The influence of paternal preconception health on infant birth weight: A scoping review
Cindy-Lee Dennis, Karen McQueen, Justine Dol, Alistair Dennis-Grantham, Daisy R. Singla, Julia Carneiro Godoy de Sousa, Tina Montreuil, Catherine S. Birken, Shefaly Shorey

TL;DR
This review explores how a father's health before conception may affect a baby's birth weight, highlighting areas needing more research.
Contribution
The study is the first scoping review to systematically examine the relationship between paternal preconception health and infant birth weight.
Findings
Paternal factors like BMI, drug use, and environmental exposures may influence infant birth weight.
Evidence is mixed for the impact of paternal nutrition, sleep, and mental health on birth weight.
Most studies were from China and the US, suggesting a need for more global research.
Abstract
Birth weight is an important determinant of infant growth and development associated with neonatal morbidity (e.g., respiratory distress, hypoglycemia) and mortality, as well as long-term health risks such as developmental delays and chronic conditions (e.g., asthma, type 2 diabetes) in later life. These adverse health outcomes are particularly concerning when infants are born small or large for their gestational age. A potential strategy to improve optimal birth weight is preconception care, with consistent evidence demonstrating a relationship between maternal preconception health and infant birth weight. However, little attention has been given to the influence of paternal preconception health on pregnancy outcomes. This scoping review aimed to capture the existing literature and highlight evidence gaps regarding associations between paternal preconception health and infant birth…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
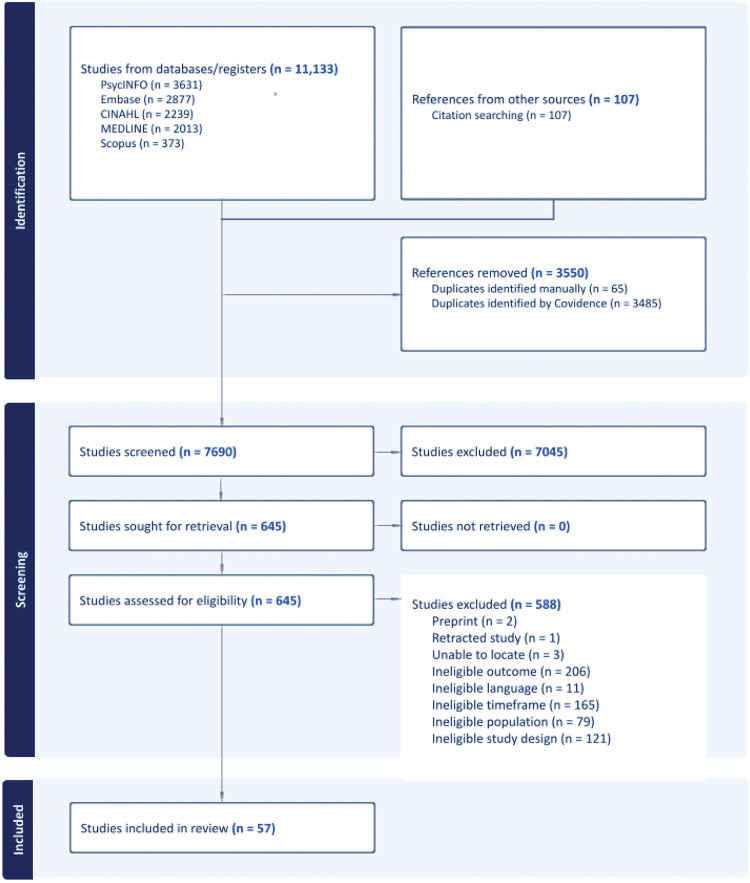 Fig 1
Fig 1- —http://dx.doi.org/10.13039/501100000024Canadian Institutes of Health Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGestational Diabetes Research and Management · Reproductive Health and Contraception · Birth, Development, and Health
Introduction
Background
Birth weight is a key determinant of neonatal health and a strong predictor of both short- and long-term developmental outcomes such as growth stunting, lower IQ and mortality [1–3]. Concerns arise when infant birth weight falls on either end (low birth weight [LBW] or high birth weight [HBW]), as both are associated with short- and long-term risks [4]. Low birth weight is a global problem affecting more than 20 million infants annually. Although the highest rates of LBW are seen in low-and middle-income countries [5], it is also a substantial concern in high-income countries because it impacts child health outcomes [6]. Infants with LBW are 20 times more likely to die compared to normal birth-weight infants [3]. Additionally, infants with LBW face considerable morbidity, including neonatal complications and an increased risk of long-term cognitive, neurological, developmental, mental, and physical impairments [1,6,7].
High birth weight, known as macrosomia, is also a significant problem [8,9]. Excessive fetal growth can be associated with increased short- and long-term risks for the mother and the infant [2]. A systematic review of maternal and neonatal complications found that pregnancies with macrosomia had a higher risk of emergency caesarean section, postpartum hemorrhage, and obstetric injury [10]. For the neonate, there was an increased risk of shoulder dystocia, obstetric brachial plexus injury, and birth fractures. Additionally, HBW is associated with greater long-term child health risks, such as obesity and metabolic syndrome [2].
A wide range of maternal factors have been associated with LBW, including sociodemographic disadvantage, obstetric complications, chronic health conditions, lifestyle behaviors, and environmental factors [11–13]. As such, LBW is widely recognized as an important indicator of maternal health, nutrition, healthcare delivery, and poverty [1]. This is reflected in the varying prevalence rates of LBW among low-middle- and high-income countries. In contrast, HBW is predominately driven by metabolic and nutritional factors with maternal obesity, gestational diabetes mellitus, and excessive gestational weight gain consistently identified as the principal factors [4].
One potential strategy to promote optimal birth weight is preconception care [14,15]. Preconception care aims to improve an individual’s (male or female) health during their reproductive years by reducing risk factors, promoting healthy lifestyle behaviours, and increasing readiness for pregnancy [16]. Addressing risks before pregnancy is ideal because it allows time to change unhealthy behaviours, such as physical inactivity or smoking, and improve health before embryonic development [17]. Emerging research suggests that when preconception health interventions effectively increase health knowledge (e.g., nutrition, chronic disease management) and behavioural change (e.g., smoking, obesity), pregnancy and neonatal outcomes may improve [16–18].
While existing evidence demonstrates a robust relationship between maternal preconception health and infant birth weight [14,15], there has been a limited focus on how paternal preconception health influences outcomes. A recent review assessed modifiable paternal health variables and risk factors in the preconception period and found a trend that higher paternal BMI was associated with higher offspring birth weight [19]. The authors concluded that the positive associations between increasing paternal BMI and infant birth weight may be due to paternal sperm quality and potential changes in sperm epigenetic profiles, and that further research was warranted. A limitation of the review was that it focused on modifiable factors, and other factors, such as paternal health (e.g., comorbidities) and treatments (e.g., medications) were excluded. Paternal physical health, such as diabetes [20], metabolic syndrome [21], and some treatment medications [22] have been associated with sub-optimal birth weight outcomes. Similarly, paternal preconception exposure to some environmental or occupational toxins have been associated with lower birth weight [23,24]. However, several studies have found no association between these paternal variables and birth weight [25–27]. Emerging research suggests that paternal preconception health may impact fertility and the genetic contribution to offspring [28,29], thus a broader examination and synthesis of paternal factors is warranted. Due to the significant health risks associated with high and low birth weight [6,7,9], it is essential to examine paternal preconception health and infant birth weight to develop comprehensive preventative preconception care.
Review objective
This review was conducted as part of HeLTI Canada (www.helticanada.com), an innovative preconception trial targeting child obesity [30]. The overarching scoping review was focused on the influence of paternal preconception health factors on perinatal and early childhood outcomes (see published protocol) [31]. Due to the large number of studies and varying outcomes in the full review, the specific objective of this review was to identify, consolidate, and synthesize the literature on paternal preconception health and infant birth weight.
Materials and methods
Design
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) extension for Scoping Reviews (PRISMA-ScR) [32] and the Joanna Briggs Institute (JBI) methodology for scoping reviews [33]. It also follows a published protocol [31]. Ethical approval was not applicable.
Search strategy
A multi-step process was followed to identify published studies. First, the search keywords were refined and specified, and a preliminary search of the Web of Science was conducted. Second, assistance from an experienced health science librarian was sought to ensure the accuracy of the search keywords and the resulting search strategy (S1 Table). The final search strategy was adapted for each database, including MEDLINE All (Ovid), Embase (Elsevier), CINAHL Full Text (EBSCO), Scopus (Elsevier), and PsycINFO (EBSCO). We also conducted a manual search of the reference lists of included studies for additional articles, ensuring that no relevant articles were missed. The search was conducted on January 16, 2024 and updated on June 30, 2024.
Inclusion and exclusion criteria
The review considered studies that included: [1] men who identified as the contributing reproductive partner for a child, [2] male preconception health exposure data, and [3] infant birth weight outcomes. Studies that solely reported on maternal exposures or did not separate paternal exposures were excluded. This review considered all English-language quantitative and qualitative studies (prospective and retrospective), including mixed methods. However, experimental studies evaluating intervention effectiveness were excluded because the review aimed to evaluate naturally occurring paternal preconception health characteristics rather than the effects of targeted interventions. Observational studies are therefore the most appropriate design for addressing our review question. Review articles, letters to the editor, editorials, commentaries, conference abstracts, dissertations, books, book chapters, and grey literature were also excluded to ensure that only peer-reviewed articles evaluating associations were included. Finally, only studies published from 2013 were included to synthesize the current evidence. The year 2013 was chosen because it reflected the past decade of research on the topic at the time the initial search was conducted.
Concept definition.
Birth weight is typically defined as the first weight of a newborn obtained after delivery. Within the included studies, birth weight was often categorized as: low birth weight (LBW) (less than 2,500 grams); normal birth weight (2,500–3,999 grams); or high birth weight (HBW) (4,000 grams or more). This classification reflects the newborn’s absolute birth weight, independent of gestational age. As such, some studies categorized birth weight by gestational age and SGA or LGA status.
Study selection
All citations identified in the search were uploaded to Covidence [34], and duplicates were removed. Prior to the full review of title/abstracts, one reviewer piloted the inclusion/exclusion criteria to ensure that the list of reasons for exclusion was clearly outlined to minimize potential confusion and conflict among reviewers. After this pilot, two reviewers screened the titles and abstracts, then the full texts of potentially relevant studies, with disagreements resolved through discussion or by a third reviewer. Reasons for exclusion at the full-text stage are reported.
Data extraction and synthesis
Data extracted from full-text articles included specific information, such as study design, sample size, participants, methods, paternal preconception exposures and measurements, and primary outcome results. Two reviewers extracted full data, which a third reviewer verified. Data were then organized and summarized by paternal preconception health exposures and infant birth weight. No quality appraisal was undertaken, consistent with the scoping review methodology [35].
Results
Search results
A total of 11,240 citations were retrieved from five databases and citation searching. After removing duplicates, the titles and abstracts of 7,690 citations were reviewed. Full-text screening was conducted for 645 studies, of which 57 were deemed eligible for inclusion. The search results and reasons for exclusion are reported in a PRISMA flow diagram (Fig 1). The most common reasons for exclusion were ineligible outcome (e.g., not infant birth weight), ineligible time frame (e.g., not pre-conception period), and ineligible study design (e.g., abstract, editorial).
PRISMA flow diagram.
Study and population characteristics
All 57 included studies were published between 2013 and 2024, with 35 (61.4%) published in the last 5 years (Table 1). Most studies were conducted in China (n = 18, 31.6%) or the United States (US) (n = 17, 29.8%), with the remaining studies primarily from developed European countries (n = 16, 28.1%). Almost all were cohort studies (n = 54, 94.7%) that utilized diverse recruitment settings, including population-based samples identified through social media, large data sets, hospitals, and community clinics.
Table 1: Characteristics of included studies.
Data synthesis
The paternal preconception health categories identified in this review included physical well-being, health behaviours, substance use, environmental exposures, mental health, and treatment effects. The reporting of infant birth weight was highly variable. Many studies operationalized birth weight by gestational age (LGA or SGA); others reported infant weight as LBW, macrosomia (>4000 grams; yes/no) or in specific grams. For our review, we utilized the definitions provided in the studies.
Physical well-being
Body mass index (BMI).
Seventeen studies reported on the influence of paternal BMI on infant birth weight. While the findings were mixed, most (n = 12 of 17, 70.6%) identified a significant association (Table 2).
Table 2: Synthesis of significant associations.
Paternal preconception BMI and HBW.
In 10 studies, researchers reported paternal BMI was associated with increased infant weight [36–45]. Two large cohort studies conducted in China found that paternal preconception overweight and obesity were significantly associated with macrosomia (p = 0.038 and p < 0.001, respectively) [40], with infants of obese fathers 1.7 times more likely to be macrosomic at birth (95%CI: 1.168, 2.444) [39]. Similar results were found in a case-control study of 6,341 Chinese fathers, where infant macrosomia was higher among fathers who were overweight (aOR=1.33; 95%CI: 1.11,1.59) and obese (aOR=1.99; 95%CI: 1.49, 2.65) [44]. In a retrospective cohort study of 4.7 million Chinese couples, overweight (OR=1.08; 95%CI: 1.06, 1.09) and obese (OR=1.19; 95%CI: 1.17, 1.20) fathers had a significantly increased odds of LGA infants, while underweight fathers had a significantly higher odds (OR=1.17; 95%CI: 1.15, 1.19) of SGA infants compared with fathers with normal BMI [37], after adjusting for potential covariates. Three additional Chinese cohort studies reported multiple HBW outcomes. One large study (n = 2,075 fathers) found paternal overweight status to be associated with LGA (aOR=1.70; 95%CI: 1.05, 2.74) and paternal obesity to significantly increase the likelihood for very LGA (aOR=2.58; 95%CI: 1.03, 6.45) and macrosomia (aOR=3.28; 95%CI: 1.33, 8.09) [45]. Two additional studies with 7,908 [41] and 1,609 [38] fathers confirm paternal preconception overweight and obesity significantly increase the odds for LGA and macrosomia compared to normal BMI controls after adjusting for confounders.
Three studies found a positive relationship between paternal BMI and increased birth weight [36,42,43]. In a cross-sectional study of 750 Pakistani fathers [36], those who were overweight had infants with significantly higher birth weights (2952.14 ± 53.64g) when compared with those in the non-overweight group (2577.24 ± 30.94g). In a longitudinal US cohort study with 429 fathers, paternal BMI (≥25.0 kg/m2) was significantly associated with increased birth weight compared to those with a BMI < 25 (mean [SD] z score, 0.38 [0.91] vs 0.11 [0.96]; p = .004) [42]. Lastly, in a cohort of 1,810 Chinese fathers, each standard deviation increment of paternal BMI was associated with an additional increase in birth weight (aOR=29.6; 95%CI: 5.7, 53.5) that was sex-specific to male infants only [43].
Paternal preconception BMI and low infant birth weight
Three studies in China reported an association between increased paternal preconception BMI and low infant birth weight [39,49,50]. A prospective cohort study that included 7,683 fathers found that paternal obesity was significantly associated with SGA infants (SGA; OR=2.866; 95%CI: 2.091, 3.930), while paternal low BMI (underweight) was also associated with SGA in infants (OR=8.506; 95%CI: 5.784, 12.509) [39]. Paternal pre-pregnancy BMI (n = 34,104) was associated with LBW among overweight (aOR=1.50; 95%CI: 1.36, 1.64) and obese (aOR=1.36; 95%CI: 1.19,1.54) fathers [49]. Very LBW was also associated with overweight (aOR=1.31; 95%CI: 1.10, 1.56) and obese (aOR=1.31; 95%CI: 1.04, 1.65) fathers. Similarly, paternal BMI (n = 34,104 fathers) was identified as a risk factor for LBW (OR=1.346; 95%CI: 1.117, 1.622) among fathers who were overweight [50].
Paternal preconception BMI and no association with infant birth weight
Five studies reported no associations between paternal preconception BMI and birth weight [20,25,46–48]. In the first US study that included 1,889 fathers, there was no statistically significant difference in infant birth weight among paternal BMI groups in the overweight, obesity, and normal categories [25]. In the other US study (n = 372 fathers), paternal overweight (OR=35.6; 95%CI: −140.0, −211.3) and obesity (OR=76.8; 95%CI: −74.6, −228) were not significantly associated with infant birth weight [20]. Data from 2,264 in a prospective population-based birth cohort found paternal BMI was also not associated with SGA (OR=0.96; 95%CI: 0.91, −1.01) [47]. Similar results were found in a sample of 1,292 fathers from China [48] and 1,778 fathers from Australia [46].
Physical health
Four studies examined the relationship between paternal physical health and birth weight [20,21,51,52]. Two studies conducted in the US noted an association between paternal physical health and infant birth weight. In the first large cohort study (n = 785,809 live births), paternal comorbidity with all or most components of metabolic syndrome was associated with 23% higher odds of an infant with LBW (95%CI: 1.01, 1.51) [21]. In the study by Moss and Harris [20], researchers found that birth weight was lower among infants born to fathers with diabetes compared to those born to fathers without the condition (difference = −783.9; 95%CI: 1014.2, 553.6, p < 0.01). Two studies in China found no association between infant birth weight and fathers with chronic disease [51] andsupp tuberculosis [52].
Health behaviours
Nutrition.
Two studies investigated the impact of paternal preconception nutritional status on birth weight [20,53]. A cohort study in the US found no significant relationship between paternal folate intake and birth weight or risk for SGA after multivariable adjustments [53]. Likewise, Moss and Harris [20] evaluated the frequency of fathers’ fast-food consumption and found no association between this dietary pattern and birth weight.
Sleep quality.
In a retrospective cohort study, researchers evaluated the association between paternal sleep quality and birth outcomes among 282 couples undergoing ART in China [54]. While there was no statistically significant difference in birth weight between the poor and good sleep groups, multivariate analysis revealed that the global sleep quality score negatively influenced birth weight (β=−63.81; 95%CI: 119.91, 8.52, p = 0.047).
Physical activity.
Two studies examined the influence of paternal physical activity on birth weight [20,47]. In a US cohort study, Moss and Harris [20] investigated the frequency of activity bouts in the past week and found no significant association with birth weight. Similarly, in the population-based cohort study, Mutsaerts et al. [47] assessed physical activity levels, defining positive activity as engaging in moderate-intensity exercise for at least 30 minutes at least once a week. Their results showed no independent association between paternal physical activity levels and birth weight.
Substance use
Recreational drugs.
One population-based retrospective cohort study (n = 18,678) linked to the national database in Taiwan demonstrated that paternal preconception use of illegal drugs within one year (−115.05g, 95%CI: −223.89, −6.21) or two years (−128.33g, 95%CI: −254.05, −2.6) was significantly associated with LBW compared to unexposed infants [55]. In a smaller US prospective cohort study, paternal use of marijuana or other drugs within the last year was not associated with birth weight [20].
Smoking.
Five studies examined paternal preconception smoking and birth weight outcomes, and none demonstrated a direct or independent effect on birth weight outcomes [20,47,51,56,57]. A large longitudinal cohort study in Taiwan investigated paternal smoking during different stages of pregnancy with birth weight. They found that paternal preconception smoking was not associated with LBW or SGA [57]. Likewise, Mutsaerts [47] found no association between paternal daily smoking and SGA. The three remaining studies evaluated paternal smoking over the last 30 days [20], smoking dichotomized as yes/no [51] and smoking 1–10 cigarettes/day vs > 10/day [56] and found no association with birth weight.
Alcohol.
Four cohort studies analyzed paternal preconception alcohol use and birth weight [20,47,51,58]. These studies found that paternal alcohol consumption was not associated with infant birth weight. In one US study [20], alcohol use was dichotomized to drinking once per month or less compared to more frequently. No significant difference was found regarding birth weight in the bivariate analysis with paternal alcohol use. In another study [47], data on paternal alcohol consumption (units per week) were collected with univariable and multivariable logistic regression analyses suggesting paternal alcohol use did not independently influence SGA. Likewise, two cohort studies conducted in China with 829 infants [51] and 980 infants [58] examined paternal alcohol use (yes/no) and LBW at birth and found no differences between groups.
Environmental exposures
Persistent organic pollutants.
Two cohort studies in the US evaluated paternal preconception exposure to various persistent organic pollutants and their impact on birth weight [23,59]. In the first study, higher paternal urinary levels of cesium (β = −237.85, 95%CI −463.04, −12.66), uranium (β = −187.34, 95%CI: −366.34, −8.35), zinc (β = −209.08, 95%CI: −417.40, −0.77) and chromium (2nd tertile: β = −140.52, 95%CI: −317.40, 36.35, 3rd tertile: β = −144.33, 95%CI: −343.28, 54.62) were associated with lower birth weight [23]. Conversely, a higher paternal urinary arsenic level was associated with higher birth weight (β = 194.71, 95%CI: 17.13, 372.30). In the other study, researchers evaluated paternal preconception exposure to 63 persistent organic pollutants among 234 infants [59]. Serum concentrations of polychlorinated diphenyl ether-183 and polychlorinated biphenyls-167 were associated with lower birth weight among 116 girls [(β = –92.13 g; 95%CI: –173.44, –10.82) and (β = –97.49 95%CI: –187.45, –7.54), respectively]. Among boys (n = 113), serum concentrations of several persistent organic pollutants were also associated with lower birth weight (range, 98–170 g).
Phthalates.
Five cohort studies evaluated paternal preconception exposure to phthalates, with four studies finding an association between paternal phthalate exposure and birth weight [24,60–63]. In a US cohort of 195 fathers, researchers found a significant negative association between paternal urinary concentration of one metabolite (sum of di[2-ethylhexyl]) phthalate (ΣDEHP) and birth weight [24]. Another US study evaluated paternal preconception urinary concentrations of 14 phthalate metabolites and infant birth weight [61]; only paternal monoethylhexyl phthalate (mEHP) was associated with a 191.93 g decrease in birth weight (95%CI: −381.61, −2.25). A third US study examined phenol and phthalate metabolite exposure to birth weight among offspring born to sub-fertile couples [63]. Multivariable linear models revealed a 63g (95%CI:–134, 7) and 73g (95%CI: –141, –5) decrease in birth weight was associated with each unit increase in paternal scores of the DEHP metabolites-BPA factor and low molecular weight phthalate factor, respectively. In a study in China [62], higher paternal prenatal concentrations of mono-benzyl phthalate (aRR = 1.40; 95%CI:1.04, 1.87) and mono-carbocisononyl phthalate (aRR = 1.53; 95%CI: 1.12, 2.09) were associated with an increase in LBW risk among spontaneously conceived offspring. Among ART-conceived offspring, the adjusted relative risk was lower for LBW with exposure to MnBP, mono-3-carboxypropyl (MCPP), mono-2-ethylhexyl (MEHP), and mono-2-ethyl-5-hydroxyhexyl (MEHHP). Finally, the fifth US study did not find a significant association between paternal DEHP concentrations and the birth weight: placental weight ratio [60].
Phenols.
Two US cohort studies evaluated paternal urinary phenol concentrations [26,64]. In the first study, researchers evaluated paternal preconception urinary phenol levels and birth weight among 346 single offspring [64]. For each log-unit increase in paternal preconception benzophenone-3 concentration in adjusted models, birth weight increased significantly by 137g (95%CI: 60, 214). In the second study, researchers evaluated paternal preconception urinary bisphenol concentration and birth weight (n = 346 infants) and found no association [26].
Other chemicals.
One US cohort study examined the relationship between birth weight and paternal preconception serum concentrations of polychlorinated biphenyl (PCB) and polybrominated biphenyl (PBB). In the US cohort study (n = 336 infants), the adjusted models revealed that an increase in paternal preconception serum concentrations of PCB and PBB were associated with increased risks of lower birth weight [65]. Another US cohort study evaluated paternal preconception serum concentrations of nine perfluoroalkyl and polyfluoroalkyl substances (PFAS) and birth weight among 312 infants [66]. Paternal preconception serum concentrations of perfluorooctanesulfonate (β:147.81g, 95%CI: − 7.90, 303.52) and perfluorohexanesulfonate (β:127.13g, 95%CI: −2.75, 257.00) were associated with higher birth weight; however, the relationships may have been imprecise due to the small sample size (n = 145) [66].
Radiation.
One cohort study in China evaluated paternal exposure to radiation (e.g., x-ray, CT, PET-CT) (n = 192,492) and birth weight [67]. Researchers found that paternal preconception exposure to radiation was associated with LBW (OR=1.54; 95%CI:1.08, 2.18). However, the average birth weight of infants in both the exposed and unexposed groups was within normal limits.
Mental health
Depression.
Three studies examined the association between paternal mental health and birth weight with mixed findings [20,21,68]. A large US cohort study using diagnostic codes from inpatient and outpatient records found that fathers with a history of depression the year before pregnancy had an increased odds of having a LBW infant (OR=1.18; 95%CI:1.12, 1.24) [21]. Conversely, no associations were observed among 421 men with persistent preconception common mental disorder symptoms and SGA [68]. Likewise, Moss and colleagues [20] found no association between paternal depression and birth weight. The researchers also noted a low degree of participants with depression within their study.
Treatment effects
Medication use.
Eighteen studies evaluated the birth weight of infants fathered by men with various health conditions receiving treatments in the preconception period [22,27,69–84]. Most studies consistently identified that paternal preconception medications were not associated with an increase in SGA or LBW infants. The studies included fathers with various health conditions such as transplants, chronic inflammatory conditions and diabetes. The fathers received a variety of treatments during the preconception period, including immunosuppressive agents [69,72,76,80], biological agents (e.g., tumour necrosis factor (TNF)-alpha inhibitors) [27,73,79], anti-inflammatory agents [74,78], antidiabetic drugs [22], thiopurines [77], disease-modifying anti-rheumatic drugs (DMARDs) [81], methotrexate [82–84], and other medications [70,71,75].
Two large cohort studies found an association between paternal medication use and increased SGA [22,70]. A Danish study evaluating antidiabetic agents and birth weight found an increased risk of SGA infants among fathers who were receiving sulfonylureas 3 months before conception (aOR=1.90; 95%CI:1.11, 2.93) compared with controls [22]. However, other antidiabetic agents such as insulin and metformin were not associated with SGA. Similarly, a Norwegian study found an increased risk of SGA among infants whose fathers were prescribed diazepam [70]. In this large cohort study (n = 349,020 fathers), researchers assessed the relationship between specific drugs dispensed to fathers within 3 months before conception and SGA. They observed no increased risk for SGA infants when fathers were prescribed any drug, drugs requiring special attention, or prednisolone. Nevertheless, among the 178 exposed infants to paternal diazepam, there was an increased risk of SGA (OR=1.4; 95%CI:1.2, 1.6).
Discussion
This comprehensive review offers growing evidence on the link between paternal preconception health and infant birth weight, a significant public health concern because of its strong connections to neonatal morbidity, childhood development, and adult chronic disease risk [5]. Although maternal health has historically been the focus of preconception research and clinical guidelines, this evidence emphasizes that paternal factors—such as body composition, chronic conditions, some medications, and environmental exposures—also significantly influence early developmental processes in offspring.
The most frequently studied exposure was paternal preconception BMI, with most studies finding significant links between higher BMI and increased infant birth weight, including LGA and macrosomia. These links were especially strong in large Chinese cohort studies [40,41], with some showing dose-response relationships where increasing BMI was associated with higher offspring birth weight. However, some studies also reported increased risks of SGA and LBW with higher paternal BMI, suggesting nonlinear associations. These findings are not contradictory; rather, they highlight the complexity of the relationship and the likely presence of multiple underlying mechanisms that contribute to infant birth weight. Emerging evidence from human and animal studies on paternal obesity and epigenetic programming indicates that excess fat may affect offspring birth outcomes by altering sperm DNA methylation, histone modifications, or small non-coding RNAs [85,86]. Additionally, there is some evidence that paternal obesity may be related to impaired placental growth and suboptimal placental functioning, leading to growth restriction [39]. Lastly, the relationship between paternal BMI and infant birth weight should be considered alongside maternal risk factors and infant birth weight (e.g., nutrition, pre-existing medical conditions, and BMI) [4,11,12].
Five studies found no significant association between paternal BMI and infant birth weight, which may be due to heterogeneity across the included studies. There may be geographic and ethnic differences among participants in the studies from North America, Asia and Europe. For example, some Chinese studies used lower BMI cutoffs for overweight (BMI 24–28) and obesity (> 28) than the US studies (overweight: 25–29.9; obesity: > 30). Likewise, in most studies, the analyses controlled for potential confounding maternal and paternal variables; however, the adjustments were inconsistent across studies. Many studies fully adjusted for maternal and paternal factors, such as age, height, BMI, ethnicity, education, pregnancy complications, smoking, and alcohol [37], while others were limited by the available data and adjusted for only maternal [25] or no potentially confounding factors [36,39,42,47]. Lastly, variation exists with the outcome of birth weight, measured as a continuous variable versus dichotomous LGA (yes/no) or SGA (yes/no). These findings highlight the need for rigorous research in this area with attention to the influence of population-specific factors, the importance of adjusting for maternal variables, and differences in BMI and outcome measurements.
Our review also found increasing evidence that suggests that paternal physical health issues, especially metabolic syndrome and diabetes, are linked to a higher risk of LBW in offspring. This aligns with research indicating that paternal conditions may contribute to low birth weight by influencing fetal development and placental health [21]. This may also partially explain the relationship between high BMI and LBW if fathers with high BMI also have co-morbid conditions. However, not all chronic diseases showed associations, as no link was found with tuberculosis or other chronic conditions in two Chinese cohorts [51,52]. These null results may reflect differences in disease severity, management, or limitations in sample size.
Evidence regarding the role of paternal nutrition, physical activity, and sleep quality remains limited and largely inconclusive. While one study found a significant inverse relationship between sleep quality and birth weight [54], most other studies did not identify statistically significant links. With growing recognition of the biological significance of paternal lifestyle factors on sperm epigenetics [87], future research using more precise exposure assessments and longitudinal data is needed. Paternal preconception lifestyle factors, including substance use—particularly tobacco and alcohol—were not consistently associated with infant birth weight. This finding is somewhat unexpected given the known adverse effects of these substances on sperm quality and DNA integrity [88]. However, one large Taiwanese study linked paternal illegal drug use within one to two years prior to conception to lower birth weights, underscoring the need for more detailed exposure data and differentiation between substance types, usage frequency, and timing relative to conception.
Research on environmental exposures and their impact on birth outcomes suggests that paternal urinary or serum phthalate levels, as well as persistent exposure to organic pollutants (POPs) and heavy metals, may be associated with lower birth weight. Research has identified that diverse paternal environmental exposures can interfere with sperm DNA damage, leading to epigenetic abnormalities [89,90]; however, studies specific to the outcome of birth weight are lacking and warrant further mechanistic investigation. Additionally, our review found chemicals such as arsenic and PFAS have been linked to higher birth weights, highlighting the complex nature of dose-response relationships and the potential for non-monotonic effects. Only one investigation examined paternal ionizing radiation exposure and found an association with low birth weight [67]. Although the birth weights remained within normal ranges, this observation warrants further research, particularly given the increasing use of medical imaging and occupational radiation among men of reproductive age.
The link between paternal depression and birth weight produced mixed results. A large US cohort found increased odds of LBW in fathers with recent depression diagnoses, but smaller studies did not verify this association [21]. This discrepancy could be due to variations in mental health assessment methods (diagnostic codes versus self-report), symptom severity, or unmeasured factors like maternal mental health and family stress. Likewise, most research on paternal medication use for chronic conditions (like DMARDs, immunosuppressants, or steroid medications) found no association with LBW or SGA. Nevertheless, two large cohort studies noted increased SGA risks linked to paternal use of sulfonylureas and diazepam, hinting at drug-specific effects that need further investigation. These insights are clinically important because paternal medication use is often overlooked in reproductive counseling and risk assessment evaluations. However, further evaluation is still required to confirm the safety or risks of paternal preconception medications. Paternal medication exposures were often assessed through self-reports at a single time point, which may miss changing or cumulative impacts. Several studies evaluated pharmacy databases and prescriptions filled (yes/no), which do not consider dosage or length of administration.
Implications for clinical practice and future research
The findings of the present review have important implications for preconception care and future research. First, given the influence of various paternal health factors on infant birth weight, greater male involvement in preconception care is warranted. Healthcare professionals and public health officials should consider factors such as paternal BMI, chronic medical conditions, medication use and environmental exposures rather than focusing mainly on maternal factors. Proper management could improve long-term health outcomes not only for the infant but also for potential parents. Where possible, healthcare providers should also inform individuals about risks and offer alternatives to minimize exposure to harmful chemicals. Identifying the specific components of paternal health that may impact infant birth weight also provides insight into developing interventions to mitigate risk and reduce adverse effects on fetal development. Lastly, this scoping review highlighted specific research gaps and limitations that warrant further investigation.
Strengths and limitations
One of the strengths of this scoping review is the application of the JBI scoping review framework in the methodology and the published protocol to guide the review. Furthermore, a team-based approach combining expertise from clinical and research backgrounds was used, strengthening the planning and execution of this scoping review. Another key strength lies in the inclusion of diverse study populations and methodologies, thereby increasing the relevance of the results. However, this review also notes several limitations. The studies in this review were primarily conducted in the USA and China, which may not be generalizable to populations in other regions. The samples were also diverse, with some being population-based, others recruited from clinics (fertility and non-fertility), and others from insurance or pharmacy databases, which could lead to selection bias. Another limitation is that certain paternal health conditions, medications, or behaviours were uncommon and accounted for only a small portion of the review’s sample. Therefore, despite having a larger sample size, the power of the findings remains low because few individuals report having these conditions or engaging in certain behaviours. Some studies using large datasets recorded only live births. Thus, infants who may have been compromised in utero and miscarried or were stillborn would not be captured. As our review was specific to paternal preconception health and birth weight, the influence of combined paternal and maternal factors was not considered and remains an area for further research, as does the influence of paternal preconception health factors on other pregnancy and neonatal outcomes. Finally, the studies included showed heterogeneity, which limits comparability between them. As is customary with scoping reviews, we did not conduct quality appraisals of the included studies. However, we have highlighted the limitations of the existing evidence and potential sources of bias (e.g., sample size and selection, various exposure measurement methods, and potential confounding factors). Despite these limitations, this review adds to the emerging evidence that men’s health before conception may be associated with infant birth weight. Further experimental studies are necessary to assess causality.
Conclusion
This scoping review provides a comprehensive overview of paternal preconception health and its influence on infant birth weight, accounting for physical, behavioral, and environmental factors. Factors such as paternal BMI, medical conditions, certain medications, and environmental exposure to toxic agents were found to be significantly associated with infant birth weight. These findings challenge the traditional emphasis on mothers in preconception care and suggest that more focus should be placed on improving paternal preconception health and raising awareness regarding its importance. Subsequent research on paternal preconception health should further explore the impact of mental health, body composition, and drug consumption. This could contribute to shrinking the research gaps identified in the present review, providing essential insights into how fetal and infant health can be enhanced through the provision of preconception healthcare.
Supporting information
S1 TableMedline Search Strategy.(DOCX)
S2 TablePRISMA ScR Checklist.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1KCA, Basel PL, Singh S. Low birth weight and its associated risk factors: Health facility-based case-control study. P Lo S One. 2020;15(6):e 0234907. doi: 10.1371/journal.pone.0234907 32569281 PMC 7307746 · doi ↗ · pubmed ↗
- 2Redfern KM, Rees GA, Pinkney JH. Maternal Lifestyle Factors and Fetal Macrosomia Risk: A Review. EMJ Repro Health. 2016;52–8. doi: 10.33590/emjreprohealth/10310887 · doi ↗
- 3Vidal E Silva SMC, Tuon RA, Probst LF, Gondinho BVC, Pereira AC, Meneghim M de C, et al. Factors associated with preventable infant death: a multiple logistic regression. Rev Saude Publica. 2018;52:32. doi: 10.11606/s 1518-8787.2018052000252 29723389 PMC 5933942 · doi ↗ · pubmed ↗
- 4Vieira MC, Sankaran S, Pasupathy D. Fetal macrosomia. Obstet Gynaecol Reprod Med. 2020;30(5):146–51.
- 5Blencowe H, Krasevec J, de Onis M, Black RE, An X, Stevens GA, et al. National, regional, and worldwide estimates of low birthweight in 2015, with trends from 2000: a systematic analysis. Lancet Glob Health. 2019;7(7):e 849–60. doi: 10.1016/S 2214-109X(18)30565-5 31103470 PMC 6560046 · doi ↗ · pubmed ↗
- 6Class QA, Rickert ME, Lichtenstein P, D’Onofrio BM. Birth weight, physical morbidity, and mortality: a population-based sibling-comparison study. Am J Epidemiol. 2014;179(5):550–8. doi: 10.1093/aje/kwt 304 24355331 PMC 3927978 · doi ↗ · pubmed ↗
- 7Weider S, Lærum AMW, Evensen KAI, Reitan SK, Lydersen S, Brubakk AM, et al. Neurocognitive function and associations with mental health in adults born preterm with very low birthweight or small for gestational age at term. Front Psychol. 2023;13:1078232. doi: 10.3389/fpsyg.2022.1078232 36743594 PMC 9890170 · doi ↗ · pubmed ↗
- 8Araujo Júnior E, Peixoto AB, Zamarian ACP, Elito Júnior J, Tonni G. Macrosomia. Best Pract Res Clin Obstet Gynaecol. 2017;38:83–96.27727018 10.1016/j.bpobgyn.2016.08.003 · doi ↗ · pubmed ↗