud M. Fathy Abo-Elmahasen, Nouran M. Eissa, Mohamed Elbialy

TL;DR
This study compares two orthodontic devices for moving maxillary molars backward, finding that one achieves the result faster than the other.
Contribution
The study introduces a randomized clinical trial comparing two skeletally anchored distalizers for maxillary molar distalization.
Findings
Both appliances achieved significant distalization of maxillary first molars with minimal angular changes.
The Hyrax Expander achieved distalization faster than the Leaf Expander with a significantly shorter treatment duration.
Skeletal and dental parameters showed no significant differences after Bonferroni correction.
Abstract
Distalization in orthodontics is one of conservative treatment modalities that result in gaining space especially in dental orthodontic cases of class ΙΙ molar relationship. A prospective parallel double group randomized clinical trial aimed to compare the distalization effects of the skeletally anchored modified Leaf Expander versus the skeletally anchored modified conventional Hyrax Expander. Skeletally anchored distalizers for orthodontic treatment are better than dentally anchored distalizers (Superiority). Thirty patients (15–18 years) who were requiring maxillary molar distalization, were randomly allocated into two groups (n = 15 each). Group 1 received the modified skeletally anchored self-activated Leaf Expander, and Group 2 received the modified skeletally anchored conventional Hyrax Expander. Pre- and post-distalization lateral cephalometric radiographs and digital dental…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
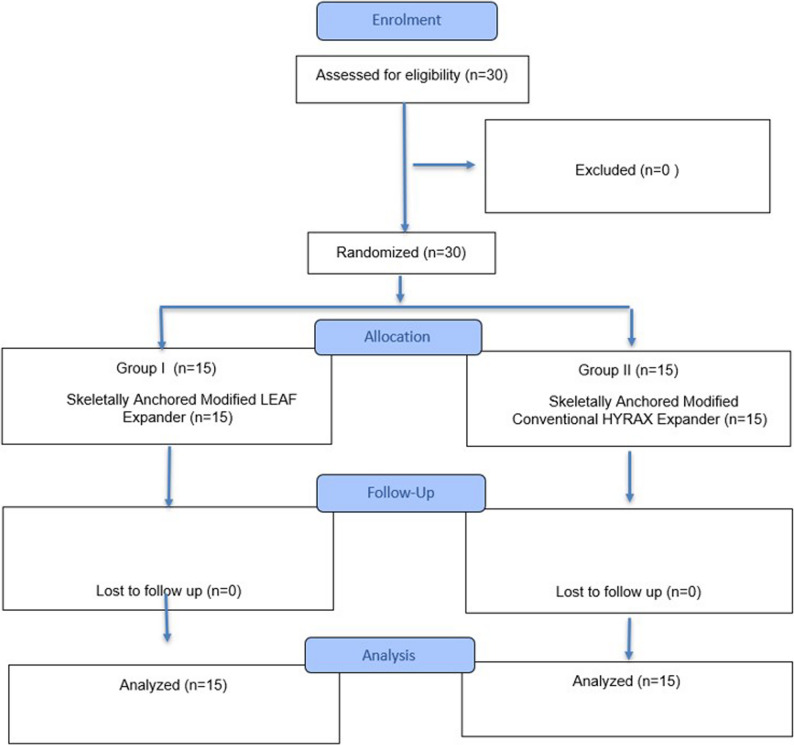 Figure 1
Figure 1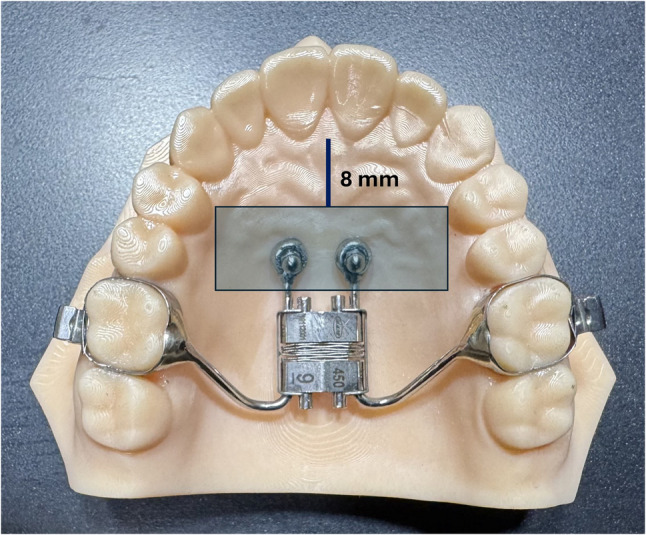 Figure 2
Figure 2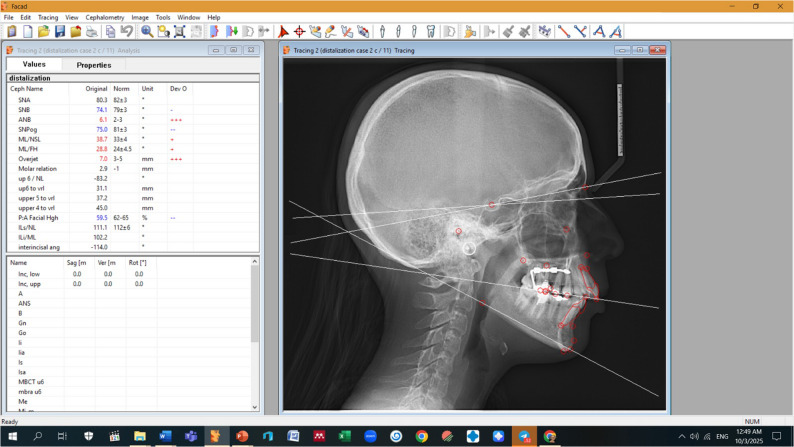 Figure 3
Figure 3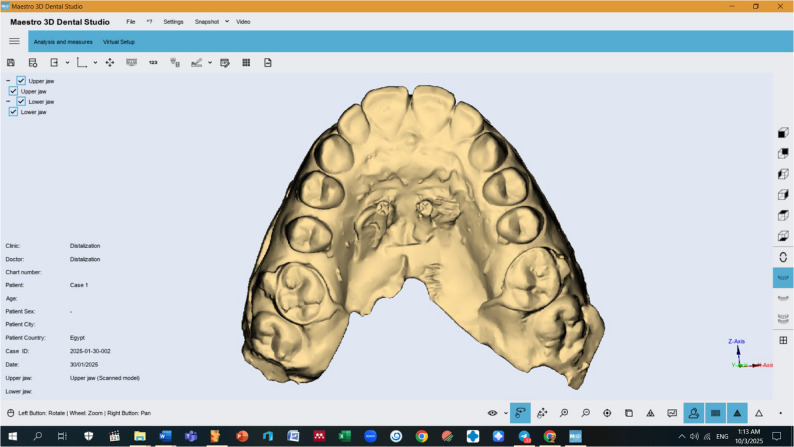 Figure 4
Figure 4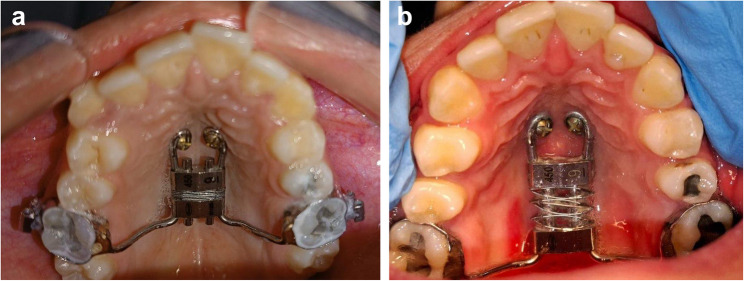 Figure 5
Figure 5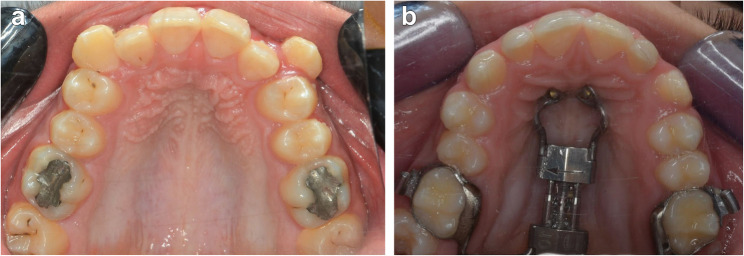 Figure 6
Figure 6- —Tanta University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthodontics and Dentofacial Orthopedics · dental development and anomalies · Craniofacial Disorders and Treatments
Introduction
Class II malocclusion is one of the most frequently encountered orthodontic problems. Generally, the management of Class II malocclusions involves two main treatment strategies: extraction or non-extraction [1]. Recently, there had been a paradigm shift towards non-extraction treatment, which is more acceptable for both patients and orthodontists [2]. In Class II cases with mild to moderate crowding in the maxillary arch and a normal mandibular arch, possible treatment approaches include interproximal reduction, expansion, derotation and/or uprighting of posterior teeth and maxillary molar distalization [3].
Several authors have been used intraoral appliances to distalize maxillary molars with either skeletal or dental anchorage. Dentally anchored distalizers effectively distalize maxillary molars; however, they are associated with distal tipping of the molars rather than bodily movement, protrusion of maxillary incisors, and subsequent anchorage loss [4, 5]. The introduction of skeletally anchored distalizers has provided better control of the incisors by preventing their proclination and reducing anchorage loss, but distal tipping of the maxillary molars was still reported [6].
In 2011, Ludwig et al. [7] introduced the skeletally anchored Frog distalizer. Although the skeletally anchored Frog appliance controlled maxillary incisor proclination, it could not provide bodily distal movement of the maxillary molars, increasing the risk of anchorage loss during uprighting [7]. These findings highlighted that the flexible connection between the frog appliance and the maxillary molars caused the line of action of distalization forces to pass away from the center of resistance of the maxillary molars. In 2022, Abo-Elmahasen et al. [8] modified the skeletally anchored Hyrax palatal expander for maxillary molar distalization. The modification aimed to realign the line of action of the distalizing force to pass through the center of resistance of the maxillary molars via a rigid connection between the appliance and molars; this resulted in bodily distal movement of the maxillary molars, evidenced by non-significant changes in molar angulation relative to the palatal plane [8].
Recently, titanium miniscrews (TMSs) have been intensively used as orthodontic implants because they usually demonstrate clinical effectiveness due to their good stability and the excellent anchorage they can provide [9–11]. However, some factors can lead to failure of orthodontic TMSs such as poor cortical bone density, bone resorption and inflammatory responses near the implant site, and corrosion of the TMS [12–14].
However, the modified skeletally anchored conventional Hyrax distalizer required periodic activation once or twice a week, which sometimes posed difficulties for patients and relied heavily on their cooperation [15–17]. The introduction of the self-activated Leaf expander offered a non-compliant method for appliance activation. The Leaf Expander is a nickel-titanium device designed to apply uniform, gradual and continuous force. Its primary benefits include straightforward activation and independence from patient cooperation, thus eliminating compliance issues. Additionally, compared to conventional RME, the Leaf Expander typically results in lower levels of pain during the initial days following its application [18–24]. Therefore, this study was conducted to compare the distalization effects of skeletally anchored modified Leaf Expander and skeletally anchored modified conventional Hyrax Expander.
Patients and methods
Study design
A prospective two-arm, parallel-group, superiority randomized clinical trial.
Trial design framework
Skeletally anchored distalizers for orthodontic treatment were better than dentally anchored distalizers (Superiority), they were not much worse than dentally anchored appliances (non-inferiority), also the different skeletally anchored distalizers may have the same effects (equivalence).
Sample size calculation
The sample size was calculated to detect a clinically significant difference in maxillary molar distalization between the two groups (primary outcome of the current study). Based on previous studies (e.g., Abo-Elmahasen et al., 2022 [8]), the expected mean difference in molar distalization was estimated to be 1.0 mm, with a standard deviation of 0.8 mm. Using a significance level (α) of 0.05 and a power (1-β) of 80%, the minimum sample size required per group was calculated was 15 patients / group.
Study setting and populations
This prospective study included 30 patients consecutively enrolled and treated at the dental clinics, Orthodontic Department, Faculty of Dentistry, Tanta University, Egypt. Patients were aged between 15 and 18 years. All patients underwent maxillary molar distalization using one of two appliances.
Groups’ randomization
The patients involved in the study groups were randomly distributed through a simple online‑generated randomization plan using online software found at the website http://www.graphpad.com/quickcalcs/index. cfm. The allocation ratio is 1:1 (Fig. 1).
Fig. 1CONSORT CHART. The consort chart shows the flow of participants through the phases of the trial. A total of 30 participants were assessed for eligibility, and all were allocated. Group I (n = 15) Skeletally Anchored Modified Leaf Expander, and Group II (n = 15) Skeletally Anchored Modified Conventional Hyrax Expander. There were no losses to follow-up in either group, and all participants (n = 30) were included in the final analysis
- Group 1: Patients treated with the modified skeletally supported self-activated Leaf expander as a distalization appliance (7 males, 8 females).
- Group 2: Patients treated with the modified skeletally supported conventional Hyrax expander as a distalization appliance (6 males, 9 females).
Blinding
Cephalometric and digital model measurements and statistical analyses were conducted by an independent examiner blinded to group allocation to minimize measurement and detection bias.
Inclusion criteria
- Class II molar relation.
- Patients aged between 15 and 18 years.
- Overjet less than 6 mm.
- ANB angle between 5° and 7°.
- Non-extraction treatment plan with molar distalization.
- Horizontal or normal growth pattern with symmetrical, balanced facial appearance.
- Minimal crowding in the mandibular arch.
Exclusion criteria
- Congenitally missing teeth
- Congenital anomalies
- Systemic diseases
- Previous orthodontic treatment
Ethical considerations
All patients were informed about the nature, purpose, risks, and benefits of the study prior to enrollment. This study was approved by the Research Ethics Committee of the Faculty of Dentistry, Tanta University, Egypt (Approval No: R-ORTH-08-25-3220). All research procedures were conducted in full accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants. For participants under 16 years of age, informed consent was obtained from their parents or legal guardians.
Declaration of patient/public involvement
Patients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
The self-activated Leaf Expander
The Leaf Expander (Leaf Expander^®^, Leone SpA, Sesto Fiorentino, Florence, Italy) resembles a rapid palatal expander but incorporates Nickel Titanium MEMORIA leaf springs that provide continuous force. It consists of two body parts connected by rods over which the leaf springs slide. The springs are held compressed by staples on each side of the body parts. The super elastic nickel-titanium leaf springs deliver a controlled, continuous force once the staples are removed. Two types of Leaf Expanders are available, delivering either 450 or 900 grams of force; the 450-gram/ 6 mm in length version was used in this study.
Intervention
Elastic separators were placed mesial and distal to the maxillary first molars bilaterally for 3 days to create space for band placement [25]. Appropriate bands were selected and fitted to the molars. An alginate impression was taken with the bands in place, and then the bands were removed and repositioned in the impression. The impression was poured in stone to fabricate the working model.
Fabrication of the modified palatally anchored expander appliance
The positions of the screws for skeletal anchorage were determined on the model within a safe square on the anterior palatal area. Four lines were drawn [8]:
- The first line, 8 mm distal to the incisive papilla, marked the anterior boundary.
- The second line, parallel to the first, passed through the distal surfaces of the second premolars to mark the posterior boundary.
- Two additional lines, each 8 mm lateral to the median palatal raphe, were drawn perpendicular to the first two lines.
The four-point support expander was modified by rotating the line of action 90° to align Antero-posteriorly for distalization [8]. The distalizer was centered on the palate. The two anterior legs were bent forward and welded to metal sleeves (3 mm diameter) placed 2 mm from the midpalatal raphe. The posterior legs were bent to be welded to the bands on the upper first molars bilaterally. The distalizer was soldered to the bands, finished, polished, and prepared for intraoral insertion (Fig. 2).
Fig. 2. Fabrication of modified skeletally anchored leaf expander as a distalization appliance
Intraoral insertion
The appliance was cemented onto the first molars. Local anesthesia was administered at palatal sites for surgical screw insertion. Two screws (2.1 mm diameter, 13 mm length) (Titanium mini-screws from the Dentaurum Company (Germany) were used in the Tomas^®^ TMS system for skeletal anchoring) were inserted freehand to provide skeletal anchorage. Patients received oral hygiene instructions and were advised to use mouthwash and clean around the screws with a soft brush. Non-steroidal anti-inflammatory drugs were prescribed for one day only.
Calibrating data for force vector for both appliances
The inverted leaf expander as a distalizer produce continuously 450 gm per side, while the inverted hyrax distalizer produce (100 gm per 0.2 mm (quarter turn activation); 400 gm per 1 mm (complete turn activation) that is nearly equal to the inverted leaf expander.
Follow-up and appliance activation
One week after insertion, appliance stability, screw health, oral hygiene, and patient comfort were assessed. The staples on the sides of the Leaf Expander were removed to activate distalization. The Leaf Expander required no further periodic activation [16] (For adverse events see quantitative table and severity grading (Table 1).
Table 1. Adverse events in quantitative table and severity gradingAdverse event term (Standardized)Grade 1 (Mild)(numbers per patients)Grade 2 (Moderate)(numbers per patients)Grade 3 (Sever)(numbers per patients)appliance instability (Group Ι)000appliance instability (Group ΙΙ)000screw loosening (Group Ι)000screw loosening (Group ΙΙ)000Bad oral hygiene (Group Ι)1050Bad oral hygiene (Group ΙΙ)1140patient discomfort (Group Ι)1320patient discomfort (Group ΙΙ)1230
Cephalometric and model analysis
Pre- and post-distalization lateral cephalometric radiographs were imported into FACAD software for analysis (Fig. 3). Measurements included:
Fig. 3. Cephalometric analysis for Group (1) Sample after distalization by FACAD software
- Skeletal angular changes: SNA, SNB, and ANB angles
- Vertical skeletal changes: FH-MP angle
A horizontal reference line was drawn at a 7° angle to the SN plane at point S; a vertical reference line perpendicular to this was drawn at point S. The horizontal distance from the mesiobuccal cusp tip of the maxillary first molar to the vertical reference line was measured to quantify distalization. The angle between the upper first molar long axis and the palatal plane was measured to evaluate molar tipping [8].
Anterior dental changes were assessed by measuring overjet, U1/PP (upper incisor to palatal plane), L1/MP (lower incisor to mandibular plane), and inter-incisal angles (Table 2).
Table 2. Cephalometric measurementsMeasurementDefinitionSNA angleThe angle formed by the intersection of SN and NA.SNB angleThe angle formed by the intersection of SN and NB.ANB angleThe angle formed by the intersection of NA and NB.FH/MP angleThe angle formed by the intersection of mandibular plane and Frankfort horizontal plane.OverjetHorizontal distance between the maxillary and mandibular incisal edges.Constructed Horizontal Plane (CHP)A line drawn 7^0^ to the SN plane at point S.Constructed Vertical Plane (CVP)a vertical reference drawn on the CHP at point S.Palatal Plane (PP)A line drawn between ANS & PNS.Upper 6 / Palatal Plane (Up6pp) angleThe angle between the long axis of the upper 1st molar ( the line between the mesiobuccal cusp tip and the mesiobuccal root apex) and the palatal plane.Upper 6 to CVP (Up6CVP)Distance of a perpendicular line (parallel to CHP) from the mesiobuccal cusp tip of the maxillary first molar (U6) to CVP.Upper 1 to PP(up1pp)The angle between the long axis of the upper central incisor and the palatal plane.Lower 1 MP(Low1mp)The angle between the long axis of the lower central incisor and the mandibular plane (Go Gn).Interincisal angleThe angle between the long axis of the upper central incisor and the lower central incisor.
Maxillary dental models were taken pre- and post-distalization were scanned using an intraoral scanner (Medit i600, Kemet Corporation, Korea) to generate STL files, analyzed with Maestro 3D software for changes in (Fig. 4; Table 3):
Fig. 4. Digital model analysis after distalization by Maestro software for Group (1) Sample after distalization
Table 3. Digital model measurementMeasurementDefinitionArch Lengththe total length of the posterior and anterior segments mesial to the first permanent molars.Intercanine WidthThe distance between cusp tips of the right and left maxillary permanent canines.Inter-1st- Premolar widthThe distance between buccal cusp tips of the right and left maxillary 1st premolars.Inter-2nd- Premolar widthThe distance between buccal cusp tips of the right and left maxillary 2nd premolars.Inter-1st- Molar widthThe distance between buccal cusp tips of the right and left maxillary 1st molars.
- Arch length.
- Inter-canine width.
- Inter-first premolar width.
- Inter-second premolar width.
- Inter-first molar width.
Study outcomes
The primary outcomes of the current study were: Arch length, Inter-canine width, Inter-first premolar width, Inter-second premolar width and Inter-first molar width, all these parameters were assessed after completion of distalization and result in class 1 molar relationship.
While the secondary outcomes were skeletal and dental cephalometric measurements; SNA, SNB, and ANB angles, FH-MP angle, overjet, U1/PP (upper incisor to palatal plane), L1/MP (lower incisor to mandibular plane), and inter-incisal angles.
Statistical analysis
Data were analyzed by using a Microsoft Excel 2010 and SPSS version 20 (SPSS Inc., Chicago, IL, USA). Numerical data are presented as means ± standard deviations (SD). The Shapiro-Wilk test confirmed normal data distribution. Parametric tests were used for analysis:
- Paired sample t-tests compared pre- and post-distalization measurements within each group.
- Statistical significance was set at (p < 0.05).
- Intraobserver reliability was assessed using the Intra-Class Correlation Coefficient (ICC).
To account for multiple comparisons, a Bonferroni correction was applied. With 11 primary comparisons, the adjusted significance threshold was α = 0.0045. P-values ≤ 0.0045 were considered statistically significant. Effect sizes (Cohen’s d) were reported to indicate clinical relevance, even when p-values exceeded the corrected threshold. Clinical relevance (effect sizes) was emphasized alongside strict statistical significance.
Error of the study
To assess measurement reliability, 10 lateral cephalometric radiographs (before and after completion of the distalization) were randomly chosen, then skeletal and dental measurements were measured again 1 month after the first measurement. Reliability was evaluated using intra-class correlation (ICC), which gave a strong intra-examiner reliability (ICC ¼ 0.998), and the Dahlberg formula, which showed minimal error that does not affect the reliability of the measurements.
Results
All thirty patients (13 males and 17 females) who met inclusion criteria have a complete analysis for assessment of distalization for the two groups, there were no discontinuous patients, all patients were cooperative and followed the inclusion criteria. (See participant flow diagram).
Clinical results
The study sample consisted of 30 patients divided equally into two groups (n = 15 each), with mean ages of 16.20 ± 0.85 years in Group 1 and 16.80 ± 0.90 years in Group 2 which confirmed homogeneity between the tested groups. Both appliances effectively corrected molar relations to Class I within 10.43 ± 1.52 months for Group 1 and 6.52 ± 1.52 months for Group 2. The treatment duration was significantly shorter in Group 2 (p < 0.05). After Bonferroni correction (α = 0.0045), treatment duration remained statistically significant, favoring the Hyrax Expander (Tables 4 and 5) (Figs. 5 and 6).
Table 4. Sample descriptionParameterGroup 1 (Leaf Expander)Group 2 (Hyrax Expander)t-testp-valueSignificant after Bonferroni?Effect Size (d)Age (years)16.20 ± 0.8516.80 ± 0.90−1.500.140No0.35 (small)(95% CI: 15.73–16.67)(95% CI: 16.30–17.30)Treatment duration (months)10.43 ± 1.526.52 ± 1.524.93< 0.001Yes2.35 (large)(95% CI: 9.94–11.46)(95% CI: 6.02–7.54)Effect sizes calculated using Cohen’s dp: p value for t-test for comparing between before and after treatment; ***: Statistically significant at p ≤ 0.05 SD: standard deviation; Bonferroni-corrected significance threshold: α = 0.0045
Table 5. Baseline characteristicsParameterGroup 1 – Modified Leaf Expander (n = 15)Group 2 – Modified HYRAX Expander (n = 15)p-valueSex: Male, n (%)7 (46.7%)6 (40.0%)— Female, n (%)8 (53.3%)9 (60.0%)—Skeletal pattern (ANB):15 (100%)15 (100%)— Skeletal Class II (ANB 5°–7°), n (%)Malocclusion type:15 (100%)15 (100%)— (Class II malocclusion, n (%))Initial molar relationship:15 (100%)15 (100%)— (Bilateral Class II molar relationship, n (%))Data are presented as mean ± SD with 95% confidence intervals (CI) where applicableCI calculated using t = 2.145 for n = 15 per group
Fig. 5A intraoral photograph showing the modified leaf expander distalizer before distalization. B intraoral photograph showing the modified leaf expander distalizer after distalization
Fig. 6A intraoral photograph group II before distalization. B intraoral photograph showing the modified conventional Hyrax expander distalizer after distalization
Gingival enlargement
Gingival enlargement was observed in one patient in Group 1 (gingival index grade 1) and two patients in Group 2 (gingival index grade 2), localized around the anterior arms of the appliances and surgical screws. Management involved removal of screws and appliances, prescription of anti-inflammatory medication, and reinforcement of oral hygiene instructions. After two weeks, appliances were adjusted to relieve pressure points and reinserted without complications.
Radiographic results
Skeletal changes
Both groups exhibited a slight decrease in SNA angle: -0.075 ± 0.27 in Group 1 and −0.006 ± 0.38 in Group 2, with no statistically significant difference between groups (p > 0.05). Similarly, SNB and ANB angles decreased in both groups without significant intergroup differences (p > 0.05). The FH-MP angle increased slightly by 0.79 ± 0.22 in Group 1 and 0.97 ± 0.45 in Group 2, again showing no significant difference between groups (p > 0.05) (Table 6).
Table 6. Cephalometric and digital model analysisParameterGroup 1 (Leaf Expander)Group 2 (Hyrax Expander)t-testp-valueSignificant after Bonferroni?Effect Size (d)SNA (°)−0.075 ± 0.27−0.006 ± 0.380.5860.562No0.21(95% CI: −0.23–0.07)(95% CI: −0.22–0.20)SNB (°)−0.013 ± 0.070.20 ± 0.791.0670.294No0.34(95% CI: −0.05–0.03)(95% CI: −0.24–0.64)ANB (°)−0.138 ± 0.16−0.206 ± 0.740.3620.720No0.11(95% CI: −0.23 – −0.05)(95% CI: −0.62–0.20)FH-MP (°)0.79 ± 0.220.97 ± 0.451.5560.130No0.44(95% CI: 0.67–0.91)(95% CI: 0.72–1.22)Overjet (mm)−0.675 ± 0.21−0.76 ± 0.130.5750.583No0.15(95% CI: −0.80 – −0.56)(95% CI: −0.83 – −0.69)U6-PP (°)−0.806 ± 0.24−0.723 ± 0.340.8470.413No0.24(95% CI: −0.94 – −0.68)(95% CI: −0.91 – −0.53)U6-VRL (mm)−7.65 ± 0.74−6.95 ± 0.822.440.020No0.87(95% CI: −8.06 – −7.24)(95% CI: −7.41 – −6.49)U1/PP (°)−3.00 ± 1.98−2.93 ± 1.831.860.230No0.04(95% CI: −4.10 – −1.90)(95% CI: −3.95 – −1.91)L1/MP (°)−0.413 ± 0.85−0.206 ± 0.680.7580.454No0.25(95% CI: −0.88–0.06)(95% CI: −0.58–0.16)Interincisal (°)2.00 ± 1.853.46 ± 2.601.8260.078No0.63(95% CI: 0.97–3.03)(95% CI: 2.02–4.90)Arch length (mm)6.32 ± 0.767.39 ± 2.481.6570.108No0.56(95% CI: 5.90–6.74)(95% CI: 6.02–8.76)Intercanine width (mm)28.56 ± 2.4730.68 ± 2.982.0000.056No0.74(95% CI: 27.19–29.93)(95% CI: 29.03–32.33)Effect sizes calculated using Cohen’s dp: p value for t-test for comparing between before and after treatment; *: Statistically significant at p ≤ 0.05 SD: standard deviation; Bonferroni-corrected significance threshold: α = 0.0045
Dental changes
The overjet decreased in both groups, with no significant difference between them (p = 0.583). Significant maxillary molar distalization was achieved in both groups. Group 1 exhibited a mean distal movement of −7.65 ± 0.74 mm, while Group 2 showed −6.95 ± 0.82 mm. Although the between-group difference was not statistically significant after Bonferroni correction (p = 0.020), it remains clinically relevant, favoring slightly greater distalization with the Leaf Expander. Both appliances maintained favorable molar angulation, as indicated by non-significant changes in the U6-PP angle, confirming significat molar distalization with non-significant changes in its angulation (Table 6).
Incisor inclination changes were minor and not statistically significant. Both groups showed a slight decrease in upper and lower incisor angulations (UP1/PP and L1/MP), along with a mild increase in the inter-incisal angle, with no significant differences between groups (Table 6).
Digital model analysis
Arch length
Both groups demonstrated an increase in maxillary arch length post-distalization (Group 1: 6.32 ± 0.76 mm; Group 2: 7.39 ± 2.48 mm), with no significant difference between groups (p = 0.108). None of these differences reached statistical significance after Bonferroni correction, though some were clinically meaningful (Table 6).
Transverse dimensions
The inter-canine width increased more in Group 2 (30.68 ± 2.98 mm) compared to Group 1 (28.56 ± 2.47 mm). Although this difference approached statistical significance (p = 0.056), it did not reach the threshold. Increases in inter-premolar widths (1st and 2nd) were observed in both groups, but no significant differences were noted. The inter-molar width decreased slightly in both groups, without statistical significance (Table 6).
Data sharing statement
- Specified data: the raw data of the current study are available.
- Indicated the platform: The raw data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Discussion
Maxillary molar distalization is a common approach in the management of Class II malocclusion. This technique relies on moving the maxillary molars distally within the arch to create space for overjet reduction and anterior alignment. Several intraoral distalization appliances have been described in the literature, utilizing either dental or skeletal anchorage. While dental anchorage provides support by resting on the premolars, it frequently causes undesirable effects such as proclination of maxillary anterior teeth and distal tipping of molars. The advantage of skeletal anchorage (mini-screws or micro-implants) addressed these issues by offering better control of anterior teeth without increasing their proclination [26–34].
All subjects in the current study exhibited bilateral class ΙΙ molar relationships since the original assembly of the appliances that used for distalization for both groups were designed for bilateral distalization, in addition to avoiding the implementation of asymmetric distalizing mechanics which might have an adverse effect on the skeletal, dentoalveolar and soft tissue measurements.
Anchorage site and screw selection
In 2023, Wilmes et al. [35] identified the anterior Para median and median regions of the hard palate as safe, minimally invasive zones for TAD insertion. These regions have been commonly used to provide skeletal anchorage in both distalization [27–30] and maxillary protraction [30–33]. Accordingly, the anterior Para median palatal area was selected in this study for TADs placement.
The literature shows variability regarding the optimal mini-screw length. Some studies have used 6 mm screws to avoid nasal cavity penetration [7], while others used 8–11 mm screws based on CBCT evaluation [14–18]. Studies evaluating palatal bone and soft tissue thickness report an average of 5 mm bone and 4–5 mm soft tissue [16, 17, 25], suggesting that 11 mm screws can safely engage the nasal cortex for enhanced stability. Given that the welded sleeves in our appliances are 2 mm thick, 13 mm surgical screws were used to ensure full bicortical engagement and reliable skeletal anchorage.
Skeletal and dentoalveolar effects
In the sagittal plane, minor reductions in SNA, SNB, and ANB angles were observed, consistent with findings by Abo-Elmahasen et al. [8] and Ngan et al. [34]. In the vertical plane, both groups exhibited clockwise mandibular rotation, as indicated by increases in the FH-MP angle. This can be attributed to the wedging effect caused by molar distalization.
The changes in (ANB) have no statistical or clinical significance; it may be attributed to retraction of anterior teeth after molar distalization.
Maxillary molar distalization
Prior studies have reported varying amounts of maxillary molar distalization depending on the appliance used. The Skeletal Frog appliance achieved approximately 4.14 mm of molar distalization [7], while the modified palatal plate produced around 3.3 mm [25, 28]. Clinically both groups resulted in class Ι molar relationship. The hybrid pendulum appliance showed slightly greater distalization, about 4.25 mm, whereas the dentally supported pendulum resulted in 3.21 mm of distal movement [14]. In comparison, the current study demonstrated that both appliances achieved substantial distalization (Leaf: −7.65 ± 0.74 mm; Hyrax: −6.95 ± 0.82 mm). While the Leaf Expander showed slightly greater distalization, the difference was not statistically significant after Bonferroni correction (p = 0.020). The effect size (d = 0.87) indicates a large clinical effect, highlighting that the Leaf Expander remains effective.
The angulation of the maxillary first molars relative to the palatal plane changed minimally by only 0.81° in Group 1 and 0.72° in Group 2, indicating non-significant changes in molar angulation; however, due to the use of the two dimensional cephalometric assessment, definitive conclusion regarding bodily movement cannot be drawn. This contrasts sharply with previous reports where the Skeletal Frog appliance exhibited 9.16° of molar tipping [7], the skeletally supported pendulum showed 9.09° [14], and the dentally supported pendulum caused 9.86° tipping [14]. The modified palatal plate demonstrated less tipping at 3.41° [25, 28]. These differences can be attributed to variations in the line of force application and the rigidity of the appliances, with more rigid designs and force vectors closer to the center of resistance resulting in reduced molar tipping.
It was worth to be mentioned that the current study depended on 2D lateral cephalometric analysis that limited the interpretation of the results for quality of distalization (bodily distalization or not) so it is recommended to use 3d CBCT analysis for future studies.
Incisor angulation and arch changes
Both groups showed minimal changes in upper and lower incisor inclination, indicating effective control over anterior anchorage. This aligns with results from other studies using skeletal anchorage [11, 12], in contrast to those using dental anchorage, which often show anterior proclination [7].
Arch length increased in both groups (Group 1: 6.32 mm, Group 2: 7.39 mm) as a result of bilateral molar distalization. Similar findings are reported across the literature, reinforcing that distalization appliances contribute to arch lengthening.
Transverse dimension changes
Both groups exhibited increases in inter-canine and inter-premolar widths, while a reduction in inter-molar width was noted. This finding is consistent with Ngan et al. [34], who attributed the narrowing to mesiolingual rotation of maxillary molars, likely due to the palatal positioning of the force vector, which lies lingual to the center of resistance.
Unlike the pendulum appliance, that tends to induce transverse expansion [14], the rigid connection in both appliances used in this study restricted transverse changes, leading to posterior crossbite tendencies. Based on this, it is advisable to remove the distalizing appliance following the distalization phase, and bond second molars during the fixed appliance phase to allow leveling and alignment.
Soft tissue response and duration
Mild gingival enlargement, seen in 3 patients across both groups, is likely a reactive response to pressure from the appliance on palatal soft tissues. This highlights the need for passive appliance fit to avoid overtightening of mini-screws and close monitoring of oral hygiene and tissue response.
A statistically significant difference in treatment duration was noted: Group 1 (Leaf Expander): 10.43 ± 1.52 months, Group 2 (HYRAX): 6.52 ± 1.52 months (p < 0.001).This difference may be attributed to the mode of force delivery self-activation in Leaf Expander versus manual activation in Hyrax.
Limitations
Short-term follow-up; long-term stability of molar distalization and transverse changes not assessed. Small sample size: the future study should be applied on larger sample size.
Single-center study; results may not extrapolate to different populations. Treatment duration difference is attributed to force delivery mode, but no biomechanical quantification of force was provided.
Absence of 3D assessment: It was worth to be mentioned that the current study depended on 2D lateral cephalometric analysis that limited the interpretation of the results for quality of distalization (bodily distalization or not) so it is recommended to use 3d CBCT analysis for future studies.
Recommendations
Appliance Selection: For effective maxillary molar distalization with minimal molar tipping, skeletally anchored appliances with rigid connections such as the modified Leaf Expander and conventional Hyrax expander are recommended over flexible designs like the Skeletal Frog or pendulum appliances.
Screw Length and Placement: Using longer mini-screws (around 11–13 mm) that engage both the palatal and nasal cortical bone in the anterior Para median palatal region enhances appliance stability and anchorage, improving treatment outcomes. Monitoring and Management of Soft Tissue: Careful appliance fitting is essential to avoid gingival enlargement or mucosal irritation. Passive fit without pressure points should be ensured, and patients must be instructed on oral hygiene and monitoring during treatment. Also soft tissue profile measurements can be performed in future studies.
Post-Distalization Protocol: Since some reduction in inter-molar width and posterior crossbite tendencies may occur, it is advisable to remove distalizing appliances promptly after achieving distalization and proceed with fixed orthodontic treatment to align and level the molars. Long-term Multicenter trials with larger sample sizes to assess stability and relapse after distalization to validate findings with 3D-based studies.
Conclusions
Within the limitations of this single-center, short-term randomized clinical trial, both appliances produced effective molar distalization with minimal angular changes on lateral cephalometric assessment. The self-activated Leaf Expander demonstrated a longer treatment duration compared to the conventional Hyrax expander, likely due to differences in force delivery mechanisms.
Minimal changes in molar angulation and incisor inclination indicate that both appliances successfully prevented undesirable tipping and anterior proclination. The rigid skeletal anchorage and force application contributed to effective molar distalization with reduced side effects.
Both appliances increased arch length but resulted in decreased inter-molar width, highlighting the need for careful post-distalization orthodontic management.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Namara JA Jr. Components of class II malocclusion in children 8–10 years of age. Angle Orthod. 1981;51(3):177–202. 10.1043/0003-3219(1981)051%3C;0177:COCIMI%3E;2.0.CO;2. PMID: 7023290.10.1043/0003-3219(1981)051<0177:COCIMI>2.0.CO;27023290 · doi ↗ · pubmed ↗
- 2Ghosh J, Nanda RS. Evaluation of an intraoral maxillary molar distalization technique. Am J Orthod Dentofacial Orthop. 1996;110(6):639–46. 10.1016/s 0889-54069680041-2. PMID: 8972811.10.1016/s 0889-5406(96)80041-28972811 · doi ↗ · pubmed ↗
- 3Fathy Abo-Elmahasen MM, Abo Dena AS, Zhran M, Albohy SAH. Do silver/hydroxyapatite and zinc oxide nano-coatings improve inflammation around titanium orthodontic mini-screws? In vitro study. Int Orthod. 2023;21. 10.1016/j.ortho.2022.100711.10.1016/j.ortho.2022.10071136463787 · doi ↗ · pubmed ↗
- 4Aboelmahasen MMF, Othman SS, Dena ASA, Zhran M, Ma M, El-Destawy MT, et al. Histomorphometric and CBCT comparison of osseointegration around orthodontic titanium miniscrews coated with different nanoparticles: an in-vivo animal study. Int Orthod. 2024;22. 10.1016/j.ortho.2023.100823.10.1016/j.ortho.2023.10082337992473 · doi ↗ · pubmed ↗
- 5Elnagar MH, Elshourbagy E, Ghobashy S, Khedr M, Evans CA. Dentoalveolar and arch dimension changes in patients treated with miniplate-anchored maxillary protraction. Am J Orthod Dentofac Orthop. 2017;151(6):1092–106 10.1016/j.ajodo.2016.10.038. PMID: 28554455.10.1016/j.ajodo.2016.10.03828554455 · doi ↗ · pubmed ↗
- 6Ngan P, Moon W. Evolution of class III treatment in orthodontics. Am J Orthod Dentofacial Orthop. 2015;148(1):22–36 10.1016/j.ajodo.2015.04.012. PMID: 26124025.10.1016/j.ajodo.2015.04.01226124025 · doi ↗ · pubmed ↗