Informing the Development of Tailored Antenatal Care Services for Pregnant Adolescents: A Systematic Review and Stakeholder Survey
Karissa Bjornstad, Emily Dawson, Amir Ali Barket Ali Samnani, Marko Kerac, Amanda Murungi, Stephanie V. Wrottesley, Natasha Lelijveld

TL;DR
This study reviews and surveys how antenatal care can be tailored for pregnant adolescents to improve maternal and child outcomes.
Contribution
The study combines a systematic review with stakeholder insights to identify key components for adolescent-tailored antenatal care.
Findings
Most studies showed positive effects on outcomes like birthweight and preterm birth with tailored ANC.
Stakeholders emphasized youth-friendly delivery and mental health support as crucial for effective ANC.
Group ANC delivery and community-based services were highlighted as important future elements.
Abstract
Background: Pregnant adolescents are at higher risk of adverse birth outcomes. Tailoring antenatal care (ANC) to adolescents’ unique needs may be a way to reduce adverse maternal and child outcomes within this population. This systematic review aimed to evaluate ANC services for pregnant adolescents and their impact on maternal and infant outcomes. Methods: Two reviewers independently searched five electronic databases (September 2024) to evaluate existing ANC services that are tailored to adolescents and the impact they have on maternal and infant outcomes. Studies were assessed for quality using the NICE quality appraisal tool and a narrative synthesis was carried out to present the findings. In addition, a survey was disseminated through the Global Adolescent Nutrition Network (GANN) to gain further insights into stakeholder views and experiences of tailored ANC for adolescents.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
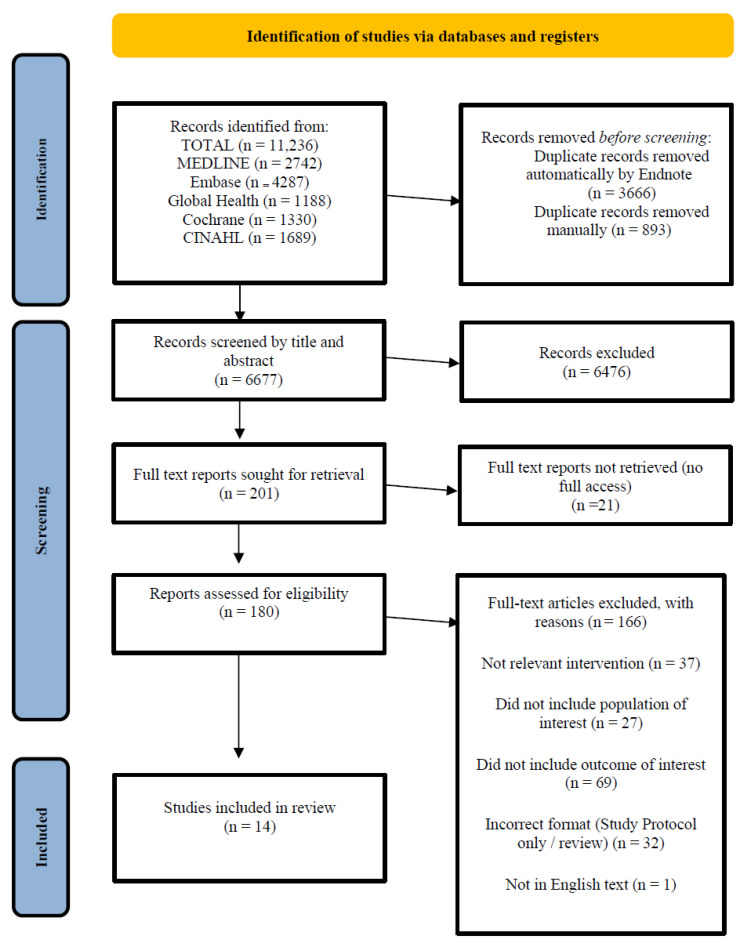 Figure 1
Figure 1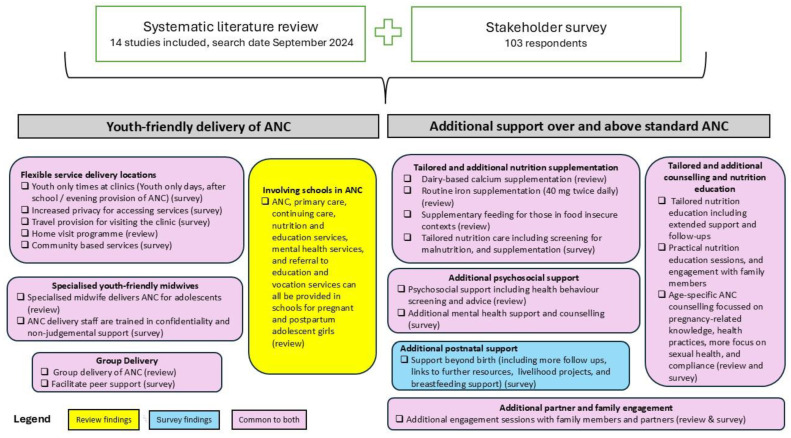 Figure 2
Figure 2- —Department of Foreign Affairs, Ireland
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild Nutrition and Water Access · Gestational Diabetes Research and Management · Breastfeeding Practices and Influences
1. Introduction
Pregnant adolescents (10–19 years) are often overlooked in global health initiatives, leading to inadequate care and support and increasing the risk of adverse outcomes [1,2]. Whilst progress has been made in lowering fertility rates worldwide [3], it is estimated that 21 million adolescents aged 15–19 years old living in low- and middle-income countries become pregnant each year, of which 12 million give birth [4]. Adolescent pregnancy increases the risk of birth complications, including stillbirth, preterm birth, and low birth weight (LBW), as well as higher maternal stigma, economic impacts, and morbidity mortality rates compared to adult pregnancies (20–40 years) [5,6]. Infants born preterm or at LBWs often face difficulties developing cognitive and motor skills as they grow older [7]. In addition, children born to adolescent mothers have an increased risk of being underweight up to the age of five [8]. Adolescents are more vulnerable to these birth complications due to increased biological, social, and economic risks [9,10].
The 2016 Antenatal Care (ANC) model developed by the World Health Organization (WHO) recommends eight ANC visits during pregnancy beginning at 12 weeks and continuing up to 40 weeks to maintain a healthy pregnancy for mother and baby, facilitate an effective transition to positive labour and birth, and achieve positive motherhood [2]. During ANC visits, essential services are provided, such as health education, maternal and foetal assessments, nutritional interventions, and disease prevention and management for mothers and infants.
Adolescents often face cultural and financial barriers to accessing ANC, resulting in missed opportunities to access these essential services [1]. Commonly reported barriers include cost of transport and distance to health facilities [11], as well as shame, blame, and stigma surrounding pregnancy [12]. Evidence from sub-group analyses of antenatal interventions also suggests that pregnant adolescents do not benefit as much as older pregnant women, potentially due to heightened health and nutrition needs that are not being met [13,14]. Overcoming these barriers is essential for ensuring healthy births and positive outcomes for pregnant adolescents. Developing tailored ANC for adolescents could address issues related to accessibility and support, improving attendance and increasing the likelihood of meeting their emotional, psychological, and physiological needs [15]. Successfully doing so could save lives and help break the intergenerational cycle of malnutrition.
Evidence remains limited on whether adolescents in low- and middle-income countries require tailored ANC services. Furthermore, it is unclear which specific services or adjustments would most effectively reduce the heightened risks of maternal and neonatal morbidity and mortality associated with adolescent pregnancies in these contexts. This report aimed to evaluate existing ANC services that are tailored to adolescents—whether to improve access to routine ANC or to provide enhanced or additional ANC services—and the impact they have on maternal and infant outcomes. The findings will contribute to informing what tailored ANC packages, if any, should be trialled to support optimal maternal and birth outcomes in pregnant adolescents in low- and middle-income countries (LMICs). To achieve this, the study had two related objectives: (1) to systematically review the literature on tailored antenatal care for adolescents; and (2) to gather insights from stakeholders working in LMICs on the relevance, availability, and components of tailored ANC for adolescents in their contexts.
2. Materials and Methods
2.1. Systematic Review
The systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 checklist (see Supplementary Material for checklist) [16]. The search strategy consisted of two key concepts: pregnant adolescents and ANC services. The full search strategy can be found in the Supplementary Material. Five databases were searched: MEDLINE, Embase, CINAHL (Cumulative Index to Nursing and Allied Health Literature), Global Health, and Cochrane Library. The initial search was performed in July 2023 and was then repeated in full in September 2024 by two reviewers.
2.1.1. Inclusion and Exclusion Criteria
A ‘PICOSS’ framework (population, intervention, comparison, outcome, setting, study design) was used to determine the eligibility criteria of the studies reviewed (Table 1). Studies were excluded if they were non-human studies, not available in English, published prior to 2000, did not include adolescents (10–24 years), or were literature reviews, systematic reviews, or meeting reports. The age range was selected to be inclusive and follows the age range recommended by Sawyer et al. based on evidence that biological and social growth and development continue beyond the age of 19 years [15]. Due to limited evidence, all settings were included in order to draw lessons from all contexts.
2.1.2. Screening and Selection Process
Once the publications were collated, duplicates were removed. Titles and abstracts were then reviewed against the inclusion/exclusion criteria. For abstracts that appeared to meet the inclusion criteria, full texts were screened. Each study was assessed independently by two researchers for quality using the Methods for the Development of NICE quality appraisal tool [21]. Studies were rated ‘good’ (+++) if the study was designed or conducted in such a way as to minimise risk of bias (based on a list of criteria in the checklist—see reference for further details); ‘average’ (++) if aspects of the study are not clear or the study has addressed some but not all potential sources of bias; and ‘poor’ (+) if significant sources of bias where common.
2.1.3. Data Extraction and Analysis
The data extracted included: title of study; first author; publication date; setting (location/region); year of study; study design; aim of study; recruitment of participants; age included; specific intervention or model of delivery; length of intervention; sample size; outcomes of interest; quality rating; and key findings and notes/comments. Due to the limited number of publications found, a meta-analysis was not possible. Therefore, a narrative synthesis was carried out to summarise and interpret the findings.
2.2. Survey
An anonymous, online, stakeholder survey was disseminated through the Global Adolescent Nutrition Network (GANN), which is a group of approximately 1000 individuals, mainly working in low- and middle-income countries (LMICs) (from 111 unique countries), and who have an interest in adolescent nutrition [22]. The survey consisted of three questions (which were designed by the authors but not tested for validity):
- Do you think that it is important for antenatal care for pregnant adolescents to include additional or altered support, compared to older pregnant adults, and/or be delivered in a youth-friendly manner?
- Expand on your answer by describing what specific elements (if any) you believe should be included in antenatal care for pregnant adolescents.
- In your context, do pregnant adolescents receive additional or tailored antenatal care? If yes, describe your context and the services being provided.
2.3. Data Analysis
Descriptive statistics were used to analyse the questions with binary yes/no options. Thematic analysis was conducted on the open-ended responses. Initial codes were generated from key concepts, which were then grouped into broader themes. These themes were refined and defined based on recurring patterns across responses, highlighting the specific elements of tailored ANC and examples of current service provision in different contexts. To provide further insight, the frequency of mentions for each theme was quantified, offering a clearer understanding of which aspects were most commonly emphasised by respondents.
3. Results
3.1. Systematic Review
A total of 11,236 titles were identified through database searches. Once duplicates were removed, 6677 articles underwent the initial screening process (Figure 1). A total of 180 full-texts were reviewed and 14 publications were included in the results and assessed for quality [13,14,23,24]. All 14 studies reported infant birthweight outcomes; other outcomes reported included preterm birth, gestational age at delivery, and still-births (outcomes and characteristics for each study are described in Table 2).
The included studies were individually assessed for quality using the NICE quality appraisal tool [21]. For internal validity, six studies were given a good rating and eight studies were given an average rating. For external validity, two studies were given a good rating, eleven studies were given an average rating, and one was given a poor rating. Some studies were conducted among small populations with limited diversity, which impacted the grading (Table 3).
3.2. Study Interventions
The following sections provide a narrative description of the literature, presented by the type of ANC intervention for pregnant adolescents.
3.2.1. Micronutrient Supplementation
Two studies examined the effects of micronutrient supplementation for adolescents during pregnancy [19,25]. Pinho-Pompeu et al. [19] conducted a cross-sectional study on the effect of WHO-recommended iron supplementation (40 mg twice daily) in anaemic pregnant adolescents on birth outcomes and found that untreated anaemic adolescents had significantly higher rates of preterm birth (p = 0.003), stillbirth (p = 0.004), and gestational age < 37 weeks (p = 0.036) compared to those who complied with treatment [19,34]. In a randomised controlled trial by Chan et al., 15- to 17-year-old pregnant adolescents who received a high dairy diet had greater intakes of calcium, phosphate, magnesium, and vitamin D than both controls (no supplementation) and the ‘orange juice fortified with calcium’ group. They also had significantly higher infant birth weights (p = 0.001) than both other groups [25].
3.2.2. Supplementary Feeding
In a randomised controlled trial in Malawi, Friebert et al. assessed malnourished pregnant adults and adolescents (mid-upper arm circumference (MUAC) ≥20.6 and ≤23.0 cm) receiving one of two supplementary foods compared to standard care [13]. Adolescents who received one of the supplementary food interventions, either ready-to-use supplementary food (RUSF) or a fortified corn soy blend (CSB+) with a daily multiple micronutrient supplement, showed no significant differences in infant outcomes at birth, 6 weeks, or 12 weeks postpartum compared to those receiving standard care (p > 0.05) [13]. In addition, the subgroup analysis indicated that while supplementary foods improved some maternal health outcomes in adults, this was limited in adolescents [13]. Similarly, Koroma et al. conducted a secondary analysis from a randomised controlled trial in Sierra Leone to compare newborn outcomes with maternal age, following a supplementary feeding intervention in malnourished pregnant women (MUAC ≤ 23 cm) [14]. The trial compared the effect of maternal age on birth weight and found that adults receiving supplementary foods had infants with higher birth weights than adolescents who received the same supplementation (difference in difference: 166 g; 95% CI, 26–306; interaction p = 0.02) [14].
3.2.3. Community-Based Delivery of ANC
The results of three studies showed that delivering ANC in the community was associated with improved infant and maternal outcomes [24,27,30]. Barnet et al. compared the outcomes between comprehensive adolescent pregnancy programmes (CAPPs) in school vs. hospital settings in the USA [24]. CAPPs must include standard ANC, primary, and preventative care for adolescent and infant, continuing care, nutrition services, educational services, mental health services, and referral to education and vocation services [24]. They found that adolescents in school-based CAPPs were significantly less likely to deliver LBW infants compared to those in hospital-based programmes (p = 0.006) [24]. Goyal et al. analysed data from the ‘Every Child Succeeds’ home visit programme in Ohio, USA, focusing on at-risk first-time mothers, with a mean maternal age of 20 years [27]. They found that a higher number of home visits was associated with reduced odds of preterm birth and small for gestational age (SGA); specifically, completing ≥ 8 visits by 26 weeks was linked to an adjusted odds ratio (aOR) of 0.38 for preterm birth and a hazard ratio (HR) of 0.32 for SGA [27]. Jacobs et al. conducted a randomised controlled trial providing tailored home visits to pregnant adolescents, also in the USA, which included goal-setting and health screenings, but found no significant impact on the ‘healthy birth’ indicator (birth weight above 2500 g and delivery at 37 weeks or more; OR 1.12, 95% CI: 0.71, 1.78) [30].
3.2.4. Group-Delivery of ANC
Two studies reported on group-style ANC for pregnant adolescents [23,29]. A cluster randomised trial in New York (USA) health centres examined group prenatal care (8–12 pregnant adolescents per group), including reproductive health promotion versus individual care [29]. The trial, conducted in low-resource areas, showed that group care led to better birth, neonatal, and reproductive outcomes, with lower rates of LBW (8.7% vs. 9.8%) [29]. Although there was no difference in the total number of ANC visits between groups, attending more group prenatal care visits, as compared to individual visits, was associated with lower odds of delivering a small-for-gestational-age, preterm, or LBW infant [29]. A cohort study in Australia compared group ANC (referred to as caseload midwifery) to standard care at a clinic for young women/girls [23]. Using intention to treat analysis, group ANC significantly reduced preterm birth outcomes among adolescents compared to standard care (p < 0.014) but did not significantly impact LBW prevalence (p < 0.48) [23]. Those who received caseload midwifery were more likely to attend five or more antenatal visits compared to those in standard care (p = 0.002) [23].
3.2.5. Tailored Nutrition Education
Two studies found nutrition education programmes to have a positive effect on outcomes [26,28]. A cohort study in USA reported on two tailored nutrition education programmes for pregnant adolescents, finding that the “Have a Healthy Baby” group had higher mean birth weights (3500 ± 600 g) and greater gestational weight gain (16.6 kg) compared to the “Eating Right is Basic” group (3200 ± 500 g; 14.8 kg) [28]. Both groups had low rates of preterm birth. The differences between these two curricula were not clear; however, the authors did state that ongoing support and follow-ups contributed to the positive outcome. In Bangladesh, a study comparing the effects of an antenatal ‘balanced plate’ nutrition education programme on pregnant adolescents versus adults found that adolescents experienced significantly higher birth weights (299.1 g; p = 0.003) compared to adults (95.6 g; p = 0.097) [26]. Additionally, the programme led to a greater reduction in LBW among adolescents (RR: 0.28; p = 0.007) compared to adults (RR: 0.54; p = 0.044) [26]. The programme was integrated into the existing community healthcare and included practical nutrition education sessions, and engagement sessions with family members.
3.2.6. Additional Support and Counselling
Three studies examined the effects of tailored support and counselling on maternal and infant outcomes in adolescents [31,32,33]. Mersal et al. examined the effects of tailored antenatal counselling which focussed on improving pregnancy-related knowledge, health practices, and compliance with ANC at a maternal health centre in Egypt [32]. Adolescents that received standard care had poorer outcomes, with more preterm births (p = 0.001), LBW infants (p = 0.008), and stillbirths [32]. Jones et al. assessed the impact of a tailored adolescent antenatal service in the UK, which included a midwife-led clinic, home visits, and tailored education (individual or group) [31]. The named midwife for teenagers would then provide all ANC for those in a higher social risk category, which was determined using a referral proforma [31]. They reported an increase in birthweight for babies born to mothers participating in the programme, but due to the small sample size this was not statistically significant [31]. Root et al. demonstrated that participation in a tailored prenatal education and support programme, ‘Starting Out Right,’ reduced the odds of low birthweight by 30% (p ≤ 0.05) [33]. All three studies included age-specific support, which addressed the unique needs of pregnant adolescents.
Barnet et al. demonstrated the positive impact of psychosocial support in the form of health behaviour screening and advice on birth outcomes [24]. Comprehensive care, defined as ‘documentation of assessment and advice for psychosocial and behavioural conditions,’ was shown to have a much stronger association with low birth weight when compared to just adequate care (defined as care occurring by the fourth month of pregnancy) [24].
3.3. Stakeholder Survey
The survey received 102 responses, without the collection of any personal or identifiable data. Respondents were assumed to be professionals or experts familiar with adolescent health and nutrition, based on their membership of the Global Adolescent Nutrition Network (GANN).
All respondents agreed that pregnant adolescents require some form of tailored ANC. A majority of respondents (57%) indicated that providing both additional support and youth-friendly delivery of ANC are crucial for pregnant adolescents. A quarter of respondents (23%) said that pregnant adolescents require additional support over and above standard ANC, and 20% felt that youth-friendly delivery is important. However, the majority (78%) reported that, in their context, pregnant adolescents do not receive either form of tailored ANC.
Thematic analysis identified nine themes from the open-ended responses regarding which specific elements should be included in ANC for pregnant adolescents (Table 4), as well as what services currently exist in their contexts.
3.3.1. Inclusive and Supportive Care
Thirty-one participants (30%) mentioned the need for inclusive and supportive care, highlighting the importance of judgement-free support and privacy.
‘Adolescent girls need to be given extra care and attention because they usually face some social and emotional related issues like stigma.’
‘Giving them clear, youth-friendly information with encouragement that they need to make informed decisions and (feel as though) their provider is here for support.’
‘Allow them to have confidants accompany them into the appointments.’
Many also suggested the need for specific training for health workers providing care for pregnant adolescents.
‘It’s important to not just think about how support can be altered for the adolescent mother, but also how we’re training healthcare workers to provide non-judgmental, respectful, supportive care to adolescent mothers. Adolescent mothers face a lot of stigma and abuse in the community, including from health workers.’
3.3.2. Tailored Health Education
Twenty-eight respondents (27%) highlighted the importance of providing tailored health education as part of ANC. Sexual and reproductive health (SRH) education was often considered a key element.
‘Have targeted health talk sessions for pregnant adolescent girls rather than a blanket one in areas such as importance of iron and folic acid supplementation, danger signs, childbirth, child stimulation and parenting.’
‘Adolescents may have limited knowledge of reproductive health, pregnancy, and childbirth. ANC should incorporate comprehensive sexual and reproductive health education to inform them about safe pregnancy practices, birth planning, postpartum care, and future contraception. Information and advice should be delivered in a way that resonates with adolescents, using engaging, age-appropriate communication tools, and offering visual and interactive learning experiences.’
3.3.3. Tailored Nutrition Care
Twenty-three respondents (23%) mentioned the importance of tailoring nutritional care to the specific needs of pregnant adolescents. This included considering the macro- and micro-nutrient needs of adolescents as well as screening for deficiencies.
‘ANC should not only address the current pregnancy nutrition needs but also ensure that they achieve their required growth and meet their specific nutrition requirements. By providing such tailored nutrition support, we can help these young mothers reach their full potential despite the dual demands of increased growth spurt and pregnancy on their physiology.’
‘Given the higher risks associated with adolescent pregnancy, I think that pregnant adolescent girls might require more follow up and/or additional tests & subsequent support. For example, ensuring that adolescent girls are not micronutrient deficient/anaemic and providing proper support through supplementation.’
3.3.4. Mental Health Support and Counselling
Twenty-two respondents highlighted the need for mental health support and counselling during pregnancy, often mentioning the rise in mental health conditions among adolescents. Additionally, they stressed the importance of screening for mental health conditions as part of ANC.
‘Psychosocial counselling for adolescent girls is to be added as this is an unexpected responsibility for them at quite a young age.’
‘Addressing mental health is crucial, as adolescent pregnancies can lead to feelings of isolation and stress.’
Other key elements identified included support beyond birth, partner and family engagement, youth only times at clinics, peer support, and flexible service locations.
3.3.5. Existing Tailored Antenatal Care
There were limited responses regarding what is currently being included in respondents’ contexts. The most frequently mentioned services were:
- Tailored nutrition care, particularly supplementation (nine mentions)
- Tailored educational support, which included nutrition and SRH education (seven mentions)
- Mental health support and counselling (seven mentions)
- Support beyond birth, such as assistance in returning to education and livelihood programmes (five mentions).
Other examples mentioned (four times or less) included peer support, youth-only clinic times, inclusive and supportive care, partner and family engagement, and flexible service locations. An overview of the results from both the survey and the literature review can be found in Figure 2.
4. Discussion
The findings from both the systematic review and the survey highlight the importance of developing adolescent-friendly ANC services for pregnant adolescent girls to improve maternal and infant health outcomes. Evidence from the review indicates that youth-friendly delivery is important, and that tailoring some aspects of antenatal support, especially counselling and nutrition education, can improve maternal and infant birth outcomes [28,31,32,33]. There is also some evidence to suggest that additional micronutrient supplements, not just iron supplements, may benefit this age group [25], and that macronutrient supplementation dosages may need to be higher than that of adult women in order to see a benefit [14].
Successful youth-friendly delivery mechanisms seen in the literature include group-based and community-focused ANC models for pregnant adolescents [20,23,24,27,29]. These approaches can provide a support system for pregnant adolescents alongside the delivery of other services and educational messages, in a comfortable, accepting setting [35]. In addition, community-based care may be a way of addressing some of the accessibility barriers often overlooked for pregnant adolescents [24] and can improve the sustainability of programmes [26].
The evidence from the review suggests that providing routine micronutrient supplementation in line with WHO recommendations can improve maternal and infant birth outcomes for adolescents [19]. Improving access for adolescent girls to routine ANC services would reap these benefits. Beyond iron supplementation, one study showed that other micronutrients are also beneficial [25], suggesting the potential need to prioritise multiple micronutrient supplements (MMS) in this age group. The benefits of MMS on birth outcomes are also well evidenced for adult mothers; however, this is yet to be recommended by WHO as routine [36]. There is an urgent need for more research into the benefits of MMS and heightened macronutrient supplementation in this age group [1,37].
Other additional ANC support that was evidenced in the literature was additional counselling on health during pregnancy, SRH, and compliance to interventions; as well as more practical nutrition education sessions, more psychosocial support and mental health interventions, and ANC sessions that also engage family members and partners. Similar suggestions were raised by respondents of the stakeholder survey, especially around additional mental health support. Adolescent mothers face significantly higher rates of depression, both prenatally and postpartum, compared to adult mothers and their nonpregnant peers [38]. Implementing routine screening for mental health conditions, as suggested by survey participants, could facilitate early intervention and support, potentially mitigating the long-term consequences of poor mental health on both mother and child. However, the survey also suggested that coverage of tailored ANC for pregnant adolescent girls is currently very low, highlighting a gap between the identified needs and the existing services for this group.
Given the limited resources for health services in many settings, especially LMICs, there will be a need to consider whether additional ANC services are cost-effective, over and above ensuring that pregnant adolescent girls access routine ANC. Staff training costs and resource constraints would need to be considered. While evidence is currently lacking for much of this area, the importance of providing inclusive, supportive, judgement-free, and confidential care was clear from both the survey and literature [12,39,40]. Stigma and shame often prevent pregnant adolescents from seeking the care they need and from accessing care early on in pregnancy [41].
4.1. Strengths
The addition of survey findings to this systematic literature review provides unique insights into stakeholder views, complementing and contextualising the other results, especially since the objectives of our review were to inform the testing of future ANC packages in LMICs, whereas much of the literature found was only from high-income settings. The survey highlights strong support for tailored ANC and identifies critical components, reinforcing the evidence from the included studies. The review, while only finding a limited number of papers, does highlight examples of studies that have evaluated ANC interventions specifically for pregnant adolescents as a separate, more vulnerable group, setting a precedent for future work.
4.2. Limitations
While the individual interventions reviewed showed largely positive effects on maternal and infant birth outcomes, the limited number of studies and lack of standardisation among interventions limited our ability to pool and compare studies. We did not assess the certainty of the evidence using ‘GRADE’ since more research is needed for policy recommendations to be made. There is a particular need for future studies to differentiate between younger and older adolescents (e.g., those <16 years vs. ≥16 year) since the risks are likely to be very different and pooling is likely to dilute or obscure these. There is also need for more high-quality, large sample size, randomised study designs. The review was also only limited to antenatal interventions and infant birth outcomes, whereas future systematic reviews should expand on these results to include postnatal services for adolescents and other maternal outcomes beyond birth. In addition, since most studies included in this review were conducted in high-income countries, it is important to note that some may not be relevant or generalisable to LMICs. A methodological limitation of our review was the lack of prior public registration of the search protocol, and the lack of inclusion of non-English-language papers. For the survey, there is a risk of non-response bias since only approximately 10% of those invited to take the survey submitted responses. In addition, due to limited access, pregnant adolescents were not surveyed, excluding a key stakeholder group and potentially limiting the study’s comprehensiveness.
5. Recommendations for Future Research
Intervention trials are needed to test a future standard ANC package for pregnant adolescents that includes the key elements outlined in this report. Such a package should be contextualised to the setting following a review of the current services provided, and should be co-designed with input from adolescent girls themselves [42]. The study should be designed to assess the cost-benefits of additional services vs. simply improving access to routine services. An effective package of tailored ANC services for pregnant adolescents could significantly contribute to reducing maternal deaths, improving new born survival, reducing childhood undernutrition, supporting adolescent mothers to reach their full physical and mental potential, and breaking the intergenerational cycle of malnutrition.
6. Conclusions
The results of the systematic review, backed by survey data, are an important starting point for identifying key elements of adolescent-tailored ANC. These include support and counselling (including mental health), health education (including SRH), greater engagement of family members, and nutrition care (macro- and micro-nutrient supplementation, dietary advice, and practical nutrition education). The services should be delivered in a youth-friendly manner, including non-judgemental care, increased privacy, group sessions, and practical considerations for access such as location, timing and cost. Trialling such packages against standard ANC should be a priority in order to gain adequate evidence to update national and global ANC guidelines, ultimately better reflecting the needs of pregnant adolescent girls.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sabet F. Prost A. Rahmanian S. Al Qudah H. Cardoso M.N. Carlin J.B. Sawyer S.M. Patton G.C. The forgotten girls: The state of evidence for health interventions for pregnant adolescents and their newborns in low-income and middle-income countries Lancet 20234021580159610.1016/S 0140-6736(23)01682-337837988 · doi ↗ · pubmed ↗
- 2World Health Organization WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience World Health Organization Geneva, Switzerland 2016152 p Available online: https://iris.who.int/handle/10665/250796(accessed on 20 August 2024)28079998 · pubmed ↗
- 3World Health Organisation Position Paper on Mainstreaming Adolescent Pregnancy in Efforts to Make Pregnancy Safer 2010 Available online: https://www.gfmer.ch/SRH-Course-2010/adolescent-sexual-reproductive-health/pdf/WHO-mainstreaming-adolescent-pregnancy-efforts-MPS-2010.pdf(accessed on 18 September 2025)
- 4Sully E.A. Biddlecom A. Darroch J.E. Riley T. Ashford L.S. Lince-Deroche N. Firestein L. Murro R. Adding It Up: Investing in Sexual and Reproductive Health 2019 Available online: https://www.guttmacher.org/report/adding-it-up-investing-in-sexual-reproductive-health-2019(accessed on 26 November 2024)
- 5Maheshwari M.V. Khalid N. Patel P.D. Alghareeb R. Hussain A. Maternal and Neonatal Outcomes of Adolescent Pregnancy: A Narrative Review Cureus 202214 e 2592110.7759/cureus.2592135844352 PMC 9282583 · doi ↗ · pubmed ↗
- 6Akseer N. Keats E.C. Thurairajah P. Cousens S. Bétran A.P. Oaks B.M. Osrin D. Piwoz E. Gomo E. Ahmed F. Characteristics and birth outcomes of pregnant adolescents compared to older women: An analysis of individual level data from 140,000 mothers from 20 RC Tse Clinical Medicine 20224510130910.1016/j.eclinm.2022.10130935243274 PMC 8885463 · doi ↗ · pubmed ↗
- 7Upadhyay R.P. Naik G. Choudhary T.S. Chowdhury R. Taneja S. Bhandari N. Martines J.C. Bahl R. Bhan M.K. Cognitive and motor outcomes in children born low birth weight: A systematic review and meta-analysis of studies from South Asia BMC Pediatr.2019193510.1186/s 12887-019-1408-830696415 PMC 6350290 · doi ↗ · pubmed ↗
- 8Welch C. Wong C.K. Lelijveld N. Kerac M. Wrottesley S.V. Adolescent pregnancy is associated with child undernutrition: Systematic review and meta-analysis Matern. Child Nutr.202320 e 1356910.1111/mcn.1356937781871 PMC 10749999 · doi ↗ · pubmed ↗