Additional interventions for enhancing the quality-of-life of older adults using hearing aids: a systematic review and narrative synthesis
Minji Kang, Yunji Han, Hyejoon Kim

TL;DR
This review explores how adding interventions to hearing aids can improve the quality of life for older adults, focusing on psychological and autonomy-related benefits.
Contribution
The study systematically evaluates the added value of supplementary interventions to hearing aids for quality-of-life outcomes in older adults.
Findings
Individual at-home training improved sensory abilities, self-efficacy, and autonomy.
Group-based auditory rehabilitation enhanced communication strategies and positive emotional outcomes.
Empowerment strategies showed favorable psychological effects, while telehealth had limited impact.
Abstract
Hearing loss in older adults substantially affects quality of life. Although hearing aids improve hearing, their effects vary. Combining hearing aids with additional interventions may offer added benefits, yet it remains unclear which quality-of-life domains benefit most. This systematic review examined the effects of hearing aids plus supplementary interventions, compared with hearing aids alone, on quality-of-life outcomes. Randomized controlled trials (1996–2024) were identified from seven databases. Eligible studies included adults aged ≥ 65 years and compared hearing aids combined with additional interventions with hearing aids alone. Outcomes were categorized into physical, psychological, and older-adult-specific domains using the WHOQOL-100 and WHOQOL-OLD frameworks. Risk of bias was assessed using RoB 2, and certainty of evidence using GRADE. A narrative synthesis was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
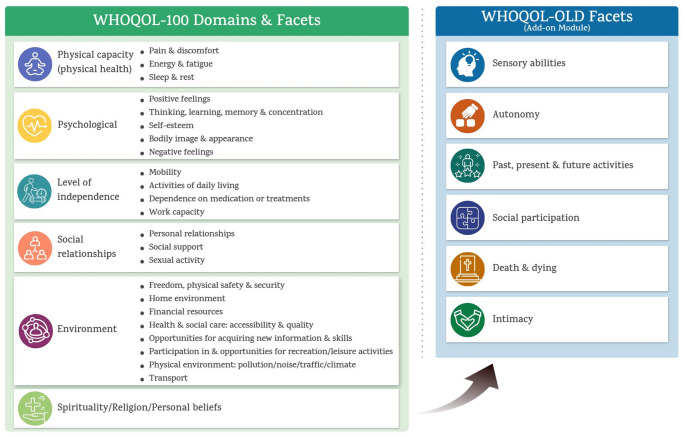 Figure 1
Figure 1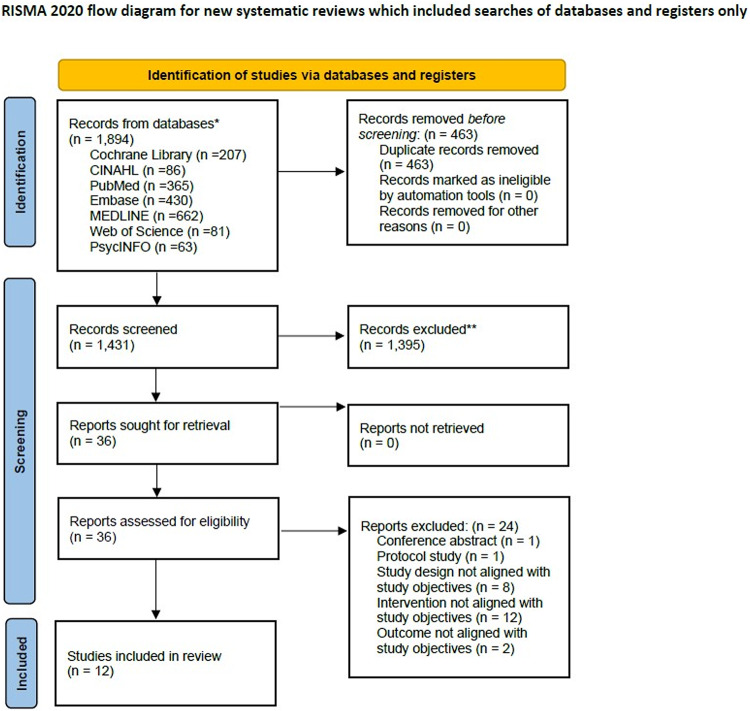 Figure 2
Figure 2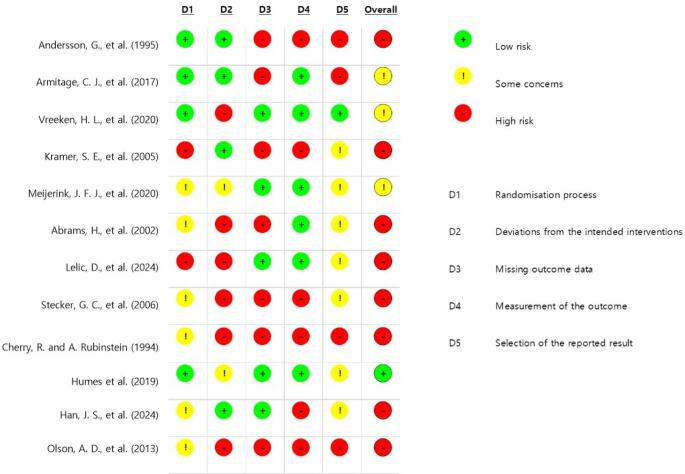 Figure 3
Figure 3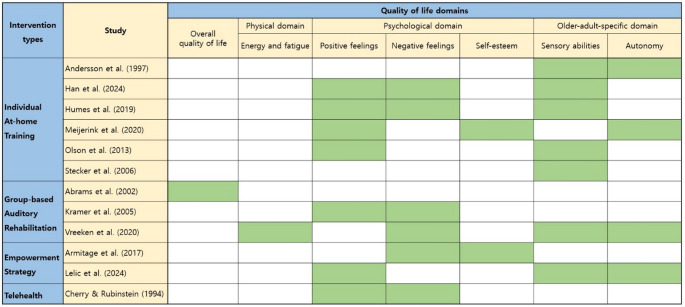 Figure 4
Figure 4- —Seoul National University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHearing Loss and Rehabilitation · Hearing Impairment and Communication · Telemedicine and Telehealth Implementation
Plain English summary
Hearing loss is common among adults aged ≥ 65 and can substantially diminish quality of life. Many individuals use hearing aids, but their benefit varies and often remains limited. This situation creates a need to understand whether adding supportive interventions to hearing aid use can provide broader improvements in daily functioning and well-being. The key issue addressed in this manuscript is the lack of clear evidence on which aspects of quality of life respond most favorably to combined interventions compared with hearing aids alone. This study aimed to systematically review randomized controlled trials that evaluated hearing aid use combined with supplemental interventions (e.g., auditory training, group-based rehabilitation, empowerment programs, or telehealth), compared with hearing aid use alone. The review found that combined approaches may improve psychological well-being, self-efficacy, and autonomy for some older adults. However, the overall certainty of evidence was low due to variability in study design, intervention content, and outcome measures. These results suggest that multifaceted rehabilitation may offer added value, while highlighting the need for more rigorous and standardized research.
Introduction
Over 42% of individuals aged 60 years and above globally experience hearing impairment, with age-related hearing loss being the third leading cause of disability [1]. This condition often leads to communication challenges, isolation, frustration, and depressive symptoms, significantly affecting overall quality of life [2–4]. Consequently, it impacts both emotional well-being and participation in social, educational, and professional settings. Research has also indicated that older adults with hearing loss are at increased risk of developing cognitive decline compared with those without hearing loss [5]. Since hearing loss profoundly affects multiple aspects of life in older adults, it is essential to examine the quality of life of those who experience hearing loss throughout their lives.
Quality of life is a complex concept that includes physical health, mental well-being, autonomy, social relationships, and interactions with the environment [6]. The World Health Organization (WHO) defines quality of life as "individuals' perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns” [6]. In the WHOQOL framework, quality of life is conceptualized as a multidimensional construct encompassing physical capacity, psychological, level of independence, social relationships, environment, spirituality/religion/personal beliefs. In this context, examining quality of life in older adults with hearing loss could provide healthcare professionals with a more holistic perspective, encouraging them to become more attuned to patients' needs and ultimately fostering the development of interventions that consider the impact on patients' overall well-being.
Hearing aids have been the most common intervention for older adults with hearing loss [7]. A robust body of evidence from systematic reviews indicates that hearing aids improve quality of life [7, 8], but their adoption rate worldwide remains low at approximately 11% [9]. To this end, several nonaudiological factors, such as group instructions and encouragement from others, were found to influence the acceleration of the use of hearing devices, along with audiological factors [10]. Evidence also suggests that hearing aids alone may not be enough to fulfill what people with hearing loss want, as amplification often fails to optimize communication in daily life [11].
Many studies have suggested that combining hearing aids with additional interventions—such as inducing self-affirmation, providing counseling, and educating communication strategies—provides greater benefits for populations with hearing loss and enhances their overall quality of life [12–14]. While some studies have examined the quality of life of older adults with hearing aids, they have focused primarily on health-related quality of life [15] or assessed a single additional intervention without comparison [16]. No studies have examined and synthesized results on which aspects of quality of life benefit more from combining hearing aids with additional interventions than from using hearing aids alone.
Given the lack of comprehensive comparative analyses, this systematic review seeks to synthesize the results and compare the effects of hearing aids combined with additional interventions with those of hearing aids alone on improving the quality of life of older adults with hearing loss.
Methods
This review followed the PRISMA 2020 guidelines for systematic reviews [17]. A protocol was registered with PROSPERO (No. 605082) prior to the review. Although the study was conducted as a systematic review, heterogeneity in interventions and outcomes precluded meta-analysis, and findings were synthesized narratively. During title revision, the PROSPERO record was withdrawn after being identified by the platform as a scoping review, which is not eligible for registration.
Eligibility criteria
We included studies on adults aged ≥ 65 with hearing loss that directly compared the effects of hearing aids combined with an additional structured intervention to hearing aids alone. Structured interventions were defined as behavioral, educational, psychosocial, or rehabilitative programs specifically designed to supplement hearing aid use and intended to improve quality of life or its related domains. The primary outcomes of interest were quality of life or its related domains, as conceptualized by the WHOQOL-100 and WHOQOL-OLD frameworks in Fig. 1 [6, 18], which provide a multidimensional approach suitable for evaluating quality of life in older adults with hearing loss. The WHOQOL-100 conceptualizes quality of life across six domains: physical capacity, psychological, level of independence, social relationships, environment, spirituality/religion/personal beliefs [6]. The WHOQOL-OLD framework is an age-specific add-on module to the WHOQOL framework, focuses on six age-relevant facets: sensory abilities, autonomy, past-present-future activities, social participation, death and dying, and intimacy [18]. These domains and facets were considered directly relevant to the present review, as hearing loss and hearing-related interventions may affect multiple aspects of later-life functioning, particularly sensory abilities, autonomy, psychological well-being, and social participation.Fig. 1. Domains and facets of the WHOQOL-100 and WHOQOL-OLD frameworks
Studies were excluded if they:
- did not include hearing aid users as the population of interest,
- lacked a control group using hearing aids alone,
- assessed outcomes not conceptually aligned with the WHOQOL-100 or WHOQOL-OLD domains,
- included participants younger than 65 years without subgroup analysis, or
- were feasibility or pilot studies not designed to evaluate intervention effectiveness.
Only randomized controlled trials (RCTs) were included, as we aimed to focus on the highest-quality evidence available to assess the effectiveness of interventions. Studies published in English from 1996 to 2024 were included, as 1996 marked the first commercial availability of digital hearing aids [19, 20]. A summary of the eligibility criteria is shown in Table 1.Table 1. Study eligibility criteriaInclusion CriteriaExclusion CriteriaPopulationOlder adults with hearing lossParticipants over 65 years or with a mean age above 65New and Experienced HA usersParticipants under 65 years oldParticipants with other otologic disordersInterventionHAs with additional interventionsStudies involving forms of amplification other than HAsComparisonHAs aloneStudies focusing on medication or surgical interventions and HA-fitting methodsOutcomeOutcomes measured using quality of life instruments, along with outcomes that could be considered related to quality of life based on the domains of the WHOQOL-100 and WHOQOL-OLDStudy designOnly RCTNon-qualitative studiesForm of publicationStudies conducted between 1996 and 2024Studies written in EnglishConference abstractHA; hearing aid, RCT; randomized controlled trial
Search and study selection
An extensive literature search was performed through seven databases, including the Cochrane Library, CINAHL, PubMed, Embase, MEDLINE, Web of Science, and PsycINFO, which use terms related to older adults, hearing loss, hearing aids, interventions, and randomized controlled trials, as outlined in Table 2. Database-specific thesauri were applied, and the term intervention was included to capture a broad range of approaches. The search strategy was refined over two weeks with input from a medical librarian and finalized on October 6, 2024. Additional searches were conducted in the International Clinical Trials Registry Platform (ICTRP), ClinicalTrials.gov, PROSPERO, and grey literature through the Web of Science and PsycINFO. Three review authors independently screened the titles and abstracts via Rayyan, a widely used screening tool [21]. Full-text articles were reviewed for eligibility, with disagreements resolved by discussion. Inter-rater agreement among the three reviewers was substantial (Fleiss’ κ = 0.681). The rationale for study exclusion was documented at the full-text level and summarized in Supplementary Material S1.Table 2. Outline of the search termsPopulationInterventionComparison Study designABCDEolder adultsagedelderlyseniorpensionretiregeriatrichearing losshearing impairmenthard of hearinghearing defectauditory defecthearing aidauditory applianceauditory prosthesishearing devicehearing apparatuslistening aidinterventionprogrameducattrainrehabilitatsupportcommunicatcounselimprovenhanc*randomized controlled trialThe keywords within each category A through E were grouped using OR, and categories A through E were combined using AND. * Asterisks indicate search term truncation
Data extraction
Three review authors manually extracted data using a standardized data extraction form. All data items were specified and agreed upon before data extraction to ensure consistency across reviewers. Disagreements were resolved through discussion, and study authors were contacted when clarification was necessary. The extracted data included study characteristics (publication year, authors, country, study aims, methods, and trial design), participant characteristics (age, gender, and duration of hearing aid use), intervention characteristics (type and content), follow-up period, outcome measures, quality-of-life-related outcomes, key findings, and funding sources.
Outcomes and prioritization
This review examines how hearing aids combined with additional interventions improve the quality of life of older adults with hearing loss. We focused on outcomes related to quality of life on the basis of the WHOQOL-100 and WHOQOL-OLD domains, as shown in Table 3.Table 3. Outcome domains and facets of quality of life (Power et al., 2005; WHO, 1998)DomainFacetDescriptionPhysical domainEnergy and fatigueAssesses a person's energy and stamina for activities, ranging from experiencing fatigue to having adequate energy levelsPsychological domainPositive feelingsConsiders an individual's perspective of positive emotions as an essential componentNegative feelingsAddresses the extent to which individuals experience negative emotions, including depression, anxiety, and a reduced sense of pleasure in lifeSelf-esteemExamines how individuals view themselves, spanning from positive to negative feelings, including aspects like self-efficacy, self-satisfaction, and controlOlder-adult-specific domainSensory abilitiesIdentifies the impact of sensory impairments on daily life, participation in activities, and the ability to interact with othersAutonomyEvaluates whether individuals can make decisions, feel a sense of control, do what they want, and whether their freedom is respected by those around them
Quality appraisal
Study quality was assessed using the Revised Cochrane Risk of Bias Tool (RoB 2). Three authors independently evaluated risk of bias using the Excel-based RoB 2.0 tool provided by the Cochrane risk-of-bias initiative, with disagreements resolved by consensus. Outcome reporting bias was evaluated by comparing study protocols with published results. Studies were categorized as low risk, some concerns, or high risk of bias based on algorithm-guided judgments from signalling questions rather than numerical scores. A study was classified as low risk of bias when all domains were judged as low risk. It was some concerns when at least one domain raised some concerns but no domain was judged as high risk, and high risk of bias when at least one domain was judged as high risk or when multiple domains with some concerns substantially lowered confidence in the results [22]. The certainty of evidence for the included studies was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) framework. Evidence from randomized controlled trials was initially rated as high and downgraded, when appropriate, based on risk of bias, inconsistency, indirectness, imprecision, and publication bias, resulting in overall certainty ratings of high, moderate, low, or very low [23].
Data synthesis
A wide variety of tools have been used to measure quality-of-life related outcomes. We classified and integrated these outcomes on the basis of the WHOQOL-100 and WHOQOL-OLD domains and facets. The reviewers carefully examined the individual items of each tool and classified them according to the domain of quality of life to which they were most closely aligned, based on conceptual relevance. Items were assigned to the domain that best represented their primary construct. Facets that primarily assessed functional status rather than quality-of-life aspects, or that were not explicitly measured by the instruments, were excluded from the final classification. Detailed domain and facet classifications are provided in Supplementary Material S2. Owing to the variety of measurement tools and statistical methods used, we reached out to ten authors for raw data, but only two responded. Due to the substantial heterogeneity among studies, primarily arising from differences in intervention content, duration, and outcome measures, a qualitative narrative synthesis was conducted [24]. Interventions were inductively categorized after study inclusion to facilitate synthesis. Two reviewers independently coded intervention characteristics using thematic analysis, with discrepancies resolved through consensus with a third reviewer. Results are summarized by intervention category in Table 4.Table 4. Summary of included studiesNoYearAuthorCountrySample sizeExperimental GroupControl GroupIntervention defined12002Abrams, H., et alUSA10553Age in years (Mean ± SD): 74.5 ± 6.9Gender (n, M/F): 31/22PTA (dB HL, Mean ± SD): 35.1 ± 11.8 (right ear) and 35.7 ± 11.5 (left ear)52Age in years (Mean ± SD): 73.0 ± 7.6Gender (n, M/F): 36/16PTA (dB HL, Mean ± SD): 34.5 ± 12.3 (right ear) and 32.1 ± 12.0 (left year)Group-Based Auditory Rehabilitation21997Andersson, G., et alSweden199Age in years(Mean ± SD): N/AGender (n, M/F): 5/410Age in years(Mean ± SD): N/AGender (n, M/F): 6/4Individual at-Home Training32017Armitage, C. J., et alUK(England)5025Age in years(Mean ± SD): 71.60 ± 12.15Gender (n, M/F): N/A25Age in years(Mean ± SD): 67.44 ± 13.51Gender (n, M/F): N/AEmpowerment Strategy41994Cherry, R. and A. RubinsteinUSA3317Age in years(Mean ± SD): 76.6 ± 8.1Gender (n, M/F): N/APTA (dB HL, Mean ± SD): 43.0 ± 14.8HA use (n, New/Previous ): 17/1316Age in years(Mean ± SD): 74.1 ± 8.5Gender (n, M/F): N/APTA (dB HL, Mean ± SD): 38.0 ± 13.3HA use (n, New/Previous ): 16/14Telehealth52024Han, J. S., et alKorea3919Age in years(Mean ± SD): 70.5 ± 6.9Gender (n, M/F): 8 / 12HL duration in months (Mean ± SD): 107.9 ± 83.3HA use duration in months (Mean ± SD): 56.1 ± 72.220Age in years(Mean ± SD): 69.5 ± 13.8Gender (n, M/F): 8 / 13HL duration in months (Mean ± SD): 98.3 ± 91.3HA use duration in months (Mean ± SD): 53.0 ± 50.7Individualat-Home Training62019Humes et alUSA4313Age in years(Mean ± SD): 71.9 ± 6.1Gender (n,M/F): 9/4PTA (dB HL,Mean ± SD):36.0 ± 12.3(right ear)34.7 ± 12.1(left ear)Active Control (AC) = 15Passive Control (PC) = 15 < AC > Age in years(Mean ± SD): 71.3 ± 7.5Gender (n, M/F): 11/4PTA (dB HL, Mean ± SD): 29.1 ± 15.2(right ear)31.1 ± 15.8 (left ear) < PC > Age in years(Mean ± SD): 72.0 ± 7.1Gender (n, M/F): 11/4PTA (dB HL, Mean ± SD):28.0 ± 16.8 (right ear)31.1 ± 16.0 (left ear)Individual at-Home Training72005Kramer, S. E., et alNetherland4824(Hearing Impaired, HI) + 24(Significant Others) < HI > Age in years(Mean ± SD): 69 ± 7.7Gender (n, M/F): 16/8PTA (dB HL, Mean ± SD): 53.7 ± 13.3HA use (n, first/experienced): 12/1224(Hearing Impaired, HI) + 22(Significant Others) < HI > Age in years(Mean ± SD): 71 ± 8.5Gender (n, M/F): 12/12PTA (dB HL, Mean ± SD): 56.3 ± 15.7HA use (n, first/experienced): 9/15Group-Based Auditory Rehabilitation82024Lelic, D., et alDenmark2111Age in years: 68 ± 7Gender (n, M/F): 8/3HA experience in years (Median [Range]): 13 [1-37]10Age in years: 64 ± 8Gender (n, M/F): 7/3HA experience in years (Median [Range]): 12.5 [1-53]Empowerment Strategy92020Meijerink, J. F. J., et alNetherland343180Age in years (Mean ± SD): 68.1 ± 8.4Gender (n, M/F): 108/72163Age in years (Mean ± SD): 68.2 ± 8.7Gender (n, M/F): 98/65Individual at-Home Training102013Olson, A. D., et alUSA298 (New HA users + Training)Age in years (Mean ± SD): 66 ± 9.6Gender (n, M/F): 4/4HL duration: 10.2 (SD = 10.3)14 (Experienced HA users + Training)Age in years (Mean ± SD): 68 ± 6.9Gender (n, M/F): 4/10HL duration: 16.4 (SD = 11.8)7 (No training, New HA use only)Age in years (Mean ± SD): 66 ± 9.3Gender (n, M/F): 6/1HL duration: 11.4 (SD = 10.2)Individualat-Home Training112006Stecker, G. C., et alUSA31Experiment 1(New HA users)12Age in years (Mean [Range]): 69 [50–80]Gender (n, M/F): N/AExperiment 2 (Experienced HA users)8Age in years (Mean [Range]): 67.7 [61–75]Gender (n, M/F): N/AHA experience in months (Mean [Range]): 16 [10–21]Experiment 1(New HA users)11Age in years (Mean [Range]): N/AGender (n, M/F): N/AExperiment 2 (Experienced HA users)NoneIndividualat-Home Training122020Vreeken, H. L., et alNetherlands and Belgium13164(Participants) + 57(Communication Partners) < Participants > Age in years(Mean ± SD [Range]): 81.3 ± 9.9 [56–97]Gender (n, M/F): 37/27DSL duration in years (Median [IQR]): 4.0 [2–7]67(Participants) + 53(Communication Partners) < Participants > Age in years(Mean ± SD [Range]): 81.9 ± 10.0 [53–99]Gender (n, M/F): 26/41DSL duration in years (Median [IQR]): 5.5 [2.75–10]Group-Based Auditory RehabilitationNoIntervention descriptionFacet of OutcomeOutcome measureTime points (time frame)Major findingsFundingRob2 Consensus1A group-based audiologic rehabilitation program approach to improving communication for the hard of hearing, covering auditory processes, strategies for challenging listening environments, anticipatory and repair techniques, and resources like assistive technology and community support for groupOverall quality of lifeSF-36 V4 weeks (Immediate): Post-intervention assessmentGreater improvement in mental health (MCS score) (p = 0.01) compared to HA aloneN/AHigh2Received coping skills training at home to enhance communication strategies and manage hearing-related difficulties1. Autonomy2. Sensory abilities1. CPHI, HCA2. VAS1wk (Immediate)Improved coping behaviors and reduced hearing problems in elderly individuals with minimal therapist involvement, better stress management and communication skills, but no significant changes in daily HA useSwedish Council & Sasakawa FundHigh3Self-affirmation was induced at baseline using an established manipulation that was embedded at the end of the research questionnaires1. Negative feelings2. Self-esteem1. Lasher and Faulkender’s anxiety about ageing scale2. Ad hoc research tool10 wksReduction in anxiety levels and improved acceptance of aging (p < 0.01), compared to the control group. HA use was higher in the intervention group but not statistically significantManchester NHS TrustSome concerns4Periodic clinician-initiated telephone contact whether HA users were experiencing any problems (e.g., feedback, discomfort, handling of aid, etc.). Problems were addressed through trouble-shooting (e.g., dead batteries) and counseling over the phone, or if indicated, subjects were scheduled for a clinic appointment1. Positive feelings2. Negative feelings1. Ad hoc research tool2. Ad hoc research tool, HHIE6wks (Immediate): Follow-up at 6wks post fitting9wks (Intermediate): Follow-up at 9wks post fitting12wks (Intermediate): Follow-up at 12wks post fitting4mths (Intermediate): Final interview at 4mthsThe intervention group had more frequent identification and resolution of hearing aid-related problems. But no statistically significant in terms of satisfaction or perceived benefitCUNY GrantHigh5Chat based mobile training contains dual auditory and word training program. Encouraged to use CMAT daily for 8 weeks (2 months). One CMAT session consisted of 20 questions, took about 5 to 10 min, and was repeated 3 times a day (30 min a day)1. Positive feelings2. Negative feelings3. Sensory abilities1. K-IOI-HA2. APHAB, K-HHIE3. Ling Six Sound test, VCIT, Monosyllable, and bi-syllable open-set tests, K-CID1mth (Immediate)2mths (Intermediate)Significant improvements in word and sentence perception (p = 0.04, p = 0.03, respectively) compared to HA aloneKorea SME MinistryHigh6Self-administered intervention at home,frequent-word auditory training. Received words, phrases, and sentences in backgrounds of noise and trial-to-trial feedback on their identification performanceInstructions were given to complete 3 sessions per week, for a total of 15 at-home sessions1. Positive feelings2. Negative feelings3. Sensory abilities1. HASS2. HHIE3. CST, CID, Trained frequent-word speech materials, PHAP, ANL5 ~ 6wks (Immediate)10 ~ 11wks (Intermediate)15 ~ 16wks (Intermediate)21 ~ 22wks (Intermediate)Participants who engaged in frequent auditory training showed greater improvements in word recognition(p < 0.05) in noise compared to HA aloneNIH NIDCD GrantLow7Training in communication strategies with significant others, speechreading, information on how to use hearing aids, and details on additional technical devicesA self-administered intervention comprised of 5 videotapes and an instruction bookletEach video depicts common daily challenges faced by the elderly, demonstrating communication strategies to improve interactions and raise awareness about hearing loss and its impact1. Positive feelings2. Negative feelings1. IOI-HA, IOI-AI2. Items derived from HHDIImmediately after the program (Immediate)6 mths (Intermediate)Increased awareness of the benefits of speechreading and improved interaction with their significant others (p < 0.05). The control group experienced a decrease in quality of life, whereas the intervention group showed improvements at the 6-month follow-up. No significant group differences were observed regarding emotional response(p > 0.05)ZonMw & Sluyterman FoundationHigh8Asked to report their positive listening experiences via an app (for 3 weeks)1. Positive feelings2. Sensory abilities3. Autonomy1. Ad hoc research tool, IOI-HA, HEARLI-Q, EMA2. COSI for "final ability"3. COSI for "degree of change"1wk (Immediate)4wks (Immediate)Increased satisfaction and perceived benefit from hearing aids (COSI)(p < 0.05) compared to HA aloneN/AHigh9A practical support booklet and online materials were delivered via email throughout their 6-month HA rehabilitation trajectoryThe online materials included 3 instruction videos on HA handling, 5 videos on communication strategies, and 3 testimonial videos1. Autonomy2. Positive feelings3. Self-esteem4. Negative feelings1. CPHI2. IOI-HA, IOI-AI3. MARS-HA, URICA-HL4. AIADH6mths (Intermediate)12mths Intermediate)Significantly greater self-efficacy for advanced HA handling (p = 0.04) and hearing aid satisfaction(p = 0.006) compared to HA aloneAudioNova & VU Medical CenterSome Concerns10Auditory training (AT) at home using the LACE DVD20 lessons from the LACE DVD program over 4 weeks1. Sensory abilities2. Positive feelings1. QuickSIN, Compressed Speech Test, SSI, SSQ2. IOI-HA, IOI-AI2wks (Intermediate): Midpoint assessment after 2wks of training4wks (Intermediate): Post-training assessmentImprovements in speech recognition(p < 0.05) compared to HA aloneUniversity of KentuckyHigh118 weeks of at-home syllable identification trainingSensory abilitiesNST1wk (Baseline): Initial assessment2wks (Intermediate): Mid-training assessment4wks (Intermediate): Post-training assessment16wks (Long-term): Retention test after trainingSignificant improvement in syllable identification and phoneme recognition(p < 0.001) compared to HA aloneVA Research GrantHigh12Participants and their communication partners received occupational therapy ‘Dual Sensory Loss Protocol’ for effective communication strategies as a groupThe protocol consisted of: (1) optimal use of HAs; (2) use of assistive devices and adaptations to the living environment; and (3) coping with DSL and use of effective communication strategies1. Energy and fatigue2. Negative feelings3. Autonomy1. FAS2. CES-D, De Jong Gierveld Loneliness Scale3. CPHI3mths (Intermediate)Significant effect (effect size SMD = 0.60, 95% CI: 0.25–0.95) in the use of verbal communication strategies (CPHI), but not significant after adjusting confounders. No significant overall improvements in HA useZonMw, Oogfonds, CapitaSome ConcernsAIADH, Amsterdam Inventory for Auditory Disability and Handicap; ANL, Acceptable Noise Level; APHAB, Abbreviated Profile of Hearing Aid Benefit; CES-D, Center for Epidemiological Studies – Depression Scale; CID, Central Institute for the Deaf sentence materials; CMAT, Chat-based Mobile Auditory Training; COSI, Client-Oriented Scale of Improvement; CPHI, Communication Profile for the Hearing Impaired; CST, Connected Speech Test; dB HL, decibels hearing level; DSL, Dual Sensory Loss; EMA, Ecological Momentary Assessment; FAS, Fatigue Assessment Scale; HA, Hearing Aid; HASS, Hearing Aid Satisfaction Survey; HCA, Hearing Coping Assessment; HEARLI-Q, Hearing-Related Lifestyle Questionnaire; HHDI, Hearing Handicap and Disability Inventory; HHIE, Hearing Handicap Inventory for the Elderly; HL, Hearing Loss; IOI-AI, International Outcome Inventory for Alternative Interventions; IOI-HA, International Outcome Inventory for Hearing Aids; IQR, Interquartile Range; K-CID, Korean version of Central Institute for the Deaf test; K-HHIE, Korean version of the Hearing Handicap Inventory for the Elderly; K-IOI-HA, Korean versions of the International Outcome Inventory for Hearing Aids; LACE, Listening And Communication Enhancement; MARS-HA, Measure of Audiologic Rehabilitation Self-Efficacy for Hearing Aids; NST, Nonsense Syllable Test; OT, Occupational Therapists; PHAP, Perception of Hearing Aid Performance; PTA, Pure Tone Average calculated for 'the better ear' over the frequencies of 0.5 ~ 4 kHz; QuickSIN, Quick Speech in Noise; SD, Standard Deviation; SF-36 V, 36-Item Short-Form Health Survey modified for the Veteran population; SSI, Synthetic Sentence Identification; SSQ, Speech, Spatial and Qualities of Hearing Scale; URICA-HL, University of Rhode Island Change Assessment adapted for Hearing Loss; VAS, Visual Analogue Scales; VCIT, Vowel and Consonant Imitation Test
Results
Study selection
We found a total of 1,894 records from seven databases, and after removing 463 duplicates, 1,431 records remained. After screening the titles and abstracts, 1,395 articles were excluded. Subsequently, 36 studies were fully screened by reviewing the full texts. Of these, 24 articles were excluded because they were nonrandomized controlled trials, were study protocol articles, lacked hearing aid users in the control group, intervention not aligned with study objectives, or reported outcomes not aligned with study objectives. Finally, 12 studies that met the study inclusion criteria were selected for this review. Our research selection process is summarized in Fig. 2.Fig. 2PRISMA 2020 flow diagram
Quality assessment
The results of the evaluation are shown in Fig. 3. The quality of the studies was graded as “high risk” across the other domains, except for the randomization process domain. After the results from all five RoB 2 domains (bias arising from the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result) were evaluated, eight studies were classified as “high risk" in quality, three as "some concerns," and one as "low risk." No studies were excluded on the basis of these quality assessments to ensure the comprehensive inclusion of all available evidence, thereby strengthening the overall synthesis.Fig. 3. Quality assessment results for individual studies for each and overall domain
Study characteristics
The published dates of the studies ranged from 1994 to 2024 in 7 countries, with most of the studies from Europe (n = 6); the Netherlands (n = 2), Denmark (n = 1), Belgium (n = 1), Sweden (n = 1), and the United Kingdom (n = 1). Additionally, five studies were from North America (United States, n = 5), and one study was from Asia (Korea, n = 1). All studies were randomized controlled trials. The sample sizes in all studies varied from 19 to 343 study participants, with a total of 892 participants across all included studies. The participants were older adults, with the experimental group aged between 64 and 81.3 years and the control group aged between 66 and 81.9 years. Both participants predominantly had bilateral sensorineural hearing loss ranging from mild-to-moderate across the studies. The severity of hearing impairment is typically measured by pure-tone audiometry, with better-ear average thresholds ranging from 30 to 60 dB HL. Additionally, other baseline testing measures, such as speech-in-noise capabilities [25–27], the National Hearing Test (NHT), the Connected Speech Test (CST), and the Nonsense Syllable Test (NST), have also been utilized in several studies [11, 26, 27]. Table 4 presents the detailed information.
All participants in the control group were hearing aid users. Several studies ensured the balanced inclusion of both first-time hearing aid users and those who have already used hearing aids. These studies evenly distributed participants across interventions involving both new and long-term users [25, 26, 28, 29]. Many studies focused on participants who have already used hearing aids [11–13, 27, 30]. In contrast, some research has specifically targeted new hearing aid users to address their acclimatization challenges [14, 31, 32].
Three studies divided participants into three groups [25–27]: (1) one experimental group and two control groups (passive and active) [26]; (2) one control group consisting of new hearing aid users who did not receive the additional intervention, and two intervention groups consisting of new hearing aid users who received the intervention and experienced hearing aid users who received the intervention [25]; and (3) experimental and control groups of new hearing aid users, and an experimental group of experienced hearing aid users [27]. Additionally, two studies included the partners of participants to evaluate their interactions with the study participants and the efficacy of the intervention [11, 29].
Interventions
The interventions were thematically clustered into four categories through iterative consensus discussions to reflect common conceptual objectives: (1) individual at-home training (n = 6), which had the highest proportion, followed by (2) group-based auditory rehabilitation (n = 3), (3) empowerment strategies (n = 2), and (4) telehealth (n = 1) in that order. These categories were determined after study inclusion to help synthesize similar approaches.
First, individual at-home training included coping skills and speech recognition training at home. The training reduced maladaptive behaviors and hearing-related problems [28], and improved speech-in-noise comprehension and communication, with greater benefits observed among new hearing aid users [25]. Chat-based auditory training improved word/sentence perception but not phoneme/consonant perception [12]. Participants reported significantly higher NST scores on laboratory-based phoneme identification tasks in noise compared with hearing aids alone [27], with gains maintained for up to 8.5 months but limited to trained materials [26]. Although emotional responses and communication strategies improved, between-group differences were not significant. However, self-efficacy in hearing aid handling and hearing aid satisfaction improved, as measured by Measure of Audiologic Rehabilitation Self-Efficacy for Hearing Aids (MARS-HA) and the International Outcome Inventory for Hearing Aids (IOI-HA), respectively. [13].
Second, group-based auditory rehabilitation included posthearing aid fitting programs (e.g., hearing aid use, communication strategies) and comprehensive communication training (e.g., raising problem awareness about hearing loss and enhancing communication). The training group showed enhanced communication strategies, quality of life and satisfaction following the treatment, whereas no such improvement was noted in the control group. The training group, unlike the control group, sustained enjoyment of life [29]. However, some studies reported no significant differences between the intervention group and the control group [11, 31].
Third, the empowerment strategy included self-affirmation (e.g., writing resolutions such as “If I feel anxious, I’ll remember past successes”) and reporting positive listening experiences. Self-affirmation reduces aging-related anxiety and improves aging acceptance but does not significantly affect self-efficacy [14]. Reporting positive listening experiences significantly improved satisfaction, perceived benefits, listening ability, and the degree of change, with a positive correlation observed between coping ability and positive reporting [30].
Finally, telehealth provided remote support through telephone (e.g., addressing problems with hearing aids). Telephone consultations did not reduce unresolved issues or increase patient satisfaction [32].
Outcomes
Among the 12 included studies, only one study explicitly used a quality of life measure (i.e., the 36-Item Short-Form Health Survey modified for the Veteran population (SF-36 V)) to evaluate how additional auditory interventions impact older hearing aid users’ overall quality of life [31]. Three quality-of-life domains[6, 18], including six facets, were identified on the basis of the WHOQOL-100 and WHOQOL-OLD domains. Nine studies (75%) reported outcomes in the psychological domain [11–14, 25, 26, 29, 30, 32], with six (50%) addressing multiple facets of the psychological domain [12–14, 26, 29, 32]. Among them, four evaluate positive and negative feelings [12, 26, 29, 32]. Eight studies (67%) focused on the older adult-specific domain [11–13, 25–28, 30], with three (50%) covering both sensory ability and autonomy [11, 28, 30]. The physical domain (e.g., energy and fatigue) was assessed in one study [11], which was also the only study covering all physical, psychological, and older-adult-specific domains. Figure 4 illustrates the quality of life domains identified according to the types of interventions and individual studies.Fig. 4. Quality of life domains identified by types of interventions in the studies
Measurement tools
The included studies utilized a diverse range of outcome measures to assess the effectiveness of interventions, particularly in terms of quality of life.
In the psychological domain of quality of life, the IOI-HA was the most frequently used measure and was used in four studies [13, 25, 29, 30] to assess positive feelings such as satisfaction and perceived benefits. The Hearing Handicap Inventory for the Elderly (HHIE), used in three studies [12, 26, 32], was employed to assess negative feelings, particularly perceived hearing handicap. Self-esteem was measured via tools such as the MARS-HA and the University of Rhode Island Change Assessment adapted for Hearing Loss (URICA-HL), both of which are applied in one study [13].
In the older-adult-specific domain of quality of life, the Communication Profile for the Hearing Impaired (CPHI), which appeared in three studies [11, 13, 28], evaluated autonomy by examining communication strategies and personal adjustment to hearing loss. Sensory abilities were assessed via various tools. For example, speech recognition in noise was assessed through the Quick Speech In Noise (QuickSIN) test [25], the CST [26], and the Client-Oriented Scale of Improvement (COSI), which assesses improvements in auditory processing and communication abilities [30]. Additionally, syllable identification training and listening enhancement programs incorporated tests such as the NST [27].
Notably, only one study utilized the Fatigue Assessment Scale (FAS) to measure energy and fatigue in physical domain of quality of life [11].
Certainty of evidence
The certainty of evidence for each outcome was assessed using the GRADE approach. Outcomes reported by only one randomized controlled trial (e.g., overall quality of life and physical domain), the certainty of evidence was downgraded for serious imprecision and inability to assess inconsistency. Evidence from specific populations (e.g., veterans) was downgraded for indirectness due to limited generalizability, and small sample sizes contributed to further downgrading. Publication bias was not formally assessed because of the small number of studies and was considered within the overall judgments. As summarized in Supplementary Material S3, certainty of evidence was rated as very low for overall quality of life and low for the physical, psychological, and older-adult-specific domains, indicating limited confidence in the estimated effects and the need for cautious interpretation.
Discussion
This review synthesized the characteristics, interventions, outcomes, and major findings of studies investigating additional interventions used with hearing aids. Across 12 randomized controlled trials published between 1996 and 2024, four intervention categories were identified: individual at-home training, group-based auditory rehabilitation, empowerment strategies, and telehealth. These findings highlight the potential benefits and limitations of supplementing hearing aid use and identify factors that may support adaptation, participation, and emotional well-being in everyday listening contexts.
Individual at-home training
Individual at-home training, the most prevalent type of intervention (six studies), showed partial improvements in positive feelings, self-esteem, sensory abilities, and autonomy [12, 13, 25–28]. These findings suggest that such training with hearing aids may increase satisfaction, self-efficacy, partial auditory abilities, and coping skills, albeit with low certainty. This aligns with prior research indicating that individual training fosters greater learning and skill development [33]. However, discomfort and negative emotions related to hearing loss generally persisted, indicating that individual training alone may be insufficient to address the emotional and interpersonal challenges of hearing impairment. Limited opportunities for real-world communication practice and interaction, which are typical of group-based rehabilitation, may explain the modest improvements in communication with others.
Hearing loss is associated with emotional distress and reduced emotional well-being [34], often manifesting as frustration, grief, and burdensomeness while communicating with others [35]. Emotional well-being also depends on accurate perception of one’s own and others’ emotions, which may be impaired by hearing loss, further exacerbating its impact [36]. Nevertheless, evidence that sensory gains were maintained for over eight months for trained materials suggests that targeted training using difficult words or sentences may produce sustained improvements in communication within trained contexts. Future longitudinal studies are needed to determine whether such benefits generalize to untrained language content.
Group-based auditory rehabilitation
Group-based auditory rehabilitation has positive impacts on both psychological and older adult-specific domains, including increased autonomy and some improvement in positive feelings [11, 29, 31]. These benefits may stem from peer support and shared experiences, which can reduce isolation and foster mutual understanding [37]. Previous studies have shown that participation in group auditory programs can reduce self-perceived hearing difficulties and improve communication skills and hearing aid use [38, 39]. The opportunity to learn and practice communication strategies in a supportive, real-world context may underlie these effects.
However, no consistent improvements were observed in overall quality of life, energy and fatigue, or negative feelings in this review. Mixed findings and potential challenges related to group dynamics, such as limited trust among participants, may have constrained effectiveness [40]. These variations highlight the need for further research to identify the most effective components of group-based interventions.
Empowerment strategy
Empowerment strategies, such as self-affirmation and sharing positive listening experiences, showed promising effects, particularly in the psychological domain [14, 30]. These strategies, which are linked to positive thinking and inner strength [41], may foster psychological empowerment by reducing anxiety and negative emotions related to aging with hearing loss and promoting positive adaptation. Evidence suggests that self-affirmation can increase receptivity to health-related information, supporting subjective well-being in the context of hearing loss [42].
Additionally, empowerment strategies may enhance self-reliance and inner resilience [43], contributing to the autonomy aspect of the older adult-specific domain. Such psychological resilience has been found to play a significant role in mediating the association between hearing impairment and social well-being in older adults. A study showed that psychological resilience accounted for 50.9% of the variance in the change in social well-being for individuals with hearing loss [44]. However, the lack of significant effects on self-efficacy in this study indicates the need for further research to refine these strategies, particularly in addressing self-esteem and other psychological aspects of quality of life.
Telehealth
Telehealth interventions, specifically telephone support, showed limited evidence of improving quality of life in older adults with hearing loss and were associated with low certainty. Previous studies reported no significant reductions in unresolved issues or improvements in satisfaction with telephone-only support, suggesting that it may not adequately address complex needs, whereas video-based telehealth showed more favorable cognitive and mental health outcomes [32, 45].
However, telehealth remains a promising avenue for healthcare delivery, particularly given its feasibility and ability to reach underserved populations. Studies have shown that telehealth can reduce barriers to access, lower medical costs, and improve chronic disease management among older adults [46, 47]. Digital health technology also enables more person-centered care beyond visit-based models, with remote hearing aid fitting showing satisfaction comparable to in-person services and artificial intelligence-based systems explored for self-fitting of hearing aids [48]. Given the growing reliance on remote healthcare solutions, further research is needed to explore modern telehealth applications, such as video consultations or hybrid models, in addressing the specific needs of older adults with hearing loss. Challenges related to digital literacy, cognitive ability, and user experience highlight the need for tailored support and improved provider communication skills [49]. Future studies should focus on enhancing accessibility, individualizing interventions, and evaluating the long-term effects of telehealth on quality of life.
Overall impact on quality-of-life domains
Reviewers examined each item and assigned it to the quality-of-life domain that best reflected its primary construct based on conceptual relevance. Items assessing functional status rather than quality of life, or not explicitly measured, were excluded from the final classification. The analysis revealed a strong focus on the psychological and older adult-specific domains, with less attention given to the physical aspects of quality of life. A significant proportion of studies (58.3%) focused on sensory abilities [11–13, 25, 27, 28, 30], positive feelings (58.3%) [12, 13, 25, 26, 29, 30, 32], and negative feelings (58.3%) [11–14, 26, 29, 32], highlighting their importance for older adults with hearing loss. However, autonomy (33.3%) [11, 13, 28, 30] and self-esteem (16.7%) [13, 14] were less emphasized, suggesting that these aspects may be underexplored in auditory rehabilitation research.
Furthermore, minimal attention to energy and fatigue (8.3%) [11] and overall quality of life (8.3%) [31] indicates that broader physical and global quality-of-life outcomes are largely neglected in the current evidence base. Although auditory and psychological outcomes appear to be prioritized in existing interventions, these findings suggest that a more comprehensive and balanced assessment across WHOQOL domains may be necessary to better capture the full impact of interventions on the lives of older adults with hearing loss.
Measurement tools
The diverse range of measurement tools used across the studies highlights the multifaceted nature of the interventions and the outcomes they aim to assess, particularly in relation to quality of life. The frequent use of tools such as the IOI-HA and the HHIE suggest that assessing both positive and negative emotional responses, particularly satisfaction and perceived hearing handicap, is central to understanding the effectiveness of interventions in improving quality of life [29, 30, 32]. In line with research by Humes et al. [26], emotional responses to hearing interventions, such as satisfaction and perceived benefits, directly influence quality-of-life outcomes by improving social participation and reducing feelings of isolation and frustration. These tools are valuable in evaluating how interventions impact individuals' psychological well-being and their perceived quality of life.
The use of measures such as the CPHI and self-esteem scales (MARS-HA, URICA-HL) underscores the importance of assessing autonomy and personal adjustment to hearing loss [13, 28]. These findings highlight the role of autonomy and self-efficacy in quality of life among individuals with hearing loss. Recent clinical recommendations in audiologic rehabilitation emphasize that addressing social-emotional well-being and individualized goals, including patients’ sense of control and adaptive capacity, is essential for supporting adjustment and overall well-being [50]. Accordingly, effective interventions should address not only sensory function but also personal agency to reduce the psychological burden of hearing loss.
The variety of sensory ability assessments, such as the QuickSIN, CST, and COSI, reflects the complex nature of auditory processing and communication challenges faced by individuals with hearing loss [25, 26, 30]. These tools are crucial in capturing improvements in auditory capabilities, which have been shown to positively influence quality of life by enhancing communication in social, educational, and professional settings. Moreover, objective measures of auditory function combined with subjective measures, as suggested by Wang et al. [51], are essential for understanding the tangible benefits of hearing interventions and their acceptance and satisfaction, which are directly linked to overall life satisfaction.
Interestingly, the use of the FAS in only one study [11] implies that energy and fatigue may be underexplored aspects of the impact of hearing loss on quality of life. Fatigue, often a consequence of hearing loss and the effort required for communication, can have a profound effect on overall well-being and quality of life. This finding suggests that future research should incorporate fatigue measures into quality-of-life assessments. One study emphasized the importance of understanding how hearing loss-related fatigue affects emotional and physical well-being and the ability to engage in daily activities [52]. The incorporation of fatigue into future studies could provide a more comprehensive understanding of how hearing interventions affect overall life satisfaction and holistic quality of life.
Overall, the variety of tools used across these studies highlights the need for a multidimensional approach for evaluating the effectiveness of hearing loss interventions in terms of quality of life. Future research should continue to integrate both objective and subjective measures to capture the full impact of interventions to enhance our understanding of the comprehensive benefits these interventions provide to individuals' overall well-being.
Limitations and strengths
Several limitations should be considered when interpreting the findings of this review. First, the diversity of interventions complicates direct comparisons. The WHOQOL-100 and WHOQOL-OLD domains helped identify gaps in quality-of-life research but were challenging to categorize, as classification relied on interpretive alignment with WHO guidelines and team consensus. The lack of standardized intervention protocols also limits conclusions about which components are most effective.
Second, quality-of-life measures were inconsistent and often incomplete. Only one study assessed overall quality of life (SF-36V), while others focused mainly on psychological or age-specific domains. More holistic assessments integrating physical, psychological, and social aspects are needed. Evidence certainty was generally low, highlighting the need for more rigorous designs. Additionally, studies on cognitive outcomes were unintentionally excluded, despite increasing evidence linking hearing loss to cognitive decline. Future research should incorporate cognitive function to capture broader impacts.
Despite these limitations, this review has several strengths. First, it includes a wide range of studies spanning over 30 years (1996–2024) encompassing global research from around the world, offering a robust dataset for assessing the impact of various interventions. Second, the review highlights the need for a more comprehensive approach to quality-of-life assessment, exploring multiple domains beyond psychological aspects. The inclusion of diverse interventions also provides valuable insights into potential strategies to increase the quality of life of older adults with hearing loss.
Conclusions
In conclusion, this review provides a comprehensive synthesis and examination of the potential impact of additional interventions on the quality of life of older adults using hearing aids. The findings highlight the potential benefits and limitations of combining hearing aids with interventions such as individual at-home training, group-based auditory rehabilitation, empowerment strategies, and telehealth. Despite some limitations, this review represents the first systematic assessment of the impact of combining additional interventions with hearing aids. While further research with more rigorous designs (e.g., larger randomized controlled trials, longer follow-up periods, and standardized outcome measures) and methodologies is necessary to fully understand these effects, the value of our review lies in its synthesis of existing evidence and the presentation of findings on the basis of the studies conducted to date.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material S1: Included and Excluded Studies
Supplementary Material S2: Categorizing measurement tools on the basis of the WHOQOL-100 and WHOQOLOLD
Supplementary Material S3: Certainty of evidence
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO. (2021). Deafness and hearing loss. https://www.who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss
- 2Popay, J. (2006). Guidance on the conduct of narrative synthesis in systematic reviews. ESRC Methods Programme.