Gynecologic conditions in the context of incarceration: A scoping review
Meredith K. Wise, Sahana Raghunathan, Sreya Upputuri, Elana Jaffe Brotkin, Tre D. Thorne, Jamie Conklin, Andrea K. Knittel

TL;DR
This review explores gynecologic health issues faced by incarcerated individuals, highlighting the prevalence of conditions and challenges in accessing care.
Contribution
The study provides a comprehensive global overview of gynecologic conditions in carceral settings and identifies gaps in addressing these health disparities.
Findings
Gynecologic conditions are common in incarcerated populations and worsened by stress, trauma, and poor access to care.
There is limited research on health education and interventions for gynecologic health disparities in carceral settings.
The review highlights the need for policy changes to improve gynecologic care and reduce stigma in prisons.
Abstract
More than 740 000 people identified as female at intake were incarcerated globally as of 2022, reflecting a 60% global increase since the year 2000, with a concomitant increase in gynecologic conditions experienced behind bars. The purpose of this scoping review was to examine the breadth of benign and malignant gynecologic conditions experienced during incarceration, including the prevalence, special management considerations, access to services, and the patient experience. The search strategy included a combination of keywords and subject headings for incarceration and benign or malignant gynecologic conditions with no language or date limits. Studies were eligible for the review if they: (i) discussed a benign or malignant gynecologic condition; (ii) included a population of people experiencing incarceration; and (iii) answered one or more of the four key questions identified prior…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
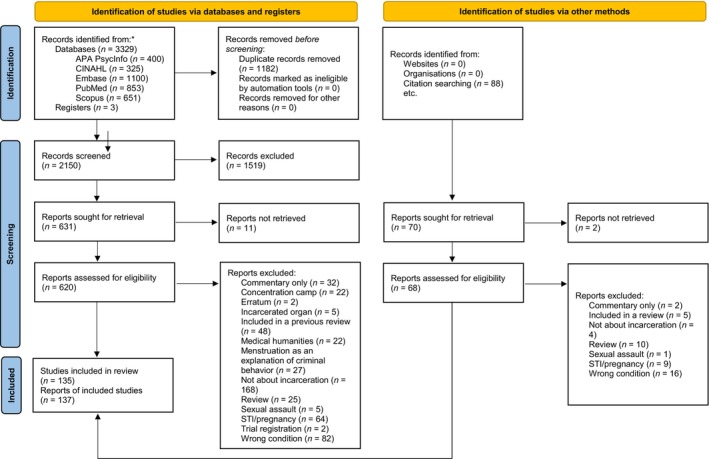 FIGURE 1
FIGURE 1| Set # | |
|---|---|
| 1 | “Correctional Facilities”[Mesh] OR “Prisoners”[Mesh] OR “Criminals”[Mesh] OR “Juvenile Delinquency”[Mesh] OR “mass incarceration”[tw] OR “incarcerated women”[tw] OR “incarcerated people”[tw] OR “incarcerated persons”[tw] OR “women incarcerated”[tw] OR “incarcerated youths”[tw] OR “incarcerated adolescent”[tw] OR “incarcerated adolescents”[tw] OR “adolescents incarcerated”[tw] OR “incarcerated girl”[tw] OR “incarcerated girls”[tw] OR “incarcerated patient”[tw] OR “incarcerated patients”[tw] OR “incarcerated individuals”[tw] OR “incarcerated populations”[tw] OR “incarcerated population”[tw] OR “incarcerated adults”[tw] OR “incarcerated adults”[tw] OR “incarcerated female”[tw] OR “incarcerated females”[tw] OR carceral[tw] OR “correctional facility”[tw] OR “correctional facilities”[tw] OR “correctional institution”[tw] OR “correctional institutions”[tw] OR “correctional center”[tw] OR “correctional centers”[tw] OR “correctional centre”[tw] OR “correctional centres”[tw] OR “correction facility”[tw] OR “correction facilities”[tw] OR “correction institution”[tw] OR “correction institutions”[tw] OR “correction center”[tw] OR “correction centers”[tw] OR “correction centre”[tw] OR “correction centres”[tw] “correctional health”[tw] OR “correctional healthcare”[tw] OR “correctional care”[tw] OR prisoner[tw] OR prisoners[tw] OR prison[tw] OR prisons[tw] OR imprisoned[tw] OR jail[tw] OR jails[tw] OR jailed[tw] OR inmate[tw] OR inmates[tw] OR criminal[tw] OR criminals[tw] OR felon[tw] OR felons[tw] OR offender[tw] OR offenders[tw] OR convict[tw] OR convicts[tw] OR “penal institution”[tw] OR “penal institutions”[tw] OR “penal facility”[tw] OR “penal facilities”[tw] OR penitentiary[tw] OR penitentiaries[tw] OR “justice involved”[tw] OR justice‐involved[tw] OR “detention centers”[tw] OR “detention center”[tw] OR “detention centres”[tw] OR “detention centre”[tw] OR “detention facility”[tw] OR “detention facilities”[tw] OR “juvenile detention”[tw] OR “youth detention”[tw] OR “juvenile delinquency”[tw] OR “juvenile justice”[tw] |
| 2 | “Gynecology”[Mesh] OR “Gynecological Examination”[Mesh] OR “Lower Urinary Tract Symptoms”[Mesh] OR “Papanicolaou Test”[Mesh] OR “Genital Diseases, Female”[Mesh] OR gynecology[tw] OR gynecology[tw] OR gynecologic[tw] OR gynaecologic[tw] OR gynecological[tw] OR gynecological[tw] OR gynecologist[tw] OR gynecologist[tw] OR gynecologists[tw] OR gynecologists[tw] OR urogynecologic[tw] OR urogynaecologic[tw] OR urogynecological[tw] OR urogynaecological[tw] OR urogynecology[tw] OR urogynaecology[tw] OR OBGYN[tw] OR OB‐GYN[tw] OR “female genital disease”[tw] OR “female genital diseases”[tw] OR “adnexal disease”[tw] OR “adnexal diseases”[tw] OR “adnexa disease”[tw] OR “adnexa diseases”[tw] OR “vaginal disease”[tw] OR “vaginal diseases”[tw] OR “vulvar disease”[tw] OR “vulvar diseases”[tw] OR “vulvovaginal disease”[tw] OR “vulvovaginal diseases”[tw] OR “vulvar diseases”[tw] OR “ovarian disease”[tw] OR “ovarian diseases”[tw] OR “ovarian cysts”[tw] OR “ovarian cyst”[tw] OR “Polycystic Ovary Syndrome”[tw] OR “uterine disease”[tw] OR “uterine diseases”[tw] OR “endometrial disease”[tw] OR “endometrial diseases”[tw] OR “cervical disease”[tw] OR “cervical diseases”[tw] OR vaginitis[tw] OR vulvovaginitis[tw] OR vulvitis[tw] OR vaginosis[tw] OR yeast[tw] OR candida[tw] OR Candidiasis[tw] OR “vaginal discharge”[tw] OR “vaginal discharges”[tw] OR “vaginal examination”[tw] OR “vaginal examinations”[tw] OR “vaginal exam”[tw] OR “vaginal exams”[tw] OR “pelvic examination”[tw] OR “pelvic examinations”[tw] OR “pelvic exam”[tw] OR “pelvic exams”[tw] OR Papanicolaou[tw] OR “pap test”[tw] OR “pap tests”[tw] OR “pap smear”[tw] OR “pap smears”[tw] OR “pap stain”[tw] OR “pap stains”[tw] OR “cervical smear”[tw] OR “cervical smears”[tw] OR “lower urinary tract symptoms”[tw] |
| 3 | “Uterine Hemorrhage”[Mesh] OR “uterine hemorrhage”[tw] OR “uterine hemorrhages”[tw] OR “uterine hemorrhaging”[tw] OR “uterus hemorrhage”[tw] OR “uterus hemorrhages”[tw] OR “uterus hemorrhaging”[tw] OR “uterine hemorrhage”[tw] OR “uterine hemorrhages”[tw] OR “uterine hemorrhaging”[tw] OR “uterus hemorrhage”[tw] OR “uterus hemorrhages”[tw] OR “uterus hemorrhaging”[tw] OR “uterine bleeding”[tw] OR “uterus bleeding”[tw] OR “vaginal hemorrhage”[tw] OR “vaginal hemorrhages”[tw] OR “vaginal hemorrhaging”[tw] OR “vaginal hemorrhage”[tw] OR “vaginal hemorrhages”[tw] OR “vaginal hemorrhaging”[tw] OR “vaginal bleeding”[tw] OR “vagina hemorrhage”[tw] OR “vagina hemorrhages”[tw] OR “vagina hemorrhaging”[tw] OR “vagina hemorrhage”[tw] OR “vagina hemorrhages”[tw] OR “vagina hemorrhaging”[tw] OR “vagina bleeding”[tw] OR “abnormal bleeding”[tw] OR “irregular bleeding”[tw] OR “abnormal menstrual bleeding”[tw] OR “abnormal menses”[tw] OR “Intermenstrual Bleeding”[tw] OR “Dysfunctional Uterine Bleeding”[tw] OR “Breakthrough Bleeding”[tw] OR “Bleeding Between Periods”[tw] OR “bleeding between menses”[tw] OR “heavy menstrual bleeding”[tw] OR “heavy menstruation”[tw] OR “heavy period”[tw] OR “heavy periods”[tw] OR “heavy menses”[tw] OR hypermenorrhea[tw] OR hypermenorrhoea[tw] OR menorrhagia[tw] OR metrorrhagia[tw] OR menometrorrhagia[tw] OR “irregular menstrual bleeding”[tw] OR “irregular menses”[tw] |
| 4 | “Menopause”[Mesh] OR menopaus*[tw] OR premenopaus*[tw] OR postmenopaus*[tw] OR perimenopause*[tw] OR “hot flashes”[tw] OR “hot flushes”[tw] |
| 5 | “Pelvic Pain”[Mesh] OR dysmenorrhea[tw] OR dysmenorrheas[tw] OR “piriformis muscle syndrome”[tw] OR “piriformis syndrome”[tw] OR endometriosis[tw] OR endometrioses[tw] OR ((“Pain”[Mesh] OR “Pain Management”[Mesh] OR pain*[tw]) AND (“Pelvis”[Mesh] OR pelvis[tw] OR pelvic[tw])) |
| 6 | “Genital Neoplasms, Female”[Mesh] OR “Squamous Intraepithelial Lesions of the Cervix”[tw] OR ((“Genitalia, Female”[Mesh] OR “female genital”[tw] OR “female genitals”[tw] OR “female genitalia”[tw] OR “female reproductive”[tw] OR Gynecologic[tw] OR cervical[tw] OR cervix[tw] OR endometrium[tw] OR endometria[tw] OR endometrial[tw] OR ovary[tw] OR ovaries[tw] OR ovarian[tw] OR uterus[tw] OR uteri[tw] OR womb[tw] OR wombs[tw] OR uterine[tw] OR vagina[tw] OR vaginas[tw] OR vaginal[tw] OR vulva[tw] OR vulvas[tw] OR vulvar[tw] OR “fallopian tube”[tw] OR “fallopian tubes”[tw]) AND (“Neoplasms”[Mesh] OR neoplasm[tw] OR neoplasms[tw] OR neoplasia[tw] OR cancer[tw] OR cancers[tw] OR cancerous[tw] OR carcinoma[tw] OR carcinomas[tw] OR malignant[tw] OR malignancy[tw] OR malignancies[tw] OR metastasis[tw] OR metastases[tw] OR metastatic[tw] OR tumor[tw] OR tumors[tw] OR tumor[tw] OR tumors[tw] OR sarcoma[tw] OR sarcomas[tw] OR oncology[tw] OR oncologist[tw] OR oncologists[tw] OR oncologica[tw])) |
| 7 | (“Pelvic Organ Prolapse”[Mesh] OR ((“Prolapse”[Mesh] OR prolapse[tw] OR prolapses[tw]) AND (“Pelvis”[Mesh] OR “Vagina”[Mesh] OR “Uterus”[Mesh] OR pelvis[tw] OR pelvic[tw] OR uterine[tw] OR visceral[tw] OR rectal[tw] OR vaginal[tw] OR vaginal[tw] OR urogenital[tw] OR genital[tw] OR urinary[tw] OR genitourinary[tw]))) |
| 8 | (“Urinary Incontinence”[Mesh] OR “Nocturia”[Mesh] OR “Urinary Bladder, Overactive”[Mesh] OR “nocturnal diuresis”[tw] OR nocturia[tw] OR ((“Urination”[Mesh] OR “Urine”[Mesh] OR urinary[tw] OR urination[tw] OR micturition[tw] OR bladder[tw] OR urine[tw]) AND (incontinence[tw] OR incontinent[tw] OR urgency[tw] OR urge[tw] OR frequency[tw] OR leakage[tw] OR overactive[tw] OR overactivity[tw]))) |
| 9 | (“Uterine Cervical Dysplasia”[Mesh] OR “Papillomavirus Infections”[Mesh] OR “Papillomaviridae”[Mesh] OR “abnormal pap”[tw] OR “abnormal paps”[tw] OR HPV[tw] OR “Human Papilloma Virus”[tw] OR “Human Papilloma Viruses”[tw] OR “Human Papillomavirus”[tw] OR “Papillomavirus Infection”[tw] OR “Papillomavirus Infections”[tw] OR “papillomaviral infection”[tw] OR “papillomaviral infections”[tw] OR ((Cervical[tw] OR cervix[tw] OR vaginal[tw] OR vagina[tw] OR vulvar[tw] OR vulva[tw] OR uterine[tw]) AND (dysplasia[tw] OR dysplasias[tw]))) |
| 10 | (“Menstrual Cycle”[Mesh] OR “Menstruation”[Mesh] OR “Menstruation Disturbances”[Mesh] OR “Menarche”[Mesh] OR menstrual[tw] OR menstruation[tw] OR menstruating[tw] OR menarche[tw] OR menses[tw] OR premenstrual[tw] OR amenorrhea[tw]) |
| 11 | #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 |
| 12 | #1 AND #11 |
| Reference and year | Country | Setting | Prevalence | Special considerations for management | Access | Experiences |
|---|---|---|---|---|---|---|
| Centro pela Justiça e pelo Direito Internacional, 2007 | Brazil | Prison | ✓ | |||
| De Araújo et al., 2020 | Brazil | Prison | ✓ | ✓ | ||
| Fink et al., 1998 | USA | Jail | ✓ | |||
| Friedman et al., 2021 | USA | Jail | ✓ | |||
| Gallagher et al., 2007 | USA | Other detention facility | ✓ | |||
| Gender, Health & Justice Research Unit, 2012 | South Africa | Prison | ✓ | ✓ | ||
| Grady, 1999 | USA | Prison | ✓ | ✓ | ✓ | |
| Harner and Burgess, 2011 | USA | Prison | ✓ | ✓ | ||
| Hatton et al., 2006 | USA | Jail | ✓ | ✓ | ||
| Holland‐Hall et al., 2002 | USA | Other detention facility | ✓ | ✓ | ✓ | |
| Hyde et al., 2022 | USA | Other detention facility | ✓ | |||
| Ingram‐Fogel, 1991 | USA | Prison | ✓ | ✓ | ||
| Kraft‐Stolar, 2015 | USA | Prison | ✓ | ✓ | ✓ | |
| Leitie Araújo, 2019 | Brazil | Other detention facility | ✓ | |||
| Lowery et al., 2019 | USA | Prison | ✓ | |||
| Miranda et al., 2004 | Brazil | Prison | ✓ | |||
| Nicolau et al., 2012 | Brazil | Prison | ✓ | ✓ | ||
| Nicolau et al., 2015 | Brazil | Prison | ✓ | ✓ | ||
| Sabbagh Steinberg, 2018 | USA | Prison | ✓ | ✓ | ✓ | |
| Sarpong et al., 2015 | Ghana | Prison | ✓ | ✓ | ||
| Tang et al., 2010 | UK | Prison | ✓ | |||
| Woodall et al., 2021 | UK | Prison | ✓ | |||
| Young and Reviere, 2001 | USA | Prison | ✓ |
| Reference and year | Country | Setting | Prevalence | Special considerations for management | Access | Experiences |
|---|---|---|---|---|---|---|
| Arua et al., 2023 | Nigeria | Prison | ||||
| Bozelko et al., 2020 | USA | Prison | ✓ | ✓ | ||
| Carlen, 1983 | UK | Prison | ✓ | |||
| Carter, 1969 | UK | Other detention facility | ✓ | |||
| Centro pela Justiça e pelo Direito Internacional, 2007 | Brazil | Prison | ✓ | |||
| Chirwa, 2001 | Uganda | Prison | ✓ | |||
| Chirwa, 2002 | Malawi | Prison, jail, ther detention facility | ✓ | |||
| Chirwa, 2004 | Ethiopia | Prison | ✓ | |||
| de Araújo et al., 2020 | Brazil | Prison | ✓ | |||
| Deboscker et al., 2021 | French Guiana | Prison | ✓ | ✓ | ✓ | |
| de Sousa‐Rodrigues et al., 2006 | Brazil | Prison | ✓ | |||
| Fontebo, 2013 | Cameroon | Prison | ✓ | ✓ | ||
| Gender, Health & Justice Research Unit, 2012 | South Africa | Prison | ✓ | |||
| Goodman et al., 2016 | USA | Jail | ✓ | ✓ | ||
| Grady, 1999 | USA | Prison | ✓ | |||
| Gullberg, 2013 | UK | Prison | ✓ | |||
| Hatton, 2006 | USA | Jail | ✓ | |||
| Ishihara, 1986 | Japan | Juvenile facility | ✓ | |||
| Kraft‐Stolar, 2015 | USA | Prison | ✓ | ✓ | ||
| Leite Araújo et al., 2019 | Brazil | Juvenile facility | ✓ | |||
| Litt and Cohen, 1973 | USA | Other detention facility | ✓ | |||
| Luyt and Du Preez, 2010 | South Africa | Prison, jail, other detention facility | ✓ | |||
| Morton et al., 1953 | USA | Prison, other detention facility | ✓ | |||
| Nangia and Fontebo, 2017 | Cameroon | Prison | ✓ | |||
| Office of the Inspectorate Te Tari Tirohia | New Zealand | Prison | ✓ | ✓ | ||
| Plugge et al., 2006 | UK | Prison | ✓ | |||
| Ribeiro et al., 2013 | Brazil | Prison | ✓ | |||
| Rowe and Waters, 1935 | USA | Prison | ✓ | |||
| Sabbagh Steinberg, 2018 | USA | Prison | ✓ | |||
| Samakayi‐Makaratie, 2003 | Zimbabwe | Prison | ✓ | ✓ | ||
| Smith, 2009 | UK | Prison | ✓ | ✓ | ||
| Todrys and Amon, 2011 | Zambia | Prison | ✓ | |||
| Topp et al., 2016 | Zambia | Prison | ✓ | |||
| Topp et al., 2017 | Zambia | Prison | ✓ | |||
| Twea, 2004 | Malawi | Prison | ✓ | |||
| United Nations, 2012 | Somalia | Prison, community alternatives | ✓ | |||
| Valent et al., 1973 | Slovakia | Other detention facility | ✓ | |||
| Young and Reviere, 2001 | USA | Prison | ✓ |
| Reference and year | Country | Setting | Prevalence | Special considerations for management | Access | Experiences |
|---|---|---|---|---|---|---|
| Adamopou‐lous et al., 1982 | Greece | Other detention facility | ✓ | |||
| Allsworth et al., 2007 | USA | Prison and jail | ✓ | |||
| Andrade et al., 2017 | Brazil | Prison | ✓ | |||
| D'Alessand‐ro et al., 1972 | Italy | Other detention facility | ✓ | |||
| de Araújo et al., 2020 | Brazil | Prison | ✓ | |||
| Deboscker et al., 2022 | French Guiana | Prison | ✓ | |||
| Harner and Burgess, 2011 | USA | Prison | ✓ | |||
| Hatton et al., 2006 | USA | Jail | ✓ | |||
| Ingram‐Fogel, 1991 | USA | Prison | ✓ | ✓ | ||
| Ishihara, 1986 | Japan | Juvenile facility | ✓ | |||
| Kraft‐Stolar, 2015 | USA | Prison | ✓ | ✓ | ✓ | |
| Plugge et al., 2006 | UK | Prison | ✓ | ✓ | ✓ | ✓ |
| Rowe and Waters, 2006 | USA | Prison | ✓ | |||
| Singla et al., 2020 | India | Prison | ✓ | |||
| Smith, 2009 | UK | Prison | ✓ | ✓ | ||
| Stephens, 2015 | USA | Juvenile facility | ✓ | |||
| Sutcliffe et al., 2010 | USA | Prison | ✓ |
| Reference and year | Country | Setting | Prevalence | Special considerations for management | Access | Experiences |
|---|---|---|---|---|---|---|
| Acheampong et al., 2021 | Ghana | Prison | ✓ | ✓ | ||
| Alcivar et al., 2020 | Venezuela | Prison | ✓ | |||
| Artymuk and Marochko, 2016 | Russia | Prison | ✓ | |||
| Artymuk and Marochko, 2016 | Russia | Unspecified | ✓ | |||
| Cañadas et al., 1998 | Spain | Prison | ✓ | |||
| Cerqueira et al., 1998 | Brazil | Prison | ✓ | |||
| Clarke et al., 2006 | USA | Prison and jail | ✓ | |||
| Coker et al., 1998 | USA | Prison | ✓ | |||
| D'Eça Junior et al., 2011 | Brazil | Prison | ✓ | |||
| De Araújo et al., 2020 | Brazil | Prison | ✓ | |||
| de Insuasty et al., 2008 | Colombia | Prison | ✓ | |||
| De Jesús Cabrera López et al., 2015 | Mexico | Juvenile facility | ✓ | |||
| De Sanjosé et al., 2000 | Spain | Prison | ✓ | |||
| Delage de Luget et al., 2022 | France | Other detention facility | ✓ | ✓ | ||
| Di Giussepe et al., 2022 | Italy | Prison | ✓ | ✓ | ||
| dos Anjos Sde et al., 2013 | Brazil | Prison | ✓ | |||
| Emerson et al., 2020 | USA | Jail | ✓ | ✓ | ✓ | ✓ |
| Emerson et al., 2020 | USA | Jail | ✓ | |||
| Emerson et al., 2021 | USA | Jail | ✓ | ✓ | ||
| Farley et al., 2000 | USA | Prison | ✓ | |||
| Gender, Health & Justice Research Unit, 2012 | South Africa | Prison | ✓ | |||
| Henderson et al., 2010 | USA | Other detention facility | ✓ | |||
| Holland‐Hall et al., 2002 | USA | Other detention facility | ✓ | ✓ | ✓ | |
| Ingram‐Fogel, 1991 | USA | Prison | ✓ | ✓ | ||
| Jiamset et al., 2019 | Thailand | Jail | ✓ | ✓ | ||
| Kanbergs et al., 2023 | USA | Prison | ✓ | ✓ | ||
| Kelly et al., 2017 | USA | Jail | ✓ | ✓ | ||
| Kelly et al., 2022 | USA | Jail | ✓ | |||
| Kesha et al., 2011 | USA | Prison | ✓ | |||
| Kim et al., 2006 | USA | Jail | ✓ | ✓ | ||
| Kim et al., 2011 | USA | Jail | ✓ | |||
| Kouyoumdjian et al., 2018 | Canada | Prison and jail | ✓ | |||
| Kraft‐Stolar, 2015 | USA | Prison | ✓ | ✓ | ✓ | |
| Lee, 1987 | Australia | Other detention facility | ✓ | |||
| Lipnicky et al., 2022 | USA | Jail | ✓ | |||
| Mahto and Zia, 2008 | UK | Prison | ✓ | ✓ | ||
| Mehta et al., 2020 | India | Prison | ✓ | |||
| Michelsen, 1969 | Colombia | Prison | ✓ | |||
| Miranda et al., 2000 | Brazil | Prison | ✓ | |||
| Miranda et al., 2004 | Brazil | Prison | ✓ | |||
| Modie‐Moroka, 2003 | Botswana | Prison | ✓ | |||
| Moore et al., 2019 | USA | Prison | ✓ | ✓ | ✓ | |
| Muscat et al., 2022 | Malta | Prison | ✓ | |||
| Nicolau et al., 2012 | Brazil | Prison | ✓ | ✓ | ||
| Pereira Borges et al., 2018 | Brazil | Prison | ✓ | |||
| Pereyra, 1961 | USA | Prison | ✓ | |||
| Philipp, 1987 | UK | Prison | ✓ | |||
| Pickett et al., 2018 | USA | Jail | ✓ | |||
| Plugge et al., 2006 | UK | Prison | ✓ | ✓ | ||
| Ribeiro et al., 2013 | Brazil | Prison | ✓ | |||
| Ruiz‐Maza et al., 2018 | Peru | Prison | ✓ | ✓ | ✓ | |
| Singla and Mehta, 2022 | India | Prison | ✓ | |||
| Stevens and Zierler, 1995 | USA | Prison | ✓ | |||
| Tavares de Oliveira et al., 2020 | Brazil | Prison | ✓ | |||
| Teck et al., 2016 | USA | Other detention facility | ✓ | |||
| Young and Reviere, 2001 | USA | Prison | ✓ |
| Reference and year | Country | Setting | Prevalence | Special considerations for management | Access | Experiences |
|---|---|---|---|---|---|---|
| Alward, 1966 | USA | Other detention facility | ✓ | |||
| Butler et al., 2000 | Australia | Prison, other detention facility | ✓ | |||
| Clarke et al., 2006 | USA | Prison and jail | ✓ | |||
| De Jesús Cabrera López et al., 2015 | Mexico | Juvenile facility | ✓ | |||
| Di Giuseppe et al., 2022 | Italy | Prison | ✓ | ✓ | ||
| Farley et al., 2000 | USA | Prison | ✓ | |||
| Gallagher, 1970 | UK | Other detention facility | ✓ | |||
| Mahto and Zia, 2008 | UK | Prison | ✓ | ✓ | ||
| Nijhawan et al., 2012 | USA | Prison and jail | ✓ | |||
| Robertson and George, 1970 | UK | Juvenile facility | ✓ | |||
| Stephens et al., 2015 | USA | Juvenile facility | ✓ |
| Reference and year | Country | Setting | Prevalence | Special considerations for management | Access | Experiences |
|---|---|---|---|---|---|---|
| Binswanger et al., 2009 | USA | Prison and jail | ✓ | |||
| Keighley, 1871 | UK | Prison | ✓ | |||
| Kraft‐Stolar, 2015 | USA | Prison | ✓ | |||
| Pereyra, 1961 | USA | Prison | ✓ | |||
| Philipp, 1987 | UK | Prison | ✓ |
| Reference and year | Country | Setting | Prevalence | Special considerations for management | Access | Experiences |
|---|---|---|---|---|---|---|
| Aday and Farney, 2014 | USA | Prison | ✓ | ✓ | ||
| de Cássia Ferreira et al., 2017 | Brazil | Prison | ✓ | |||
| Grady, 1999 | USA | Prison | ✓ | |||
| Jaffe et al., 2021 | USA | Jail and Prison | ✓ | ✓ | ✓ | |
| Jaffe et al., 2022 | USA | Prison | ✓ | ✓ | ||
| Schneider‐Reinkens, 1969 | Germany | Other Detention Facility | ✓ | |||
| Woodall et al., 2021 | UK | Prison | ✓ | |||
| Young and Reveire, 2001 | USA | Prison | ✓ |
| Reference and year | Country | Setting | Prevalence | Special considerations for management | Access | Experiences |
|---|---|---|---|---|---|---|
| de Araújo et al., 2020 | Brazil | Prison | ✓ | |||
| Getachew et al., 2021 | Ethiopia | Prison | ✓ | |||
| Haller et al., 2010 | Switzerland | Juvenile facility | ✓ | |||
| Hatton et al., 2006 | USA | Jail | ✓ | ✓ | ||
| Kraft‐Stolar, 2015 | USA | Prison | ✓ | ✓ | ||
| Miranda et al., 2000 | Brazil | Prison | ✓ | |||
| Modie‐Moroka, 2003 | Botswana | Prison | ✓ | ✓ | ||
| Ribeiro De Menenzes et al., 2021 | Brazil | Prison | ✓ | ✓ | ||
| Singla et al., 2020 | India | Prison | ✓ | |||
| Smith, 2009 | UK | Prison | ✓ | ✓ | ||
| Sutcliffe et al., 2010 | USA | Prison | ✓ | |||
| Stephens et al., 2015 | USA | Juvenile facility | ✓ | |||
| Young, 1998 | USA | Prison | ✓ |
| Reference and year | Country | Setting | Prevalence | Special considerations for management | Access | Experiences |
|---|---|---|---|---|---|---|
| Drennan et al., 2010 | UK | Prison | ✓ | ✓ | ✓ | |
| Grady, 1999 | USA | Prison | ✓ | ✓ | ✓ | |
| Mahmood et al., 2020 | Pakistan | Jail | ✓ | |||
| Ribeiro de Menezes, 2021 | Brazil | Prison | ✓ | ✓ | ||
| Rice et al., 2021 | Australia | Prison | ✓ | |||
| Philipp, 1987 | UK | Prison | ✓ | |||
| Young and Reviere, 2001 | USA | Prison | ✓ |
| Reference and year | Country | Setting | Prevalence | Special considerations for management | Access | Experiences |
|---|---|---|---|---|---|---|
| Alonso‐Sanz et al., 1996 | Spain | Prison | ✓ | |||
| Caloenescu et al., 1973 | Canada | Other detention facility | ✓ | |||
| Celia Bórquez et al., 2022 | Chile | Prison | ✓ | |||
| Farhoudi et al., 2022 | Iran | Prison | ✓ | |||
| Farley et al., 2000 | USA | Prison | ✓ | |||
| Friedman et al., 2021 | USA | Jail | ✓ | |||
| Gallagher, 1970 | UK | Other detention facility | ✓ | |||
| Garcia et al., 2004 | Portugal | Prison | ✓ | |||
| Getachew et al., 2021 | Ethiopia | Prison | ✓ | |||
| Haller et al., 2009 | Switzerland | Juvenile facility | ✓ | |||
| Haller et al., 2010 | Switzerland | Juvenile facility | ✓ | |||
| Hatton et al., 2006 | USA | Jail | ✓ | ✓ | ||
| Holland‐Hall et al., 2002 | USA | Other detention facility | ✓ | ✓ | ✓ | |
| Keighley, 1971 | UK | Prison | ✓ | |||
| Klobusický et al., 1989 | Slovakia | Prison | ✓ | |||
| Kraft‐Stolar, 2006 | USA | Prison | ✓ | |||
| Lee, 1987 | Australia | Jevenile facility | ✓ | |||
| Leite Araújo et al., 2019 | Brazil | Juvenile facility | ✓ | |||
| López‐Barbosa et al., 2009 | Colombia | Jail | ✓ | |||
| Mahto and Zia, 2008 | UK | Prison | ✓ | ✓ | ||
| Miranda et al., 2000 | Brazil | Prison | ✓ | |||
| Miranda et al., 2004 | Brazil | Prison | ✓ | |||
| Muscat et al., 2022 | Malta | Prison | ✓ | |||
| Nicholson et al., 2003 | Australia | Prison | ✓ | |||
| Nijhawan et al., 2012 | USA | Jail and Prison | ✓ | |||
| Oliván Gonzalvo, 2002 | Spain | Other detention facility | ✓ | |||
| Pereira Borges et al., 2018 | Brazil | Prison | ✓ | |||
| Ribeiro et al., 2013 | Brazil | Prison | ✓ | |||
| Ris and Dodge, 1973 | USA | Juvenile facility | ✓ | |||
| Risser et al., 2004 | USA | Juvenile facility | ✓ | |||
| Sabbagh Steinberg, 2018 | USA | Prison | ✓ | ✓ | ✓ | |
| Sarpong et al., 2015 | Ghana | Prison | ✓ | ✓ | ||
| Stephens et al., 2015 | USA | Juvenile facility | ✓ | |||
| Sutcliffe et al., 2010 | USA | Prison | ✓ | |||
| Valent et al., 1973 | Slovakia | Juvenile facility | ✓ | |||
| Young, 1998 | USA | Prison | ✓ |
| Reference and year | Country | Setting | Condition | Prevalence | Special considerations for management | Access | Experiences |
|---|---|---|---|---|---|---|---|
| Alward, 1966 | USA | Juvenile facility | Erosion of cervix, Müllerian anomalies | ✓ | |||
| Andrade, et al., 2017 | Brazil | Prison | Pelvic ultrasound abnromalities | ✓ | |||
| Rowe and Waters, 1935 | USA | Prison | Ovarian failure | ✓ | |||
| Young, 1998 | USA | Prison | Ovarian cysts | ✓ |
- —National Institute of Child Health and Human Development10.13039/100009633
- —University of Minnesota10.13039/100007249
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCriminal Justice and Corrections Analysis · Sexual Assault and Victimization Studies · Adolescent Sexual and Reproductive Health
INTRODUCTION
1
More than 740 000 people identified as female in intake are incarcerated globally as of 2022, reflecting a 60% global increase since the year 2000.1 The USA unfortunately leads this trend, with the increase in incarceration among people assigned female far outpacing both those assigned as male in the USA and female incarceration in all other countries.1, 2 The scope of this review is global, but considering national disparities in rates of incarceration, much of the framing centers on the US criminal legal system. In the USA, carceral settings include jails, which generally house people awaiting trial or serving short sentences, and prisons, which house people with longer sentences. The terminology used to describe facilities outside of the USA varies, as do the criminal legal structures that determine where and for how long individuals are incarcerated in those settings.3
Many gynecologic conditions, including the physiologic processes of menstruation and menopause, likely require accommodation for those experiencing incarceration in settings where people lack control over access to menstrual products or lifestyle modifications.4, 5 Moreover, managing common gynecologic concerns including abnormal uterine bleeding and cervical dysplasia, which might be more common or less well managed among people who are incarcerated, requires special considerations given the high prevalence of trauma history and the long‐documented history of reproductive coercion by carceral facilities and criminal legal system staff members.5, 6, 7, 8, 9
The American College of Obstetricians and Gynecologists states that people experiencing incarceration should have access to the full scope of reproductive care.5 Historically, however, research on the obstetric and gynecologic healthcare needs of people experiencing incarceration has focused on pregnancy care, sexually transmitted infections, and cervical dysplasia.10, 11, 12, 13 Recent reviews highlighting the difficult realities of contraception and abortion access in carceral settings and the ongoing high prevalence of human papilloma virus (HPV) and cervical dysplasia and cancer among people experiencing incarceration reflect the prioritization of these issues.7, 14, 15, 16
The aim of this review was to answer the following questions: (1) What is the prevalence of benign and malignant gynecologic conditions among people experiencing incarceration? (2) What are special considerations for managing benign and malignant gynecologic conditions in carceral settings? (3) What is access to services for benign and malignant gynecologic conditions like during incarceration? (4) How does incarceration affect experiences of benign and malignant gynecologic conditions?
METHODS
2
Reporting guidelines and registration
2.1
This review follows the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) extension for scoping reviews.17
Eligibility criteria
2.2
We considered carceral facilities to include jails, prisons, remand facilities, and other settings detaining people below the age of majority. Studies were eligible for the review if they (i) discussed a benign or malignant gynecologic condition; (ii) included a population of people experiencing incarceration; and (iii) answered one or more of the four key questions identified prior to the search. These questions were modeled after aspects of the Aday and Anderson Framework for the Study of Access to Care and addressed prevalence, special management considerations, access to services, and patient experience.18 All reference types were included except for review articles, commentaries, and book reviews. Gynecologic conditions included abnormal bleeding, menopause, pelvic pain, pelvic organ prolapse, urinary incontinence, cervical cancer screening, dysplasia, HPV, vaginitis, menstruation, and gynecologic malignancy. We also included general gynecologic care.
We excluded several groups of studies. First, studies focused on care for sexually transmitted infections, pregnancy, contraception, and abortion in carceral contexts have been covered extensively in previous reviews. Second, we excluded studies reviewed in two prior systematic reviews on the prevalence of cervical dysplasia and HPV in populations experiencing incarceration.7, 16 Third, we excluded studies conducted in World War II incarceration camps to avoid inclusion of data known to have been collected in violation of human rights. Studies describing US immigration detention centers were also excluded as they represent a part of the civil legal system.1, 3, 19 Finally, we excluded studies reporting on topics we did not consider benign or malignant gynecologic conditions: sexual behavior, forensics, sexual assault, domestic violence, intimate partner violence, and menstruation as a criminal defense or explanation of criminal behavior.
Information sources and search strategy
2.3
Our research team, including a health sciences librarian, developed the search strategy. With a final search date of April 19, 2023, the librarian searched APA PsycInfo (EBSCOhost), CINAHL Plus with Full Text (EBSCOhost), Embase (Elsevier), PubMed (https://pubmed.ncbi.nlm.nih.gov/), Scopus (Elsevier), and the ClinicalTrials.gov registry.
The search strategy included a combination of keywords and subject headings for incarceration and benign or malignant gynecologic conditions with no language or date limits. The PubMed search is shown in Table 1, and the complete, reproducible search strategy for all databases is available in the supplementary files. The research team also searched the cited references of all included studies.
References were exported to Endnote X9 (Philadelphia, Pennsylvania, USA), where duplicates were removed. The remaining studies were imported into Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia, available at www.covidence.org) to organize and complete the review process.
Study selection
2.4
One researcher independently screened each reference title and abstract for eligibility. In the full text review stage, two reviewers independently screened each reference. Conflicts were resolved by consensus of the full research team or by the lead author.
Data extraction and synthesis
2.5
We created a data extraction template capturing the reference title, lead author, year of publication, country, gynecologic condition, and key question type (prevalence, management, access, or experience). One researcher extracted data from each study, with a second reviewer verifying the extracted data.
We synthesized data according to the condition described and by the four key questions above pertaining to prevalence, management, access, or experience.
RESULTS
3
We identified 3417 citations that met our search criteria (Figure 1). After removing duplicates, we assessed 2150 titles and abstracts and 688 full texts for eligibility; 135 studies were included, corresponding to 137 reports. Included studies addressed all four of the key questions, and most addressed more than one. The studies came from 38 distinct countries, with the majority from the USA (n = 49) Brazil (n = 17) and the UK (n = 13). There were a variety of study designs, with a majority being cross‐sectional descriptive studies, including many survey studies and chart review studies. There were also many studies that included qualitative methodologies. Some reports were published by governmental agencies and non‐governmental organizations. Because of the heterogeneity of data sources, the study design and methods were not always explicitly stated. The studies were conducted in a variety of settings, with a majority in prisons or jails, and a fair number in juvenile detention facilities.6, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108, 109, 110, 111, 112, 113, 114, 115, 116, 117, 118, 119, 120, 121, 122, 123, 124, 125, 126, 127, 128, 129, 130, 131, 132, 133, 134, 135, 136, 137, 138, 139, 140, 141, 142, 143, 144, 145, 146, 147, 148, 149, 150, 151, 152, 153, 154, 155
PRISMA flow diagram demonstrating study selection process.
Gynecologic care and exams
3.1
Twenty‐three studies discussed the provision of routine or screening gynecologic care and exams, including 13 US studies, six from Brazil, two from the UK, and one each from Ghana and South Africa. Sixteen studies took place in prisons, three in jails, and four in other or a combination of facility types (Table 2).46, 63, 65, 67, 69, 72, 76, 77, 79, 80, 81, 95, 97, 101, 107, 117, 118, 127, 136, 138, 145, 153, 155 Two studies discussed the prevalence of requesting a gynecology appointment, and six studies discussed the prevalence of receiving gynecologic exams in carceral facilities.46, 79, 80, 81, 97, 107, 117, 118 A study in a Brazilian correctional facility for adolescents found that 13 of 26 (50%) individuals received a gynecological cancer prevention exam, with eight (61.5%) of those being more than 1 year ago.97 A study in a juvenile facility in the USA found that 87/133 (77%) of sexually active adolescents reported that they had a pelvic exam within the past year.79 Ingram‐Fogel found that in a prison in the USA, 72.7% of health care appointments made by participants were for gynecologic conditions, and 39.6% of the participants had “chronic” gynecological conditions.81 Several studies described rates of ongoing gynecologic care. Nicolau et al. found that 65 women (42%) received routine gynecologic care gynecologic care while incarcerated, ranging from every month to annually, and some were at inconsistent intervals.117, 118 De Araújo et al. found that in a Brazilian prison, 9% (n = 115) of women had never had a gynecological exam.46
Special considerations for routine gynecologic care discussed in seven studies included the need for gynecology‐focused educational initiatives and disparities in gynecologic care by socio‐demographic factors.63, 72, 76, 79, 95, 136, 138 In one of these, Fink et al. described a curriculum developed around gynecologic care in a correctional center instructing on four areas: anatomy and physiology, vaginal ecology, the pelvic exam, and sexual health.63 Gallagher et al. found that access varied in juvenile facilities and was significantly more likely in “all‐female, state‐owned, large populations and longer stay facilities” compared to short‐term, mixed gender, or locally‐ or privately‐operated facilities.67
Access to services was discussed in 18 studies, and key themes discussed were difficulty requesting appointments, lack of appropriate gynecologic healthcare, and financial burden of obtaining gynecologic care during incarceration.46, 65, 67, 69, 72, 77, 79, 81, 95, 101, 117, 118, 127, 136, 138, 145, 153, 155 Incarceration affecting experiences of gynecologic care and exams was discussed in five studies.69, 72, 77, 95, 136 For example, one US jail was reported to have inadequate health care for gynecologic conditions and unsanitary living conditions, such as residents being provided used underwear, causing them to develop gynecologic symptoms.77
Consistent and reliable access to gynecological care and exams is generally difficult in carceral settings and is complicated by the availability of gynecologic appointments and providers, patients' trust in their providers, and many of the social determinants of health that also affect care outside of carceral settings.
Normal menstruation
3.2
Thirty‐eight studies discussed normal menstruation during incarceration (Table 3).29, 31, 35, 36, 39, 40, 41, 46, 51, 52, 64, 69, 71, 72, 73, 77, 82, 95, 97, 99, 102, 112, 114, 115, 120, 126, 127, 129, 134, 136, 137, 148, 149, 150, 151, 152, 155, 156 The studies were performed in the USA (n = 10), the UK (n = 5), Brazil (n = 5), Zambia (n = 3), Cameroon (n = 2), Malawi (n = 2), and South Africa (n = 2), and one each in Ethiopia, French Guiana, Japan, Malawi, New Zealand, Nigeria, Somalia, and Slovakia, Uganda, and Zimbabwe. Twenty‐seven studies were conducted in prisons, two in jails, two in juvenile facilities, three in other detention facilities, and four in a combination of facility types. Twelve studies discussed the prevalence of normal menstruation, premenstrual syndrome, or details about menstruation such as age of menarche or length of menstrual cycle.36, 46, 51, 52, 82, 97, 99, 112, 129, 134, 152, 156 Three studies reported a prevalence of regular menstruation between 13/115 (11%) and 806/1198 (76.4%).46, 82, 156 In another, only one woman of 14 interviewed reported normal cycles.52 Several studies in juvenile facilities reported 12–13 years as the mean or modal age at menarche, similar to a comparison group from one study of non‐institutionalized young people.36, 97, 99, 129, 152 Studies reported a 29%–67% (20/29) prevalence of “PMS,” severe premenstrual symptoms, or bothersome periods.36, 51, 112, 156
Twenty‐four studies discussed access to care for and management of normal menstruation, most of which centered on a lack of adequate supply of menstrual products, with many people relying on donations from outside groups like non‐governmental organizations or churches or on their families to bring in period management supplies.30, 38, 39, 40, 51, 63, 68, 70, 71, 76, 94, 101, 113, 114, 119, 125, 126, 135, 136, 147, 148, 149, 150, 154 The number of these studies is high, and they almost uniformly describe inadequate access to period products and a lack of autonomy in obtaining the products they need, with one study reporting that people must approach male correctional officers and provide specific reasons to request products.72 Another study discussed a lack of access to a toilet early in the morning, which was often when participants reported discovering that their period had started.136 One study, in contrast, stated that “83.89% [of respondents] indicated that the availability of women's hygiene articles was not a problem.”102 A survey found that 64/65 (98%) of institutions reported that they asked patients about menstrual cycles on intake and/or physical examinations.155 Outside discussions of access to management of normal menstruation and experiences of normal menstruation during incarceration, no studies focused on special considerations for management of normal menstruation in these settings.
Ten studies discussed experiences of normal menstruation by people experiencing incarceration.31, 35, 52, 64, 71, 73, 95, 120, 137, 156 Much of the focus of these was on the impact on self‐esteem and powerlessness that menstruating without proper access to period products has, how this is another area where the prison has control, and the people menstruating experience humiliation and violation of privacy.31, 52, 71, 73, 95, 120, 156 Studies also discussed the alternatives people used to manage menstruation in response to the lack of adequate supply of products, including using “newspapers by rubbing the numbers to make them more absorbent.”137
Many studies regarding access to products for managing normal menstruation and exploring the ways incarceration impacts experiences of normal menstruation met our inclusion criteria, and most focused on the inadequacy of period products and the shame and lack of privacy and autonomy that accompany menstruating while experiencing incarceration.
Abnormal uterine bleeding
3.3
Seventeen studies addressed abnormal uterine bleeding (AUB) (Table 4).6, 21, 26, 44, 46, 52, 76, 77, 81, 82, 95, 126, 134, 140, 142, 144, 156 These studies were performed in the USA (n = 8), Brazil (n = 2), the UK (n = 2), and one each in French Guiana, Greece, India, Italy, and Japan. They took place in prisons (n = 11), jails (n = 1), and other or multiple institutional facilities (n = 5). Prevalence of AUB was discussed in 13 studies and ranged from 6.4% (of 507) to 88.7% (n = 102).6, 26, 44, 46, 52, 81, 82, 126, 134, 140, 142, 144, 156 A study in a UK prison found that 49% of women reported their periods changed following imprisonment.156 Deboscker et al. found that nearly all study participants in a French Guianan prison experienced changes in their menstrual cycle during incarceration.52
Four studies emphasized special considerations for AUB, including a lack of access to hygiene products and trauma history.21, 76, 95, 126 Access to services was discussed in three studies, and key themes were the receipt of an inadequate number of menstrual products and a lack of full‐spectrum medical and surgical management options for AUB.81, 95, 126 For example, Kraft‐Stolar, in a New York state report, describes women reporting hysterectomies performed for abnormal uterine bleeding without proper education regarding alternatives to major surgery.95 In the USA, Ingram‐Fogel found that many individuals with menstrual difficulties reported not seeking health care as they found the prison system to be unresponsive, and they did not trust the health care they were given.81 The effect of incarceration on the experience of abnormal uterine bleeding was discussed in four studies.77, 95, 126, 156 Multiple studies discussed a lack of education for patients in carceral settings around the causes and options for management of abnormal uterine bleeding.
Overall, abnormal uterine bleeding is highly prevalent in carceral facilities, with patients reporting a lack of education around their conditions and diagnoses, decreased autonomy related to medical decision‐making, and not enough access to either menstrual products or gynecological providers while incarcerated.
Cervical dysplasia and human papillomavirus
3.4
After excluding studies included in past systematic reviews on cervical dysplasia and HPV in people experiencing incarceration, there were 56 studies that met our inclusion criteria (Table 5).20, 23, 27, 28, 34, 38, 42, 43, 45, 46, 48, 49, 50, 53, 54, 55, 58, 59, 60, 62, 69, 78, 79, 81, 85, 86, 88, 89, 90, 91, 92, 94, 95, 96, 98, 104, 105, 106, 107, 108, 109, 111, 113, 118, 122, 123, 124, 125, 126, 129, 135, 140, 143, 146, 147, 155 They were performed in the USA (n = 23), Brazil (n = 10), the UK (n = 3), Colombia (n = 2), India (n = 2), Russia (n = 2), Spain (n = 2), and one study each in Australia, Botswana, Canada, France, Ghana, Italy, Malta, Mexico, Peru, South Africa, Thailand, and Venezuela. Most took place in prisons (n = 37), and 10 were in jails, with 9 in other or multiple institutional facilities. Forty‐one studies reported a prevalence of cervical dysplasia (1/38 [2.6%]–47/157 [29.9%]) and HPV (8/214 [3.3%]–44/93 [52.7%]).20, 23, 27, 28, 34, 38, 42, 43, 45, 48, 49, 50, 53, 54, 55, 60, 62, 79, 81, 85, 90, 91, 92, 96, 104, 105, 106, 107, 108, 109, 111, 113, 118, 123, 124, 125, 126, 129, 135, 140, 143
Special considerations affecting management of HPV and cervical dysplasia in people experiencing incarceration were discussed in 14 studies and often centered on HPV vaccination status and histories of sexual abuse.20, 53, 54, 58, 59, 60, 79, 86, 88, 89, 92, 95, 135, 147 Other key themes included a delay or lack of proper follow‐up care or procedures, structural and financial challenges, competing demands, and lack of stability.89, 95 A study in a US prison found that women who had sexual intercourse at an earlier age or experienced sexual abuse were more likely to enter prison with cervical dysplasia.43 Emerson et al. found that in a US jail, age was a risk factor for out‐of‐date Pap smears; the odds of up‐to‐date cervical cancer screening decreased by 5% (P < 0.05) for every 1‐year increase in age.60
Access to services was discussed in 20 studies.46, 59, 60, 69, 78, 79, 81, 85, 86, 94, 95, 98, 104, 111, 118, 122, 126, 135, 146 Pereira Borges reported that 38 of 56 women (67.86%) incarcerated in a Brazilian prison received guideline‐concordant screening.122 US carceral facilities and administrators who believed offering the HPV vaccine was important were more likely to provide other preventive sexual health services; just 39 of 50 states reported offering the HPV vaccine to incarcerated females in juvenile facilities.78, 98 Incarceration affecting experiences of cervical dysplasia and HPV was discussed in four studies.60, 89, 95, 111
Women with a history of incarceration had higher rates of reported cervical cancer and abnormal Pap smears compared to women without this history.58 There is an abundance of data on cervical dysplasia and HPV compared to the other gynecological conditions studied, detailing the high burden of these conditions in populations experiencing incarceration and the challenges of achieving universal preventive, screening, and follow‐up care.
Genital warts
3.5
Eleven studies addressed genital warts in prisons (n = 2), juvenile facilities (n = 3), other detention facilities (n = 3) or a combination of settings (n = 3) (Table 6).25, 32, 42, 49, 54, 62, 66, 104, 119, 133, 142 Five studies were performed in the USA, three in the UK, and one each in Australia, Italy, and Mexico. From 10 studies, the prevalence of genital warts was 3/110 (2.7%)–12/132 (9.1%), 36/378 (9.5%) while incarcerated and 33/474 (6.9%) of participants reporting a history of prior genital warts. Examining conditions with shared risk factors, Nijhawan et al. reported an equal rate of genital warts in patients who tested positive for trichomonas (n = 5/53, 10%) and those who did not (n = 31/325, 10%), and a study of juveniles experiencing incarceration reported that 1.7% of adolescents disclosing ecstasy use reported genital warts in the past year compared to 1.6% among those without ecstasy use (OR 0.91, 95% CI 0.32–2.61).119, 142
One study discussed special considerations for managing genital warts in carceral settings, noting that only 84/214 (39.2%) of participants in a survey knew that HPV vaccination could prevent genital warts.54 One study discussed access to services for patients with genital warts, noting a new female genito‐urinary consultant was hired to increase onsite testing and access to treatment for conditions including genital warts.104 One study discussed experiences of genital warts in the carceral setting, with 152 of 214 (71%) juvenile facility participants reporting that they would feel embarrassed to have genital warts.54 Prevalence of genital warts was reported in many studies that met our inclusion criteria, but there were limited data addressing the other key questions.
Gynecologic malignancies
3.6
There were five studies (USA, n = 3, UK, n = 2) that discussed gynecologic malignancies among people experiencing incarceration; four were conducted in prisons and one in a combination of prison and jail settings (Table 7).30, 87, 95, 123, 124 Prevalence of gynecologic malignancies was discussed in four studies, all of which reported on the prevalence of cervical cancer. The prevalence of cervical cancer ranged from 6/583 (1.0%) to 15/601 (2.5%).87, 123 Another study reported a 9% combined prevalence of premalignant or malignant conditions of the cervix.124 In the fourth, individuals in jails and prisons had increased odds of cervical cancer compared to a non‐institutionalized population (OR for jail 4.16, 95% CI 3.13–5.53, OR for prison, 4.82, 95% CI 3.74–6.22).30 One study also mentioned that “several cases of ovarian cancer were also diagnosed” but did not report a specific prevalence.124 Access to services for gynecologic malignancies was discussed in one study, which stated that “patients reported delays in gyn care leading to symptoms worsening and delays in diagnosis and treatment of cancer and cervical dysplasia.”95
Special considerations for management of gynecologic malignancies for people experiencing incarceration and experiences of gynecologic malignancies in carceral settings were not discussed in any studies. There are minimal data on gynecologic malignancies in populations experiencing incarceration, and what does exist largely focuses on cervical cancer, further highlighting both the burden of and emphasis on cervical dysplasia and cancer that occurs in this population.
Menopause
3.7
There were eight studies that discussed menopause during incarceration (Table 8).22, 47, 72, 83, 84, 139, 153, 155 Five studies were performed in the USA, one in the UK, one in Brazil, and one in Germany. Six studies took place in prisons and one in both prison and jail; the German study was conducted in an unspecified facility. Two studies reported on prevalence: a study in southeastern US prisons found that 30% of 327 of women surveyed reported “menopause problems,” with a higher rate in Black women compared to non‐Black women.22 In a North Carolina prison, 382/863 (32.8%) of all prescriptions in the facility were found to be relevant to menopause; the most prescribed medication type that can be used to manage menopause (n = 346, 30.9%) was selective serotonin reuptake inhibitors, and 68 (6.1%) were hormonal therapies.84 Special considerations affecting menopause care during incarceration, discussed in five studies, included the impact of coexisting medical conditions and poor general health.22, 72, 83, 84, 139 Two studies discussed the high prevalence of coexisting medical conditions, including hypertension, cardiovascular conditions, and mental health conditions in people experiencing incarceration that complicates management of22, 84 Jaffe et al. reported a rate of 40/1120 (3.6%) of individuals aged 45–75 receiving estrogen‐containing menopausal hormone therapy.84
Access to services was discussed in three studies.83, 153, 155 Two studies only briefly mentioned that the patients in the facilities they studied were asked about symptoms of menopause or provided education about menopause.153, 155 One qualitative study discussed a lack of access to lifestyle management of menopause, including replacement clothing and clean bedding to manage abnormal bleeding and night sweats associated with the menopause transition as well as few ceiling fans and no air conditioning.83 Incarceration affecting the experience of menopause was discussed in two studies.47, 83 Participants raised issues including a lack of menopause knowledge and the threat of disciplinary action for certain methods of coping with menopause symptoms such as sleeping without underwear to help with hot flushes.83
The studies on menopause in carceral settings highlight the complexity of caring for these patients given their lack of access to lifestyle management techniques and the high prevalence of comorbid conditions that affect pharmacologic management of menopause.
Pelvic organ prolapse
3.8
There were no studies that discussed pelvic organ prolapse in individuals experiencing incarceration.
Pelvic pain
3.9
Thirteen studies discussed pelvic pain, although this was not the primary focus of any of these studies, but rather the discussion of pelvic pain was embedded in studies on other topics, most commonly in studies on sexually transmitted infections (Table 9).46, 70, 74, 77, 95, 108, 109, 128, 140, 142, 144, 154, 156 These studies were from the USA (n = 5), Brazil (n = 2), and one each in Botswana, Ethiopia, India, Switzerland, and the UK; 10 were conducted in prisons, one in a jail, and two in juvenile facilities. Twelve of these studies reported the prevalence of pelvic pain in patients experiencing incarceration, which ranged from 5.1% (n = 6/121) to 54% (of 111).46, 70, 74, 105, 107, 108, 109, 128, 142, 144, 154, 156 Most studies reported on pelvic pain in general or primary dysmenorrhea, although the focus of one paper was on bladder pain, and another reported the prevalence of “endometriosis/ovarian cysts.”128, 154
One study discussed special considerations for management of pelvic pain, reviewing the importance of informed consent for treatment of patients experiencing incarceration.95 One study mentioned access to services for pelvic pain with study participants finding “health care inappropriate for their needs and not set up to handle female diseases … [including] endometriosis.”77 Five studies discussed experiences of pelvic pain while incarcerated.77, 95, 109, 128, 156 A participant in one study reported feeling disempowered and distressed by the care she received related to pelvic pain due to a lack of adequate explanation.95 In another study, participants reported that their dysmenorrhea worsened during their incarceration.156
These studies highlight the range of prevalence of pelvic pain in people experiencing incarceration. The qualitative studies that include direct quotes from participants highlight the impact incarceration has on pelvic symptoms, contributing to worsening pain and a lack of control in managing these symptoms.
Urinary incontinence
3.10
Seven studies addressed urinary incontinence, including two from the USA, two from the UK, and one each from Australia, Brazil, and Pakistan (Table 10).56, 72, 103, 124, 128, 130, 155 Six studies took place in prisons, and one took place in a jail. Five of these discussed the prevalence of urinary incontinence, ranging from 14% (2/14) to 93%, with one study reporting that most patients over the age of 50 have urinary incontinence.56, 103, 124, 128, 130 One study discussed special considerations for managing urinary incontinence in the carceral setting, citing one patient's inability to follow recommendations to keep a voiding diary due to the diary being confiscated by an officer.72 Three studies discussed access to services for patients with urinary incontinence.56, 72, 155 One survey found that 46/65 (71%) of respondents reported being asked about urinary incontinence at their intake visit.155 Another mentions that patients must ask officers for incontinence pads.72
Three studies discussed experiences of urinary incontinence during incarceration, highlighting the condition's impact on quality of life. Reported experiences included restricting food and water intake to manage incontinence, worrying about malodor due to incontinence, and choosing to delay treatment until a return to the community.56, 72, 128 The studies demonstrate a relatively high prevalence of urinary incontinence in people experiencing incarceration and the barriers that providers and patients experience in managing urinary incontinence during incarceration, including lack of privacy and lack of free access to sanitary supplies.
Vaginitis
3.11
There were 36 studies that discussed vaginitis among people experiencing incarceration (Table 11).24, 33, 37, 61, 62, 65, 66, 68, 70, 74, 75, 77, 79, 87, 93, 95, 96, 97, 100, 104, 107, 108, 113, 116, 119, 121, 122, 129, 131, 132, 136, 138, 142, 144, 152, 154 The studies were conducted in the USA (n = 11), Brazil (n = 5), the UK (n = 3), two each in Australia, Slovakia, Spain, and Switzerland, and one each in Canada, Chile, Colombia, Ethiopia, Ghana, Iran, Portugal, and Malta; 20 were conducted in prisons, three in jails, one in a combination of prison and jail sites, eight in juvenile facilities, and four in other detention facilities. Prevalence of vaginitis was defined variably across 32 studies as the presence of specific microorganisms, vaginal discharge, or vaginal pruritis.24, 33, 37, 61, 62, 66, 68, 70, 74, 75, 79, 87, 93, 96, 97, 100, 104, 107, 108, 113, 116, 119, 121, 122, 129, 131, 132, 136, 142, 144, 152, 154
Overall vaginitis rates ranged from n = 5/85 (6%) to n = 16/26 (62%).24, 61, 70, 74, 75, 97, 107, 108, 119, 122, 129, 144, 154 Several studies reported specific rates of Gardnerella vaginalis or bacterial vaginosis (7/66 [3%]–10/25 [40%]), trichomonas vaginalis (25/583 [4.3%]–329/556 [59%]), and candida species or yeast organisms (1/53 [2%]–91/486 [19%]).24, 33, 37, 68, 74, 79, 93, 96, 100, 104, 108, 113, 116, 119, 121, 131, 144, 152 Among women with HIV incarcerated in Rhode Island, 27/110 (25%) had vaginal candidiasis.62 Among patients being treated for trichomoniasis, there was a co‐infection rate of 25/583 (4%) for candida vaginitis.87 Individuals in a juvenile facility who had used ecstasy previously were more likely to report vaginal discharge or odor (OR 2.33, 95% CI 1.16–4.65).142
Special considerations for management of vaginitis in carceral settings were discussed in two studies and included giving patients the option to self‐test and the high rate of recurrence attributed to limited hygiene facilities.79, 138 Access to services was discussed in four studies.65, 77, 104, 138 One study described the process of accessing care and included a quote from a patient who had received advice from a nurse to exaggerate symptoms to have requests for medical care related to vaginitis be taken seriously.65 Another study found that women identified a lack of resources to maintain hygiene as a contributor to the development of vaginitis.77 One study improved access for vaginitis care by hiring a female genitourinary consultant.104 A study from Ghana described an intermittent lack of availability of drugs to treat candidiasis.138
Incarceration affecting experiences of vaginitis was discussed in one study that mentioned a patient feeling like they were not receiving adequate communication or education as to why they were having recurrent yeast infections.
Prevalence of vaginitis was commonly reported in studies about gynecologic care in carceral settings, highlighting the commonality of this complaint in this population. Experiences of vaginitis in carceral settings centered on difficulty accessing care for treatment and theorizing that hygiene practices in some facilities affected vaginitis rates.
Other gynecologic conditions
3.12
Four studies addressed the prevalence of other conditions (Table 12).25, 26, 134, 154 Young reported a rate of 6/129 (4.7%) of “endometriosis/ovarian cysts” in a US prison.154 Rowe and Waters noted premature ovarian failure in 25 patients in a Massachusetts facility in 1935 (one attributed to oophorectomy, 10 attributed to prior gonorrhea infection, and 10 without a proposed etiology).134 A 1965 presentation of data from a Los Angeles juvenile facility reported 102 cases of cervical erosion and one case of an absent vagina.25 Andrade et al. reported a rate of 58/146 (39.72%) of ultrasound abnormalities in 146 patients experiencing menstrual irregularities in a Brazil prison.26
DISCUSSION
4
Synthesis of the 135 studies included in this review demonstrated both that gynecologic conditions are common in carceral settings and that disparities in the experience of gynecologic conditions have three underpinning mechanisms. First, there are gynecologic conditions that are brought on or exacerbated by the physical and emotional stress of incarceration, such as abnormal uterine bleeding, pelvic pain, or menopausal symptoms. Second, there are shared social and structural factors, such as substance use and physical, emotional, and sexual abuse and trauma that are common among individuals experiencing incarceration and might exacerbate some gynecologic disparities (e.g., cervical dysplasia and cancer). Third, conditions of confinement, lack of access to care, and intersectional stigma intensify the physical and emotional experience of some conditions, including normal menstruation, urinary incontinence, and pelvic pain.
These findings enrich and extend the findings of previous, condition‐specific reviews. Conducting this literature review across multiple gynecologic conditions, languages, global contexts, and many decades (1930s‐present) resulted in several important throughlines. A unifying theme across time and place was the lack of adequate accommodations and supplies to manage normal menstruation or any gynecologic conditions that a person might experience during incarceration. Additionally, although we excluded studies focused exclusively on sexually transmitted infections as well as the many studies of cervical dysplasia included in recent systematic reviews, the most frequently addressed gynecologic conditions in our review, apart from normal menstruation, were cervical dysplasia and vaginitis. The persistent and international emphasis on gynecologic conditions related to sexual health would seem to belie the other gynecologic health disparities experienced by people who are incarcerated. Finally, although there have been more descriptions of interventions to improve care for gynecologic health conditions in carceral settings in recent years, there are relatively few studies proposing or testing interventions to address these health needs compared with the number of descriptive studies.
There are important policy implications from our findings. Although mass de‐carceration is likely the most straightforward approach to minimizing the gynecologic disparities that result from incarceration, interim steps to improve conditions of confinement are needed. The most urgent of these might be the provision of adequate sanitary supplies for people experiencing normal menstruation, abnormal uterine bleeding, and urinary incontinence. Although philosophies of incarceration and punishment vary across settings, the United Nations Basic Principles for Treatment of Prisoners require treatment “with respect due to their inherent dignity and value as human beings,” precluding shaming and/or degrading incarcerated individuals for their bodily functions.157
Adequate provision of basic supplies will go a long way toward the humane management of gynecologic conditions, and studies on normal and abnormal menstruation, pelvic pain, urinary incontinence, and vaginitis also emphasized the importance of decreasing stigma and promoting bodily autonomy and self‐determination. The practice of trauma‐informed care (i.e., care that identifies trauma and related symptoms, trains staff on the effects of trauma, and minimizes re‐traumatization) offers a way forward in clinical spaces.158 Programs such as Amend at the University of California, San Francisco, which bring dignity‐driven and public health‐oriented practices from Norway and elsewhere to improve the culture in US prisons, can serve as a roadmap for carceral systems where trauma‐informed care is not yet the norm.159
There are also critical changes needed globally to the systems of care that people access during incarceration. The studies we reviewed evinced substantial concerns expressed about the lack of competent and trustworthy providers in the context of accessing routine gynecologic care and care for abnormal uterine bleeding, menopause, and vaginitis. Addressing these gaps in the provider workforce will require multi‐pronged efforts to dismiss or remediate providers who are not prepared to provide trauma‐informed, community‐standard care and to make clinical positions within carceral facilities desirable to providers with the necessary skills. Important steps to accomplish the latter will include improving the physical and human resources in carceral clinical settings, actively destigmatizing carceral medicine as a valued public service career path and establishing universal training in trauma‐informed care.
Beyond improvements to clinical services, studies across multiple gynecologic conditions also identified a need for health education about abnormal uterine bleeding and menopause. Although there have been reports of educational interventions focused on reducing risk for STIs including HIV, similar educational programs focused on non‐sexually transmitted gynecologic conditions are limited.160, 161 In addition, although the authors are aware of educational activities outside the USA (Knittel, personal communication), fewer of these interventions have been published in the peer‐reviewed literature. Taking inspiration from the internet‐based sexual health empowerment curriculum developed in Midwestern USA, health researchers and educators globally would do well to create low‐cost, easily disseminated, and scientifically accurate educational resources about gynecologic conditions across the life course.162
Finally, this synthesis of global literature reveals a substantial gap in the literature on studies of conditions that disproportionately affect aging and older adults. We found relatively few studies examining either gynecologic cancer experiences and outcomes or menopause experiences and no studies addressing pelvic organ prolapse. This gap remains more than a decade after the publication of a policy setting agenda to address disparities for those aging in custody that included recognition of their gynecologic needs.163
This review is not without limitations. Our scoping review methodology included a wide range of studies that varied in terms of methods, clinical focus, and quality. While this allowed us to review the global landscape of gynecologic conditions in settings of incarceration, the breadth precluded meta‐analysis or other quantitative approaches to synthesize findings. We were also limited in our review by a relative lack of intervention trials and publications describing ways to address the gynecologic health disparities identified.
CONCLUSION
5
In summary, in carceral settings across the globe, gynecologic conditions are common and often exacerbated by the physical and emotional stress of incarceration, trauma histories, lack of access to care, and conditions of confinement in these settings. Additional research efforts are needed in the arenas of health education and interventions to address gynecologic health disparities, as well as to increase understanding of the gynecologic health needs of aging and older adults. Most pressing, however, is the need for parallel efforts at global de‐carceration and policy interventions to provide for basic gynecologic needs, decrease intersectional stigma, and improve the conditions of confinement.
AUTHOR CONTRIBUTIONS
Meredith K. Wise: review conceptualization, search strategy design, abstract and full text review, data abstraction, data synthesis, manuscript drafting, final manuscript approval; Sahana Raghunathan: data abstraction, data synthesis, manuscript drafting, final manuscript approval; Sreya Upputuri: abstract and full text review, data abstraction, final manuscript approval; Elana Jaffe Brotkin: abstract and full text review, data abstraction, final manuscript approval; Tre D. Thorne: data abstraction; final manuscript approval; Jamie Conklin: search strategy design, search and database management, manuscript drafting, final manuscript approval; Andrea K. Knittel: review conceptualization, data abstraction, manuscript drafting, final manuscript approval, supervision.
FUNDING INFORMATION
This project was supported in part by funds from the National Institute of Child Health and Human Development (NICHD) (Knittel, K12HD103085, PI Neal‐Perry) and the University of Minnesota Department of Obstetrics and Gynecology (Wise).
CONFLICT OF INTEREST STATEMENT
The authors report no conflicts of interest.
Supporting information
File S1: Full Search Strategy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fair H , Walmsley R . World Female Imprisonment List: Institute for Crime & Justice Policy Research; 2022. https://www.icpr.org.uk/news‐events/2022/world‐female‐prison‐population‐60‐2000
- 2Kajstura A , Sawyer W . Women's Mass Incarceration: The Whole Pie 2023: Prison Policy Initiative; 2023. https://www.prisonpolicy.org/reports/pie 2023 women.html
- 3National Institute of Justice . Correctional Facilities: United States Government, Department of Justice. https://nij.ojp.gov/topics/corrections/correctional‐facilities#:~:text=Institutional%20corrections%20facilities%20include%20prisons,typically%20longer%20than%20a%20year
- 4American College of Obstetricians and Gynecologists ACOG practice bulletin No. 141: management of menopausal symptoms. Obstet Gynecol. 2014;123(1):202‐216.24463691 10.1097/01.AOG.0000441353.20693.78 · doi ↗ · pubmed ↗
- 5American College of Obstetricians and Gynecologists Committee on health Care for Underserved Women . ACOG Committee Opinion No. 830: reproductive health care for incarcerated pregnant, postpartum, and nonpregnant individuals. Obstet Gynecol. 2021;138(1):e 24‐e 34.33906198 10.1097/AOG.0000000000004429 · doi ↗ · pubmed ↗
- 6Allsworth JE , Clarke J , Peipert JF , Hebert MR , Cooper A , Boardman LA . The influence of stress on the menstrual cycle among newly incarcerated women. Womens Health Issues. 2007;17(4):202‐209.17560123 10.1016/j.whi.2007.02.002PMC 2170522 · doi ↗ · pubmed ↗
- 7Brousseau EC , Ahn S , Matteson KA . Cervical cancer screening access, outcomes, and prevalence of dysplasia in correctional facilities: a systematic review. J Womens Health (Larchmt). 2019;28(12):1661‐1669.30939063 10.1089/jwh.2018.7440 PMC 6919241 · doi ↗ · pubmed ↗
- 8Mc Daniels‐Wilson C , Belknap J . The extensive sexual violation and sexual abuse histories of incarcerated women. Violence Against Women. 2008;14(10):1090‐1127.18757348 10.1177/1077801208323160 · doi ↗ · pubmed ↗