Nodular Pulmonary Amyloidosis Associated With Sjögren's Syndrome
Raquel Borrego, André Soveral, Sandra André

TL;DR
A rare case of lung amyloid deposits in a man with Sjögren's syndrome is reported, highlighting the need for proper diagnosis to avoid unnecessary treatment.
Contribution
This case report adds to the understanding of nodular pulmonary amyloidosis in Sjögren's syndrome patients and emphasizes the importance of histological evaluation.
Findings
A 61-year-old man with Sjögren’s syndrome was found to have multiple asymptomatic pulmonary nodules.
Histological analysis confirmed nodular pulmonary amyloidosis with kappa light chain predominance and no systemic involvement.
Abstract
Nodular pulmonary amyloidosis is a rare entity characterized by extracellular deposits of amyloid protein in the pulmonary parenchyma, usually with a benign prognosis and often asymptomatic. We report a case of a 61-year-old man with a prior diagnosis of Sjögren’s syndrome who, during routine follow-up, was found to have multiple asymptomatic pulmonary nodules in the right lung, with uptake on positron emission tomography-computed tomography (PET CT) (SUVmax 2.11). Surgical resection was performed, and histological analysis revealed nodular deposits of amyloid protein with kappa light chain predominance, without evidence of systemic involvement. This case highlights the importance of considering nodular pulmonary amyloidosis in the differential diagnosis of pulmonary nodules in patients with Sjögren’s syndrome, emphasizing the need for histological evaluation to avoid misdiagnosis and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
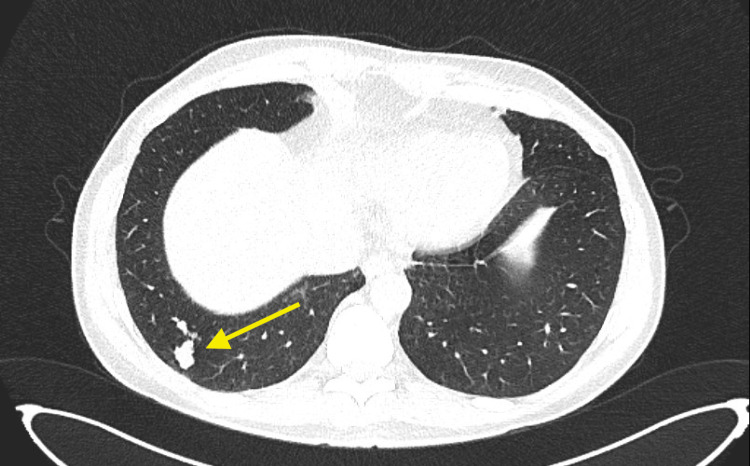 Figure 1
Figure 1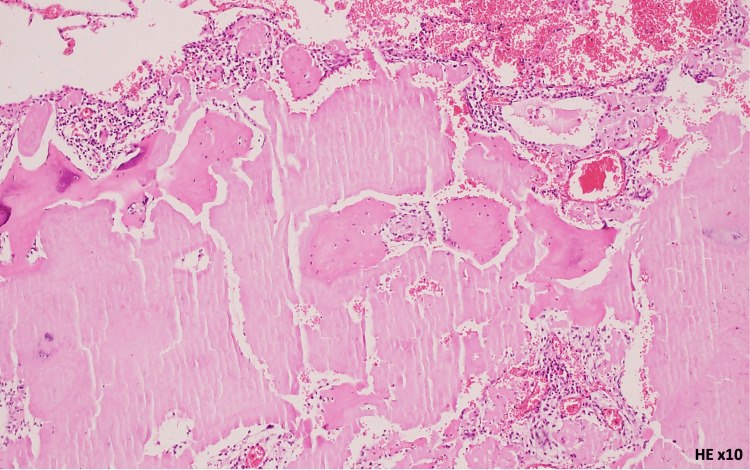 Figure 2
Figure 2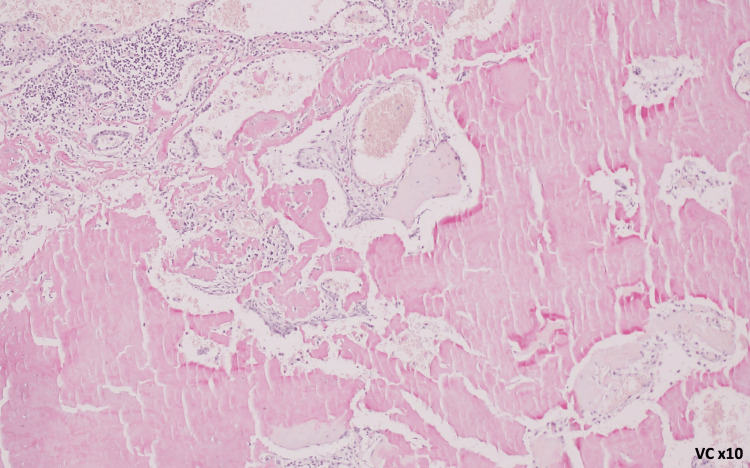 Figure 3
Figure 3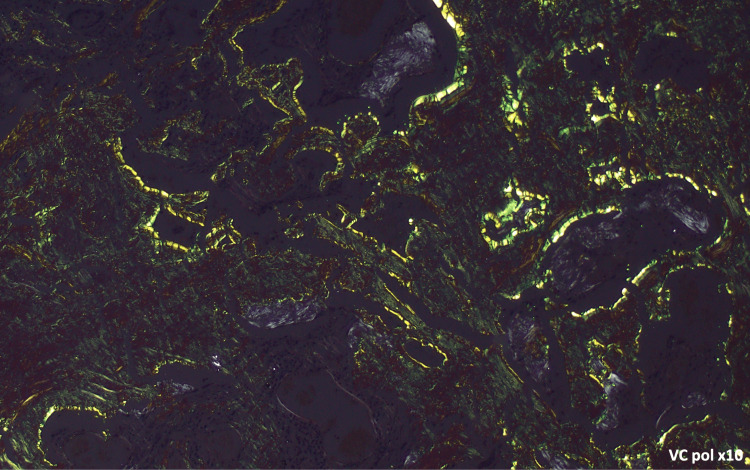 Figure 4
Figure 4| Test items | Laboratory results | Reference range |
| White blood cell (×109/L) | 5.6 | 4.0-10.0 |
| Hemoglobin (g/L) | 124 | 130-170 |
| Platelet (×109/L) | 208 | 150-400 |
| Urea (mg/dL) | 46 | 17-49 |
| Creatinine (mg/dL) | 1.2 | 0.7-1.3 |
| Sodium (mEq/L) | 140 | 136-145 |
| Potassium (mEq/L) | 4.14 | 3.5-5.1 |
| Calcium (mg/dL) | 10.1 | 8.4-10.2 |
| Total bilirubin (mg/dL) | 0.23 | <1.40 |
| Aspartate transaminase (UI/L) | 24 | <40 |
| Alanine transaminase (UI/L) | 28 | <41 |
| Gamma-glutamyl transferase (UI/L) | 11 | 10-71 |
| Alkaline phosphatase (UI/L) | 51 | 40-130 |
| C-reactive protein (mg/dL) | <0.10 | <0.50 |
| Erythrocyte sedimentation rate (mm/h) | 36 | <15 |
| Immunoglobulin G (mg/dL) | 2180 | 600-1500 |
| Immunoglobulin A (mg/dL) | 347 | 50-400 |
| Immunoglobulin M (mg/dL) | 57.9 | 50-300 |
| Serum protein electrophoresis | Polyclonal hypergammaglobulinemia | Normal pattern with no monoclonal bands |
| Serum κ light chain (mg/dL) | 524 | 170-370 |
| Serum λ light chain (mg/dL) | 220 | 90-210 |
| κ/λ ratio | 2.38 | 1.35-2.65 |
| Serum κ free light chain (mg/L) | 39 | 6.7-22.4 |
| Serum λ free light chain (mg/L) | 37.6 | 8.3-27 |
| Fκ/Fλ ratio | 1.04 | 0.31-1.56 |
| Rheumatoid factor (IU/mL) | 51 | <15 |
| Anti-nuclear antibody | >1/1280 | Negative |
| Anti-SS-A/Ro60 antibody | Strong positive | Negative |
| Anti-SS-A/Ro52 antibody | Strong positive | Negative |
| Anti-SS-B/La antibody | Strong positive | Negative |
| NT-pro Brain natriuretic peptide (pg/mL) | 45 | <300 |
| Summary of urine analysis | Negative for glucose, proteins, ketone bodies, and hemoglobin | Negative |
| Cells | Laboratory results | Reference range |
| Blast | 2.2% | 0.5-2.0% |
| Promyelocyte | 2.2% | 2.0-4.6% |
| Myelocyte | 6.4% | 8.1-16.9% |
| Metamyelocyte | 7.3% | 7.1-25.3% |
| Neutrophil | 24.8% | 16.5-36.8% |
| Eosinophil | 2.9% | 1.2-6.2% |
| Basophil | 0.2% | 0.0-0.2% |
| Monocyte | 4.4% | 0.2-5.0% |
| Lymphocyte | 13.7% | 10.8-22.7% |
| Plasma cell | 3.7% | 0.2-3.9% |
| Erythroblast | 32.2% | 20-50% |
| Myeloid/erythroid ratio | 1.6 | 1.2-5.0 |
| Myeloid series | No maturation/morphologic abnormalities | |
| Lymphoid series | Small lymphocytes with mature morphology | |
| Erythroid series | No maturation/morphologic abnormalities | |
| Megakaryocyte series | Normal number and without dysmorphias |
| Cells | Laboratory results | Reference range |
| Bone marrow immunophenotyping | ||
| Granulocytes | 64.5% | 50-65% |
| Lymphocytes | 13.9% | 10-20% |
| B lymphocytes (CD19) | 3.55% | 3-10% |
| Slg κ | 0.56% | 0.40-0.60% |
| Slg λ | 0.36% | 0.20-0.40% |
| κ/λ ratio | 1.56 | 0.8-3 |
| Plasma cells | 0.38% | <0.40% |
| Comment | No abnormal population of lymphocytes found | |
| Bone marrow biopsy | ||
| Amyloid protein (red Congo stain) | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmyloidosis: Diagnosis, Treatment, Outcomes · Medical Imaging and Pathology Studies · IgG4-Related and Inflammatory Diseases
Introduction
Pulmonary amyloidosis is a rare disorder characterized by extracellular deposition of amyloid protein in the lungs, which can be localized or part of systemic amyloidosis. In the lung, this entity can present as nodular, diffuse alveoloseptal, or tracheobronchial involvement. Nodular pulmonary amyloidosis is defined by one or more localized nodular deposits of amyloid protein in the lungs [1,2]. Nodular pulmonary amyloidosis often does not involve other organs and has a benign prognosis. In most cases, patients are asymptomatic, and nodules are incidentally detected on imaging studies [2,3]. However, this condition may be associated with lymphoproliferative disorders or autoimmune diseases such as Sjögren’s syndrome [2,4], as in this clinical case. Moreover, it may mimic other diagnoses, including malignancy [5]. Therefore, histological diagnosis and investigation of associated conditions are essential.
Case presentation
A 61-year-old man, non-smoker, with a longstanding (>10 years) diagnosis of Sjögren’s syndrome, positive for antinuclear antibodies (ANA), anti-Sjögren’s-syndrome-related antigen A antibodies (anti-SSA [Ro60]), and anti-Sjögren’s-syndrome-related antigen B antibodies (anti-SSB [La]), underwent routine computed tomography (CT) of the chest, which revealed multiple solid peripheral nodules with lower predominance in the right lung measuring 0.8-2.0 cm (Figure 1).
Chest CT with multiple nodulesChest CT with multiple nodules 0.8-2.0 cm. Arrow points to a solid nodule in the right lung.
The patient had no respiratory symptoms, sicca symptoms, or abnormal findings on physical examination, and no family history of pulmonary disease. The patient was not under any medication. Given the presence of these nodules and the suspicion of malignancy, PET/CT was performed, showing mild homogeneous uptake in the same nodules (SUVmax 2.11). A transthoracic lung biopsy was considered but was technically not feasible due to the interposition of anatomical structures. Following multidisciplinary discussion, the patient underwent atypical resection of the right upper and lower lobes with lymph node sampling via video-assisted thoracoscopic surgery (VATS) without immediate or later complications. Histopathological analysis of the lung parenchyma revealed nodules composed of eosinophilic, amorphous material, occasionally associated with calcifications. Amyloid deposits were confirmed by Congo red staining, demonstrating apple-green birefringence under polarized light, with a predominance of kappa chains on immunohistochemistry, without features suggestive of mucosa-associated lymphoid tissue lymphoproliferation or plasmacytoma (Figures 2-4). The biopsy is consistent with nodular pulmonary amyloidosis.
Amyloid substance: amorphous eosinophilic material (hematoxylin-eosin stain, ×10 magnification)
Amyloid substance: amorphous material highlighted in red by the Congo red histochemical technique (×10 magnification)
Amyloid substance: amorphous material demonstrated by Congo red histochemical staining with apple-green birefringence under polarized light (×10 magnification)
Systemic evaluation followed with blood analysis, including a liver panel, bone marrow evaluation, serum immunoglobulins, and serum protein electrophoresis (Tables 1-3). The patient also underwent an echocardiogram, which was normal. Since surgery, the patient has remained under follow-up (1.5 years) without development of new nodules.
Discussion
Sjögren's syndrome is a chronic systemic autoimmune exocrinopathy characterized by lymphocytic infiltration and progressive destruction of exocrine glands, predominantly the lacrimal and salivary glands. Pathologically, it is defined by focal lymphocytic sialadenitis with periductal aggregates of CD4⁺ T cells, B cells, and plasma cells within salivary gland tissue, often accompanied by B-cell hyperactivity and autoantibody production, particularly anti-SSA/Ro and anti-SSB/La antibodies.
The treatment for Sjögren syndrome is individualized and depends on the severity and type of manifestations. The first line of treatment is symptomatic (sicca symptoms and pain), and in severe extraglandular manifestations, systemic immunosuppressive therapy is used. The most frequent complication of systemic immunosuppressive therapy is infection, followed by malignancy. Also, patients with primary Sjögren's syndrome have a two-to-four-fold increased risk of overall malignancy compared with the general population and a 10- to 20-fold increased risk of lymphoma.
As a systemic disease, Sjögren's syndrome is associated with multiple pulmonary manifestations, with interstitial lung disease being the most frequent [6]. Nodular pulmonary amyloidosis as a manifestation of Sjögren's syndrome is rarely reported. Many cases of pulmonary amyloidosis, especially asymptomatic ones, are incidentally detected on imaging studies [7].
It is essential to differentiate nodular pulmonary amyloidosis from other causes of nodules, including malignancy and infection, given the implications for treatment and prognosis [8].
On imaging, nodular pulmonary amyloidosis may present as solitary or multiple nodules, sometimes with cavitation or calcifications, generally showing slow growth. However, these findings can mimic primary or metastatic neoplasms as well as infections, obscuring the differential diagnosis. Therefore, imaging alone is insufficient for diagnosis, as different entities can produce similar findings on CT and PET scans [9]. Definitive diagnosis of nodular pulmonary amyloidosis requires histopathological confirmation of amyloid deposition using Congo red staining, which demonstrates apple-green birefringence under polarized light [1-3]. In addition to diagnostic confirmation, it is crucial to exclude systemic involvement.
In the present clinical case, the development of pulmonary nodules in an asymptomatic patient with an autoimmune disease raised concern for malignancy. Also, due to the number and size of the nodules, the suspicion of malignancy was elevated.
For the study of malignancy, the patient underwent PET/CT, which showed mild homogeneous uptake in the same nodules (SUVmax 2.11). There is no universal cutoff value for the maximum standardized uptake value (SUVmax) in PET scans, as the optimal threshold varies by clinical context, organ system, and disease. However, in the evaluation of mediastinal and hilar lymph nodes for malignancy, a commonly used cutoff is 2.5, but this value is associated with high sensitivity and low specificity.
After ascertaining the need for nodule sampling, a multidisciplinary discussion between Radiology, Pulmonology, and Thoracic Surgery followed. Due to the location of the nodules, percutaneous thoracic biopsy was not feasible because of the interposition of other anatomical structures, and bronchial fibroscopy could not reach the nodules. Therefore, it was determined that a surgical approach was the best option to sample the nodules.
The patient underwent atypical resection of the right upper and lower lobes with lymph node sampling via VATS, which obtained the needed material.
The malignant hypothesis was excluded by histological evaluation of the surgical specimen. The histology revealed deposits of amyloid protein, raising the question of pulmonary versus systemic amyloidosis (Figures 2-4).
Amyloidosis is a group of disorders characterized by extracellular deposition of misfolded proteins (amyloid fibrils) in tissues and organs, leading to progressive disruption of normal structure and function. The major biochemical types are classified by their deposits: AL (light-chain) amyloidosis, ATTR (transthyretin), AA (amyloid A protein), Aβ₂M (dialysis-related), and Aβ in Alzheimer's disease. Clinically, amyloidosis can be categorized by distribution as systemic or localized.
To exclude systemic amyloidosis, the patient underwent echocardiography and NT-proBNP assay to exclude cardiac involvement, a liver panel with normal hepatic function to exclude liver involvement, and urine and renal function testing to exclude kidney involvement. Hematologic evaluation was also performed with immunologic and serologic blood work plus bone marrow study.
In the present case, the patient had no involvement of other organs, so pulmonary amyloidosis was assumed. Most cases of nodular pulmonary amyloidosis associated with Sjögren's syndrome are localized, and treatment is generally conservative, as most lesions remain stable over time without progression. Surgical excision may be considered for diagnostic or symptomatic lesions and is usually curative. Long-term prognosis is excellent, with rare recurrence or progression to systemic disease [1,5].
Long-term follow-up with chest CT, complete blood count, renal and liver function tests, and NT-proBNP is recommended, as rare cases progress or are associated with mucosa-associated lymphoid tissue lymphomas [10].
Conclusions
Nodular pulmonary amyloidosis should be considered in the differential diagnosis of pulmonary involvement in Sjögren’s syndrome and in the evaluation of pulmonary nodules. This case illustrates a rare association between these two entities.
Even though the biopsy may be technically challenging, histology is required to avoid misdiagnosis and overtreatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Amyloidosis of the lung Arch Pathol Lab Med Khoor A Colby TV 24725414120172813458710.5858/arpa.2016-0102-RA · doi ↗ · pubmed ↗
- 2The lung in amyloidosis Eur Respir Rev Milani P Basset M Russo F Foli A Palladini G Merlini G 26201710.1183/16000617.0046-2017 PMC 948892028877975 · doi ↗ · pubmed ↗
- 3Pulmonary amyloidosis. The Mayo Clinic experience from 1980 to 1993 Ann Intern Med Utz JP Swensen SJ Gertz MA 4074131241996855424910.7326/0003-4819-124-4-199602150-00004 · doi ↗ · pubmed ↗
- 4Pulmonary calcified nodules and cysts as the initial presentation of Sjögren's syndrome secondary nodular pulmonary amyloidosis: a rare case report BMC Pulm Med Jin Y Zhang C Zhu X Fang Z 4272520254099941310.1186/s 12890-025-03876-7PMC 12465482 · doi ↗ · pubmed ↗
- 5Mimicking pulmonary multiple metastatic tumors: a case of primary nodular parenchymal pulmonary amyloidosis with review of the literature Oncol Lett Zhang LN Xue XY Wang N Wang JX 13661370420122320513710.3892/ol.2012.923PMC 3506749 · doi ↗ · pubmed ↗
- 6Diagnosis and management of lung involvement in systemic lupus erythematosus and Sjögren's syndrome: a literature review Ther Adv Musculoskelet Dis Depascale R Del Frate G Gasparotto M 175972013202110.1177/1759720 X 211040696 PMC 848852134616495 · doi ↗ · pubmed ↗
- 7Amyloid-associated cystic lung disease Chest Zamora AC White DB Sykes AM Hoskote SS Moua T Yi ES Ryu JH 1223123314920162651352510.1378/chest.15-1539 · doi ↗ · pubmed ↗
- 8A descriptive analysis of 21 patients with pulmonary amyloidosis: an observational study Medicine (Baltimore) Demirkol B Satici C Eren R 0103202410.1097/MD.0000000000040535 PMC 1155696439533551 · doi ↗ · pubmed ↗