Muscle damage in oblique lumbar interbody fusion and unilateral biportal endoscopic-transforaminal lumbar interbody fusion for single-level lumbar degeneration diseases: retrospective cohort study
Tangyiheng Chen, Xin Wang, Renjie Li, Sen Yang, Xuefeng Li, Yi Zhu, Hong Zhou, Ying Zhuang, Han Sun, Weimin Jiang, Yijie Liu

TL;DR
This study compares muscle damage from two types of lumbar fusion surgeries, finding that one causes less muscle damage and is safer for patients.
Contribution
The study provides a direct comparison of muscle damage between OLIF and UBE-TLIF surgeries using cross-sectional muscle area measurements.
Findings
OLIF resulted in significantly less blood loss, shorter operation time, and lower creatine kinase levels compared to UBE-TLIF.
OLIF caused less damage to paraspinal muscles but more damage to psoas muscles compared to UBE-TLIF.
The incidence of complications was similar between the two surgical approaches.
Abstract
Iatrogenic injury and approach-related complications in lumbar fusion surgery have become significant concerns. This study aims to assess the muscle damage with oblique lumbar interbody fusion (OLIF) compared with unilateral biportal endoscopic-transforaminal lumbar interbody fusion (UBE-TLIF). This assessment will guide better clinical surgical choice in lumbar degeneration diseases. This was a retrospective study comparing OLIF combined with anterolateral single screw–rod fixation and UBE-TLIF combined with percutaneous pedicle screws under navigation from January 2021 to December 2023. Individuals with single-level degenerative lumbar disease participated in the study. This study compared the baseline and perioperative parameters (blood loss, operation time, and haematological indicators) and clinical outcome (visual analogue scale scores, Japanese Orthopaedic Association scores,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
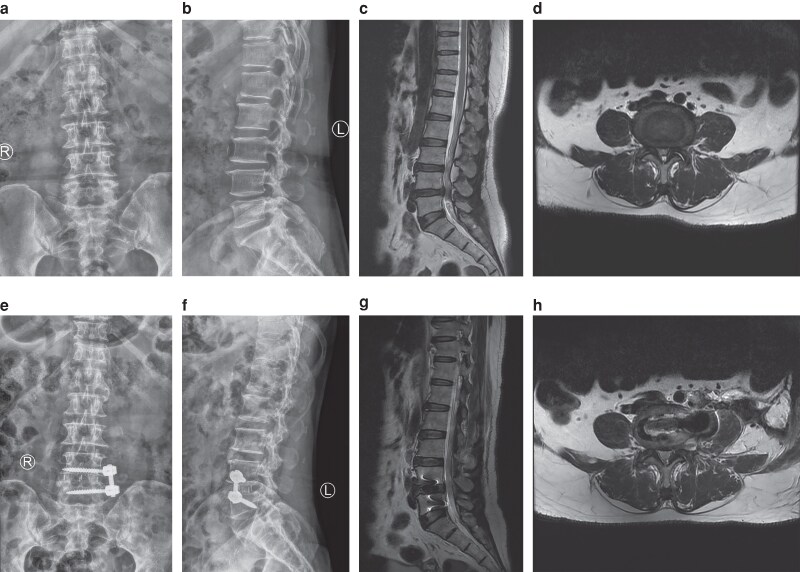 Fig. 1
Fig. 1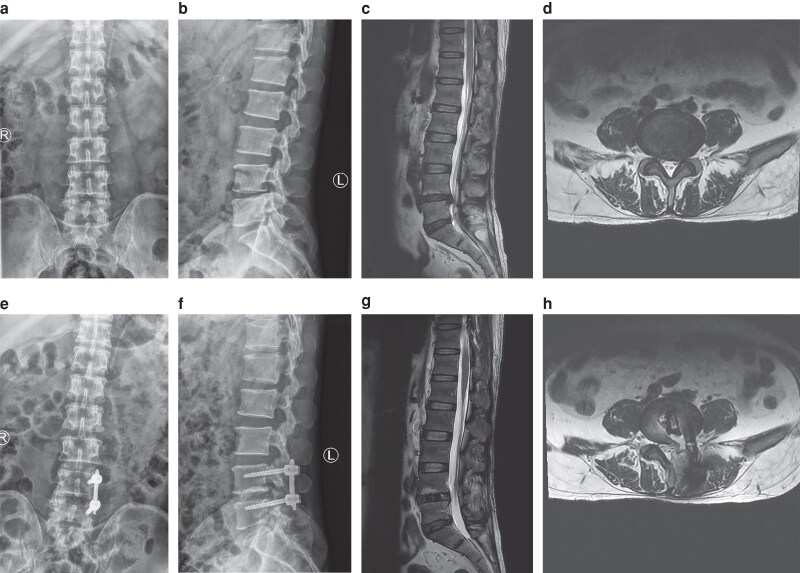 Fig. 2
Fig. 2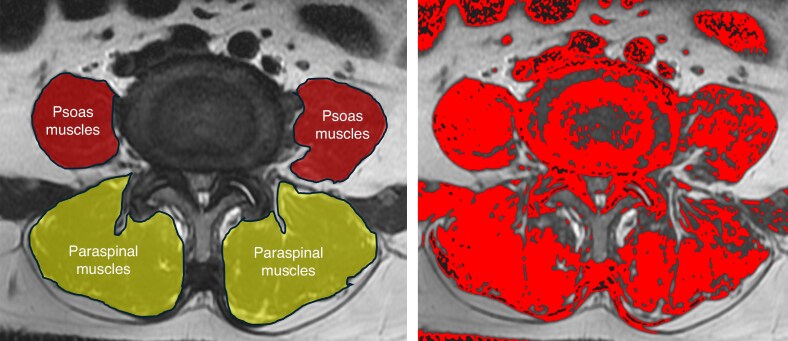 Fig. 3
Fig. 3| OLIF ( | UBE-TLIF ( |
| |
|---|---|---|---|
|
| 0.883 | ||
| Male | 48 (42.9%) | 36 (45.0%) | |
| Female | 64 (57.1%) | 44 (55.0%) | |
| Age (years), mean(s.d.) | 65.1(5.4) | 64.6(6.6) | 0.601 |
| BMI (kg/m2), mean(s.d.) | 24.2(2.7) | 24.1(2.6) | 0.786 |
|
| 0.957 | ||
| Lumbar spinal canal stenosis | 80 (71.4%) | 56 (70.0%) | |
| Lumbar disc herniation | 32 (28.6%) | 24 (30.0%) | |
|
| 0.701 | ||
| L3-4 | 32 (28.6%) | 20 (25.0%) | |
| L4-5 | 80 (71.4%) | 60 (75.0%) | |
| Operation time (min), mean(s.d.) | 89.9(13.0) | 121.5(14.7) | < 0.001 |
| Blood loss (ml), mean(s.d.) | 29.8(9.9) | 59.0(24.7) | < 0.001 |
| OLIF ( | UBE-TLIF ( |
| |
|---|---|---|---|
|
| |||
| Preoperative, mean(s.d.) | 8.3(1.4) | 8.4(1.5) | 0.710 |
| Postoperative 3 days, mean(s.d.) | 3.1(1.0) | 4.3(1.4) | < 0.001 |
| 1 month, mean(s.d.) | 1.6(1.0) | 1.9(1.3) | 0.108 |
| 3 months, mean(s.d.) | 1.6(0.9) | 1.7(1.1) | 0.592 |
| 12 months, mean(s.d.) | 1.5(0.9) | 1.5(1.0) | 1.000 |
|
| |||
| Preoperative, mean(s.d.) | 8.5(1.3) | 8.4(1.4) | 0.340 |
| Postoperative 3 days, mean(s.d.) | 4.0(1.2) | 3.0(0.9) | < 0.001 |
| 1 month, mean(s.d.) | 1.9(0.8) | 1.8(1.0) | 0.347 |
| 3 months, mean(s.d.) | 1.8(0.9) | 1.7 (1.0) | 0.383 |
| 12 months, mean(s.d.) | 1.6(0.9) | 1.6(1.1) | 0.777 |
|
| |||
| Preoperative, mean(s.d.) | 8.2(1.0) | 8.0(1.0) | 0.142 |
| Postoperative 3 days, mean(s.d.) | 13.0(1.2) | 13.1(1.0) | 0.545 |
| 1 month, mean(s.d.) | 15.3(1.1) | 15.3(1.3) | 0.959 |
| 3 months, mean(s.d.) | 15.5(0.9) | 15.6(1.1) | 0.597 |
| 12 months, mean(s.d.) | 15.7(0.8) | 15.9(1.0) | 0.086 |
|
| 0.362 | ||
| Grade I | 76 (67.9%) | 60 (75.0%) | |
| Grade II | 36 (32.1%) | 20 (25.0%) | |
| Grade III | 0 (0.0%) | 0 (0.0%) | |
| Grade IV | 0 (0.0%) | 0 (0.0%) | |
|
| 17.8% | 18.7% | 0.874 |
| Spinal cord hypertension syndrome | 0 (0.0%) | 8 (10.0%) | |
| Dural injury | 0 (0.0%) | 4 (5.0%) | |
| Hip flexion weakness | 12 (10.7%) | 0 (0.0%) | |
| Cage subsidence | 8 (7.1%) | 3 (3.7%) | |
| Vascular or peritoneal injury | 0 (0.0%) | 0 (0.0%) |
| OLIF ( | UBE-TLIF ( |
| |
|---|---|---|---|
| Preoperative HCT (%) | 39.9(2.4) | 39.5(2.3) | 0.367 |
| Postoperative HCT (%) | 37.6(3.4) | 35.4(3.1) | < 0.001 |
| Preoperative Hb (g/L) | 135.3(8.7) | 135.1(8.4) | 0.882 |
| Postoperative Hb (g/L) | 127.9(10.3) | 122.5(10.7) | < 0.001 |
| Preoperative RBC | 4.3(0.3) | 4.3(0.3) | 0.893 |
| Postoperative RBC | 4.1(0.4) | 3.9(0.3) | < 0.001 |
| Preoperative albumin | 42.6(3.2) | 42.7(2.1) | 0.670 |
| Postoperative albumin | 38.9(2.7) | 38.8(2.0) | 0.862 |
| Preoperative prealbumin | 239.7.2(51.3) | 232.0(51.5) | 0.306 |
| Postoperative prealbumin | 215.9.9(45.9) | 208.2(48.6) | 0.268 |
| Preoperative CK | 144.8(94.7) | 151.4(93.2) | 0.783 |
| Postoperative CK | 176.3(124.5) | 421.6(220.9) | < 0.001 |
| Postoperative CRP | 17.9(10.0) | 18.0(7.0) | 0.917 |
| Postoperative WBC | 13.4(1.8) | 13.4(2.3) | 0.783 |
| OLIF ( | UBE-TLIF ( |
| |
|---|---|---|---|
|
| |||
| Preoperative TCSA (mm2), mean(s.d.) | 976.8(209.3) | 1022.0(171.3) | 0.114 |
| Postoperative TCSA (mm2), mean(s.d.) | 1122.1(248.6) | 1117.2(167.4) | 0.869 |
| Change in TCAS (mm2), mean(s.d.) | 145.4(89.4) | 95.2(33.4) | < 0.001 |
| Goutallier classification | 0.483 | ||
| Grade 0 | 0 (0.0%) | 0 (0.0%) | |
| Grade 1 | 29 (25.9%) | 16 (20.0%) | |
| Grade 2 | 55 (49.1%) | 40 (50.0%) | |
| Grade 3 | 21 (18.7%) | 21 (26.3%) | |
| Grade 4 | 7 (6.3%) | 3 (3.7%) | |
|
| |||
| Preoperative TCSA (mm2), mean(s.d.) | 1855.3(271.5) | 1822.0(203.3) | 0.333 |
| Postoperative TCSA (mm2), mean(s.d.) | 1910.6(289.7) | 2133.0(247.6) | < 0.001 |
| Change in TCAS (mm2), mean(s.d.) | 55.3(208.4) | 311.1(145.0) | < 0.001 |
| Goutallier classification | < 0.001 | ||
| Grade 0 | 20 (17.9%) | 0 (0.0%) | |
| Grade 1 | 72 (64.3%) | 8 (10.0%) | |
| Grade 2 | 20 (17.8%) | 32 (40.0%) | |
| Grade 3 | 0 (0.0%) | 36 (45.0%) | |
| Grade 4 | 0 (0.0%) | 4 (5.0%) |
- —Research on collaborative innovation of medical and industrial integration in Suzhou10.13039/501100020450
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Cervical and Thoracic Myelopathy · Scoliosis diagnosis and treatment
Introduction
Lumbar fusion surgery is a commonly employed procedure for various spinal ailments. Traditional open posterior approaches that necessitate extensive dissection of the paraspinal musculature can lead to permanent denervation of the erector spinae, functional loss, and late-onset spinal instability. Consequently, iatrogenic injury to the paraspinal muscles, disruption of the posterior tension band, and approach-related complications have become significant concerns. Recently, there has been increased interest in the role of paravertebral muscles as predictors of surgical outcomes in spinal procedures. Research indicates that the elevation and continuous wide retraction of paraspinal muscles can result in ischaemia, denervation, and dysfunction, which contribute to chronic pain and suboptimal postoperative clinical outcomes^1–3^. Tsutsumimoto et al.^4^ suggest that the sustained stretching of paraspinal muscles caused by retractors elevates the pressure within these muscles, adversely affecting the blood perfusion of their capillaries during traditional open surgery. This ischaemic change in paraspinal muscles ultimately leads to functional alterations and muscle atrophy. Alarmingly, statistics reveal that approximately 30% of patients experience exacerbated back pain after surgery compared with their preoperative status^5^. Thus, iatrogenic muscle injury has emerged as a major concern for practising spine surgeons.
Several studies emphasize the prevalence of invasive muscle damage associated with posterior spinal surgeries. For instance, the traditional procedure of posterior lumbar interbody fusion has been demonstrated to lead to increased degeneration of the multifidus muscle and heightened postoperative low back pain when contrasted with minimally invasive methods like percutaneous pedicle screw fixation^6,7^. Consequently, minimally invasive spine surgery has garnered increasing attention in recent years. The rapid advancement of endoscopic techniques over the past few decades has facilitated the application of spinal endoscopic methods to lumbar intervertebral fusion surgery. Recently, unilateral biportal endoscopic-transforaminal lumbar interbody fusion (UBE-TLIF) has emerged as a notable technique, as it features independent endoscopic and instrument channels. Furthermore, the efficacy and validity of minimally invasive lumbar interbody fusions utilizing percutaneous pedicle screws for spondylodiscitis have been documented^8,9^. Clinical trials^10^ indicate that these minimally invasive interbody fusions effectively minimize muscle injuries. In addition, oblique lumbar interbody fusion (OLIF) is becoming increasingly popular among spinal surgeons because of its minimally invasive nature. This method is specifically aimed at the anterolateral region of the intervertebral disc located between the psoas major and major vasculature through the oblique lateral corridor. Additionally, the Wiltse technique reduces damage to the posterior paravertebral muscles, which in turn lowers the likelihood of experiencing chronic low back pain following surgery^11,12^. Additionally, OLIF facilitates correction of spondylolisthesis and rotatory deformities, as well as indirect nerve decompression through ligamentotaxis. These benefits may lead to reduced surgical pain and expedited recovery compared with traditional surgical methods^13^.
The advantages of minimally invasive techniques over open techniques include reduced blood loss, less surgical site pain, faster recovery, and a lower incidence of postoperative wound infections. The aim of this study was to assess the muscle changes at the operated level in OLIF compared with UBE-TLIF. This assessment will provide insight into the potential disability patients may experience during their postoperative period. To evaluate the invasiveness and tolerability of UBE-TLIF in comparison with OLIF, this study assessed serum markers of muscle damage and inflammation, conducted quantitative analyses using magnetic resonance imaging (MRI), and measured surgical pain, blood loss, and postoperative recovery of activities.
Methods
Basic demographics and serology
This study was conducted at six participating centres in China. The study duration was from January 2021 to December 2023. Ethical approval was received from the Institutional Ethics committee, reference number 211046. This is a retrospective study. Individuals with single-level degenerative lumbar disease participated in the study. Before the operation, patients were told the disadvantages and advantages of the two procedures. They could choose the procedure themselves. Informed consent was obtained from those who agreed to allow the use of clinical data, including imaging. Routine follow-up was performed at 3 days, 1 month, 3 months, 6 months, 1 year after surgery, and then every 6 months thereafter. All patients were followed up for at least 24 months. If one patient was followed up for two years, then the final follow-up was 2 years. Exclusions from the study included patients undergoing revision lumbar surgery, those who had decompression-only procedures, individuals with multilevel fusion surgeries, those with diagnoses unrelated to degenerative conditions (such as infection, tumours, and so on), or those with a previous history of radiation treatment.
Demographic data for both groups were gathered before surgery, and included age, sex, body mass index (BMI), diagnosis, and the specific surgical level. Information related to the perioperative period, such as surgical duration, blood loss, and haematological markers, was documented both before and after the operation. A strobe checklist was added in the supplementary template.
Clinical and radiological indicators
The baseline health status of patients was assessed both before and after surgery. Japanese Orthopaedic Association (JOA) and visual analogue scale (VAS) scores were documented before surgery as well as at 3 days, 1 month, 3 months, and 12 months following the operation. The fusion rate was evaluated using Bridwell’s fusion grading system^11^ at the 3-month, 6-month, and final follow-up periods. Spinal fusion was categorized as grades I and II. Two independent observers conducted all radiographic assessments, and the average of their measurements was utilized for analysis. Additionally, any perioperative complications were noted. The typical cases are shown in Fig. 1 and Fig. 2.
A 63-year-old female with lumbar disc herniation who underwent L4-5 oblique lumbar interbody fusion a, b preoperative anterolateral X-ray; c preoperative T2 sagittal MRI showed L4-5 herniation; d preoperative T2 axial MRI; e, f postoperative anterolateral X-ray; g preoperative T2 sagittal MRI; h preoperative T2 axial MRI. MRI, magnetic resonance imaging.
A 56-year-old male with lumbar disc herniation who underwent L4-5 unilateral biportal endoscopic-transforaminal lumbar interbody fusion a, b preoperative anterolateral X-ray; c preoperative T2 sagittal MRI showed L4-5 herniation; d preoperative T2 axial MRI; e, f postoperative anterolateral X-ray; g preoperative T2 sagittal MRI; h preoperative T2 axial MRI. MRI, magnetic resonance imaging.
Muscle assessments were performed by trained research staff on standard axial T2-weighted MRI, specifically targeting the mid-disk space for both psoas and paraspinal muscles using Image J (Fig. 3). A spine surgeon and two clinical researchers received comprehensive training in the Goutallier classification system^14^, with cases assigned randomly without previous knowledge of the specific procedure. The muscle grading criteria were as follows: grade 0 indicates no intramuscular fat; grade 1 indicates the presence of minor fatty streaks; grade 2 shows fat that is apparent but still less than the muscle tissue; grade 3 signifies an equal amount of fat and muscle; and grade 4 denotes a higher fat content compared with muscle tissue.
Bilateral manual segmentation of psoas and posterior paraspinal muscles on preoperative axial T2-weighted magnetic resonance imagingCross-sectional area measured by Image J.
Statistical analysis
Analyses of statistical data were conducted using SPSS^®^ Statistics version 26.0 (IBM, Armonk, NY, USA). For parametric data, results are reported as mean(standard deviation(s.d.)) and analysed using the Student t-test. Nonparametric data are expressed as median (i.q.r.) and are evaluated with the Mann-Whitney U-test. Nominal data were analysed using the chi-square test. *P-*values of less than 0.05 were deemed statistically significant.
Results
This retrospective study enrolled 192 patients: 112 OLIF with lateral vertebral screws and 80 UBE-TLIF with percutaneous pedicle screws under navigation. Patient demographics and preoperative characteristics are summarized in Table 1. There were no statistical differences in the age, sex, BMI, lesion level, and preoperative diagnoses between patients undergoing OLIF and UBE-TLIF. The operation time of OLIF was shorter than UBE-TLIF (89.9 ± 13.0 minutes (min) versus 121.5 ± 14.7 min; P < 0.001), and the blood loss with OLIF was less than with UBE-TLIF (29.8 ± 9.9 ml versus 59.0 ± 24.7 ml; P < 0.001).
Comparison of follow-up clinical outcomes are outlined in Table 2. The mean(s.d.) VAS scores decreased, and the corresponding JOA scores increased in both groups. The VAS scores of the back with OLIF were lower than those with UBE-TLIF at 3 days after surgery, whereas the VAS scores of the leg with OLIF were higher than those with UBE-TLIF. At 1 month, 3 months, and 12 months, there were no significant differences between two groups. In the OLIF group, using Bridwell’s fusion grading system^11^, there were 76 grade I and 36 grade II. In the UBE-TLIF group, there were 60 grade I and 20 grade II. The fusion rates did not differ between the two groups (P = 0.362).
There was no significant difference between the OLIF group and the UBE-TLIF group with regards to the rate of complications (17.8% versus 18.7%; P = 0.874). Specifically, in the OLIF group, 12 patients experienced hip flexion weakness. The symptoms completely disappeared after relieving swelling treatment and routine guidance of functional exercise. Eight patients experienced cage subsidence; however, they achieved good fusion with osteogenesis therapy in the last follow-up. In the UBE-TLIF group, eight patients experienced spinal cord hypertension syndrome. The symptoms completely disappeared after sedation and hormone treatment. Four patients experienced dural injury. They recovered well after treatment such as reducing stress and anti-infective therapy. Three patients experienced cage subsidence. They achieved good fusion in the last follow-up. There was no vascular or peritoneal injury in either group.
Blood and biochemical tests are shown in Table 3. There were no significant differences in the levels of albumin and prealbumin before and after surgery, whereas the differences were significant for hematocrit, haemoglobin, and red blood cell levels. C-reactive protein (CRP) and white blood cell (WBC) levels increased after surgery. However, there were no significant differences between OLIF and UBE-TLIF. Postoperative creatine kinase (CK) increased significantly with UBE-TLIF compared with OLIF (mean(s.d) 421.6(220.9) U/L versus 176.3(124.5) U/L; P < 0.001).
The changes in TCSA in the psoas muscles were significantly higher in the OLIF group than in the UBE-TLIF group (mean(s.d.) 145.4(89.4) mm^2^ versus 95.2(33.4) mm^2^; P < 0.001). The changes in the total cross-sectional area (TCSA) in the paraspinal muscles were significantly lower in the OLIF group than in the UBE-TLIF group (mean(s.d.) 55.4(208.4) mm^2^ versus 311.1(145.0) mm^2^; P < 0.001). According to Goutallier classification, there were 0 grade 0, 29 grade 1, 55 grade 2, 21 grade 3 and 7 grade 4 for the psoas muscles in the OLIF group; 0 grade 0, 16 grade 1, 40 grade 2, 21 grade 3, and 3 grade 4 for the psoas muscles in the UBE-TLIF group; 20 grade 0, 72 grade 1, 20 grade 2, 0 grade 3, and 0 grade 4 for the paraspinal muscles in the OLIF group; and 0 grade 0, 8 grade 1, 32 grade 2, 36 grade 3, and 4 grade 4 for the paraspinal muscles in the UBE-TLIF group. There were significant differences in the fatty infiltration of paraspinal muscles between the two groups (Table 4).
Discussion
Minimally invasive spine surgery was developed as a potential solution to reduce the incidence of iatrogenic soft-tissue injury while still achieving the traditional goals of open procedures. Two typical surgical techniques are OLIF and UBE-TLIF. OLIF employs a retroperitoneal fat and lumbar major muscle gap approach, effectively avoiding critical neurovascular structures, and is therefore gradually gaining acceptance among spine surgeons. The UBE-TLIF technique establishes its working area within the trigone of the multifidus muscle, utilizing the potential gap between the multifidus and the spinous process of the posterior lamina^15^. UBE-TLIF allows for the identification and complete removal of cartilage endplates under direct endoscopic visualization, creating an optimal environment for intervertebral fusion. The operation time of the UBE-TLIF group remained significantly longer than that of the OLIF group in this study. Such delicate endoscopic manipulation not only necessitates surgical experience but may also be time-consuming, potentially explaining why the UBE-TLIF group experienced longer surgical durations compared with OLIF. There were no severe complications requiring revision in either group. The different complications in the two groups were determined by the different characteristics of the two approaches. Specifically, because of the hydraulic pressure, cases of spinal cord hypertension syndrome occurred after UBE-TLIF. However, the symptoms completely disappeared after sedation and hormone treatment. Because of the irritation of the psoas muscle, hip flexion weakness occurred after OLIF. However, the symptoms completely disappeared after relieving swelling treatment and routine guidance of functional exercise. All the complications were temporary or disappeared after appropriate treatment. This indicates that both techniques are safe and effective.
In this study, both VAS scores and JOA scores showed significant improvement in both groups at each time point when compared with preoperative measurements. The clinical outcomes at 1 month, 3 months, and 1 year were comparable between the groups, with no significant differences observed. This suggests that both surgical techniques are advantageous for patients with lumbar degenerative disease, yielding similar medium- and short-term clinical results. Notably, for VAS scores related to back pain, the OLIF group demonstrated superior outcomes compared with the UBE-TLIF group at 3 days after surgery. This advantage can be attributed to the OLIF technique's preservation of the posterior spinal muscles and avoidance of bony structures such as the laminae, which minimizes peripheral tissue damage and reduces the risk of medically induced neurological disorders^16^. Conversely, for VAS scores concerning leg pain, the UBE-TLIF group outperformed the OLIF group at 3 days after surgery, likely due to the irritation of the psoas muscles caused by anterolateral single screw-rod fixation, which can lead to hip flexion weakness.
The use of serum markers for inflammation and muscle damage provides objective measures of the invasiveness of surgical procedures. Creatine kinase (CK) acts as a quantitative measure of muscle injury, and a relationship is noted between CK levels and the pressure applied to paraspinal muscles during retraction^17,18^. In a prospective cohort investigation, Arts et al.^19^ identified a dose–response relationship linking CK levels and the extent of surgical invasiveness. Muscle injury associated with spinal surgery leads to a rise in serum CK concentration, which is commonly employed for assessing muscle injury in the immediate postoperative period. In the authors’ research, both CRP and WBC levels showed an increase following surgery; however, significant differences were not observed between the OLIF group and the UBE-TLIF group. Kawaguchi et al.^17,20^ determined that back muscle injury, as indicated by elevated serum creatine phosphokinase levels, is directly related to retraction pressure, duration, and the extent of surgical exposure. Notably, postoperative CK levels were significantly higher in UBE-TLIF compared with OLIF. The findings of the authors of the present study suggest that, whereas both procedures improve various clinical outcome measures, OLIF significantly reduces paraspinal muscle injury relative to UBE-TLIF, as evidenced by less blood loss, lower serum CK levels, and a reduced incidence of postoperative low back pain.
In this retrospective study, the quantitative changes were examined in the occurring morphology of the psoas and paraspinal muscles. Kang et al.^21^ confirmed through MRI that the degree of paraspinal muscle degeneration can be assessed by the decrease in paraspinal muscle CSA and fatty infiltration. The changes in TCSA of the psoas muscles were significantly greater in the OLIF group compared with the UBE-TLIF group. Conversely, the changes in TCSA of the paraspinal muscles were significantly lower in the OLIF group than in the UBE-TLIF group. Notably, there were significant differences in the fatty infiltration of paraspinal muscles between the two groups. Previous studies^22^ have indicated that the reduction in muscle volume and the increase in fat deposition are primary characteristics of paraspinal muscle degeneration. In an animal model, the duration of retraction on the multifidus muscle was identified as a critical factor contributing to muscle injury and atrophy, with oedema, necrosis, and inflammation primarily occurring in the early stages, whereas fatty degeneration became pronounced 12 weeks after surgery and beyond^23^. This phenomenon aligns with the findings of this study. The fatty infiltration of the lumbar multifidus muscles following posterior surgeries is clinically associated with low back pain, which may explain why several patients experienced back pain after undergoing UBE-TLIF. Paraspinal muscle dysfunction, resulting from degeneration in the postoperative period, plays a crucial role in the progression to failed back syndrome. The utilization of UBE involves two notches to create passage channels (one for observation and another for operation) along with the ion-knife separation of portions of the paravertebral muscle and lamina attachment points, which results in artificially created cavities. Concurrently, the procedure continues to utilize high-pressure saline for irrigation. The repeated insertion and removal of instruments leads to greater injury to the paravertebral muscles. Kambin et al.^24^ conducted a follow-up study on 88 patients with lumbar degenerative diseases who underwent UBE surgery, assessing the extent of paravertebral muscle injury via MRI. Their findings indicated that the degree of postoperative ipsilateral paravertebral muscle injury increased with prolonged operation time, consequently extending recovery periods. Regarding the psoas muscles, the radiological assessment of the postoperative changes in the psoas major by the authors of the present study indicated that the TCSA on the approach side significantly increased after surgery, with a notable rise in the mean TCSA ratio in the OLIF group. They hypothesize that this condition may be attributed to temporary postoperative swelling resulting from intraoperative muscle retraction, suggesting that the OLIF approach minimally impacts the psoas major. Furthermore, this study considered that swelling of the psoas major or haematoma formation could have occurred due to surgical manipulation and irritation of the screw tail cap. Several patients experienced transient clinical weakness of hip flexion. Radiologically, some degree of atrophy was observed, likely due to compromised microcirculation in the psoas muscle; however, spontaneous recovery was noted in the later stages.
Some limitations of the present study warrant discussion. The hip flexor muscles include the iliopsoas, pectineus, rectus femoris, and adductor longus. This study assessed hip flexion weakness as an indicator of psoas muscle injury. However, isolating the specific muscle action proved challenging. Furthermore, this study did not conduct a histopathological assessment of the muscle, relying solely on MRI to evaluate muscle degeneration.
In conclusion, both OLIF and UBE-TLIF yield favourable outcomes in the management of single-level degenerative lumbar diseases. After surgery, OLIF was associated with temporary swelling of the psoas muscle; however, long-term damage to the psoas was not significant, and there was no evident damage to the erector spinae and multifidus muscles. In comparison with UBE-TLIF, OLIF demonstrated lower creatine kinase levels, reduced blood loss, and less muscle damage. Consequently, in cases where both procedures are equally indicated, OLIF is advocated as the safer and less-invasive option, making it the preferred choice for patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stevens KJ, Spenciner DB, Griffiths KL, Kim KD, Zwienenberg-Lee M, Alamin T et al Comparison of minimally invasive and conventional open posterolateral lumbar fusion using magnetic resonance imaging and retraction pressure studies. J Spinal Disord Tech 2006;19:77–8616760779 10.1097/01.bsd.0000193820.42522.d 9 · doi ↗ · pubmed ↗
- 2Ren G, Eiskjær S, Kaspersen J, Christensen FB, Rasmussen S. Microdialysis of paraspinal muscle in healthy volunteers and patients underwent posterior lumbar fusion surgery. Eur Spine J 2009;18:1604–160919418074 10.1007/s 00586-009-1021-x PMC 2899392 · doi ↗ · pubmed ↗
- 3Fritzell P, Hägg O, Wessberg P, Nordwall A. Chronic low back pain and fusion: a comparison of three surgical techniques: a prospective multicenter randomized study from the Swedish lumbar spine study group. Spine (Phila Pa 1976) 2002;27:1131–114112045508 10.1097/00007632-200206010-00002 · doi ↗ · pubmed ↗
- 4Tsutsumimoto T, Shimogata M, Ohta H, Misawa H. Mini-open versus conventional open posterior lumbar interbody fusion for the treatment of lumbar degenerative spondylolisthesis: comparison of paraspinal muscle damage and slip reduction. Spine (Phila Pa 1976) 2009;34:1923–192819652636 10.1097/BRS.0b 013e 3181 a 9d 28e · doi ↗ · pubmed ↗
- 5Cha J-R, Kim Y-C, Yoon W-K, Lee W-G, Kim T-H, Oh J-K et al The recovery of damaged paraspinal muscles by posterior surgical treatment for patients with lumbar degenerative diseases and its clinical consequence. J Back Musculoskelet Rehabil 2017;30:801–80928372312 10.3233/BMR-150455 · doi ↗ · pubmed ↗
- 6Fan S, Hu Z, Zhao F, Zhao X, Huang Y, Fang X. Multifidus muscle changes and clinical effects of one-level posterior lumbar interbody fusion: minimally invasive procedure versus conventional open approach. Eur Spine J 2010;19:316–32419876659 10.1007/s 00586-009-1191-6PMC 2899808 · doi ↗ · pubmed ↗
- 7Kim D-Y, Lee S-H, Chung SK, Lee H-Y. Comparison of multifidus muscle atrophy and trunk extension muscle strength: percutaneous versus open pedicle screw fixation. Spine (Phila Pa 1976) 2005;30:123–12915626992 · pubmed ↗
- 8Youssef JA, Mc Afee PC, Patty CA, Raley E, De Bauche S, Shucosky E et al Minimally invasive surgery: lateral approach interbody fusion: results and review. Spine (Phila Pa 1976) 2010;35:S 302–S 31121160394 10.1097/BRS.0b 013e 3182023438 · doi ↗ · pubmed ↗