Set-up and use of the “Asclepius tube”: a slim drainage tube to facilitate saline-immersion endoscopic submucosal dissection
Elisabet Maristany Bosch, Georgios Kalopitas, Elisabetta Dell’Unto, Yoshikazu Hayashi, Hironori Yamamoto, Alberto Murino, Edward J. Despott

TL;DR
A new drainage tube called the 'Asclepius tube' improves saline-immersion endoscopic submucosal dissection by maintaining fluid balance and enhancing patient comfort.
Contribution
The Asclepius tube is introduced as a low-cost, practical solution to optimize saline-immersion endoscopic submucosal dissection.
Findings
The Asclepius tube successfully maintained fluid balance during a 170-minute ESD procedure.
The procedure achieved an en bloc resection with an R0 histopathological result.
The device enhances patient comfort and allows use of conscious sedation without affecting scope maneuverability.
Abstract
Endoscopic submucosal dissection (ESD) is recognized as the reference standard for en bloc resection of large colorectal and gastric lesions, but conventional carbon dioxide–insufflation ESD presents challenges. The saline-immersion/irrigation technique (SITE) offers multiple advantages, especially when combined with a drainage tube. The video showcases the set-up and practical use of the “Asclepius tube” to optimize SITE-ESD, maintaining its advantages, allowing for a more efficient dissection, keeping an adequate balance of fluid and improving patient comfort. A 72-year-old man with a 60-mm sessile lesion (Paris 0-Is) at the rectosigmoid junction was referred for ESD. SITE-ESD was performed using the pocket-creation method with the patient under conscious sedation. The Asclepius tube was wrapped around the scope and connected to continuous low-flow suction (<20 kPa) to drain…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
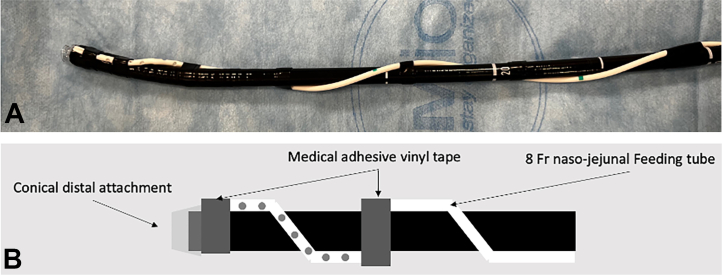 Figure 1
Figure 1 Figure 2
Figure 2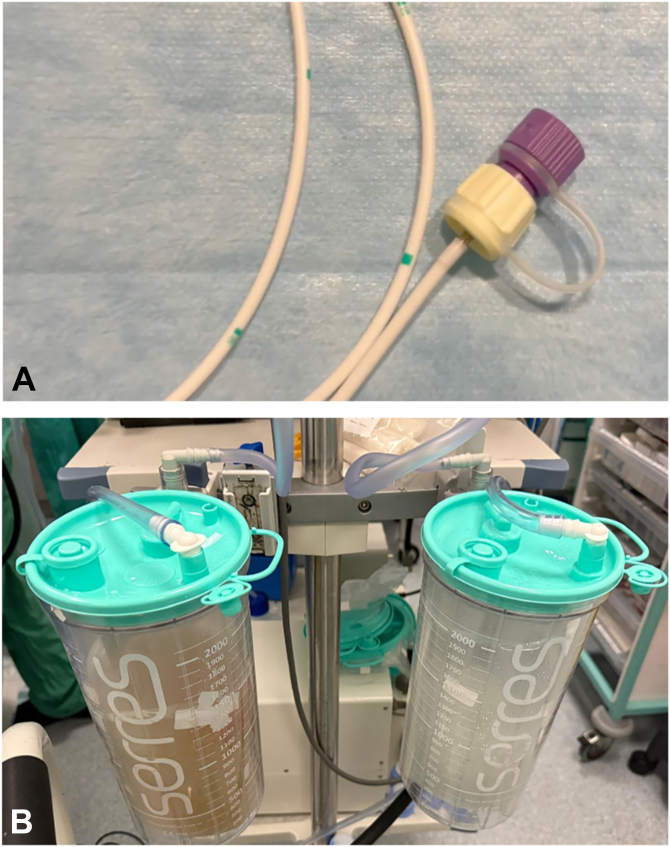 Figure 3
Figure 3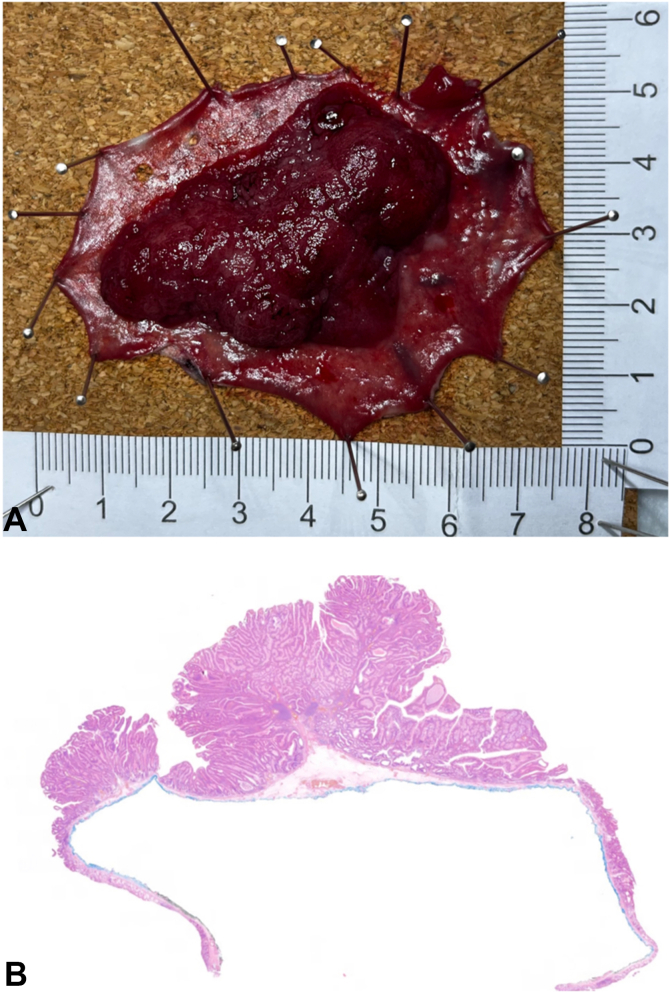 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Esophageal Cancer Research and Treatment · Gastrointestinal Tumor Research and Treatment
Introduction
Endoscopic submucosal dissection (ESD) increasingly is recognized as the reference standard for en bloc resection of colorectal and gastric lesions.1 In conventional ESD, carbon dioxide insufflation typically is used. However, the introduction of the saline-immersion/irrigation technique (SITE) in 20172 addresses both the drawbacks of gaseous insufflation and previously described underwater ESD techniques with the use of deionized water.3 SITE replaces carbon dioxide and water with isotonic saline solution, allowing enhanced optical clarity and magnification; minimization of any gas/liquid interface and lens-soiling with fat; buoyancy of the submucosal flap; improved conductivity through the electrolytes in saline, facilitating vessel precoagulation, and effectively managing intraprocedural bleeding. Our preliminary experience suggests that SITE also enhances patient comfort, because saline, particularly when combined with external drainage, causes less distension than gas.
Multiple types of drainage tubes have been described, such as the Foley catheter or transanal tube through gravity-assisted outflow or connected to low-pressure suction, to facilitate distal colonic ESD.4^,^5 We have also described the use of a slim fenestrated feeding tube wrapped around the scope and secured with vinyl tape to facilitate ESD in the right-sided colon6 when using SITE and maintain its advantages. This tube, which we named the “Asclepius tube,” given its similarity to the medical symbol of the snake around the rod of Asclepius7 (Figs. 1 and 2), has the objective to drain redundant fluid from the continuous saline-irrigation during ESD and gas generated by diathermy, obviating the need for endoscopic aspiration through the scope. This allows for a more efficient dissection, keeping an adequate balance of fluid inside the lumen, avoiding overdistension of the bowel, maintaining patient comfort, as well as providing better access to the submucosal layer. A retrospective study by Kagaya et al8 comparing rectal ESD with or without the Foley catheter showed that the presence of drainage notably improved efficiency of rectal ESD performed by novice endoscopists by increasing dissection speed.Figure 1. Photograph (A) and graphical representation (B) show the setting of an 8F nasojejunal fenestrated feeding tube wrapped around the distal part of the endoscope and secured with generic medical adhesive vinyl tape. A conical distal attachment has been previously placed and secured with the same adhesive vinyl tape at the tip of the scope to avoid movement during the procedure.Figure 2. Graphic symbol of “the rod of Asclepius” (A), and photograph (B) of the maintained flexibility of the scope with the Asclepius tube wrapped around.
In our clinical practice, we monitor the saline balance (in vs out) because we find that the optimal working volume of saline to maintain patient comfort and optimize maneuverability for effective and efficient dissection is about 500 mL. We present a video to showcase the straightforward set-up of the Asclepius tube and practical application with ESD of a large rectal lesion performed by 2 novice endoscopists. The case presents a 72-year-old man with a 60-mm sessile (Paris 0-Is, focal Japan Narrow-Band Imaging Expert Team type 2B lesion in the rectosigmoid junction referred for ESD with the patient under operator-delivered conscious sedation (Video 1, available online at www.videogie.org). A slim 7.9-mm gastroscope with a 3.2-mm working channel (EG-840 TP; Fujifilm Healthcare, Tokyo, Japan) was used to achieve maximum maneuverability within the rectosigmoid junction. SITE combined with the bridge-formation variation9^,^10 of the pocket-creation method11, 12, 13 was used for resection. The scope was equipped with a conical-short, transparent hood (ST Hood DH-083ST; Fujifilm, Tokyo, Japan) to facilitate ESD using the pocket-creation method, and the Asclepius tube (8F nasojejunal tube; Cook Medical Europe, Ltd, Limerick, Ireland) was wrapped around the scope and attached to continuous low-flow suction (<20 kPa) (Fig. 3), initiated at the start of the procedure once the lumen is filled with saline.Figure 3. The end tip of the Asclepius tube is connected to the suction attachment (A) and attached to continuous low-flow suction (<20 kPa) to drain redundant saline and gas (B).
A 1.5-mm ball-tipped needle-type knife (FlushKnife BTs 1.5 mm; Fujifilm) was used. Any vessels or mild episodes of bleeding were managed with knife-tip coagulation using swiftCOAG effect 2.5 (VIO 3; Erbe Elektromedizin, Tübingen, Germany) combined with continuous saline irrigation for optimal coagulation effect, causing gradual whitening of the vessel.
The procedure was completed in 170 minutes (dissection speed of 20.1 mm^2^/min) by 2 fellows training in ESD, without significant intraprocedural adverse events, and the patient was discharged on the same day. Histopathology confirmed R0, curative resection of a low-grade dysplastic tubulovillous adenoma (Fig. 4).Figure 4. The specimen was removed en bloc (A), and histopathology (B) confirmed complete R0, curative resection of a low-grade dysplastic tubulovillous adenoma.
We have started using this tube for all our colorectal SITE-ESDs because it is low-cost and easy to set up and helps maintain an adequate fluid balance during the procedure, enhancing patient comfort, and its use does not appear to affect scope maneuverability or any other hindrance through friction. Further prospective comparative studies are warranted to validate our findings.
Patient Consent
The patient in this article has given written informed consent to publication of their case details.
Disclosure
The following authors disclosed financial relationships: H. Yamamoto: Consultant and support (honoraria, grants, and royalties): Fujifilm Corporation. A. Murino: Speaker honoraria: Olympus Medical, Laborie, Boston Scientific, and Fujifilm Healthcare Europe. E. J. Despott: Educational grants in support of conference organization, and honoraria, from Fujifilm Healthcare Europe, Pentax, and Olympus Medical; and honoraria: Ambu and Fujifilm Healthcare Europe. All other authors disclosed no financial relationships.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Libânio D.Pimentel-Nunes P.Bastiaansen B.Endoscopic submucosal dissection techniques and technology: European Society of Gastrointestinal Endoscopy (ESGE) technical review Endoscopy 5520233613893688209010.1055/a-2031-0874 · doi ↗ · pubmed ↗
- 2Despott E.J.Murino A.Saline-immersion therapeutic endoscopy (SITE): an evolution of underwater endoscopic lesion resection Dig Liver Dis 49201713762896763210.1016/j.dld.2017.08.035 · doi ↗ · pubmed ↗
- 3Yoshii S.Hayashi Y.Matsui T.“Underwater” endoscopic submucosal dissection: a novel technique for complete resection of a rectal neuroendocrine tumor Endoscopy 48 Suppl 1 UCTN 2016 E 67E 682689054710.1055/s-0042-101855 · doi ↗ · pubmed ↗
- 4Morikawa T.Hayashi Y.Fukuda H.Trans-anal tube facilitates endoscopic submucosal dissection of a >10 cm rectal laterally spreading tumor Dig Endosc 352023 e 107e 1083730326010.1111/den.14603 · doi ↗ · pubmed ↗
- 5Kagaya Y.Hayashi Y.Morikawa T.Trans-anal Foley catheter facilitates endoscopic submucosal dissection of a distal rectal tumor Dig Endosc 352023 e 155e 1573777945310.1111/den.14680 · doi ↗ · pubmed ↗
- 6Morikawa T.Murino A.Ishii H.The ”Asclepius tube”: a slim drainage tube wrapped around the distal part of the endoscope, for cecal endoscopic submucosal dissection Video GIE 1020241551594001289510.1016/j.vgie.2024.10.002PMC 11853374 · doi ↗ · pubmed ↗
- 7Muhtaseb M.Muhtaseb A.Caduceus and Asclepius: a tale of two rods Eye (Lond)362022222622273541465510.1038/s 41433-022-02054-x PMC 9582002 · doi ↗ · pubmed ↗
- 8Kagaya Y.Ishii H.Hayashi Y.Retrospective study comparing rectal endoscopic submucosal dissection with and without Foley catheter drainage tube placement Endosc Int Open 132025 a 263176944061184110.1055/a-2631-7694 PMC 12223953 · doi ↗ · pubmed ↗