Comparative evaluation of prophylactic strategies for postpartum hemorrhage in vaginal delivery
Stefania Fieni, Giovanni Morganelli, Alissa Valenti, Debora Formisano, Gabriella Maria Celora, Biancamaria Mastrandrea, Tullio Ghi

TL;DR
This study compares different oxytocin regimens to prevent postpartum hemorrhage after vaginal delivery and finds that intravenous administration is more effective than intramuscular.
Contribution
The study provides new evidence on the relative effectiveness of different oxytocin administration methods for preventing postpartum hemorrhage.
Findings
Intravenous oxytocin (5 IU or 10 IU) is more effective than intramuscular (10 IU) in reducing postpartum hemorrhage.
The two intravenous regimens (5 IU and 10 IU) show similar efficacy in preventing postpartum hemorrhage.
Nulliparity, perineal tears, and other factors are independently associated with postpartum hemorrhage.
Abstract
To compare the efficacy of different prophylactic oxytocin regimens in preventing postpartum hemorrhage (PPH) after vaginal delivery. Single‐center retrospective cohort study including all vaginal deliveries between February 1, 2022, and December 31, 2023, at a tertiary referral unit. Throughout the study period, the local protocol for PPH prevention in vaginal delivery was changed from oxytocin 10 IU intramuscular injection (IM) to 5 IU intravenous bolus (IV) and eventually to 10 IU IV. Data regarding base maternal characteristics, pregnancy course, labor, and maternal outcomes were retrospectively collected from institutional labor ward registries. The incidence of PPH was compared among the three historical cohorts who received different oxytocin regimens (10 IU IM, group A; 5 IU IV, group B; and 10 IU IV, group C) following propensity score matching for those variables that proved…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
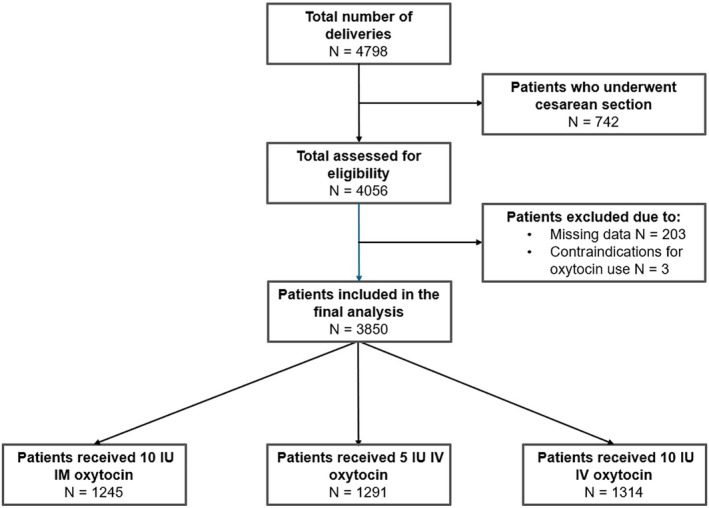 FIGURE 1
FIGURE 1| Variables | Physiologic ( | PPH ( |
|
|---|---|---|---|
| Age, year | 32.0 ± 5.22 | 31.9 ± 5.48 | 0.793 |
| BMI | 23.9 ± 4.97 | 24.1 ± 4.74 | 0.548 |
| Gestational age at delivery, week | 39.5 ± 1.72 | 39.7 ± 1.67 | 0.003 |
| Multiple gestation | 17 (0.5) | 10 (1.5) | 0.009 |
| Nulliparity | 1542 (48.8) | 435 (63.2) | <0.001 |
| Induction of labor | 1105 (34.9) | 312 (45.3) | <0.001 |
| Length of first stage, min | 180 (95–315) | 240 (135–400) | <0.001 |
| Length of second stage, min | 31 (13–85) | 62 (20–147) | <0.001 |
| Epidural analgesia | 1431 (45.3) | 402 (58.4) | <0.001 |
| Mode of delivery | |||
| Vaginal delivery | 2975 (94.1) | 615 (89.4) | <0.001 |
| Assisted vaginal delivery | 187 (5.9) | 73 (10.6) | |
| Perineal tears | |||
| None/first‐degree | 2279 (72.1) | 355 (51.6) | <0.001 |
| Episiotomy/second‐degree or higher | 883 (27.9) | 333 (48.4) | |
| Manual placenta removal | 227 (7.2) | 90 (13.1) | <0.001 |
| Birth weight, g | 3302 ± 487 | 3464 ± 514 | <0.001 |
| Variables | aOR | 95% CI |
|
|---|---|---|---|
| Age | 1.01 | 0.986–1.04 | 0.356 |
| BMI | 1.01 | 0.984–1.04 | 0.408 |
| Gestational age at delivery | 0.92 | 0.816–1.03 | 0.128 |
| Multiple gestation | 1.20 | 0.036–1.23 | 0.083 |
| Nulliparity | 1.80 | 1.298–2.50 | <0.001 |
| Induction of labor | 1.17 | 0.878–1.56 | 0.285 |
| Length of first stage | 1.00 | 0.999–1.000 | 0.298 |
| Length of second stage | 1.00 | 0.999–1.000 | 0.226 |
| Epidural analgesia | 1.18 | 0.862–1.61 | 0.302 |
| Assisted vaginal delivery | 1.20 | 0.73–1.93 | 0.464 |
| Episiotomy/second‐degree or higher tears | 2.16 | 1.623–2.86 | <0.001 |
| Manual placenta removal | 2.38 | 1.598–3.53 | <0.001 |
| Birth weight | 1.90 | 1.001–2.000 | <0.001 |
| Variables | Group A vs. Group B | Group A vs. Group C | Group B vs. Group C | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 10 IU IM ( | 5 IU IV ( |
| 10 IU IM ( | 10 IU IV ( |
| 5 IU IV ( | 10 IU IV ( |
| |
| Age, year | 32.1 ± 5.43 | 31.9 ± 5.06 | 0.688 | 32.2 ± 5.38 | 31.7 ± 5.33 | 0.177 | 31.8 ± 5.10 | 31.7 ± 5.32 | 0.753 |
| BMI | 23.8 ± 4.47 | 23.4 ± 4.61 | 0.308 | 23.9 ± 4.98 | 24.0 ± 5.14 | 0.773 | 24.0 ± 5.13 | 24.4 ± 4.79 | 0.428 |
| Gestational age at delivery, week | 39.8 ± 1.24 | 39.8 ± 1.13 | 0.877 | 39.7 ± 1.31 | 39.8 ± 1.18 | 0.193 | 39.8 ± 1.20 | 39.7 ± 1.17 | 0.624 |
| Multiple gestation | 0 | 2 (0.4) | 0.157 | 0 | 0 | ‐ | 1 (0.2) | 1 (0.2) | 1.000 |
| Nulliparity | 219 (52.8) | 219 (52.8) | 1.000 | 273 (53.3) | 273 (53.3) | 1.000 | 244 (50.3) | 244 (50.3) | 1.000 |
| Induction of labor | 147 (31.7) | 165 (35.6) | 0.211 | 158 (30.9) | 173 (33.8) | 0.316 | 165 (34.0) | 178 (36.7) | 0.383 |
| Length of first stage, min | 188 (100–380) | 190 (98–375) | 0.840 | 187 (90–380) | 179 (90–285) | 0.164 | 185 (105–360) | 160 (90–268) | 0.113 |
| Length of second stage, min | 34 (15–107) | 33 (13–85) | 0.434 | 39 (15–97) | 39 (11–100) | 0.665 | 27 (12–80) | 31 (13–97) | 0.557 |
| Epidural analgesia | 176 (38.0) | 212 (46.0) | 0.014 | 220 (43.1) | 258 (50.5) | 0.017 | 226 (46.8) | 242 (50.1) | 0.303 |
| Mode of delivery | 0.762 | 0.091 | 0.195 | ||||||
| Vaginal delivery | 442 (95.3) | 440 (94.8) | 487 (95.1) | 474 (92.6) | 464 (95.7) | 455 (93.8) | |||
| Assisted vaginal delivery | 22 (4.7) | 24 (5.2) | 25 (4.9) | 38 (7.4) | 21 (4.3) | 30 (6.2) | |||
| Perineal tears | 1.000 | 1.000 | 1.000 | ||||||
| None/first‐degree | 340 (73.3) | 340 (94.8) | 383 (74.8) | 383 (74.8) | 375 (77.3) | 375 (77.3) | |||
| Episiotomy/second‐degree or higher | 124 (26.7) | 124 (26.7) | 129 (25.2) | 129 (25.2) | 110 (22.7) | 110 (22.7) | |||
| Manual placenta removal | 7 (1.5) | 7 (1.5) | 1.000 | 1 (0.2) | 1 (0.2) | 1.000 | 10 (2.1) | 10 (2.1) | 1.000 |
| Birth weight, g | 33 704 ± 359 | 3374 ± 359 | 1.000 | 3359 ± 350 | 3359 ± 350 | 1.000 | 3358 ± 364 | 3358 ± 364 | 1.000 |
| PPH | 99 (21.3) | 51 (11.0) | <0.001 | 113 (22.1) | 86 (16.8) | 0.033 | 53 (10.9) | 67 (13.8) | 0.172 |
| Minor | 83 (83.8) | 38 (74.5) | 0.438 | 98 (86.7) | 65 (75.6) | 0.100 | 39 (73.6) | 48 (71.6) | 0.976 |
| Major (1000–1500 mL) | 13 (13.1) | 10 (19.6) | 9 (8.0) | 15 (17.4) | 8 (15.1) | 12 (17.9) | |||
| Massive (>1500 mL) | 3 (3.0) | 3 (5.9) | 6 (5.3) | 6 (7.0) | 6 (11.3) | 7 (10.5) | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and fetal healthcare · Trauma, Hemostasis, Coagulopathy, Resuscitation · Blood transfusion and management
INTRODUCTION
1
Postpartum hemorrhage (PPH) is an obstetric emergency and one of the leading causes of maternal mortality in both high‐ and low‐resource settings, although the absolute risk of death from PPH is significantly lower in the former group (from 0.001% to 0.01%).1 Active management of the third stage of labor is recommended to prevent this complication and is mostly based on the prophylactic administration of oxytocin at shoulder delivery.2
Recent research has investigated the efficacy of different routes of oxytocin administration in preventing PPH following vaginal delivery, reporting higher effectiveness for intravenous (IV) administration when compared with the intramuscular (IM) route.3 However, no data are available on the minimum effective dose.
According to the World Health Organization (WHO), oxytocin 10 IU (either IV or IM) is recommended following vaginal delivery for the prevention of PPH.4
This study aimed to compare the historically used regimen of 10 IU IM oxytocin with IV administration of 5 and 10 IU oxytocin to determine the most effective route of administration and the minimum effective dose to prevent PPH following vaginal birth.
MATERIALS AND METHODS
2
This retrospective observational study was conducted at the Maternity Hospital of the University of Parma, Italy, following approval from the local Ethical Committee (code protocol 153/2025/OSS/AOUPR—REMOVE24). Considering the retrospective and observational design of the study, a specific informed consent form was not collected because of the large size of the study sample, in accordance with the applicable regulations. The study was conducted on routinely collected data for clinical audit purposes, after local Ethical Committee approval, authorization and publication of the Data Protection Impact Assessment.
Study population and patient selection
2.1
We included all women who gave birth vaginally between February 1, 2022, and December 31, 2023, and received active management of the third stage of labor with oxytocin administration. Patients submitted to elective or emergency cesarean sections and those not eligible for oxytocin administration because of intolerance were not included.
During the study period, the institutional protocols for active management of the third stage of labor were periodically updated. Historically, 10 IU IM oxytocin was administered at shoulder delivery, as per the Italian national guidelines on intrapartum care.5 From October 1, 2022, the prophylactic oxytocin regimen was switched to an IV bolus of 5 IU as recommended by updated guidelines on prevention and treatment of PPH in cesarean section by the Italian Institute of Health, the Royal College of Obstetricians and Gynecologists, and the National Institute for Health and Care Excellence.5, 6, 7 Subsequently, from June 1, 2023, the dose was increased to a 10 IU IV bolus, in accordance with the American College of Obstetricians and Gynecologists guidelines for PPH prophylaxis following vaginal delivery.8
Active management of the third stage of labor, including uterotonics administration, early mother‐baby skin‐to‐skin contact (when possible), delayed cord clamping, and controlled cord traction,9 was consistently performed in all the groups. Blood loss was systematically estimated using graduated bags and gauze weighing. PPH was classified as minor, major, or massive depending on the amount of estimated blood loss (500–999, 1000–1499, and ≥1500 mL, respectively).
Clinical and epidemiologic data for each patient were collected from delivery ward records, including data regarding maternal characteristics (age, pre‐pregnancy body mass index [calculated as weight in kilograms divided by the square of height in meters], ethnicity, parity), pregnancy course (number of fetuses, gestational age at delivery, induction of labor), labor (epidural analgesia, labor augmentation, labor duration, mode of delivery, placental delivery method, postpartum blood loss, birth weight), oxytocin administration (route and dose), perineal outcomes (episiotomy and/or vaginal‐perineal lacerations).
The primary aim of the current study was to compare the incidence of PPH (blood loss >500 mL) among the three historical groups who received a different oxytocin regimen: 10 IU IM (group A), 5 IU IV (group B), and 10 IU IV (group C).
Propensity score matching was used to balance confounders between groups, ensuring a near‐randomized effect. Matching was performed with a 1:1 ratio using a caliper of 0.1.
Statistical analysis
2.2
Data were digitized into an anonymized spreadsheet using a unique numeric code. Risk factors for PPH were analyzed within each cohort using univariate analysis. Continuous variables were compared using Student t‐test or Mann–Whitney U‐test as appropriate, and categorical variables were analyzed using the χ^2^ test or Fisher exact test, as appropriate. Those variables that were statistically significant at univariate analysis were subsequently analyzed in a multivariable logistic regression model to test the impact of each factor on the risk of PPH. Post‐match univariate analysis was performed to evaluate differences in PPH incidence between the matched cohorts.
SPSS Statistics, Version 21.0 or later (IBM, Armonk, NY, USA), was used for data analysis.
RESULTS
3
During the study period, a total of 4798 women gave birth at our Maternity Unit. After excluding 742 women who underwent cesarean section, 4056 vaginal deliveries were analyzed. Of these, 203 (5.0%) were excluded because of incomplete data, and three were excluded because of contraindications to oxytocin administration (Figure 1).
Flowchart illustrating the study population and cohort distribution.
The final sample consisted of 3850 patients, split into the following groups: group A, 1245 patients administered 10 IU IM oxytocin; group B, 1291 patients administered 5 IU IV oxytocin; and group C, 1314 patients administered 10 IU IV oxytocin.
Initially, to evaluate which factors were significantly associated with the occurrence of PPH, pairwise comparisons were conducted in the overall population between patients with and without a blood loss greater than 500 mL (Table 1). Patients who experienced PPH exhibited significantly higher gestational age at delivery (39.7 ± 1.67 versus 39.5 ± 1.72 weeks; P = 0.009); longer first stage (240 versus 180 min; P < 0.001) and second stage (62 versus 31 min; P < 0.001) of labor; increased rates of multiple gestation (1.5% versus 0.5%; P < 0.001), nulliparity (63.2% versus 48.8%; P < 0.001), labor induction (45.3% versus 34.9%; P < 0.001), epidural analgesia (58.4% versus 45.3%; P < 0.001), operative vaginal delivery (10.6% versus 5.9%; P < 0.001), second‐degree or higher perineal lacerations/episiotomy (48.4% versus 27.9%; P < 0.001), and manual placental removal (13.1% versus 7.2%; P < 0.001); and higher birth weight (3464 ± 514 versus 3302 ± 487 g; P < 0.001).
TABLE 1: Univariate analysis of factors associated with postpartum hemorrhage in the total cohort. a
Binomial logistic regression identified nulliparity, severe perineal lacerations/episiotomy, manual placental removal, and birth weight as independent risk factors for PPH (Table 2).
Patients from group A (10 IU IM), group B (5 IU IV), and group C (10 IU IV) were matched in a 1:1 ratio for the variables independently associated with the occurrence of PPH after logistic regression analysis and compared.
A significantly lower incidence of PPH was found between patients receiving 5 IU IV (group B) versus 10 IU IM (group A) oxytocin (11% versus 21.3%; P < 0.001) and between those receiving 10 IU IV (group C) versus 10 IU IM (group A) oxytocin (16.8% versus 22.1%; P = 0.033) whereas no significant difference in the incidence of PPH was observed between patients receiving 5 IU IV or 10 IU IV oxytocin (10.9% versus 13.8%; P = 0.172) (Table 3).
TABLE 3: Pairwise comparisons between patients administered 10 IU IM versus 5 IU IV bolus (Group A vs. Group B), patients administered 10 IU IM versus 10 IU IV bolus (Group A vs. Group C), and patients administered 5 IU IV versus 10 IU IV bolus (Group B vs. Group C) after propensity score matching. a
Additionally, compared with group A (10 IU IM) the administration of epidural analgesia was significantly more frequent in group B (5 IU IV) (46% versus 38%; P = 0.014) and group C (10 IU IV) (50.5% versus 43.1%; P = 0.017).
No significant differences in the grade of PPH (minor, major, massive) were found among the groups.
DISCUSSION
4
This retrospective, observational study, conducted on historical cohorts of patients matched by propensity score analysis, showed that the IV administration of oxytocin as a bolus of either 5 or 10 IU after vaginal birth was more effective in reducing the incidence of PPH when compared with a 10 IU IM injection. Notably, the IV administration of 10 IU compared with 5 IU was not found to be superior in preventing a blood loss greater than 500 mL.
The efficacy of IV oxytocin administration for PPH prevention in patients undergoing cesarean section has been largely investigated, but few randomized studies on the efficacy of PPH prophylaxis following vaginal delivery have been conducted.3, 9, 10, 11 Available evidence suggests greater effectiveness for the IV route compared with the IM route, and this aligns with the findings of our study.
A meta‐analysis of seven randomized studies, including 7817 participants and comparing the efficacy of IV and IM oxytocin administration in reducing blood loss during the third stage of labor, reported that IV administration is associated with a significantly lower risk of PPH (5.6% versus 7.2%, relative risk [RR] 0.78, 95% confidence interval [CI] 0.66–0.92) and need for blood transfusions (0.6% versus 1.3%, RR 0.44, 95% CI 0.26–0.77). Furthermore, a reduction in severe maternal morbidity (0.3% versus 0.6%, RR 0.47, 95% CI 0.22–1.00) and PPH of 1000 mL or greater (1.5% versus 2.3%, RR 0.65, 95% CI 0.39–1.08) were noted, whereas adverse effects profiles were similar between the groups.3
With regard to dosages, previous research has compared the efficacy among various IV regimens following cesarean delivery; however, to our knowledge, only one study has been conducted after vaginal birth. A double‐masked randomized trial comparing three different prophylactic dosages of oxytocin (80, 40, or 10 IU in 500 mL saline infused over 1 h) including almost 1800 vaginal deliveries, found no significant differences in the incidence of PPH requiring treatment (administration of therapeutic uterotonics, blood transfusion, uterine tamponade, embolization, or surgery), which occurred in 6%–7% of the cases in each group.11
In a sub‐analysis on 2901 patients included in their meta‐analysis, Salati et al.12 found that the administration of 10 IU IV oxytocin reduced the need for supplementary drugs when compared with lower dosages (RR 0.48, 95% CI 0.33–0.68). However, most of the studies included in this review were not blinded; hence, high risk of bias was reported by the authors themselves. Furthermore, the cumulative study population given doses less than 10 IU was smaller when compared with the population given 10 IU (273 versus 2901 patients); this aspect raises concerns on the generalizability of the reported findings.12
The present study is the first study reporting non‐significant differences in the incidence of PPH when comparing a 5 IU with a 10 IU IV bolus after vaginal delivery.
After propensity score matching, a statistically significant difference in the rate of patients undergoing epidural analgesia was reported when comparing both groups B and C (5 and 10 IU IV) with group A (10 IU IM), respectively. This finding may be the result of increased access to epidural analgesia at our center during the second period of the study. However, epidural analgesia was not independently associated with PPH when investigating risk factors in the multivariable analysis; hence, it is unlikely that it might have influenced the incidence of PPH.
Results from the present study confirm that IV oxytocin administration is more effective in preventing PPH after vaginal delivery when compared with IM injection. Previous studies reported that IM administered oxytocin starts its uterotonic effect 3–7 min after administration; in contrast, IV administration has been proven to have immediate effect on uterine tone.13
On this basis, it seems appropriate to replace the IM oxytocin injection with IV administration as a standard of care to enhance PPH prevention after vaginal delivery.
Our study looked at the incidence of PPH as the principal outcome of interest, but based on our findings, dosages of IV oxytocin greater than 5 IU seem to bring no significant improvement in the rate of PPH after vaginal delivery.
This is in contrast to the most recent WHO guidelines, which for the IV route recommend the administration of 10 IU of oxytocin but do not provide clear evidence to support this.4
Establishing the minimum effective dose of IV oxytocin to prevent PPH after vaginal delivery is a key factor as the adverse effects from IV oxytocin administration are likely be dose dependent and are known to clinicians.
Among these, hypotension, arrhythmia, and other cardiovascular events have been reported to potentially occur in patients without pre‐existing cardiovascular risk factors.14, 15 A slow injection over 3 min is recommended to mitigate cardiovascular responses (e.g. reduction in blood pressure and systemic vascular resistance index, increased cardiac and left ventricular workload indices) associated with IV bolus administration.16
Our study makes a contribution to the field and suggests that in the general population 5 IU of oxytocin administered IV may be equally effective to 10 IU in preventing PPH at vaginal delivery.
Regarding the strengths of the present study, the collection of large cohorts in a relatively short time is likely to minimize the possibility that changes in local practice could have influenced the outcome. Furthermore, propensity scoring analysis and matching helped to control the effect of confounding factors on the incidence of PPH observed across the groups.
The major limitation of our study is its retrospective design. Additionally, as a result of the incompleteness of data, our analysis has not included other outcomes of clinical interest (e.g. adverse effects associated with IV oxytocin infusion compared with the IM route, post‐delivery hemoglobin levels, need for blood transfusions).
In conclusion, the present study shows that IV oxytocin is more effective than IM oxytocin in preventing the occurrence of PPH following vaginal delivery. Moreover, IV boluses of 5 or 10 IU seem to have comparable efficacies. Further well‐designed studies are needed to obtain higher quality evidence, which may lead to a more appropriate management of the third stage of labor.
AUTHOR CONTRIBUTIONS
SF, GM, and TG contributed to conceptualization; GM, AV, GMC, and BM contributed to data curation; SF and TG supervised the study; SF, GM, DF, and TG contributed to the methodology; GM and DF performed the formal analysis; all the authors contributed to the investigation; SF and AV wrote the original draft; and GM, GMC, BM, and TG performed the reviewing and editing. All authors have read and agreed to the final version of the manuscript.
CONFLICT OF INTEREST STATEMENT
The authors have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shakur H , Elbourne D , Gülmezoglu M , et al. The WOMAN Trial (World Maternal Antifibrinolytic Trial): tranexamic acid for the treatment of postpartum haemorrhage: an international randomised, double blind placebo controlled trial. Rials. 2010;11:40.10.1186/1745-6215-11-40PMC 286426220398351 · doi ↗ · pubmed ↗
- 2Begley CM , Gyte GM , Devane D , et al. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2019;2:CD 007412.25730178 10.1002/14651858.CD 007412.pub 4 · doi ↗ · pubmed ↗
- 3Oladapo OT , Okusanya BO , Abalos E , Gallos ID , Papadopoulou A . Intravenous versus intramuscular prophylactic oxytocin for the third stage of labour. Cochrane Database Syst Rev. 2020;11:CD 009332.33169839 10.1002/14651858.CD 009332.pub 4PMC 8236306 · doi ↗ · pubmed ↗
- 4World Health Organization . WHO Recommendations: Uterotonics for the Prevention of Postpartum Haemorrhage. WHO; 2018.30645062 · pubmed ↗
- 5National Guidelines System, Istituto Superiore di Sanità (ISS) . Postpartum Hemorrage: How to Prevent It, How to Treat It. 2016. Guideline 26. https://www.epicentro.iss.it/itoss/pdf/SNLG_EPP‐2016 web_corrige.pdf
- 6Royal College of Obstetricians and Gynaecologists . Prevention and Management of Postpartum Haemorrhage. Green‐Top Guideline No. 52. RCOG; 2016.10.1111/1471-0528.1417827981719 · doi ↗ · pubmed ↗
- 7National Institute for Health and Care Excellence . Intrapartum Care. NICE Clinical Guideline 235. NICE; 2023.
- 8ACOG . Postpartum hemorrhage. ACOG Pract Bull. 2017;130(4):e 168.