Bladder necrosis following uterine artery embolization for post‐abortion uterine arteriovenous malformation: A rare complication
Mira Zlotnik, Marcos de Lorenzo Messina, Eduardo Zlotnik, José Maria Soares Júnior, Edmund Chada Baracat

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
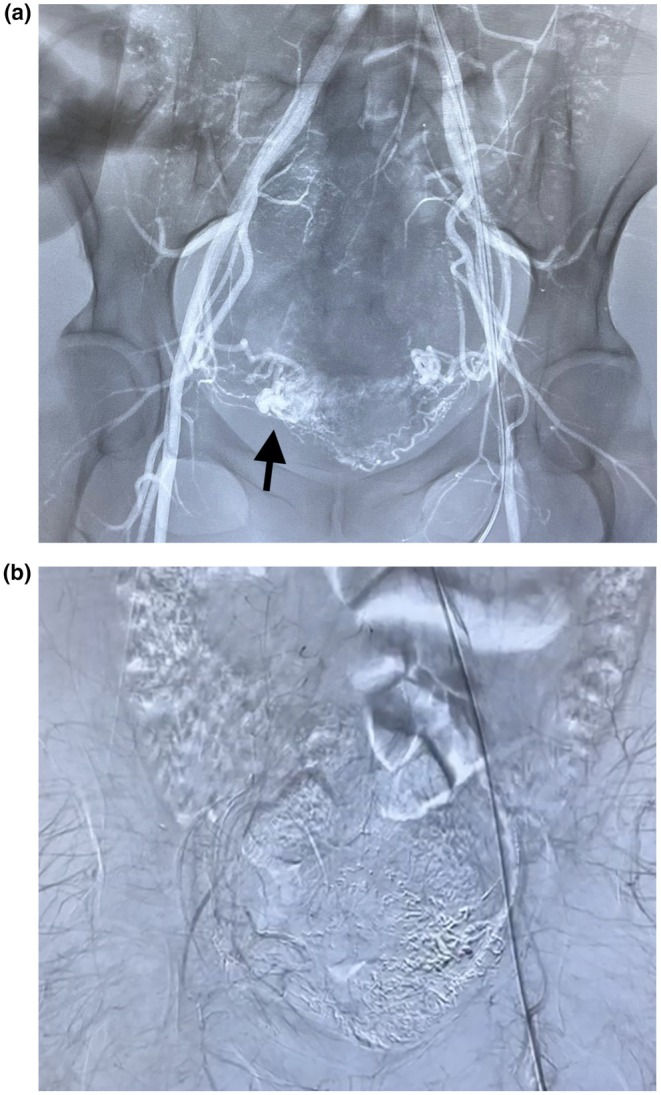 Figure 1
Figure 1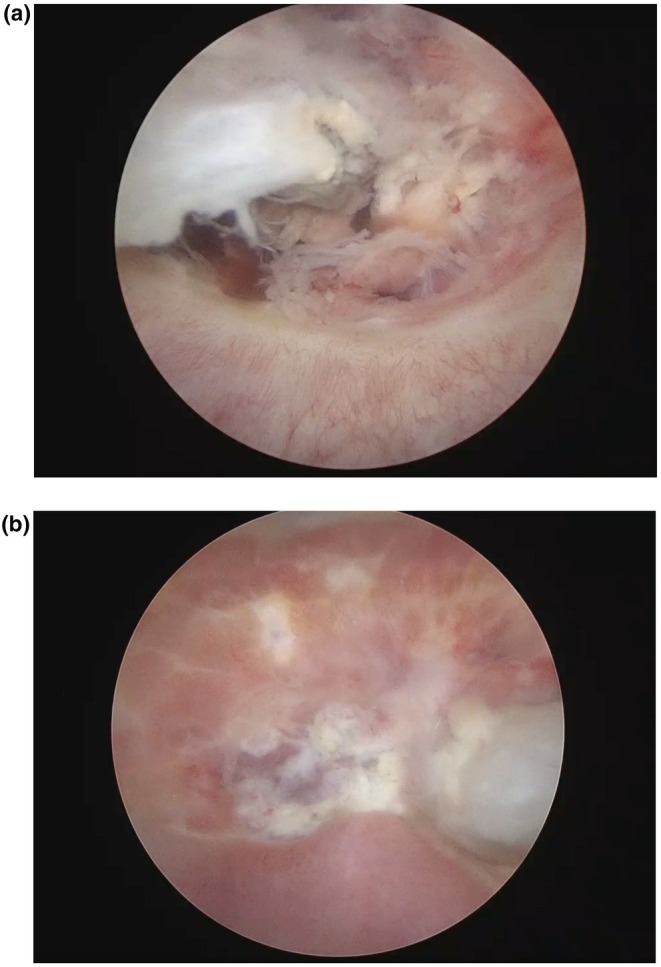 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and fetal healthcare · Ectopic Pregnancy Diagnosis and Management · Reproductive Health and Contraception
Uterine arteriovenous malformations are uncommon but potentially serious causes of abnormal uterine bleeding, often acquired after procedures such as curettage, manual vacuum aspiration (MVA), or uterine surgery.1 Uterine artery embolization (UAE) is an effective, minimally invasive treatment, offering high success rates while preserving fertility.2 However, complications such as uterine necrosis have been reported, while bladder involvement remains extremely rare.3, 4
We report the case of a 35‐year‐old woman (G2P1A1) with reproductive desire who underwent MVA for abortion. She developed profuse vaginal bleeding and anemia. Two months after the MVA, she was diagnosed with a uterine arteriovenous malformation. Pelvic angiography confirmed uterine arteriovenous fistula, with nidus on the right (Figure 1a). Catheterization of the right uterine artery revealed a patent, tortuous vessel with parenchymal blush. Superselective embolization was performed using ethylene vinyl alcohol copolymer. Persistent perfusion via the right cervical artery required additional embolization using the same agent. The left uterine artery was similarly involved and was embolized using Histoacryl diluted in Lipiodol after superselective catheterization (Figure 1b).
One month after embolization she returned to the hospital with abdominal pain and hematuria. Magnetic resonance imaging raised the hypothesis of fistula as it revealed a 1.3‐cm defect in the posterior bladder wall communicating with the embolized uterine region. Cystoscopy revealed a well‐demarcated 4‐cm necrotic area with central ulceration, consistent with bladder wall necrosis (Figure 2). Instillation of methylene blue with a vaginal tampon was negative for vesicouterine fistula. It was managed conservatively with a Foley catheter for 3 weeks. Follow‐up cystoscopy showed healing mucosa. Hormonal blockade with a gonadotropin‐releasing hormone analog was initiated for persistent light bleeding, which was effective, and the patient remains in amenorrhea. Follow‐up magnetic resonance imaging demonstrated no abnormalities in the uterus or bladder.
Bladder necrosis following UAE is exceptionally rare, especially without uterine involvement. Conservative management proved successful in this case, avoiding surgical reconstruction while preserving fertility potential. Early diagnosis is important for successful preservation of organs by adopting conservative management when the patient's hemodynamic status is stable.3, 4 This case emphasizes the importance of recognizing rare complications of UAE and demonstrates that conservative management can be successful. Written informed consent was obtained from the patient for publication of this case report in accordance with institutional ethics guidelines.
AUTHOR CONTRIBUTIONS
Mira Zlotnik: Conceptualization; investigation; writing—original draft; writing—review and editing. Marcos de Lorenzo Messina and Eduardo Zlotnik: Investigation; data analysis; writing—review and editing. José Maria Soares Júnior and Edmund Chada Baracat: Supervision; writing—review and editing; final approval.
FUNDING INFORMATION
None.
CONFLICT OF INTEREST STATEMENT
The authors have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Szpera‐Goździewicz A , Woźniak S , Węglarz B , Gaca M , Wilczyński J . Uterine arteriovenous malformation—diagnosis and management. Ginekol Pol. 2018;89(5):276‐279. doi:10.5603/GP.a 2018.0047 30084480 · doi ↗ · pubmed ↗
- 2Barral PA , Saeed‐Kilani M , Tradi F , et al. Transcatheter arterial embolization with ethylene vinyl alcohol copolymer (Onyx) for the treatment of hemorrhage due to uterine arteriovenous malformations. Diagn Interv Imaging. 2017;98:415‐421.27776896 10.1016/j.diii.2016.09.003 · doi ↗ · pubmed ↗
- 3Poujade O , Ceccaldi PF , Davitian C , Hudry D , Fernandez H . Uterine necrosis after embolization for postpartum hemorrhage: review of the literature. Gynecol Obstet Fertil. 2013;41(10):588‐592. doi:10.1016/j.gyobfe.2013.08.006 24094595 · doi ↗
- 4Huang LY , Cheng YF , Huang CC , Chang SY , Kung FT . Incomplete vaginal expulsion of pyoadenomyoma with sepsis and focal bladder necrosis after uterine artery embolization for symptomatic adenomyosis: case report. Hum Reprod. 2003;18(1):167‐171. doi:10.1093/humrep/deg 035 12525461 · doi ↗ · pubmed ↗