Clinical and gustatory features in taste disorder patients based on oral Candida culture status
Sung Min Kim, Hong-Seop Kho

TL;DR
The study explores how oral Candida infections affect taste disorders, particularly in patients with burning mouth syndrome, and finds that Candida can worsen symptoms and psychological stress in specific groups.
Contribution
The paper introduces a classification of taste disorder patients by Candida status and BMS subtype to assess Candida's independent impact on taste and psychological factors.
Findings
Candida-positive patients with primary BMS had lower taste scores and reduced salivary flow.
Psychological distress was more severe in Candida-positive subgroups of primary BMS and overall BMS groups.
Candida status was linked to gustatory deficits and hyposalivation in specific subgroups, not universally.
Abstract
To investigate the clinical, gustatory, salivary, psychological, and laboratory features of patients with taste disturbances, stratified by burning mouth syndrome (BMS) and Candida status, and to determine the contribution of oral Candida status independent of BMS subtype. This retrospective study analyzed 141 patients with taste disturbances, classified into six groups based on burning mouth symptoms and oral Candida culture status: primary BMS, secondary BMS, and non-BMS patients, each subdivided by Candida status. To evaluate the independent role of Candida, positive Candida culture was not considered a local factor in defining secondary BMS. Clinical characteristics, taste test results, whole salivary flow rates, psychological profiles, and blood laboratory parameters were compared across groups, with age-matching applied when groups differed in age. In the primary BMS,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
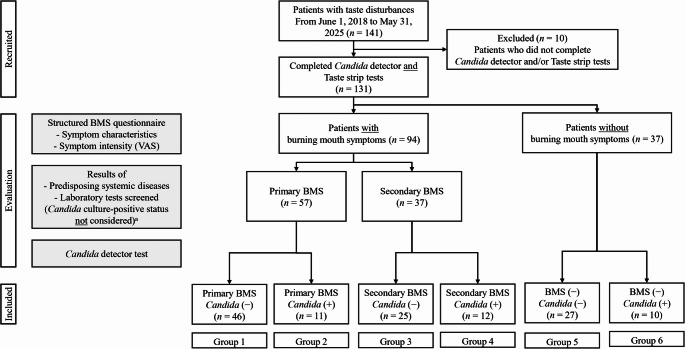 Figure 1
Figure 1- —Seoul National University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Disorders and Functions · Olfactory and Sensory Function Studies · Biochemical Analysis and Sensing Techniques
Introduction
Taste disturbances are increasingly reported in dental practice and may impair appetite, reduce dietary intake, and diminish quality of life [1, 2]. Their prevalence increases with age due to physiological decline in gustatory function and the cumulative burden of multimorbidity, polypharmacy, and oral health problems in older adults [1, 3], leading to changes in dietary habits, nutritional compromise, and greater physical frailty risk [4]. Etiologies are multifactorial, including aging-related degeneration, local or systemic diseases, medication use, salivary gland hypofunction, and psychological conditions such as depression or anxiety [1, 5]. Aging-related degeneration may involve structural and functional changes in taste buds, peripheral gustatory nerves, and salivary gland function, which together contribute to reduced taste sensitivity in older adults [6]. Clinically, taste disturbances are evaluated using a combination of subjective symptom assessment and objective testing methods, including psychophysical taste tests (e.g., taste strips or whole-mouth testing), salivary flow rate measurements, and laboratory or microbiological investigations when indicated. However, diagnosis is further complicated by discrepancies between self-reported symptoms and objective test results, as well as variability in psychophysical testing methods [3, 7].
Burning mouth syndrome (BMS) is a chronic orofacial pain disorder characterized by persistent intraoral burning or dysesthetic sensations without visible mucosal abnormalities, often accompanied by dysgeusia and xerostomia [8–10]. It is classified as primary BMS when no cause is identified, and secondary BMS when symptoms relate to local or systemic factors such as candidiasis, anemia, or nutritional deficiencies [11]. Differentiation remains challenging due to overlapping symptoms and a lack of standardized criteria [12, 13]. Taste disturbances are among the most frequent BMS-associated symptoms and may involve neuropathic mechanisms, including altered taste–pain interactions. These complexities highlight the need for diagnostic approaches that consider the diverse mechanisms underlying both burning symptoms and taste disturbances [14, 15].
Oral Candida infection is common in patients with oral burning sensations, xerostomia, or taste disturbances, particularly among older adults [16, 17], and has been linked to mucosal irritation, reduced salivary function, and nutritional deficiencies [18]. Although often considered a contributor to oral discomfort and taste disturbances, its role remains controversial. Some studies have suggested that even without overt candidiasis, colonization can cause subclinical mucosal changes leading to oral pain or dysgeusia, which improves following antifungal therapy [19, 20]. Others, however, report inconsistent findings [21].
Given these inconsistencies, further research is needed to clarify the independent role of Candida in taste disturbances. Prior studies have been limited by inadequate patient stratification according to burning symptoms or Candida status, as well as by insufficient control for confounders such as age and systemic health. Furthermore, few studies have simultaneously evaluated subjective and objective taste measures, salivary flow rates, psychological profiles, and laboratory data. These limitations have hindered a clearer understanding of role that Candida plays in taste disorders and related symptoms.
To address these gaps, this retrospective study classified patients with taste disturbances according to the presence or absence of burning mouth symptoms and oral Candida culture status. To specifically examine the independent effects of Candida, a positive Candida culture was deliberately excluded as a criterion for secondary BMS. This classification strategy enabled a clearer analysis of how oral Candida culture status influences taste function. This study aimed to investigate the effects of Candida on taste and related symptoms in patients with and without BMS.
Materials and methods
This retrospective study analyzed electronic medical records of patients who presented to the Department of Oral Medicine, Seoul National University Dental Hospital, between June 1, 2018 and May 31, 2025 for evaluation of taste disturbances. The study protocol adhered to the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of Seoul National University School of Dentistry (IRB No. S-D20250010; approved on July 8, 2025). Owing to the retrospective design, the IRB waived the requirement for informed consent.
Inclusion and exclusion criteria
Eligible patients were those who reported taste disturbances as their chief complaint and underwent comprehensive clinical evaluation, including oral Candida culture, quantitative gustatory testing using filter paper strips and salivary flow rate measurement. Patients who were under 18 years of age, pregnant, had significant communication or comprehension difficulties, or were unable to reliably complete the study questionnaires were excluded.
Examination procedures
All patients underwent comprehensive assessments, including oral Candida culture, gustatory testing, salivary flow rate measurement, structured questionnaires on taste disturbances and burning mouth symptoms, psychological evaluation using the Symptom Checklist-90-Revised (SCL-90-R), and laboratory blood tests. Detailed procedures are described in the following sections.
Oral Candida culture
Oral Candida culture status was assessed using a Candida Detector (Kamemizu Chemical Ind. Co., Ltd., Osaka, Japan), according to the manufacturer’s instructions. This system is designed as a semi-quantitative, culture-based screening tool for clinical evaluation of oral Candida presence. A swab sample was collected from the dorsum of the tongue, cultured at 37 °C for 48 h, after which colony growth was assessed based on predefined density categories. According to the manufacturer’s interpretation guidelines, a growth level corresponding to ≥ 10³ CFU/mL was considered indicative of positive Candida culture warranting clinical evaluation. Oral mucosal examination was routinely performed at the initial visit to assess clinical signs suggestive of oral candidiasis; however, for the purpose of this study, subgroup classification was based on culture results. When clinical findings were suggestive of oral candidiasis, patients received routine clinical management, including topical or oral antifungal therapy when indicated.
Taste function test
Taste function was assessed using filter paper strips impregnated with tastants (Taste Strips; Burghart Messtechnik, Holm, Pinneberg, Germany) following the manufacturer’s instructions [22]. Each strip, with a tip area of 2 cm², was placed on the midline of the anterior tongue. A total of 18 strips were administered in a pseudo-random order per patient: four concentrations each of sweet (sucrose: 0.4, 0.2, 0.1, and 0.05 g/mL), salty (sodium chloride: 0.25, 0.1, 0.04, and 0.016 g/mL), sour (citric acid: 0.3, 0.165, 0.09, and 0.05 g/mL), and bitter (quinine hydrochloride: 0.006, 0.0024, 0.0009, and 0.0004 g/mL) tastes, plus two blanks.
After each application, the patients identified the perceived taste quality from predefined options (sweet, salty, sour, bitter, or no taste) and rinsed their mouth with water before placing the next strip. Each correct response to the 16 tastant strips was scored one point, resulting in a maximum possible score of 16. The two blank strips were not included in the scoring and were used solely for quality control to assess false-positive responses, in accordance with the original taste strip protocol [23]. Hypogeusia was defined as a total score below nine, whereas dysgeusia was defined as incorrect responses at the strongest or second-strongest concentration for any taste quality.
Salivary flow rate measurement
Whole salivary flow rates were measured under unstimulated and stimulated conditions. Unstimulated whole saliva (UWS) was collected into polypropylene tubes using the spitting method over 10 min. For stimulated whole saliva (SWS), patients chewed paraffin wax for 2 min and swallowed the initial saliva; chewing continued, and saliva was collected for 5 min. The salivary flow rates are expressed in mL/min.
Questionnaire for the subjective assessment of taste disturbances
All patients completed a structured questionnaire assessing the factors potentially related to taste disturbances [15]. The questionnaire included demographic and medical history, olfactory symptoms, and taste-related complaints.
Subjective taste function was also evaluated using the following predefined statements: ‘I can detect sweetness in cocoa, cakes, or candies’; ‘I can detect salt in chips or salted nuts’; ‘I can detect sourness in vinegar, pickles, or lemon’; and ‘I can detect bitterness in coffee, beer, or tonic water’. The responses were scored as follows: 2 points for ‘recognize easily’, 1 point for ‘recognize somewhat’, and 0 points for ‘recognize not at all’, with total scores ranging from 0 to 8.
Patients further selected descriptors best reflecting the type of taste disturbance they experienced: distorted taste (dysgeusia), phantom taste (phantogeusia), exaggerated taste (hypergeusia), reduced taste (hypogeusia), absent taste (ageusia), or normal taste (normogeusia). For classification, patients reporting dysgeusia, hypergeusia, and phantogeusia were grouped as having subjective dysgeusia; those reporting hypogeusia and ageusia were classified as having subjective hypogeusia and ageusia, respectively; and those reporting normal taste sensation were grouped as having subjective normogeusia.
Questionnaire on burning mouth symptoms
Patients reporting burning mouth symptoms completed a structured questionnaire adapted from previous studies [24]. The questionnaire assessed the characteristics and severity of their symptoms, including burning, aching, stinging, numbness, taste disturbance, xerostomia, and the effect of oral complaints on daily life (Eff-life). Each symptom was rated using a visual analogue scale (VAS) ranging from 0 (no symptom) to 10 (most extreme symptom imaginable), and both the average and maximum intensities were recorded.
Psychological distress evaluation
Psychological distress was assessed using the SCL-90-R [25], a 90-item self-report questionnaire in which each item is rated on a 5-point Likert scale ranging from 0 (“not at all”) to 4 (“extremely”), with higher scores indicating greater psychological distress. For analysis, standardized T-scores were used for the intergroup comparisons of nine symptom dimensions—Somatization, Obsessive–Compulsive, Interpersonal Sensitivity, Depression, Anxiety, Hostility, Phobic Anxiety, Paranoid Ideation, and Psychoticism—as well as for the three global indices: the Global Severity Index (GSI), Positive Symptom Distress Index, and Positive Symptom Total (PST).
Laboratory blood tests
Laboratory blood tests were performed as part of the routine clinical work-up for patients presenting with taste disturbances and/or burning mouth symptoms. The tests included complete blood count, erythrocyte sedimentation rate, blood chemistry, serum iron, ferritin, magnesium, zinc, vitamin B_12_, folate, and thyroid function tests (T3, free T4, and thyroid stimulating hormone).
Patient classification
Figure 1 illustrates the patient inclusion, evaluation, and grouping process. Between June 1, 2018, and May 31, 2025, 141 patients visited the clinic for taste disturbances. Ten patients were excluded for incomplete diagnostic data, including missing Candida culture or taste strip test results. The final analysis included 131 patients (25 males, 63.0 ± 12.8 years; 106 females, 63.0 ± 11.0 years) who completed both oral Candida culture and taste function testing.
Fig. 1. Flow diagram of patient recruitment, evaluation, and classification. Patients were categorized by the presence or absence of burning mouth symptoms and oral Candida culture status. Among those with burning mouth symptoms, classification into primary or secondary burning mouth syndrome (BMS) was determined by the presence of identifiable systemic abnormalities or local contributing factors. Group allocation (Groups 1–6) was based on the combination of BMS and oral Candida culture status for subsequent analyses ^a^ A positive oral Candida culture was not considered a local contributing factor for secondary BMS, aligning with the study’s aim of evaluating its influence independently
Of these, 94 patients reported burning mouth symptoms and were classified as having BMS based on their responses to the structured burning mouth symptom questionnaire; the remaining 37 reported no such symptoms. Patients with BMS were further subclassified as primary or secondary BMS based on the presence of identifiable systemic abnormalities or local contributing factors identified on clinical oral examinations, excluding positive oral Candida culture. Oral Candida culture-positive status was deliberately excluded as a contributing local factor for defining secondary BMS because the study aimed to evaluate its independent association with taste function regardless of BMS subtype. Accordingly, some Candida-positive patients without other explanatory conditions were classified as having primary BMS.
In Candida-positive BMS patients, classification into primary or secondary BMS was further supported by treatment response. In both subgroups, symptoms did not resolve with antifungal therapy alone, and neuropathic pain management was required. In secondary BMS, positive Candida culture coexisted with other identifiable systemic or local abnormalities linked to burning mouth symptoms, whereas in primary BMS, no such factors were identified despite persistent symptoms.
Subsequently, patients were categorized into six groups based on burning mouth symptoms and Candida culture results as follows: Group 1, primary BMS with Candida-negative results; Group 2, primary BMS with Candida-positive results; Group 3, secondary BMS with Candida-negative results; Group 4, secondary BMS with Candida-positive results; Group 5, non-BMS with Candida-negative results; and Group 6, non-BMS with Candida-positive results. These six groups were used for all subsequent analyses.
Statistical analysis
Data normality was tested using the Shapiro–Wilk test. Depending on distribution, continuous variables between groups were compared using either Student’s t-test or the Mann–Whitney U test, whereas categorical variables were compared using the chi-square or Fisher’s exact tests, as appropriate.
When significant age differences were observed between the Candida-negative and Candida-positive subgroups, age-matching was performed to control for confounding factors. Specifically, the older half of the Candida-negative group was selected to match the age distribution of the Candida-positive group within each relevant comparison. All statistical analyses were conducted using IBM SPSS Statistics version 29.0 (IBM Corp., Armonk, NY, USA), with p < 0.05 considered statistically significant.
Results
Demographic characteristics and salivary flow rates
Table 1 summarizes the demographic characteristics and salivary flow rates across the six patient groups stratified by burning mouth symptoms and oral Candida culture status. Significant age differences were observed between the Candida-negative and Candida-positive subgroups within the primary BMS group (p = 0.009), with the Candida-positive patients being older. Similar age differences were also found in the total sample (p = 0.002) and in the overall burning mouth symptoms group (p = 0.010) (Supplementary Tables 1–1). Sex distribution did not differ in any comparison.
Table 1. Demographic characteristics and salivary flow rates based on burning mouth symptoms and oral Candida culture status; mean ± SD, median [Q1–Q3], n (%)Primary BMS (n = 57) p Secondary BMS (n = 37) p BM symptoms (−) (n = 37) p C (−) (n = 46)C (+) (n = 11)C (−) (n = 25)C (+) (n = 12)C (−) (n = 27)C (+) (n = 10)Age (years)59.6 ± 9.868.3 ± 8.20.00964.9 ± 10.667.5 ± 11.30.42660.8 ± 13.968.9 ± 9.50.100Gender Male4 (8.7)1 (9.1)1.0003 (12.0)2 (16.7)1.00012 (44.4)3 (30.0)0.481 Female42 (91.3)10 (90.9)22 (88.0)10 (83.3)15 (55.6)7 (70.0)SFR (mL/min) UWS0.26 [0.16–0.37]0.15 [0.07–0.27]0.2410.12 [0.05–0.30]0.14 [0.06–0.21]0.8710.19 [0.08–0.30]0.14 [0.03–0.31]0.421 SWS1.32 [0.80–1.64]0.81 [0.73–0.97]^a^0.0011.07 [0.67–1.61]1.29 [0.66–1.75]^a^0.3361.10 [0.67–1.83]^a^0.81 [0.55–1.02]^a^0.006**^a^ Stimulated whole saliva could not be collected from two patients with primary BMS (oral Candida (+)), two with secondary BMS (oral Candida (+)), and three without BM symptoms (one oral Candida (−), two oral Candida (+)), due to inability to chew paraffin wax caused by missing posterior teethP-values were calculated using the Student’s t-test or Mann–Whitney U test for continuous variables, as appropriate, and the Fisher’s exact test for gender comparisonsBM burning mouth, BMS burning mouth syndrome, C (−) oral Candida culture negative, C (+) oral Candida culture positive, Q1 25th percentile, Q3 75th percentile, SD standard deviation, SFR salivary flow rate, SWS stimulated whole saliva, UWS unstimulated whole saliva** p < 0.01
In the primary BMS group, Candida-positive patients exhibited significantly lower SWS flow rates than Candida-negative patients, which are the patients with true primary BMS (p = 0.001), and this remained significant after age-matching (p = 0.043; Supplementary Tables 1–2). Among patients without burning mouth symptoms, the Candida-positive subgroup also had significantly lower SWS flow rate than the Candida-negative subgroup (p = 0.006). The UWS flow rates did not differ significantly in any comparison.
Subjective and objective taste function
Table 2 presents the subjective and objective taste scores across the six patient groups. No significant differences in total subjective or objective taste scores were observed between the Candida-negative and Candida-positive subgroups in any comparison, including the total sample and the burning mouth symptoms group (Supplementary Tables 2 − 1). Similarly, no significant differences were found for individual taste qualities—sweet, salty, sour, and bitter. However, in the age-matched analysis, primary BMS patients with positive Candida culture exhibited significantly lower objective total taste scores than Candida-negative patients (p = 0.049; Supplementary Tables 2–2).
Table 2. Subjective and objective taste scores based on burning mouth symptoms and oral Candida culture status; median [Q1–Q3]Primary BMS (n = 57) p Secondary BMS (n = 37) p BM symptoms (−) (n = 37) p C (−) (n = 46)C (+) (n = 11)C (−) (n = 25)C (+) (n = 12)C (−) (n = 27)C (+) (n = 10)Subjective taste Sweet2.0 [1.0–2.0]2.0 [1.0–2.0]0.6812.0 [1.0–2.0]2.0 [1.0–2.0]0.8672.0 [1.0–2.0]2.0 [1.8–2.0]0.431 Sour2.0 [1.8–2.0]2.0 [2.0–2.0]0.2722.0 [1.0–2.0]2.0 [1.3–2.0]0.9172.0 [1.0–2.0]2.0 [1.8–2.0]0.629 Salty2.0 [1.0–2.0]2.0 [1.0–2.0]0.7842.0 [1.0–2.0]2.0 [1.0–2.0]0.8742.0 [1.0–2.0]2.0 [2.0–2.0]0.147 Bitter2.0 [1.0–2.0]2.0 [1.0–2.0]0.8232.0 [1.0–2.0]1.5 [1.0–2.0]0.2742.0 [2.0–2.0]2.0 [0.8–2.0]0.379 Total8.0 [5.5–8.0]7.0 [7.0–8.0]0.6178.0 [4.0–8.0]7.0 [4.0–8.0]0.5378.0 [5.0–8.0]8.0 [5.8–8.0]0.802Objective taste Sweet4.0 [2.8–4.0]4.0 [3.0–4.0]0.8673.0 [2.0–4.0]4.0 [3.0–4.0]0.5033.0 [1.0–4.0]3.0 [0.0–4.0]0.986 Sour2.0 [1.8–3.0]1.0 [1.0–2.0]0.1172.0 [0.5–3.0]2.5 [1.3–3.0]0.2902.0 [1.0–2.0]1.0 [0.0–2.3]0.076 Salty3.0 [2.0–4.0]3.0 [3.0–3.0]0.9752.0 [1.0–3.5]1.5 [0.3–3.0]0.2002.0 [1.0–3.0]3.0 [1.8–4.0]0.141 Bitter3.0 [2.0–4.0]3.0 [0.0–3.0]0.0863.0 [1.0–4.0]3.5 [1.3–4.0]0.6952.0 [1.0–3.0]3.0 [0.8–3.0]0.874 Total11.5 [9.0–13.0]10.0 [8.0–12.0]0.09410.0 [7.0–13.0]10.5 [7.3–13.0]0.8358.0 [6.0–11.0]8.5 [5.5–12.0]0.893Subjective taste scores were obtained from a structured questionnaire in which patients rated their ability to detect each taste quality on a scale from 0 (not at all) to 2 (easily), yielding a maximum total score of 8. Objective taste scores were obtained using filter paper taste strips (Taste Strips; Burghart Messtechnik, Holm, Pinneberg, Germany), with each taste quality (sweet, salty, sour, and bitter) scored 0–4 based on correct identifications (maximum total score 16)P-values were calculated using the Student’s t-test or the Mann–Whitney U test, as appropriate, for comparisons between Candida (+) and Candida (−) within each groupBM burning mouth, BMS burning mouth syndrome, *C *(−) oral Candida culture negative, C (+) oral Candida culture positive, *Q1 *25th percentile, Q3 75th percentile
Distribution of taste diagnoses
Table 3 and Supplementary Tables 3−1 summarize the distribution of objective and subjective taste diagnoses across the patient groups. In the primary BMS group, the distribution of objective taste diagnoses differed significantly between the Candida-negative and Candida-positive subgroups (p = 0.018). Specifically, none of the Candida-positive patients were classified as normogeusia, whereas 39.1% of the Candida-negative patients were. This difference persisted after age-matching (p = 0.008; Supplementary Tables 3−2). No significant differences were observed in the distribution of subjective taste diagnoses in any of the groups.
Table 3. Distribution of subjective and objective taste diagnoses based on oral Candida culture status in patients with primary burning mouth syndrome, secondary burning mouth syndrome, and without burning mouth symptoms; n (%)Primary BMS (n = 57) p Secondary BMS (n = 37) p BM symptoms (−) (n = 37) p C (−) (n = 46)C (+) (n = 11)C (−) (n = 25)C (+) (n = 12)C (−) (n = 27)C (+) (n = 10)Subjective taste Normogeusia5 (10.9)2 (18.2)0.3774 (16.0)2 (16.7)0.9492 (7.4)2 (20.0)0.484 Hypogeusia13 (28.3)6 (54.5)11 (44.0)6 (50.0)13 (48.1)6 (60.0) Dysgeusia12 (26.1)1 (9.1)2 (8.0)1 (8.3)5 (18.5)2 (20.0) Hypo + Dysgeusia13 (28.3)2 (18.2)7 (28.0)2 (16.7)5 (18.5)0 (0.0) Ageusia3 (6.5)0 (0.0)1 (4.0)1 (8.3)2 (7.4)0 (0.0)Objective taste Normogeusia18 (39.1)0 (0.0)0.0185 (20.0)3 (25.0)1.0004 (14.8)1 (10.0)1.000 Hypogeusia3 (6.5)0 (0.0)2 (8.0)0 (0.0)2 (7.4)1 (10.0) Dysgeusia19 (41.3)7 (63.6)10 (40.0)5 (41.7)9 (33.3)4 (40.0) Hypo + Dysgeusia6 (13.0)4 (36.4)8 (32.0)4 (33.3)12 (44.4)4 (40.0)Subjective taste diagnoses were based on questionnaire responses: normogeusia was defined as normal taste perception; hypogeusia as self-reported decreased taste; dysgeusia as distorted, exaggerated, or phantom taste sensations; and ageusia as complete taste loss. Objective taste diagnoses were based on taste strip test results: normogeusia was defined as a total score ≥ 9; hypogeusia as a total score < 9; dysgeusia as incorrect responses at the strongest or second-strongest concentration for any taste quality. Hypo + dysgeusia indicates patients meeting both criteriaP*-values were calculated using the Chi-square test or the Fisher’s exact test, as appropriate, for comparisons between oral Candida (−) and oral Candida (+) within each groupBM burning mouth, BMS burning mouth syndrome, C (−) oral Candida culture negative, C (+) oral Candida culture positive* p < 0.05
Intensities of burning mouth symptoms
Table 4 compares the burning mouth symptom intensities between Candida-negative and Candida-positive subgroups within each BMS category. In the primary BMS group, Candida-positive patients reported significantly higher VAS scores for the average levels of burning (p = 0.045) and aching (p = 0.032) symptoms than Candida-negative patients. In the age-matched analysis (Supplementary Tables 4−1), these differences were no longer statistically significant. In contrast, stinging intensity was significantly higher in Candida-positive patients for both average (p = 0.037) and maximum (p = 0.030) VAS scores. No other symptom domains showed statistically significant differences in either analysis.
Table 4. Burning mouth symptom intensities based on burning mouth symptoms and oral Candida culture status; median [Q1–Q3]Intensity (VAS)Primary BMS (n = 57) p Secondary BMS (n = 37) p BMS (+) (n = 94) p C (−) (n = 46)C (+) (n = 11)C (−) (n = 25)C (+) (n = 12)C (−) (n = 71)C (+) (n = 23)BurningAVG3.5 [2.0–5.0]5.0 [3.0–7.0]0.0455.0 [2.0–7.0]5.0 [3.3–5.0]0.4804.0 [2.0–6.0]5.0 [3.0–7.0]0.223MAX7.0 [5.0–8.0]8.0 [6.0–8.0]0.3518.0 [3.0–9.0]7.0 [4.3–8.0]0.5997.0 [5.0–8.0]7.0 [5.0–8.0]0.734AchingAVG2.0 [0.0–4.0]5.0 [0.0–6.0]0.0320.0 [0.0–6.5]0.5 [0.0–3.8]0.6711.0 [0.0–5.0]3.0 [0.0–5.0]0.387MAX3.5 [0.0–7.0]7.0 [0.0–8.0]0.2541.0 [0.0–8.0]2.0 [0.0–7.8]0.8492.0 [0.0–7.0]6.0 [0.0–8.0]0.563StingingAVG0.0 [0.0–2.0]2.0 [0.0–7.0]0.0550.0 [0.0–4.5]0.0 [0.0–2.5]0.3860.0 [0.0–3.0]1.0 [0.0–5.0]0.409MAX0.0 [0.0–5.0]7.0 [0.0–8.0]0.0520.0 [0.0–7.5]0.5 [0.0–6.5]0.8340.0 [0.0–5.0]3.0 [0.0–8.0]0.208NumbnessAVG0.0 [0.0–3.0]1.0 [0.0–5.0]0.2740.0 [0.0–0.5]0.0 [0.0–4.8]0.2610.0 [0.0–2.0]0.0 [0.0–5.0]0.146MAX0.0 [0.0–5.3]1.0 [0.0–8.0]0.3490.0 [0.0–1.5]0.0 [0.0–6.0]0.3100.0 [0.0–5.0]0.0 [0.0–7.0]0.220Taste−distAVG5.0 [2.0–7.0]7.0 [3.0–7.5]0.2996.0 [3.5–8.0]5.0 [4.0–8.5]0.9615.0 [2.0–8.0]6.0 [4.0–7.5]0.416MAX8.0 [5.0–9.0]8.0 [6.0–8.0]0.9108.0 [5.5–9.0]7.0 [5.3–9.8]0.7938.0 [5.0–9.0]8.0 [6.0–9.0]0.834XerostomiaAVG2.5 [0.8–5.0]5.0 [3.0–7.0]0.1443.0 [1.0–5.0]4.0 [3.3–6.8]0.3003.0 [1.0–5.0]5.0 [3.0–7.0]0.061MAX5.0 [2.0–8.0]8.0 [3.0–9.0]0.2065.0 [1.5–8.0]6.0 [5.0–8.8]0.5105.0 [2.0–8.0]7.0 [5.0–9.0]0.172Eff−lifeAVG5.0 [2.0–7.0]5.0 [4.0–8.0]0.5306.0 [4.5–8.0]5.0 [3.0–7.3]0.3315.0 [2.0–7.0]5.0 [3.0–8.0]0.898MAX7.0 [4.8–9.0]8.0 [5.0–9.0]0.6608.0 [6.5–9.0]7.0 [4.3–9.8]0.7188.0 [5.0–9.0]8.0 [5.0–9.0]0.887Symptom intensities were assessed using visual analogue scale (VAS) scores ranging from 0 (no symptom) to 10 (most extreme symptom imaginable). AVG and MAX represent average and maximum scores, respectively, for each symptom domainP-values were calculated using the Mann–Whitney U test for comparisons between Candida (+) and Candida (−) within each group.AVG average, BMS burning mouth syndrome, C (−) oral Candida culture negative, C (+) oral Candida culture positive, Eff-life effect of symptoms on daily life, MAX maximum, Q1 25th percentile, Q3 75th percentile, Taste-dist taste disturbance, VAS visual analogue scale
Psychological profiles
Table 5 presents the psychological profiles derived from the SCL-90-R across the six patient groups. In the primary BMS group, the Candida-positive subgroup showed significantly higher t-scores for somatization (p = 0.010), anxiety (p = 0.042), psychoticism (p = 0.049), GSI (p = 0.044), and PST (p = 0.032) than the Candida-negative subgroup. However, none of these differences remained statistically significant in the age-matched analysis. In both the total sample and the overall BMS group, the Candida-positive subgroup demonstrated significantly higher phobic anxiety (p = 0.026 and 0.045, respectively), psychoticism (p = 0.015 and 0.029), and PST (p = 0.025 and 0.021) than the Candida-negative subgroup. Some of these findings persisted in the age-matched analysis. In the age-matched total sample, the Candida-positive subgroup showed significantly higher scores for interpersonal sensitivity (p = 0.036), psychoticism (p = 0.048), and PST (p = 0.037). In the age-matched overall BMS group, the Candida-positive subgroup continued to show significantly higher PST scores (p = 0.040) (Supplementary Tables 5−1 and 5−2).
Table 5. Psychological profiles based on burning mouth symptoms and oral Candida culture status; median [Q1–Q3]t-scorePrimary BMS (n = 56)^a^ p Secondary BMS (n = 35)^a^ p BM symptoms (−) (n = 27)^a^ p C **(−) (**n **= 45)**C **(+) (**n **= 11)**C **(−) (**n **= 24)**C **(+) (**n **= 11)**C **(−) (**n **= 19)**C **(+) (**n = 8)Somatization43.0 [38.0–47.5]48.0 [45.0–51.0]0.01049.5 [44.3–53.0]45.0 [43.0–54.0]0.64541.0 [38.0–44.0]42.5 [37.3–44.8]0.593O-C41.0 [34.5–46.0]45.0 [40.0–51.0]0.09044.5 [39.0–50.3]43.0 [38.0–57.0]0.56040.0 [36.0–44.0]40.5 [38.5–46.0]0.937I-S41.0 [36.0–48.0]43.0 [41.0–52.0]0.09143.0 [39.0–44.0]44.0 [36.0–55.0]0.34539.0 [36.0–41.0]42.0 [36.8–46.0]0.251Depression43.0 [37.0–49.0]46.0 [42.0–53.0]0.08848.0 [43.3–53.8]44.0 [41.0–54.0]0.76040.0 [38.0–48.0]45.5 [37.3–52.3]0.650Anxiety41.0 [38.0–44.0]44.0 [42.0–46.0]0.04245.0 [41.3–51.3]43.0 [38.0–49.0]0.54940.0 [37.0–46.0]40.0 [39.3–47.5]0.540Hostility42.0 [38.0–45.0]45.0 [42.0–48.0]0.07443.0 [40.0–45.0]43.0 [38.0–47.0]0.80140.0 [38.0–43.0]40.0 [40.0–42.8]0.785Phobic anxiety42.0 [40.0–45.0]43.0 [40.0–48.0]0.29542.0 [40.0–45.0]43.0 [42.0–56.0]0.09543.0 [40.0–45.0]44.0 [42.0–47.3]0.464Paranoid ideation40.0 [38.0–42.0]40.0 [38.0–51.0]0.37840.0 [38.0–44.3]40.0 [38.0–48.0]0.54638.0 [38.0–42.0]40.0 [38.0–43.8]0.405Psychoticism41.0 [39.0–45.0]45.0 [41.0–50.0]0.04944.0 [41.3–47.5]45.0 [42.0–50.0]0.16441.0 [38.0–45.0]43.5 [41.0–50.5]0.238GSI42.0 [37.0–46.5]44.0 [42.0–50.0]0.04445.0 [42.0–49.8]43.0 [39.0–58.0]0.76240.0 [37.0–44.0]41.5 [37.5–47.0]0.678PSDI41.0 [39.0–45.0]41.0 [39.0–48.0]0.97547.0 [43.3–53.5]43.0 [39.0–52.0]0.15144.0 [39.0–48.0]44.5 [37.5–48.0]0.937PST42.0 [33.5–48.0]48.0 [42.0–57.0]0.03246.0 [39.3–50.0]46.0 [37.0–58.0]0.44240.0 [35.0–43.0]44.0 [33.8–49.8]0.238Psychological profile scores are presented as t-scores from the Symptom Checklist-90-Revised (SCL-90-R), comprising nine symptom dimensions and three global indices^a^Due to incomplete responses, SCL-90-R data were available for 56 of 57 primary BMS patients, 35 of 37 secondary BMS patients, and 27 of 37 patients without burning mouth symptomsP-values were calculated using the Student’s t-test or the Mann–Whitney U test, as appropriate, for comparisons between Candida (+) and Candida (−) within each groupBM burning mouth, BMS burning mouth syndrome, C (−) oral Candida culture negative, C (+) oral Candida culture positive, GSI global severity index, I-S interpersonal sensitivity, O-C obsessive compulsive, PSDI positive symptom distress index, PST positive symptom total, Q1 25th percentile, Q3 75th percentile p < 0.05
Laboratory blood test results
No statistically significant differences were observed between Candida subgroups within either the primary or secondary BMS groups (data not shown). Among patients without burning mouth symptoms, however, the Candida-positive subgroup showed significantly lower serum albumin (p = 0.030), and higher alkaline phosphatase (p = 0.039) levels than the Candida-negative subgroup. In the total sample, the Candida-positive group exhibited significantly lower total cholesterol level (p = 0.041). In the overall BMS group, the Candida-positive subgroup also showed lower eosinophil counts (p = 0.041) and lower total cholesterol (p = 0.028) and lower serum iron (p = 0.048) levels than the Candida-negative subgroup (data not shown).
In the age-matched analyses, the primary BMS group again showed no significant differences between Candida subgroups. However, the age-matched total sample revealed lower mean corpuscular volume (p = 0.021) in the Candida-positive group, whereas in the age-matched burning mouth symptoms group, the Candida-positive subgroup had significantly higher red blood cell counts (p = 0.046) than the Candida-negative group (data not shown).
Discussion
This retrospective study examined the clinical, gustatory, salivary, psychological, and laboratory profiles of patients with taste disturbances based on burning mouth symptoms and culture-detected oral Candida status identified using a semi-quantitative screening assay, using a six-group classification. Unlike previous studies, we deliberately excluded Candida culture-positive status from the definition of secondary BMS, allowing us to isolate its potential independent contribution to taste-related outcomes. This approach enabled direct comparison of subgroups rarely distinguished in earlier work and provided new insights into how oral Candida culture-positive status may interact with neuropathic mechanisms in BMS to influence gustatory function. Notably, oral Candida culture-positive primary BMS patients displayed a distinctive gustatory profile warranting closer examination.
In this cohort, Candida culture-positive primary BMS patients exhibited no normogeusia and a significantly reduced objective taste score after age-matching, indicating a selective vulnerability of this subgroup to Candida-associated gustatory impairment. This vulnerability may reflect neuropathic alterations characteristic of primary BMS, including peripheral small-fiber dysfunction and altered taste–pain interactions, which create a sensitized baseline state [26–28]. Within this context, additional effects of oral Candida colonization may exceed functional thresholds and manifest as clinically apparent gustatory impairment [29–31].
Beyond peripheral mechanisms, a subset of primary BMS patients has been shown to exhibit central sensitization, characterized by amplified nociceptive processing and exaggerated responses to minor stimuli [32]. Within this peripherally and centrally sensitized trigeminal–gustatory network, oral Candida presence may further influence taste perception and intensify oral discomfort. Reports of taste improvement after antifungal therapy in some patients without overt candidiasis support the possibility of microbially mediated aggravation of pre-existing neural dysfunction [19, 20], although inconsistent findings across studies suggest that such effects may depend on the underlying neuropathic context of primary BMS [21]. Collectively, these findings support a potential interaction between neuropathic susceptibility and oral Candida colonization in shaping gustatory disturbances. These interpretations should be regarded as hypothesis-generating and based on observed associations rather than causal mechanisms, consistent with our finding of greater pain severity in Candida-positive patients.
Furthermore, Candida-positive patients with primary BMS and those without burning mouth symptoms exhibited significantly lower stimulated whole salivary flow rates, a difference that remained significant in the primary BMS subgroup after age-matching. This finding is consistent with meta-analytic evidence that hyposalivation increases the risk of oral Candida colonization or candidiasis by approximately threefold [33]. The relationship is likely bidirectional: reduced salivary flow impairs mechanical clearance, lowers the concentrations of antifungal proteins, including histatins, lactoferrin, and lysozyme, and reduces buffer capacity [34, 35], thereby facilitating Candida adhesion, hyphal transformation, and biofilm formation [16, 36].
Conversely, Candida infection itself may impair salivary gland function either through inflammatory involvement of the ductal epithelium or by altering local neural regulation of secretion, creating a vicious cycle of persistent colonization and salivary hypofunction [37]. Clinical data support this reciprocity, as antifungal therapy has been shown to significantly increase stimulated salivary flow rates and reduce xerostomia and tongue pain [38]. In our study, reduced stimulated salivary flow rates were consistently observed in Candida-positive patients, even in those without burning mouth symptoms, suggesting that salivary hypofunction predisposes to Candida colonization and that persistent infection, in turn, exacerbates salivary dysfunction, with potential implications for oral comfort, taste perception, and quality of life.
Psychological profiling also revealed distinct patterns. Candida-positive patients with primary BMS demonstrated higher distress scores in somatization, anxiety, and psychoticism, whereas Candida-positive patients in the total sample and overall BMS subgroup demonstrated higher phobic anxiety and psychoticism scores. The high prevalence of psychological distress in BMS—including depression and anxiety—is well established [39, 40]. Beyond this, recent evidence suggests that psychological distress-related neuroendocrine–immune pathways can modulate oral microbial ecology, impair salivary gland function and alter mucosal immunity [41]. Experimental models confirm that psychological stress promotes oral Candida albicans colonization and hyphal invasion, effects reversed by anxiolytic treatment [42]. Clinical studies in psychiatric populations similarly report oral fungal dysbiosis, including Candida overgrowth, linked to systemic immune dysregulation and heightened pro-inflammatory signaling [43].
In BMS, altered bacterial microbiota and salivary metabolites have been linked to higher anxiety and depression scores, and distinct oral microbiome profiles have been identified in BMS patients without salivary hypofunction, suggesting that microbial alterations may be intrinsic to the disorder [44, 45]. Collectively, these findings support a bidirectional model in which psychological distress increases susceptibility to Candida colonization, while Candida infection, within a peripherally and centrally sensitized trigeminal–gustatory network, further amplifies sensory disturbances and psychological burden. This perspective aligns with a biopsychosocial framework for BMS and taste disorders, in which microbial, neural, and psychological factors interact synergistically to shape clinical outcomes.
Our results highlight the importance of considering positive oral Candida culture as an independent factor in patients with taste disturbances, rather than automatically categorizing it as a cause of secondary BMS. This approach avoids misclassification and enables more targeted interventions—such as antifungal therapy, salivary stimulation, or psychosocial support—particularly for older adults with reduced salivary flow. Clinicians should recognize that Candida-related taste changes may be subtle and detectable only through objective testing.
However, this study has several limitations. First, the retrospective design limits causal inference, and unmeasured confounding cannot be excluded. Second, microbiological analysis relied on culture-based Candida detection without precise quantification, species-level identification, or assessment of strain virulence. Third, despite age-matching, other potential confounders, including medication use and systemic comorbidities, were not fully controlled. Moreover, the cohort was predominantly female and consisted mainly of middle-to-older adults, which may limit the generalizability of the findings to male patients or younger populations. Finally, the cross-sectional gustatory testing precludes determining whether Candida colonization precedes or follows taste alterations. Future studies incorporating molecular microbiome profiling, quantitative salivary biomarker diagnostics, and multiple standardized gustatory testing methods could provide more definitive evidence. Randomized controlled trials of antifungal therapy in well-stratified patient populations would be particularly valuable in clarifying the causal role of Candida in taste disturbances and burning mouth symptoms.
Conclusions
This study demonstrates that positive oral Candida culture is not universally associated with impaired taste function but may contribute to subtle gustatory deficits and reduced stimulated salivary flow in specific patient subgroups, particularly in primary BMS. Psychological distress was also more pronounced in certain Candida-positive subgroups, emphasizing the complex interplay between microbial, physiological, and psychosocial factors in oral symptomatology. By strategically excluding Candida culture-positive status from the definition of secondary BMS, we evaluated its independent impact, providing evidence to support more precise diagnostic classification and tailored management. These findings highlight the value of an integrated clinical approach that combines microbiological, salivary, gustatory, and psychological evaluations in patients with taste disturbances, particularly older adults who are at increased risk of salivary hypofunction and oral Candida colonization.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1 (DOCX 75.4 KB)