Diagnosing Urinary Tract Infection in Young Febrile Children in the Emergency Department
Ceilidh Kinlin, Jocelyn Gravel, Nick Barrowman, Vid Bijelik, Ramona Cook, Natasha Wills-Ibarra, Roger Zemek, Nader Shaikh, Maala Bhatt

TL;DR
UTICalc version 3.0 is a reliable tool for predicting urinary tract infections in young febrile children in emergency departments, potentially reducing unnecessary testing.
Contribution
Prospectively validated UTICalc version 3.0 as a race-neutral UTI prediction model for young children in emergency settings.
Findings
UTICalc clinical model achieved an AUROC of 84.1% for predicting UTIs in febrile children.
Incorporating dipstick results increased the model's AUROC to 95.3%.
UTICalc showed strong calibration and net benefit across various risk thresholds.
Abstract
What is the diagnostic accuracy of UTICalc version 3.0 in predicting urinary tract infections (UTIs) for febrile children aged 2 to 24 months in the emergency department? In this diagnostic study with 2561 children, UTICalc showed strong discrimination, with an area under the receiver operating characteristic curve (AUROC) of 84.1% for the clinical model and an AUROC of 95.3% for the clinical and dipstick model. In this study, UTICalc had high accuracy in identifying UTIs in young febrile children, which may help guide testing and treatment decisions in the emergency department. This diagnostic study validates UTICalc version 3.0, a race-neutral prediction model for urinary tract infections in children, and evaluates its clinical utility among children aged 2 to 24 months presenting to the emergency department with fever. Diagnosing urinary tract infection (UTI) in preverbal,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
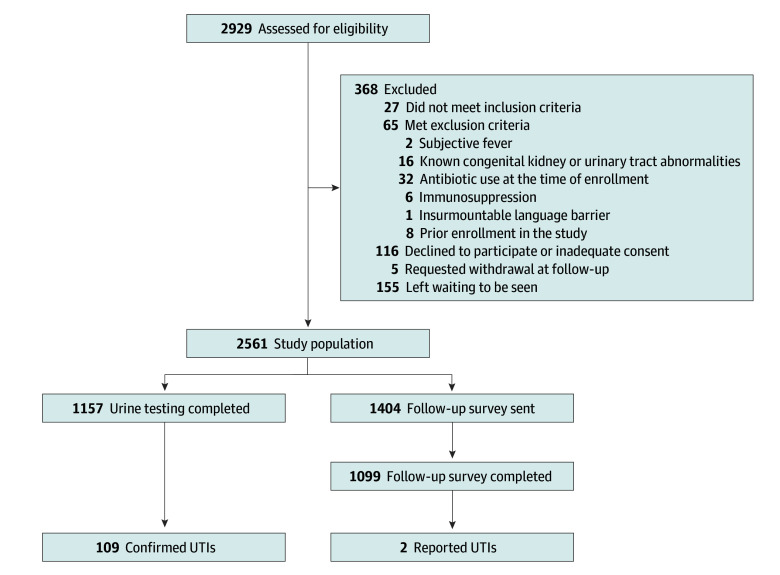 Figure 1
Figure 1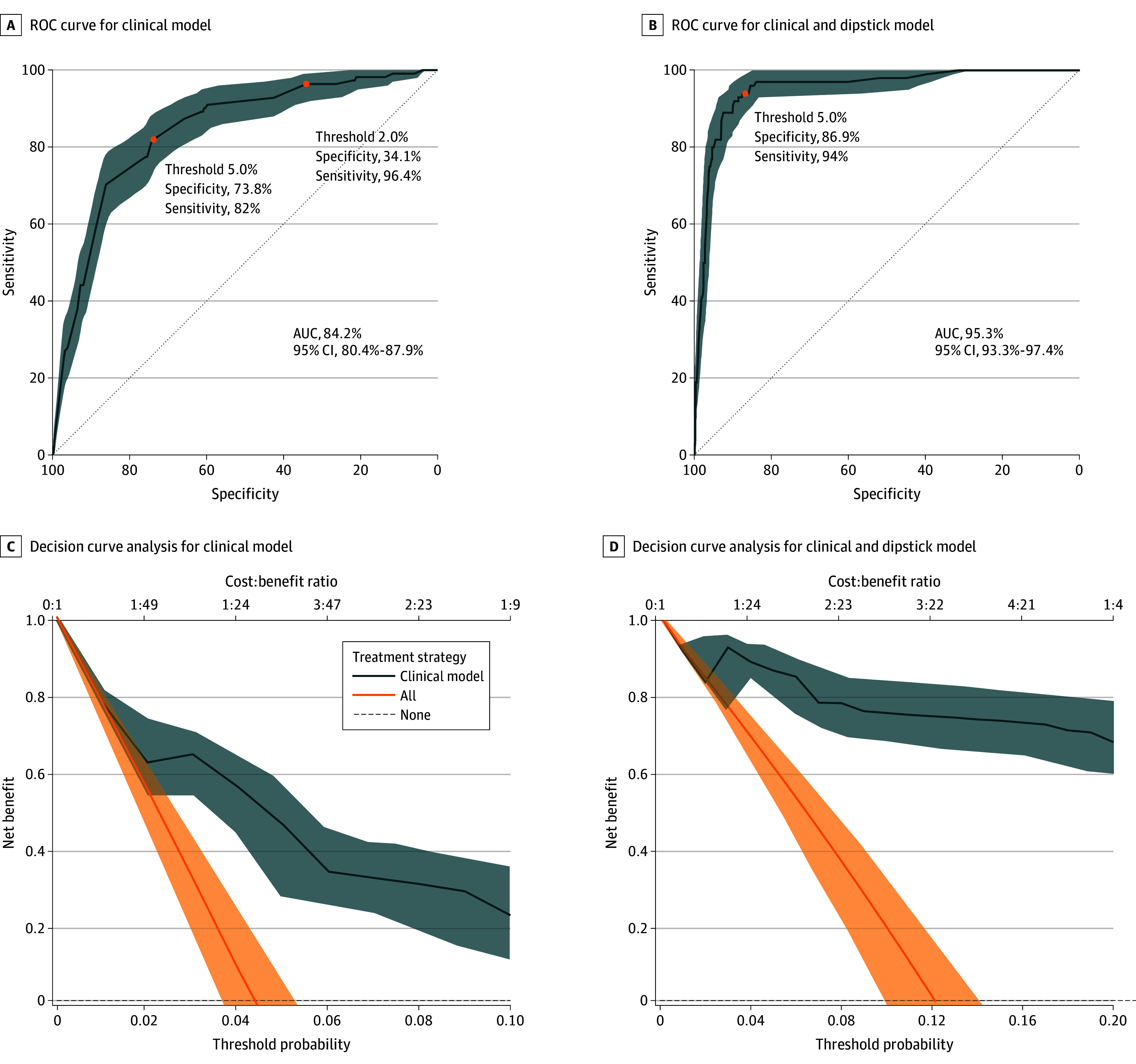 Figure 2
Figure 2| Predictor variable | Participants. No. (%) | ||
|---|---|---|---|
| Overall (N = 2561) | UTI status | ||
| Positive (n = 111) | Negative (n = 2450) | ||
| Clinical characteristics | |||
| Age, mo | |||
| 2 to <12 | 1326 (52) | 71 (64) | 1580 (64) |
| 12 to <24 | 1235 (48) | 40 (36) | 870 (36) |
| Maximum temperature, °C | |||
| <39 | 855 (33) | 32 (29) | 823 (34) |
| ≥39 | 1706 (67) | 79 (71) | 1627 (66) |
| History of UTI | |||
| Yes | 133 (5) | 9 (8) | 124 (5) |
| No | 2428 (95) | 102 (92) | 2326 (95) |
| Sex and circumcision status | |||
| Female | 1212 (47) | 69 (62) | 1143 (47) |
| Uncircumcised male | 866 (34) | 39 (35) | 827 (34) |
| Circumcised male | 479 (19) | 3 (3) | 476 (19) |
| Missing | 4 (<1) | 0 | 4 (<1) |
| Duration of fever, h | |||
| <48 | 1129 (44) | 45 (41) | 1084 (44) |
| ≥48 | 1432 (56) | 66 (59) | 1366 (56) |
| Other fever source | |||
| Yes | 2050 (81) | 27 (24) | 2023 (83) |
| Upper respiratory tract infection | 1025 (50) | 12 (44) | 1013 (50) |
| Lower respiratory tract infection | 246 (12) | 3 (11) | 243 (12) |
| Acute otitis media | 452 (22) | 4 (15) | 448 (22) |
| Gastroenteritis | 108 (5) | 7 (26) | 101 (5) |
| Other | 219 (11) | 1 (4) | 218 (11) |
| None | 511 (19) | 84 (76) | 427 (17) |
| Dipstick results | |||
| No. | 895 | 100 | 795 |
| Nitrite | |||
| Positive | 41 (5) | 33 (33) | 8 (1) |
| Negative | 854 (95) | 77 (77) | 787 (99) |
| Leukocyte esterase | |||
| None | 637 (71) | 3 (3) | 634 (80) |
| Trace | 80 (9) | 8 (8) | 72 (9) |
| 1+ | 81 (9) | 24 (24) | 57 (7) |
| 2+ | 50 (6) | 33 (33) | 17 (2) |
| 3+ | 47 (5) | 32 (32) | 15 (2) |
| Clinical characteristics | Result | |
|---|---|---|
| Dipstick | Urine culture | |
| Uncircumcised male aged 4 mo with 18 h of fever, a maximum recorded temperature of 40.1 °C without a clear source of fever on history or examination | Nitrite negative 3+ Leukocyte esterase | ≥10 × 107 CFU/L ≥10 × 107 CFU/L extended spectrum beta lactamase |
| Uncircumcised male aged 2 mo with 120 h of fever, a maximum recorded temperature of 39.8 °C without a clear source of fever on history or examination | Nitrite negative Trace leukocyte esterase | ≥10 × 107 CFU/L ≥10 × 107 CFU/L |
| Female aged 6 mo with 72 h of fever, a maximum recorded temperature of 39.4 °C without a clear source of fever on history or examination | Nitrite negative 2+ Leukocyte esterase | ≥10 × 107 CFU/L ≥10 × 107 CFU/L |
| Female aged 4 mo with 120 h of fever, a maximum recorded temperature of 40.2 °C without a clear source of fever on history or examination | Nitrite negative 3+ Leukocyte esterase | ≥10 × 107 CFU/L ≥10 × 107 CFU/L |
| Metric | Model, value (95% CI) | ||
|---|---|---|---|
| Clinical (n = 2557) | Clinical and dipstick, 5% risk threshold (n = 895) | ||
| 2% Risk threshold | 5% Risk threshold | ||
| Discrimination | |||
| Sensitivity, % | 96.4 (92.8-99.1) | 82 (74.8-88.3) | 94.0 (89.0-98.0) |
| Specificity, % | 34.1 (32.2-35.9) | 73.8 (72.1-75.5) | 86.9 (84.5-89.1) |
| Positive predictive value | 6.2 (5.9-6.5) | 12.5 (11.3-13.7) | 47.5 (43.1-52.2) |
| Negative predictive value | 99.5 (99.0-99.9) | 98.9 (98.5-99.3) | 99.1 (98.4-99.7) |
| Calibration | |||
| Area under the receiver operating characteristic curve | 84.1 (80.4-87.9) | 95.3 (93.3-97.4) | |
| Calibration in the large | 0.01 | 0.05 | |
| Calibration slope | 0.11 (0.09-0.13) | 0.06 (0.05-0.07) | |
| Observed-to-expected ratio | 0.84 (0.69-0.99) | 0.97 (0.79-1.17) | |
| Brier score | 0.04 (0.03-0.05) | 0.05 (0.04-0.06) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric Urology and Nephrology Studies · Urinary Tract Infections Management · Bladder and Urothelial Cancer Treatments
Introduction
Febrile illness accounts for 14% of children emergency department (ED) visits, with urinary tract infection (UTIs) responsible for as many as 7% of these cases.^1,2,3^ Diagnosing UTIs in preverbal and pre–toilet trained children is particularly challenging due to nonspecific symptoms and difficulty obtaining clean urine samples.^4^ In this population, urethral catheterization can cause patient discomfort and carries a risk of iatrogenic infection,^5,6^ and clean-catch methods are prone to contimination.^7^ Accurate diagnosis is critical; missed UTIs risk potential progression to urosepsis and may have long-term consequences such as kidney scarring,^8,9,10,11,12^ while overuse of antibiotics contributes to antimicrobial resistance.^13^
Over the years, researchers have studied this population to identify risk factors for UTIs, aiming to guide clinicians in risk stratification and inform decisions about testing and treatment.^11^ UTICalc is a clinical prediction tool designed to improve the diagnosis of UTIs in young children by estimating risk based on clinical and laboratory data.^14^ Initially developed using a nested case-control study, UTICalc version 1.0 demonstrated strong diagnostic performance (area under the receiver operating characteristic curve [AUROC], 0.81; 95% CI, 0.72-0.89), which improved further with the inclusion of dipstick results (AUROC, 0.99; 95% CI, 0.98-0.99).^14^ The tool is available via a web-based interface,^15^ where users input patient characteristics to calculate UTI risk.
To address concerns about racial bias in clinical decision-making, UTICalc underwent iterative updates that replaced race as a variable with duration of fever and history of UTI, while preserving its diagnostic performance.^16,17,18^ In 2023, version 3.0 introduced updated risk thresholds to guide testing decisions: testing is recommended for children with a calculated risk of greater than 5%, not recommended for a risk of less than 2%, and shared-decision making is encouraged for risks between 2% and 5%.^14,16^ These changes reflect the tool’s high sensitivity within the 2% to 5% risk threshold range and reinforce commitment to equitable, evidence-based care.
Despite widespread use and thoughtful evolution, UTICalc has only been retrospectively validated.^16,19^ Retrospective validation, while useful for initial assessment, is inherently limited by selection bias and missing data, which can lead to overestimation of a tool’s performance.^20^ Prospective validation is essential to evaluate the accuracy of UTICalc, its generalizability across diverse clinical settings, and its potential impact on clinical outcomes.^21^ This study aimed to provide a prospective external validation of UTICalc version 3.0 in children aged 2 to 24 months presenting to the pediatric ED with fever. The primary objective was to assess the model’s discriminative ability. Secondary objectives included evaluating its calibration and clinical utility.
Methods
Study Design and Settings
We conducted a multicenter prospective diagnostic study between November 2022 and January 2025 in 2 Canadian tertiary care pediatric EDs, both members of the Pediatric Emergency Research Canada (PERC) network^22^: Children’s Hospital of Eastern Ontario (CHEO) (Ottawa, Ontario) and Centre Hospitalier Universitaire Ste Justine (Montreal, Quebec). These are high-volume EDs, each with an annual census exceeding 70 000 visits. The study received approval from the research ethics board at both institutions. The legal guardian of all participants provided written informed consent prior to study enrollment. This study protocol was not registered in a public research repository. This study was reported in accordance Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) and Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD)^23^ reporting guidelines.
Study Population
Children aged 2 to 24 months presenting with fever were eligible for enrollment. Fever was defined as a temperature of 38.0 °C higher, objectively measured in the ED or at home within the previous 24 hours by any method. Exclusion criteria included known congenital kidney or urinary tract abnormalities (including neurogenic bladder), oral or intravenous antibiotic use for any reason at the time of eligibility screening, immunosuppression, insurmountable language barrier, or prior enrollment in the study.
Sample Size
Sample size calculations were based on calibration and precision criteria for external validation of a prediction model with a binary outcome.^24^ Assuming a C-statistic (AUROC) of 0.81, as reported in the original UTICalc derivation, with a standard error of 0.025, and standard errors of 0.10 for both calibration-in-the-large and calibration slope, we estimated the need for 118 UTI events.^14,24^ Given a UTI prevalence of 4.6% at the lead site, this translated to a total required sample size of 2561 participants.
Study Protocol
Trained research staff were in the ED for up to 12 hours per day (9 am to 9 pm, 7 days a week) to screen and enroll eligible children. Research assistants prospectively screened patients for eligibility. For eligible patients, caregivers provided written informed consent for participation and contact information for follow-up. Decisions regarding urinalysis, urine culture, empiric antibiotic treatment, and ED disposition were made at the clinical team’s discretion according to usual care and were not influenced by study participation. Treating clinicians and caregivers were unaware of the final UTI status, which was determined using predefined urinalysis and urine culture criteria. Diagnostic and treatment decisions were made at the discretion of the treating team, including whether to use UTICalc. Customary practice at one ED was not to use UTICalc and varied at the second ED. Case predictions were not explicitly shared with the team.
Data Collection and Outcome Measures
During the index visit, consenting caregivers completed a standardized electronic data collection form, capturing demographic and clinical characteristics for their child, including age, sex, circumcision status, fever duration, and maximum recorded temperature as well as prior history of UTI. The treating team completed a standardized paper data collection form with questions related to fever source. Within 1 week of the ED visit, medical record reviews were conducted to collect laboratory predictor variables and culture results. These were performed by 2 study personnel (N.W.-I. and R.C.), with approximately 5% independently reviewed by each site investigator (C.K. and J.G.) to ensure data quality.
If no urine sample was collected in the ED, email or phone follow-up was completed with caregivers to identify any UTI diagnoses made within 48 hours of the index visit. Questionnaires were sent 3 days after the visit, with 2 reminder messages at 3-day intervals. If there was no response, up to 3 follow-up phone calls were made, each spaced at least 24 hours apart. All study data were securely captured in REDCap, a secure online research program, and housed at CHEO.
Participants were classified as UTI positive if they met both of the following criteria: (1) urinalysis showing either any leukocyte esterase greater than trace on dipstick or greater than 5 white blood cells per high-power field on microscopy and (2) urine culture demonstrating growth of a single uropathogen at 10 × 10^7^ colony-forming units (CFU)/L or greater from a clean-void or clean-catch sample or 5 × 10^7^ CFU/L or greater from a catheter sample. Uropathogens included Escherichia coli, Klebsiella spp, Proteus spp, Enterobacter spp, Enterococcus spp, Citrobacter spp, and Serratia marcescens, consistent with published definitions.^4,25^ During medical record review, any case in which the treating clinician diagnosed a UTI despite not meeting the a priori criteria was flagged and reviewed by study personnel to reach consensus. Additionally, cases were considered UTI positive if a UTI was reported in the follow-up questionnaire. Participants were considered UTI negative if they met any of the following criteria: (1) no missed UTIs reported on the follow-up questionnaire, (2) urinalysis was negative and no urine culture was performed, or (3) a urine culture was performed but it did not meet the study definition for UTI.
UTICalc version 3.0 clinical model includes 5 categorical clinical risk factors (age <12 months, sex and circumcision status, temperature >39 °C, no other fever source, and duration of fever >48 hours). The clinical and dipstick model includes variables from the clinical model plus leukocyte esterase and nitrite values.
Statistical Analysis
Participant characteristics were compared using descriptive statistics (frequency and percentage for categorical variables). Predicted probabilities of UTI were calculated a posteriori by the research team using the UTICalc version 3.0 algorithm, which was provided by the developing team and is based on previously published derivation and validation studies.^14,16^ Model parameters were applied to the clinical and laboratory data collected in our cohort without any recalibration.
Model performance was assessed by constructing a receiver operating characteristic (ROC) curve, illustrating model discrimination (sensitivity and specificity) across the full range of possible thresholds. The AUROC was then computed. Sensitivity, specificity, and positive and negative predictive values were reported using operational UTICalc version 3.0 risk thresholds (2% and 5% for the clinical model and 5% for the clinical and dipstick model).^14,16^ Calibration was evaluated using calibration plots comparing predicted probabilities with observed outcomes and quantified using the calibration slope, which reflects agreement between predicted and observed risks; the observed-to-expected ratio, which compares the number of observed events with the number of expected events by the model and for which a ratio of 1 would indicate perfect agreement; and the Brier score, which measures the mean squared difference between predicted probabilities and observed outcomes. Clinical utility was assessed using decision curve analysis to calculate the net benefit of the models across a range of threshold probabilities (defined as the minimum probability of UTI at which testing or treatment would be warranted) compared with default treat-all or treat-none strategies; a model with higher net benefit at a given threshold was considered clinically useful.^26^ We also compared UTICalc recommendation for urine testing to clinician practice.
Missing predictor variable data were handled by excluding incomplete cases. The potential impact of missing data was assessed by comparing observed characteristics between participants with and without missing information. All statistical analyses were performed using R version 4.4.1 (R Project for Statistical Computing), with a 2-sided significance level of α = .05.
Results
Participant Flow and Characteristics
Among 2561 included participants (1212 [47%] female; 1326 [64%] <12 months) (Figure 1 and Table 1), 111 children (4%) were classified as having UTI. Of these, 105 met the UTI-positive case definition, 2 were reported on follow-up questionnaire, and 4 were adjudicated as UTI-positive cases (Table 2). All adjudicated UTI-positive cases were infants with positive dipstick results and had significant growth of 2 uropathogens. Clinical and laboratory characteristics are summarized in Table 1, overall and by UTI status. Among children with UTI, 71 (64%) were younger than 12 months compared with 40 (36%) aged 12 to younger than 24 months. Female children represented 47% of the overall cohort (1204 of 2561) and 62% of UTI cases (69 of 111). Uncircumcised males represented 34% of the sample (870 children) and 35% of UTI cases (39 children), whereas circumcised males accounted for 19% of participants (487 children) and 3% of UTI cases (3 children).
Participant Flow DiagramUTI indicates urinary tract infection.
Missing Data
In the clinical model, data were missing for 1 predictor variable (sex and circumcision status) in 4 of 2561 participants (<1%). For the clinical and laboratory model, urine dipstick results were available for 898 of 1723 participants (52%) whose predicted UTI risk exceeded 2% based on clinical predictors (and thus would have been included in modeling). As this was an observational cohort, the decision to obtain urine testing was at the discretion of the clinical team. Follow-up survey data to assess for missed UTIs were obtained for 1099 of 1404 participants (78%) who did not undergo urine testing at the index visit, leading to complete data for 2256 participants (88%). The characteristics of survey responders and nonresponders were comparable (eTable in Supplement 1).
Model Performance
Model performance was evaluated at predefined risk thresholds. We evaluated performance at 2% for the clinical model and 5% for both models.
Clinical Model at 2% Threshold
At the 2% threshold, the clinical model demonstrated high sensitivity (96.4%; 95% CI, 92.8%-99.1%) but low specificity (34.1%; 95% CI, 32.2%-35.9%). The positive predictive value (PPV) was 6.2%, and the negative predictive value (NPV) was 99.5%.
Clinical Model at 5% Threshold
At the 5% threshold, the clinical model showed improved specificity (73.8%; 95% CI, 72.1%-75.5%) with reduced sensitivity (82.0%; 95% CI, 74.8%-88.3%). The PPV was 12.5%, and the NPV was 98.9%.
Clinical and Dipstick Model at 5% Threshold
The clinical and dipstick model demonstrated high sensitivity (94.0%; 95% CI, 89.0%-98.0%) and specificity (86.9%; 95% CI, 84.5%-89.2%) at the 5% threshold. The PPV was 47.5%, and the NPV was 99.1%.
Discrimination and Calibration
Discrimination was strong for both models, with AUROC values of 0.84 (95% CI, 0.80-0.88) for the clinical model and 0.95 (95% CI, 0.93-0.97) for the clinical and dipstick model. Brier scores were low for both models, reflecting good overall predictive accuracy. Calibration-in-the-large was close to 0, and both models had calibration slopes less than 1, suggesting some overfitting. The observed-to-expected event ratio indicated underprediction with the clinical model and good calibration with the clinical and dipstick model. Full performance metrics are presented in Table 3, with ROC curves shown in Figure 2.
Receiver Operating Characteristic (ROC) Curves and Decision Curve Analyses for Clinical and Clinical and Dipstick UTICalc ModelsA higher net benefit indicates greater clinical utility. AUC indicates area under the curve.
Clinical Utility
Decision Curve Analysis
Decision curve analysis demonstrated clinical utility across a range of threshold probabilities. As shown in Figure 2, the clinical model was associated with a higher net benefit than either the treat-all or treat-none strategies across threshold probabilities ranging from 0.01 to 0.08, with the greatest clinical advantage observed between 0.02 and 0.06. Similarly, the clinical and dipstick model was associated with superior net benefit over the same comparators from threshold probabilities of 0.01 to 0.18, with particularly robust benefit in the 0.04 to 0.12 range. These results suggest that both models could aid clinical decision-making by identifying patients more likely to benefit from intervention, with the clinical and dipstick model demonstrating an extended range of utility.
Comparison of UTICalc Urine Testing Recommendations vs Clinician Judgement
In our sample, clinicians obtained urine testing for 1157 children, missing 2 cases of UTI. This yielded a sensitivity of 98.2% (95% CI, 93.7%-99.5%) and a specificity of 57.3% (95% CI, 55.4%-59.3%). When compared with UTICalc recommendations at a 2% risk threshold, the model would recommend urine testing in 1719 cases, missing 4 UTIs but increasing the number of urine tests by 565. At a 5% risk threshold, UTICalc would have recommended testing in only 731 cases, missing 20 UTIs. This represents a substantial reduction in testing volume, albeit with a trade-off in sensitivity.
Discussion
This multicenter diagnostic study prospectively provides the final stage of external validation for UTICalc in young febrile children. We found strong discrimination for the model, which was improved when incorporating dipstick data. This study supports integration into clinical care as a tool for diagnostic stewardship in pediatric care.
Decision curve analysis supported the utility of both UTICalc models across relevant thresholds. However, clinician judgment demonstrated higher sensitivity in the high-volume tertiary centers where this study was conducted, reflecting pediatric emergency medicine practitioner expertise. Because most children presenting for acute care are evaluated outside tertiary centers,^27^ possibly with limited pediatric expertise and uncertain follow-up, using a 5% risk threshold—despite reducing testing—may not be ideal due to reduced sensitivity. UTICalc may serve as a useful adjunct for clinicians with less pediatric experience or in cases of diagnostic uncertainty, with lower risk thresholds (eg, 2%) potentially more appropriate for patients with persistent symptoms or anticipated barriers to follow-up.
The observed UTI prevalence of 4% in our cohort is consistent with previously reported risk estimates in this population, which ranges from 3% to 11%.^2,28,29^ Model performance in our study was comparable with the original derivation and validation study published in 2018, which reported an AUROC of 0.80 in the clinical model and 0.97 in the clinical and dipstick model. Low PPV in our sample is reflective of low disease prevalence.
Since the internal validation of UTICalc,^14^ 2 external validation studies^16,30^ have been conducted with important limitations. In 2021, Boon et al^30^ evaluated UTICalc in a small subgroup (n = 96) with only 4 positive UTI cases and resultant large confidence intervals in their conclusions, limiting interpretation. More recently, Smith et al^16^ conducted a retrospective case-control study comparing UTICalc version 1.0 with the current version 3.0 (excluding race as a predictor). While they demonstrated reasonable discrimination (AUROC, 73.8; 95% CI, 68.7-78.8), this study was limited by the retrospective design and inclusion of only those children who had both a urinalysis and urine culture performed, potentially introducing significant selection and verification bias. Given that UTICalc is designed to identify which undifferentiated, febrile child warrants urine testing (and potentially empiric treatment), prospective validation in this population is essential. Our study provides clinical evidence of its performance in the population for which it was designed.
Strengths of this study include its prospective design, large sample size, and follow-up to identify missed cases. Inclusion of 2 distinct settings, one where UTICalc is rarely used, enhances the generalizability of findings. The model’s performance was rigorously evaluated using TRIPOD-recommended metrics.^23^
Limitations
This study had several limitations. Maximum recorded temperature, duration of fever, and prior history of UTI were obtained from caregivers; however, any minor discrepancies between caregiver report and clinician documentation are unlikely to meaningfully affect results, as these elements are routinely obtained during clinical history taking. Missing urinalysis data, while reflective of the realities of clinical decision-making, may have introduced verification bias. We mitigated this by implementing a follow-up strategy to identify missed UTI diagnoses; however, follow-up data were not available for a small proportion of participants. UTIs may have been missed if patients were treated for other apparent infections (eg, acute otitis media). We were also unable to validate the Gram stain model, as neither participating site reported Gram stain results. Validation of the hemocytometer method was limited due to inconsistencies in white blood cell unit conversions. Furthermore, interrater reliability and clinical acceptability of the tool were not assessed in this study, which may affect its practical utility in clinical settings.
Conclusions
In this multicenter prospective cohort study of 2561 febrile children aged 2 to 24 months presenting to the ED, UTICalc demonstrated strong discrimination, calibration, and clinical utility. Although UTICalc did not outperform clinician performance at the high-volume tertiary pediatric centers in which the study was conducted, the prospective design of the study allows for generalizability of its discrimination, overall accuracy, and net benefit. These findings support the use of UTICalc to guide UTI evaluation and management in young children. Future research should assess UTICalc performance across varying levels of clinician pretest suspicion and evaluate earlier integration into ED workflows, potentially using only historical and clinical features, to support earlier risk stratification and streamline urine collection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sands R, Shanmugavadivel D, Stephenson T, Wood D. Medical problems presenting to paediatric emergency departments: 10 years on. Emerg Med J. 2012;29(5):379-382. doi:10.1136/emj.2010.10622921609944 · doi ↗ · pubmed ↗
- 2Shaikh N, Morone NE, Bost JE, Farrell MH. Prevalence of urinary tract infection in childhood: a meta-analysis. Pediatr Infect Dis J. 2008;27(4):302-308. doi:10.1097/INF.0b 013e 31815 e 412218316994 · doi ↗ · pubmed ↗
- 3Cioffredi LA, Jhaveri R. Evaluation and management of febrile children: a review. JAMA Pediatr. 2016;170(8):794-800. doi:10.1001/jamapediatrics.2016.059627322346 · doi ↗ · pubmed ↗
- 4Mattoo TK, Shaikh N, Nelson CP. Contemporary management of urinary tract infection in children. Pediatrics. 2021;147(2):e 2020012138. doi:10.1542/peds.2020-01213833479164 · doi ↗ · pubmed ↗
- 5O’Brien K, Stanton N, Edwards A, Hood K, Butler CC. Prevalence of urinary tract infection (UTI) in sequential acutely unwell children presenting in primary care: exploratory study. Scand J Prim Health Care. 2011;29(1):19-22. doi:10.3109/02813432.2011.55426821323495 PMC 3347928 · doi ↗ · pubmed ↗
- 6Ouellet-Pelletier J, Guimont C, Gauthier M, Gravel J. Adverse events following diagnostic urethral catheterization in the pediatric emergency department. CJEM. 2016;18(6):437-442. doi:10.1017/cem.2016.527780500 · doi ↗ · pubmed ↗
- 7Labrosse M, Levy A, Autmizguine J, Gravel J. Evaluation of a new strategy for clean-catch urine in infants. Pediatrics. 2016;138(3):e 20160573. doi:10.1542/peds.2016-057327542848 · doi ↗ · pubmed ↗
- 8Karavanaki KA, Soldatou A, Koufadaki AM, Tsentidis C, Haliotis FA, Stefanidis CJ. Delayed treatment of the first febrile urinary tract infection in early childhood increased the risk of renal scarring. Acta Paediatr. 2017;106(1):149-154. doi:10.1111/apa.1363627748543 · doi ↗ · pubmed ↗