Obstructive sleep apnea and outcomes in acute pulmonary embolism: A large-scale database study
Saud Alawad, Nawaf Al-Saeed, Ahmad Jarrar, Sijin Wen, Sunil Sharma, Kartikeya Rajdev, Kartikeya Rajdev, Kartikeya Rajdev, Kartikeya Rajdev

TL;DR
This study finds that people with obstructive sleep apnea have a higher risk of pulmonary embolism but lower short-term mortality and cardiac arrest after diagnosis.
Contribution
The study reveals a paradoxical protective effect of obstructive sleep apnea against mortality in acute pulmonary embolism.
Findings
OSA patients had higher PE incidence and prevalence compared to non-OSA patients.
OSA patients with PE had significantly lower risks of cardiac arrest and all-cause mortality.
The relationship between OSA and PE outcomes suggests a need for further investigation into underlying mechanisms.
Abstract
To evaluate the impact of obstructive sleep apnea (OSA) on outcomes of acute pulmonary embolism (PE). The primary objective was to compare 30-day mortality and incidence of cardiac arrest in patients with known OSA who developed acute PE versus those with acute PE without OSA. A retrospective cohort study was conducted using the TriNetX global health research network. Two cohorts were defined: adult patients with OSA and acute PE, and adult patients with PE without OSA. Propensity score matching was used to address demographic and comorbidity differences. Data from January 1, 2013, to December 1, 2024, were analyzed, with a one-month follow-up for secondary outcomes. The OSA group (n = 3,547,220) had higher PE incidence proportion (3.48% vs 0.639%) and prevalence (3.794% vs 0.708%) than the control group (n = 103,659,571). Following propensity score matching, 76,636 individuals per…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
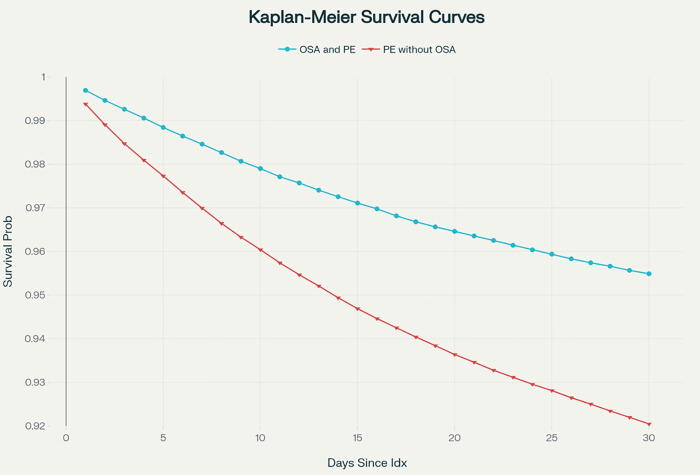 Fig 1
Fig 1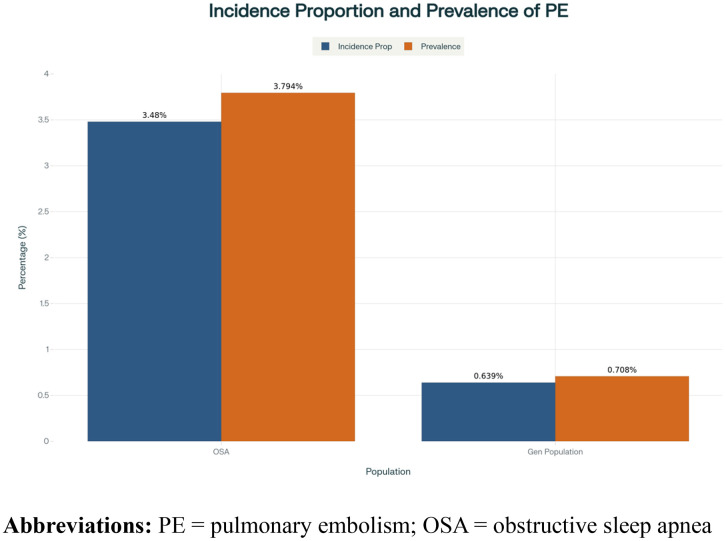 Fig 2
Fig 2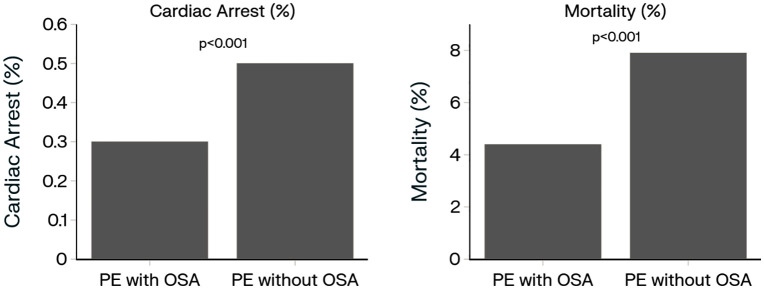 Fig 3
Fig 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObstructive Sleep Apnea Research · Cardiovascular and Diving-Related Complications · Venous Thromboembolism Diagnosis and Management
Introduction
Obstructive sleep apnea (OSA) is a common and often underdiagnosed sleep disorder, affecting an estimated 25% of men and 10% of women [1]. Characterized by recurrent episodes of partial or complete obstruction of the upper airway during sleep, OSA leads to intermittent hypoxia, systemic inflammation, and other metabolic disturbances [2–5]. These pathophysiological mechanisms have been associated with an increased risk of thromboembolic events in OSA [6]. Recent research shows that patients with OSA could have a higher risk of an acute pulmonary embolism (PE), with a prevalence of 3.5% to 6.5%, compared to the general population, which has a prevalence of about 1% in patients [7,8].
A serious condition characterized by the obstruction of pulmonary arteries, and usually caused by thromboembolic events, PE can lead to significant outcomes, such as higher mortality, higher hospitalization rates, and need for critical care [9–12]. While the association between OSA and an elevated risk of PE has been suggested [7], the exact incidence of acute PE in individuals with OSA compared to the general population remains unclear. Furthermore, the outcome of acute PE in OSA patients has not been studied. Our primary hypothesis was that among patients with acute PE, those with OSA have higher 30-day mortality and cardiac arrest than adults without OSA. Secondary hypothesis included with greater intensive care needs (ICU) and endotracheal intubation in patients with acute PE and OSA compared to acute PE without OSA. By performing a multicenter retrospective study, we sought to understand the contributions of OSA to the management and eventual outcomes of PE and develop more precise clinical methods to evaluate a high risk patient population.
Methodology
Study design and data source
We carried out a retrospective cohort study through the TriNetX research network that collects de-identified electronic health record (EHR) data from numerous health care organizations in the United States and other countries [13]. TriNetX is a federated real-world data network that links healthcare organizations (HCOs)—including academic medical centers and hospitals—across multiple countries to create a harmonized repository of de-identified patient data for research and clinical investigation [13]. This research followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. TriNetX de-identifies patient records based on the HIPAA Safe Harbor method by removing all 18 identifiers. Data are shared only in the aggregate, and because patients cannot be re-identified, institutional review board oversight was not required for this analysis. Portions of the data that were available included demographics, comorbidities (ICD-9-CM and ICD-10-CM codes), procedures (CPT), medications (Veterans Affairs National Formulary), lab values (LOINC) and visit type. Data curation was done on August 16, 2025 (Fig 1).
Kaplan-Meier survival curves for all-cause mortality.Abbreviations: PE = pulmonary embolism; OSA = obstructive sleep apnea.
Cohort definition
The study population included adults (≥ 18 years) with an index acute PE event from January 1, 2013, to December 31, 2024, with 30 days of follow-up the outcomes after the PE incidence. There were two cohorts defined: (1) patients had a prior diagnosis of OSA and acute PE (OSA-PE cohort), and (2) patients had acute PE without prior OSA (PE-only cohort), these make the study population as defined under our inclusion criteria. OSA status was defined using ICD-10-CM G47.33, the ICD-9 codes are in Supplemental Table 1 in S1 File. PE was defined using ICD-10-CM I26 and the related ICD-9 codes, The data used from the years 2013−2015 employed the ICD-9-CM codes, which were then converted to ICD-10-CM equivalents, through the application of validated mapping algorithms [14,15]. Patients were excluded if they had other sleep-related breathing disorders such as central sleep apnea (ICD-10-CM G47.30; ICD-9 327.20) or alveolar hypoventilation (ICD-10-CM G47.30) to preserve diagnostic fidelity. We identified acute PE cases using the relevant ICD-9/ICD-10 diagnosis codes in both cohorts, without restricting to inpatient-specific encounter types, which may allow for identification of non-hospitalized cases even though acute PE almost always requires hospitalization.
Outcomes
The two primary outcomes were all-cause mortality and cardiac arrest in the 30 days after the PE diagnosis. Patients were excluded from death and cardiac arrest if this occurred before the index PE event.
Statistical analysis
The statistical analyses were performed using TriNetX Query Builder and Analytics. We used propensity score matching (1:1 nearest-neighbor) with a caliper of 0.1 of pooled standard deviations, and the maximum difference in propensity scores used for matching was 0.01. The match covariates were demographics (age, sex, race/ethnicity), comorbidities (hypertension, ischemic heart disease, heart failure, diabetes, cancer, liver disease, chronic lower lung diseases, including COPD and asthma), body mass index category, smoking and alcohol use, medication classes [antiplatelet agents, anticoagulants including direct oral anticoagulants (DOAC’s), aspirin], and laboratory results (hemoglobin, platelets, INR, creatinine, bicarbonate). The balance was assessed using standardized mean differences, with < 0.1 acceptable.
Descriptive statistics were used to summarize baseline characteristics. Outcomes were expressed as incidence rates, relative risks (RRs), and risk differences (RDs) with 95% confidence intervals (CIs). Kaplan–Meier survival curves were produced for mortality and cardiac arrest outcomes, and log-rank tests were performed. The E-values were also calculated for effect estimates to examine sensitivity to unmeasured confounding.
Results
Study constituents
Within the entire cohort of 424,602 individuals with a diagnosis of PE, 92,461 had a prior OSA diagnosis and 332,141 did not. Before propensity score matching, patients with PE and OSA on average, were older (62.6 ± 13.9 vs 60.6 ± 17.9 years), they were more often male (53.5% vs 46.9%) and were more likely to be white (74.7% vs 69.5%) or non-Hispanic/Latino (80.6% vs 77.1%). They had substantially higher BMI (36.1 ± 9.6 vs 29.1 ± 7.3 kg/m²) and more than two-thirds were classified as obese (BMI ≥ 30) compared with approximately one-third of those without OSA. The cohort also had a more significant comorbidity burden, including more frequent hypertension, diabetes, chronic lower respiratory disease, ischemic heart disease, and venous disease. Again, consistent with these comorbidities, they had higher rates of medication use especially anticoagulant (65.2% vs 37.5%), but also antiplatelet therapy, including aspirin (40–42% vs ~ 20%). Their laboratory values were consistent with subtle physiologic differences, higher bicarbonate levels, and somewhat higher hemoglobin and creatinine levels in the OSA group.
After performing 1:1 propensity score matching, each group had 76,636 individuals included in the analysis. Matching achieved excellent balance with respect to demographics, comorbidities, and medication use. The mean age was similar (62.7 vs 63.6 years) and the distribution of sex (~53% male), race, and ethnicity was almost identical. Cardiometabolic comorbidities and medication use were similar across groups. BMI remained mildly higher in the OSA group (34.5 vs 32.7 kg/m², SMD 0.21), with little difference for other clinical or laboratory metrics, providing additional evidence in support of the adequacy of covariate balance for later outcome comparisons (Table 1).
Table 1: Pre-matching and post-matching characteristics of Group 1(PE with OSA) and Group 2 (PE without OSA).
Incidence proportion of PE
This analysis assessed the occurrence of PE from 1/1/2013 until 12/31/2024. The incidence proportion and prevalence of PE in individuals with OSA (n = 3,547,220) was compared to the general population without OSA (n = 103,659,571). An incidence proportion of PE in patients with OSA was 3.48% compared to 0.639% in the general population. and the prevalence was 3.794% in OSA group compared to 0.708% in general population (Fig 2).
Incidence proportion and prevalence of PE (2013-2024).Abbreviations: PE = pulmonary embolism; OSA = obstructive sleep apnea.
Primary outcomes
The two groups were followed for 30 days from the index event and assessed for the occurrence of cardiac arrest and all-cause mortality. In Group 1 (PE with OSA), 228 (0.3%) individuals had at least a single cardiac arrest event compared to 357 (0.5%) individuals in Group 2 (PE without OSA) (RD −0.175%, RR 0.636 [CI, 0.539–0.751]; P < 0.0001; E-value for RR 2.25) (Table 2 and Fig 3). The groups were then assessed for all-cause mortality with 3,340 (4.4%) in Group 1 compared to 5,979 (7.9%) in Group 2 (RD −3.511%, RR 0.555 [CI, 0.533–0.579]; P < 0.0001; E-value for RR 3.16) (Table 2 and Fig 3).
Table 2: Comparison of outcomes between PE in OSA patients versus PE in patients without OSA.
Comparison 30-day cardiac arrest and mortality occurrence in OSA patients with acute PE versus without OSA.Abbreviations: PE = pulmonary embolism; OSA = obstructive sleep apnea.
Secondary outcomes
Secondary outcomes were defined as the requirement of critical care services, intubation occurrence, occurrence of gastrointestinal bleeding, and intracranial bleeding. Group 1 had fewer critical care admissions than Group 2, but the differences were not statistically significant [3,349 (5.7%) vs 3,488 (6.0%); RD −0.217%, RR 0.964 [CI, 0.920–1.009]; P = 0.114; E-value for RR 1.64]. Intubation was performed less often in Group 1 than in Group 2 [1,363 (1.8%) vs 1,504 (2.0%); RD −0.196%, RR 0.904 [CI, 0.841–0.972]; P = 0.006; E-value for RR 1.8]. Gastrointestinal bleeding occurred less often in Group 1 than in Group 2 [741 (1.1%) vs 997 (1.5%); RD −0.374%, RR 0.745 [CI, 0.678–0.819]; P < 0.0001; E-value for RR 2.5]. All forms of intracranial bleeding occurred less often in Group 1 than in Group 2 [144 (0.2%) vs 233 (0.3%); RD −0.119%, RR 0.616 [CI, 0.501–0.759]; P < 0.0001; E-value for RR 3.08].
Discussion
This is the one of the largest propensity-matched studies to date assessing PE and its relation to OSA. A higher incidence (3.48%, 0.639%) of acute PE was observed in patients with OSA compared to those without Interestingly, despite this increased incidence and prevalence, patients with OSA experienced better outcomes per acute event of PE, with significantly lower rates of cardiac arrest and all-cause mortality within 30 days of the event. These findings suggest a potential influence of OSA on the clinical course of acute PE, although the underlying mechanisms remain uncertain.
This study identifies a significant association between OSA and an increased incidence of PE, with an incidence proportion of 3.794% in OSA patients compared to 0.64% in the general population without sleep disorders. These findings indicate that individuals with OSA are more than 6 times likely of having PE occur than those in the non-OSA general population. This finding is consistent with prior reports that OSA may be an important risk factor for thromboembolic events (DVT/PE) [6,7,16,17]. Moreover, Zhang et al observed that OSA patients had an elevated pulmonary artery obstruction index and PE severity scores, suggesting that OSA is associated with higher severity of PE [18]. The pathophysiological basis for thromboembolic risk is believed to be through hypoxia-induced platelet activation, coagulation cascade dysregulation, and endothelial dysfunction. OSA influences all components of Virchow’s triad, leading to a hypercoagulable state and elevated VTE risk [17,19,20]. Alonso-Fernández et al (2020) also emphasized that intermittent hypoxia and sympathetic activation in OSA may accelerate the development of vascular thrombosis, making these patients more susceptible to PE [6].
Recent studies have revealed a complicated relationship between OSA and PE. Konnerth et al. documented acute PE as being more severe in those patients with OSA associated with higher mortality and prolonged hospital stay [8]. Conversely Ghaisi et al. reported that there was no increased risk of 30-day mortality in patients with PE and OSA as compared to those with PE without OSA [21]. These findings are inconsistent with our findings of lower 30-day mortality in patients with acute PE and OSA. However, Ghaisi et al.‘s study was limited by a relatively small sample size, which could influence the results. In contrast, Huang et al. noted that OSA patients with PE had lower in-hospital mortality despite needing more ventilation [22]. Joshi et al. evaluated a large database and found that OSA was associated with lower in-patient mortality [23]. In keeping with this, a meta-analysis performed by Zhang et al. also found significantly lower in-hospital mortality [16]. Our study, which utilized a large database and is the only propensity-matched analysis specifically examining 30-day mortality and cardiac arrest, is supported by findings from prior smaller studies [7,23]. This potential association with improved outcome may stem from the protective effect of chronic intermittent hypoxia, proposed by Alonso-Fernández et al. (2019) [6]. Nevertheless, OSA patients will still have an increased rate of long-term adverse events such as PE recurrence as discussed in studies that reported higher rates of PE recurrence underscoring the need for OSA screening in PE patients and the hypothetical benefits of treating OSA to modulate risk of PE recurrence [18,24].
We expand on the existing literature not just by evaluating outcome beyond in-hospital mortality to all-cause mortality by 30 days which gives a broader perspective to the prognosis of post-PE, but we also provide stratification of risk for cardiac arrest which was significantly greater for patients with acute PE without comorbid OSA. It is important to note that there was no difference shown in the requirements for intensive care unit service between those with OSA and those without OSA (5.7% versus 6.0%; P = 0.114). This suggests that even though the OSA patients had lower rates of 30-day mortality and cardiac arrest, their immediate critical care requirements were similar to the patients without OSA.
This study also revealed an unexpected finding: higher rates of gastrointestinal bleeding, intracerebral hemorrhage, and subdural bleeds in PE occurred in individuals without OSA compared to those with OSA and PE. This observation is similar to reports of obese stroke patients having less bleeding complications after thrombolytics compared to nonobese stroke patients (most likely due to lower weight-adjusted thrombolytic doses) [25]. Our findings align with some studies that have noted the paradoxical effects of OSA in patients with PE. For instance, Jiang et al observed that patients with OSA required higher doses of warfarin and had increased PE recurrence after anticoagulation discontinuation [26]. This supports the hypothesis that chronic intermittent hypoxia in OSA might lead to adaptive changes in the coagulation system, potentially reducing bleeding risks in PE [27].
These findings highlight the complex interplay between OSA and acute PE. While OSA appears to positively influence against 30-day mortality, cardiac arrest, and intubation rate, it has also shown increased risk of PE occurrence and recurrence. This underscores the importance of early OSA diagnosis and treatment in patients who have experienced acute PE [7]. further studies are needed to determine if early intervention with positive airway therapy would reduce recurrence.
Strengths and limitation
The strength of the study is the examination of both a large dataset in a real-world setting and of several key outcomes based on a 30-day post-event period and not limited to hospitalization alone. Elsewhere, this study has several limitations that should be considered when interpreting the results. First, the dataset, specifically, had no documented follow-up duration limits in relation of outcomes against defined time points. That said, median follow-up was 28 days for the OSA cohort and 27 days for the general cohort. Second, despite propensity score matching, small baseline differences persisted between groups, which, given the large sample size, may have been statistically significant and potentially influenced associated measures. Third, the study is susceptible to unmeasured confounders, such as OSA severity, hypoxemic burden, polysomnography versus clinical OSA diagnosis, and pulmonary embolism severity (massive, submassive, segmental etc). Additionally, information is not available on positive airway pressure therapy in these patients and how it may have influenced outcome, although historically the adherence to PAP therapy has been low. Furthermore, In addition, while our findings indicate a potentially “protective” relationship, we caution against reading too much into this observation due to the nature of our study and missing key data about important factors such as CPAP treatment. Obesity is an independent risk factor for pulmonary embolism and is also associated with OSA [28]. However, the extent to which OSA contributes additional risk beyond that conferred by obesity remains unclear. Fourth, a residual BMI difference persisted between the groups (34.5 vs. 32.7 kg/m²; SMD = 0.214) despite propensity score matching. Although both values fall within the same obesity class, this imbalance could introduce confounding, given the independent association between obesity and PE risk as well as prognosis. Fifth, The study period (2013–2024) encompasses multiple advancements and shifts in PE management, including direct oral anticoagulants, catheter-directed therapies, and new criteria and protocols for risk stratification. We are unable to account for temporal bias. Finaly, limitations of the TriNetX platform prevented calculating cause-specific mortality and cardiac arrest and precluded the use of cluster-robust standard errors to account for patient clustering. Finally, as the study relied on ICD and procedure codes, its conclusions depend on consistent and accurate physician coding. Coding bias may be introduced if coding practices vary across healthcare organizations, including differences in how conditions are classified or managed in inpatient versus outpatient settings.
Conclusion
This study contributes to our understanding of the complex relationship between OSA and PE. While OSA increases the risk of PE occurrence, it appears to be potentially associated with better outcome against severe outcomes like 30-dat mortality, cardiac arrest and bleeding complications. These findings demonstrate the need for a multidimensional approach to treating PE in patients with OSA, and emphasize the importance of further investigating methods of care for this patient group.
Supporting information
S1 FilePropensity Score Matching for OSA and without OSA Groups with Acute PE.Supplement table: Codes.(DOCX)
S2 FilePE in OSA Query key for TriNetX.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Senaratna CV, Perret JL, Lodge CJ, Lowe AJ, Campbell BE, Matheson MC, et al. Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Med Rev. 2017;34:70–81. doi: 10.1016/j.smrv.2016.07.002 27568340 · doi ↗ · pubmed ↗
- 2Lavie L. Oxidative stress in obstructive sleep apnea and intermittent hypoxia--revisited--the bad ugly and good: implications to the heart and brain. Sleep Med Rev. 2015;20:27–45. doi: 10.1016/j.smrv.2014.07.003 25155182 · doi ↗ · pubmed ↗
- 3Drager LF, Polotsky VY, O’Donnell CP, Cravo SL, Lorenzi-Filho G, Machado BH. Translational approaches to understanding metabolic dysfunction and cardiovascular consequences of obstructive sleep apnea. Am J Physiol Heart Circ Physiol. 2015;309(7):H 1101-11. doi: 10.1152/ajpheart.00094.2015 26232233 PMC 4816265 · doi ↗ · pubmed ↗
- 4Parker AT, Sharma S. Effect of cardiac rehabilitation on inflammatory markers in patients with high risk for obstructive sleep apnea: a pilot study. J Interferon Cytokine Res. 2011;31(7):527–31. doi: 10.1089/jir.2010.0151 21574823 · doi ↗ · pubmed ↗
- 5Sharma S, Malur A, Marshall I, Huizar I, Barna BP, Pories W, et al. Alveolar macrophage activation in obese patients with obstructive sleep apnea. Surgery. 2012;151(1):107–12. doi: 10.1016/j.surg.2011.06.035 21982524 · doi ↗ · pubmed ↗
- 6Alonso-Fernández A, Toledo-Pons N, García-Río F. Obstructive sleep apnea and venous thromboembolism: overview of an emerging relationship. Sleep Med Rev. 2020;50:101233. doi: 10.1016/j.smrv.2019.101233 31838272 · doi ↗ · pubmed ↗
- 7Seckin ZI, Helmi H, Weister TJ, Lee A, Festic E. Acute pulmonary embolism in patients with obstructive sleep apnea: frequency, hospital outcomes, and recurrence. J Clin Sleep Med. 2020;16(7):1029–36. doi: 10.5664/jcsm.8380 32065110 PMC 7954077 · doi ↗ · pubmed ↗
- 8Konnerth D, Schwarz F, Probst M, Seidler M, Wagner T, Faul C, et al. Is acute pulmonary embolism more severe in the presence of obstructive sleep apnea? Results from an observational cohort study. J Thromb Thrombolysis. 2018;46(2):253–9. doi: 10.1007/s 11239-018-1665-7 29675617 · doi ↗ · pubmed ↗