Short course of antimicrobial treatment for uncomplicated enterococcal bacteremia
Virgile Zimmermann, Nicolas Fourré, Laurence Senn, Benoit Guery, Matthaios Papadimitriou-Olivgeris

TL;DR
This study finds that short antimicrobial treatment (4–10 days) is as effective as longer treatment for uncomplicated enterococcal bacteremia.
Contribution
The study provides evidence that short-course antimicrobial treatment is non-inferior to longer regimens for uncomplicated enterococcal bacteremia.
Findings
No difference in mortality, recurrence, or joint infection was found between short and long treatment durations.
Risk factors like malignancy and sepsis were associated with worse outcomes, but treatment duration was not.
Short-course treatment (4–10 days) is reasonable for uncomplicated enterococcal bacteremia.
Abstract
Duration of treatment for uncomplicated enterococcal bacteremia is unknown. This study aims to evaluate the clinical outcomes of patients treated with short courses (4–10 days) compared to those receiving longer regimens (11–18 days). This retrospective study was conducted at the Lausanne University Hospital, Switzerland (January 2015-June 2024) and included adult patients with uncomplicated enterococcal bacteremia. Primary outcome was a composite of mortality, recurrence of bacteremia by the same enterococcal species and development of bone and joint infection within 120 days. During the study period, 331 episodes of uncomplicated enterococcal bacteremia were included. The median duration of antimicrobial treatment was 12 days (interquartile range: 8–15); 138 (42%) and 193 (58%) episodes received a short (4–10 days) and long (11–18 days) duration of antimicrobial treatment,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1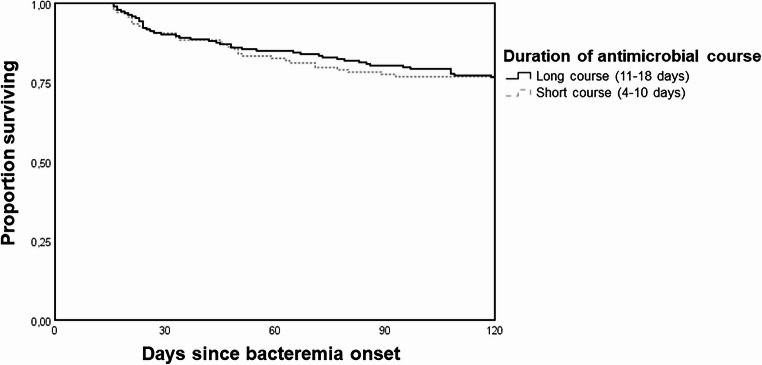 Figure 2
Figure 2- —University of Lausanne
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntimicrobial Resistance in Staphylococcus · Bacterial Identification and Susceptibility Testing · Clostridium difficile and Clostridium perfringens research
Introduction
Bacteremia remains a critical public health challenge, associated with substantial morbidity and mortality [1, 2]. Historically, most bacteremias were treated with antimicrobial regimens lasting at least 14 days [3, 4]. Over the past two decades, multiple randomized controlled trials, primarily addressing Gram-negative bacteremias, have compared short-duration treatments with traditional longer courses, consistently demonstrating similar efficacy and safety between the two approaches [5, 6].
In contrast, studies examining treatment duration for bacteremia caused by Gram-positive cocci are limited, and predominantly focus on Staphylococcus aureusbacteremia [7, 8]. Current guidelines and narrative reviews recommend a treatment duration of 7–14 days for uncomplicated enterococcal bacteremia [9, 10]. Retrospective studies have reported a median treatment duration of 10–14 days for these cases [11–14]. Only two studies have assessed the impact of treatment duration on outcomes in uncomplicated enterococcal bacteremia, both concluding that short courses were safe and not associated with treatment failure [11, 12]. However, these studies were limited to catheter-related infections and were subject to allocation bias, as shorter antibiotic durations were typically prescribed for healthier patients. The randomized BALANCE trial, which included 3,608 cases of bacteremia, with 250 attributed to enterococci, demonstrated that a 7-day antibiotic regimen for uncomplicated bacteremia caused by pathogens other than S. aureuswas non-inferior to a 14-day regimen; [6] however, no pathogen-specific analysis was conducted for the enterococcal cases.
To address the lack of evidence regarding shorter durations of antimicrobial treatment for all uncomplicated enterococcal bacteremias, this study aims to evaluate the clinical outcomes of patients treated with short courses compared to those receiving longer regimens.
Materials and methods
This retrospective study was conducted at Lausanne University Hospital, Switzerland from January 2015 to June 2024 combining two cohorts: the retrospective bacteremia cohort (January 2015 to December 2021), and the prospective cohort of patients with suspected IE (January 2022 to June 2024).
Inclusion criteria were adults (≥ 18 years old) with at least one blood culture for Enterococcus spp. and absence of patient’s decline of the use of their data. Exclusion criteria were incomplete medical records (transfer to other hospital without follow-up in our institution), absence of initiation of appropriate antimicrobial treatment within 48 h from first positive blood culture, death or instauration of palliative care within 14 days from the first positive blood culture, infection classified as complicated (those requiring a de facto duration of treatment longer than 10 days) and delay of the decision on total duration of antimicrobial treatment after day nine. Criteria for complicated disease were: infective endocarditis, bone and joint infection, deep vein septic thrombophlebitis, vascular graft infections, prostatitis, persistent bacteremia for at least 48 h, neutropenia, clinical instability at day five of bacteremia onset, polymicrobial bacteremia involving S. aureus or Candida spp., and lack of warranted source control interventions within 48 h.
Blood cultures were processed using the BacT/ALERT System (bioMerieux, Marcy l’Etoile, France) and species identification was performed using matrix-assisted laser desorption-ionization time of flight mass spectrometry (MALDI-TOF MS; Bruker Daltonics, Bremen, Germany). Susceptibility results were assessed in accordance with the EUCAST criteria [15].
Data were extracted from electronic medical records, encompassing demographics (age, sex), comorbidities, Charlson Comorbidity Index, antimicrobial treatment (intravenous, oral, duration), adverse events (allergic reactions, interstitial nephritis, and Clostridioides difficile infection), source control, presence of sepsis or septic shock, and site of infection were retrieved from patients’ electronic health records by internal medicine and infectious diseases (ID) consultants. All data were reviewed by an ID consultant.
In our institution, ID consultants were informed for positive blood cultures after species identification. For enterococcal bacteremia, ID consultation was not mandatory. Decisions on cardiac imaging studies were guided by the ID consultant, or left to the treating physician’s discretion if no ID consultation was provided [2].
The primary endpoint included mortality, recurrence of bacteremia by the same enterococcal species and the development of bone and joint infection within 120 days from the first positive blood culture. Short and long course of antimicrobial treatment was defined as 4–10 days, and 11–18 days, respectively. The date of collection of the first positive blood culture was defined as the onset of bacteremia. A new episode was included if more than 120 days had elapsed since the initial bacteremia. Bacteremia was classified as community, healthcare-associated, or nosocomial based on Friedman et al. [16]. Sepsis and septic shock were defined in accordance with the criteria proposed by the Sepsis-3 International Consensus [17]. The infection focus was determined by the ID consultants responsible for the case or, if no ID consultation was provided, by the treating physician based on clinical, radiological, microbiological, and surgical findings. Clinical stability by day five was characterized by hemodynamic stability, absence of fever, and no supplemental oxygen requirement. Documentation of the decision on the total treatment duration was recorded in ID or treating physician notes. Warranted source control measures included removal of venous catheter in patients with catheter-related bacteremia or bacteremia of unknown origin with the presence of a venous catheter, imaging-guided or surgical drainage of infected collections, and correction of urinary-tract obstruction.
SPSS version 26.0 (SPSS, Chicago, IL, USA) were used for data analyses. Fisher exact test or chi-square were used for categorical variables and Mann–Whitney U test for continuous ones. Univariate logistic regression models were assessed with 120-day primary endpoint as dependent variable. Clinically relevant non collinear covariates, assessed through variance inflation factor, were used in multivariable analysis. After checking Cox assumptions, a multivariable Cox proportional hazards regression models were performed with 120-day primary endpoint as the time-to-event. Adjusted hazard ratios (aHRs) and 95% confidence intervals (CIs) were calculated to evaluate the strength of any association. All statistic tests were 2-tailed and P < 0.05 was considered statistically significant. We finally performed Kaplan-Meier curves of the primary endpoint free probability according to duration of antimicrobial treatment.
Results
Of the 768 enterococcal bacteremia episodes, 331 episodes involving 303 patients were included (Fig. 1). From the bacteremia cohort (656 episodes), 283 (43%) had uncomplicated bacteremia. E. faecalis was the most frequently isolated species, accounting for 187 (56%) episodes. Resistance to ampicillin and vancomycin was observed in 113 (34%) and 15 (5%) isolates, respectively; all vancomycin-resistant isolates carried the vanA gene. Abdominal (139; 42%) and urinary-tract (81; 24%) were the most common foci of infection. Sepsis or septic shock occurred in 108 (45%) episodes. Follow-up blood cultures were performed in 260 (79%) episodes.
Fig. 1. Flowchart of patients’ selection
Cardiac imaging to rule out infective endocarditis was performed in 158 (48%) episodes, with the first imaging exam conducted at a median of 3 days (interquartile range [IQR]: 1–4 days) and the full diagnostic evaluation completed within a median of 4 days (IQR: 2–6 days). Transthoracic, transesophageal echocardiography, and ^18^F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography were performed in 152 (46%), 29 (9%), and 15 (5%) episodes, respectively, with 158 (48%) episodes undergoing at least one type of cardiac imaging.
The median duration of antimicrobial treatment was 12 days (IQR: 8–15), with 138 (42%) episodes receiving short course (4–10 days) of antimicrobial treatment and 193 (58%) episodes receiving long course (11–18 days). Table 1 shows the comparison of the episodes that received short and long courses of antimicrobial treatment. The median duration of intravenous antimicrobial treatment was 9 days (IQR: 7–14). Step down oral antimicrobial treatment was implemented in 66 (20%) episodes. Supplementary Table 1 shows details on the antimicrobial agents used for intravenous and oral therapy. Nine (3%) episodes presented C. difficile infection, 5 (2%) interstitial nephritis, and one (0.3%) allergic reaction.
Table 1. Comparison of episodes with short (4–10 days) and long duration of antimicrobial treatment (11–18 days)Short duration(n = 138)Long duration(n = 193) P Demographics Male sex94 (68)139 (72)0.465 Age (years)70 (57–81)72 (61–80)0.369 Age > 60 years94 (68)146 (76)0.136Co-morbidities Diabetes mellitus36 (26)63 (36)0.224 Obesity (body mass index ≥ 30 kg/m^2^)29 (21)39 (20)0.891 Chronic kidney disease (moderate or severe)29 (21)58 (30)0.076 Malignancy (solid organ or hematologic)45 (32)63 (32)1.000 Immunosuppression^a^32 (23)57 (30)0.211 Chronic obstructive pulmonary disease14 (10)19 (10)1.000 Cirrhosis13 (9)20 (10)0.854 Congestive heart failure11 (8)11 (6)0.503 Charlson Comorbidity Index5 (3–7)6 (4–8)0.221 Charlson Comorbidity Index > 479 (57)120 (62)0.426Indwelling material Prosthetic valve10 (7)11 (6)0.649 Cardiac implantable electronic device9 (7)20 (10)0.244 Vascular graft6 (4)12 (6)0.624 Arthroplasty25 (18)26 (14)0.281Setting of bacteremia onset Community32 (23)36 (19) Healthcare-associated19 (14)37 (19) Nosocomial87 (63)120 (62)1.000Microbiological data Two or more positive blood culture sets55 (40)106 (55)0.008 Pathogens E. faecalis64 (46)123 (64)0.002
- E. faecium63 (46)74 (38)0.213 Non-faecalis, non-faecium enterococci16 (12)3 (2)< 0.001 Polymicrobial bloodstream infection^b^44 (32)49 (25)0.216 Ampicillin-resistant49 (36)64 (33)0.724 Vancomycin-resistant12 (9)3 (2)0.003 Follow-up blood cultures108 (79)152 (79)1.000Infection data Fever119 (86)166 (86)1.000 Sepsis or septic shock68 (49)80 (42)0.179 Septic shock alone21 (15)23 (12)0.414 Intensive Care Unit admission31 (23)20 (10)0.003Focus of infection Unknown focus15 (11)13 (7)0.230 Catheter-related32 (23)29 (15)0.063 Abdominal infection73 (53)66 (34)0.001 Urinary-tract infection12 (9)69 (36)< 0.001 Other focus8 (6)15 (8)0.520Management Infectious diseases consultation104 (75)163 (85)0.048 Infectious diseases consultation within 48 h91 (66)148 (77)0.035 Source control Not warranted60 (44)88 (46) Warranted and performed within 48 h78 (57)105 (54)0.737Antimicrobial treatment Initiation before blood culture results106 (77)148 (77)1.000 Step down oral treatment15 (11)51 (26)< 0.001 Duration of IV antimicrobial treatment8 (6–9)14 (13–16)< 0.001 Total duration of antimicrobial treatment8 (5–9)13 (10–15)< 0.001 Adverse events Allergic reaction1 (0.7)0 (0)0.417 Interstitial nephritis1 (0.7)4 (2.1)0.406 * Clostridioides difficile infection within 120 days2 (1)7 (4)0.314Duration of hospitalization15 (9–27)15 (8–28)0.648Mortality at 30 days12 (9)17 (9)1.000Mortality at 60 days21 (15)25 (13)0.629Mortality at 90 days28 (20)34 (18)0.569Primary endpoint at 120 days32 (23)45 (23)1.000 Mortality29 (21)40 (21)1.000 Recurrence of bacteremia with the same organism4 (3)8 (4)0.767 New bone and joint infection1 (0.7)1 (0.5)1.000Data are depicted as number (%) or median (interquartile range)^a^ongoing immunosuppressive treatment at bacteremia onset, intravenous chemotherapy in the 30 days prior to bacteremia onset, AIDS, and asplenia^b^11 with multiple enterococcal species, 22 with other Gram-positive bacteria, and 74 with Gram-negative bacteria
The primary endpoint, comprising 120-day mortality, recurrence of bacteremia caused by the same enterococcal species, or development of bone and joint infections, was observed in 77 (23%) episodes; 69 episodes (21%) resulted in mortality, 12 (4%) had recurrence of bacteremia, and 2 (0.6%) developed bone and joint infection (Supplementary Table 2). There was no difference in primary endpoint between episodes treated with short and long courses of antimicrobial treatment in the whole cohort (23% versus 23%; P = 1.000), among the 187 episodes with E. faecalis bacteremia (23% versus 21%; P = 0.714), or the 155 episodes with bacteremia by other enterococcal species (24% versus 25%; P = 1.000) (Supplementary Table 3). Table 2 shows the comparison of episodes meeting and not meeting the primary endpoint. The Cox multivariable regression model (Table 3) identified malignancy (solid organ or hematologic) (P = 0.004; aHR 2.00, 95% CI 1.24–3.22), immunosuppression (P = 0.021; aHR 1.78, 95% CI 1.09–2.90), cirrhosis (P = 0.002; aHR 2.53, 95% CI 1.42–4.51), and sepsis or septic shock (P < 0.001; aHR 2.48, 95% CI 1.52–4.03) as factors associated with the primary endpoint. The duration of antimicrobial therapy was not associated with the primary endpoint (P 0.913; aHR 1.03, 95% CI 0.65–1.62).
Table 2. Comparison of episodes that did and did not Meet the primary endpoint (mortality, recurrence of enterococcal bacteremia and bone and joint infection within 120 days)No primary endpoint (n = 254)Primary endpoint(n = 77) P Demographics Male sex173 (68)60 (78)0.117 Age (years)71 (59–80)74 (58–81)0.566 Age > 60 years185 (73)55 (71)0.884Co-morbidities Diabetes mellitus72 (28)27 (35)0.260 Obesity (body mass index ≥ 30 kg/m^2^)49 (19)19 (25)0.335 Chronic kidney disease (moderate or severe)65 (26)22 (29)0.658 Malignancy (solid organ or hematologic)69 (27)39 (51)< 0.001 Immunosuppression^a^61 (24)28 (36)0.040 Chronic obstructive pulmonary disease22 (9)11 (14)0.191 Cirrhosis18 (7)15 (20)0.004 Congestive heart failure15 (6)7 (9)0.307 Charlson Comorbidity Index5 (3–7)7 (5–9)< 0.001 Charlson Comorbidity Index > 4140 (55)59 (77)0.001Indwelling material Prosthetic valve19 (8)2 (3)0.181 Cardiac implantable electronic device25 (10)4 (5)0.255 Vascular graft17 (7)1 (1)0.085 Arthroplasty38 (15)13 (17)0.719Setting of bacteremia onset Community57 (22)11 (14) Healthcare-associated44 (17)12 (16) Nosocomial153 (60)54 (70)0.139Microbiological data Two or more positive blood culture sets122 (48)39 (51)0.698 Pathogens E. faecalis146 (58)41 (53)0.515
- E. faecium*103 (41)34 (44)0.599 Non-faecalis, non-faecium enterococci14 (6)5 (7)0.781 Polymicrobial bloodstream infection^b^73 (29)20 (26)0.667 Ampicillin-resistant81 (32)32 (42)0.132 Vancomycin-resistant12 (5)3 (4)1.000 Follow-up blood cultures198 (78)62 (81)0.752Infection data Fever223 (88)62 (81)0.131 Sepsis or septic shock98 (39)50 (65)< 0.001 Septic shock alone30 (12)14 (18)0.179 Intensive Care Unit admission37 (15)14 (18)0.472Focus of infection Unknown focus19 (8)9 (12)0.248 Catheter-related48 (19)13 (17)0.740 Abdominal infection111 (44)28 (36)0.292 Urinary-tract infection62 (24)19 (25)1.000 Other focus15 (6)8 (10)0.201Management Infectious diseases consultation207 (82)60 (80)0.511 Infectious diseases consultation within 48 h187 (74)52 (68)0.311 Source control Not warranted113 (45)35 (46) Warranted and performed within 48 h141 (56)42 (55)0.897Antimicrobial treatment Initiation before blood culture results194 (77)60 (78)0.878 Duration of antimicrobial treatment Long duration148 (58)45 (58)1.000 Short duration106 (42)32 (42)Data are depicted as number (%) or median (interquartile range)^a^ongoing immunosuppressive treatment at bacteremia onset, intravenous chemotherapy in the 30 days prior to bacteremia onset, AIDS, and asplenia^b^11 with multiple enterococcal species, 22 with other Gram-positive bacteria, and 74 with Gram-negative bacteria
Table 3. Cox proportional hazard multivariable regression of 120-day composite endpoint (mortality, recurrence of bacteremia, new bone and joint infection) among patients with uncomplicated enterococcal bacteremia P aHR (95% CI)Malignancy (solid organ or hematologic)0.0042.00 (1.24–3.22)Immunosuppression^a^0.0211.78 (1.09–2.90)Cirrhosis0.0022.53 (1.42–4.51)Charlson Comorbidity Index > 40.0691.67 (0.96–2.90)Sepsis or septic shock< 0.0012.48 (1.52–4.03)Short duration of treatment0.9131.03 (0.65–1.62)CI: confidence interval; aHR: adjusted hazard ratio^a^ongoing immunosuppressive treatment at bacteremia onset, intravenous chemotherapy in the 30 days prior to bacteremia onset, AIDS, and asplenia
Kaplan–Meier analysis (Fig. 2) showed no significant difference in primary endpoint-free survival between short and long course antimicrobial treatment groups for episodes of uncomplicated enterococcal bacteremia (log-rank test: P = 0.916).
Fig. 2. Kaplan–Meier curves for primary endpoint free probability for episodes with uncomplicated enterococcal bacteremia based on the duration of antimicrobial treatment (log-rank test: P = 0.916)
Discussion
Among cases of uncomplicated enterococcal bacteremia no significant difference in clinical failure was observed between patients treated with short or long courses of antimicrobial treatment.
The median duration of antimicrobial treatment was 12 days, aligning with previous reports (median duration of 10–15 days) [11–14, 18]. Current guidelines typically recommend 7–14 days of treatment, [9, 10] but practices vary. A survey among European professionals, 85% of which were ID consultants or clinical microbiologists, reported a median treatment duration of 10 days (interquartile range: 10–14) [19]. Practices vary between countries or specialties [3, 4]. ID consultants from Germany treated for 10 days on average compared to 14 days in France [3]. Meanwhile, in Australia and New Zealand, ID consultants tended to prescribe longer courses than intensive care physicians.[4] Similarly, in the present study, longer courses were more common when patients had ID consultation (85%versus 75%; P = 0.048).
Only two prior studies specifically evaluated the impact of treatment duration on outcomes in enterococcal catheter-related bacteremia, reporting median durations of 11 and 12 days [11, 12]. These studies defined short courses differently: 7 days in the study by Bahrs et al. [11] and 9 days in the study by Marschall et al. [12] with short-course treatment used in 26% and 36% of cases, respectively. In contrast, the present study defined short courses as ≤ 10 days, with 42% of patients receiving this regimen. Both earlier studies concluded that short courses were safe and not linked to treatment failure, including mortality or bacteremia recurrence, though their retrospective design introduced allocation bias favoring healthier patients having received shorter courses [11, 12]. To address this limitation, the current study included only cases where clinical stability was achieved within five days of the initial positive blood culture and treatment duration decisions were finalized by day seven. The randomized BALANCE trial, which investigated uncomplicated bacteremias from pathogens excluding S. aureus, demonstrated noninferiority of 7-day versus 14-day antibiotic regimens, but was dominated by Gram-negative pathogens, with only 250 enterococcal cases and no pathogen-specific analysis [6].
In the present study, 120-day mortality (21%) was lower than that reported in previous studies (90-day mortality: 30–45%) [11, 12, 20, 21]. In addition to including patients who achieved clinical stability within five days, we also ensured the inclusion of those who received appropriate antimicrobial treatment within 48 h and who underwent necessary source control procedures within the same timeframe. Timely source control interventions have been previously demonstrated to significantly improve outcomes across various types of infections [22–26]. Moreover, the lower incidence of VRE (5%) in this study, compared to previous studies (34–100%), also played a role in the observed improved outcomes [12, 20, 21]. Consistent with previous findings, malignancy, immunosuppression, and cirrhosis were linked to poorer long-term outcomes, highlighting the influence of underlying comorbidities on the prognosis of patients who survived the initial period.[27, 28]However, an initial presentation with sepsis or septic shock, despite achieving clinical stability within five days, was associated with poorer long-term outcomes, aligning with findings from previous studies [29, 30].
Bacteremia recurrence within 120 days occurred in 4% of cases, with no significant difference between short- and long-course antimicrobial treatment. This rate was lower than previously reported recurrence rates (7–11% over 90 days) [12, 20, 21]. The same factors contributing to lower mortality likely influenced the reduced recurrence rates. Patients with uncomplicated E. faecalis bacteremia more frequently received longer durations of antimicrobial treatment, compared to non-E. faecalis species. This difference likely reflects the higher perceived risk of infective endocarditis with E. faecalis, despite negative diagnostic workup for endocarditis [28]. Notably, only two cases of bone and joint infections were observed within 120 days, and no cases of infective endocarditis were identified. These findings challenge the rationale for prolonged antimicrobial treatment in uncomplicated bacteremia due to non-staphylococcal Gram-positive cocci, which is often driven by concerns about recurrence or metastatic infections, as seen withS. aureusbacteremia [31].
This study has several limitations. It was a retrospective, single-center analysis with a modest sample size, though to the best of our knowledge, it represents the largest study to date on duration of treatment of uncomplicated enterococcal bacteremia and the only one not exclusively focused on catheter-related cases. Moreover, the setting in a tertiary care center with high rates of ID consultation limits generalizability. Furthermore, decisions on treatment duration may have been influenced by undocumented factors. However, patient selection was based on stringent clinical criteria, including early clinical stability, prompt source control, and finalized treatment plans by day nine. To mitigate immortal time bias inherent to retrospective studies, cases of early death or transition to palliative care within 14 days were excluded. Despite these precautions, randomized controlled trials remain essential. Currently, a multicenter, open-label, randomized trial (INTENSE) is ongoing, aiming to demonstrate that a 7-day regimen is non-inferior to 14 days for treating uncomplicated enterococcal bacteremia [32].
In conclusion, this study suggests that shorter antimicrobial courses for uncomplicated enterococcal bacteremia is a reasonable option, with no differences in long-term mortality, recurrence, metastatic infections, or treatment-related adverse events between short- and long-course regimens. These findings contribute to the growing body of evidence suggesting that antimicrobial treatment can be safely shortened in a carefully selected subset of patients with uncomplicated disease. Patients presenting with sepsis remained at higher risk of poor long-term outcomes despite initial good response. Standardized definitions of uncomplicated enterococcal bacteremia and randomized trials are urgently needed to refine treatment duration recommendations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alwan M, Davis JS, Daneman N, Fowler R, Shehabi Y, Rogers B (2019) Duration of therapy recommended for bacteraemic illness varies widely amongst clinicians. Int J Antimicrob Agents 54:184-18810.1016/j.ijantimicag.2019.05.01131085297 · doi ↗ · pubmed ↗
- 2Schnizer M, Schellong P, Rose N, Fleischmann-Struzek C, Hagel S, Abbas M, et al (2024) Long versus short course anti-MICROBIAL therapy of uncomplicated Staphylococcus aureus bacteraemia: a systematic review. Clin Microbiol Infect 10.1016/j.cmi.2024.05.01538823452 · doi ↗ · pubmed ↗
- 3Narayanan N, Rai R, Vaidya P, Desai A, Bhowmick T, Weinstein MP (2019) Comparison of linezolid and daptomycin for the treatment of vancomycin-resistant enterococcal bacteremia. Ther Adv Infect Dis 6:204993611982896410.1177/2049936119828964 PMC 637649130792858 · doi ↗ · pubmed ↗
- 4The European Committee on Antimicrobial Susceptibility Testing (2022) Breakpoint tables for interpretation of MI Cs and zone diameters. Version 12.0. http://www.eucast.org
- 5Plachouras D, Karki T, Hansen S, Hopkins S, Lyytikainen O, Moro ML, et al (2018) Antimicrobial use in European acute care hospitals: results from the second point prevalence survey (PPS) of healthcare-associated infections and antimicrobial use, 2016 to 2017. Euro Surveill 2310.2807/1560-7917.ES.23.46.1800393 PMC 624746330458917 · doi ↗ · pubmed ↗
- 6Fourre N, Zimmermann V, Senn L, Aruanno M, Guery B, Papadimitriou-Olivgeris M (2024) Predictors of mortality of streptococcal bacteremia and the role of infectious diseases consultation; a retrospective cohort study. Clin Infect Dis 10.1093/cid/ciae 168PMC 1117567738525878 · doi ↗ · pubmed ↗
- 7Papadimitriou-Olivgeris M, Senn L, Jacot D, Guery B (2024) Predictors of mortality of Pseudomonas aeruginosa bacteraemia and the role of infectious diseases consultation and source control; a retrospective cohort study. Infection 10.1007/s 15010-024-02326-6PMC 1182553138900392 · doi ↗ · pubmed ↗
- 8Papadimitriou-Olivgeris M, Monney P, Frank M, Tzimas G, Tozzi P, Kirsch M, et al (2024) Evaluation of the 2023 Duke-ISCVID and 2023 Duke-ESC clinical criteria for the diagnosis of infective endocarditis in a multicenter cohort of patients with Staphylococcus aureus bacteremia. Clin Infect Dis 10.1093/cid/ciae 003PMC 1095433138168726 · doi ↗ · pubmed ↗