Assessment of Knowledge, Awareness, and Perceptions of Robotic-Assisted Surgery Among the Adult Population in the United Arab Emirates
Fatma Almadani, Malak Sondoqah, Razan Abdulsattar Awad, Yusur Al-Sudani, MHD Munzer Hussin Alali, Mohamed Feras Ebedin

TL;DR
This study finds that most people in the UAE lack awareness of robotic-assisted surgery, with knowledge linked to education, occupation, and tech skills.
Contribution
The study identifies key demographic factors influencing RAS awareness in the UAE and advocates for targeted public education.
Findings
81.1% of respondents had inadequate awareness of robotic-assisted surgery.
Medical professionals and those with postgraduate education showed higher RAS awareness.
Technologically literate individuals were 2.5 times more likely to know about RAS.
Abstract
Background: Successful adoption of robotic-assisted surgery (RAS) requires acceptance not only from healthcare organizations that implement these technologies but also from the general public, who would ultimately undergo such procedures. This study aimed to assess public awareness, knowledge, and perceptions of RAS in the United Arab Emirates (UAE). Materials and methods: This cross-sectional study was conducted among 433 adults aged 18 years and above residing in the UAE between September 2021 and March 2023. Participants were recruited via convenience sampling through social media platforms. Data were collected using a 20-item self-administered questionnaire assessing knowledge, awareness, and perceptions of RAS. Responses were anonymized to ensure confidentiality. Data were analyzed in SPSS Statistics version 22 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version…
Click any figure to enlarge with its caption.
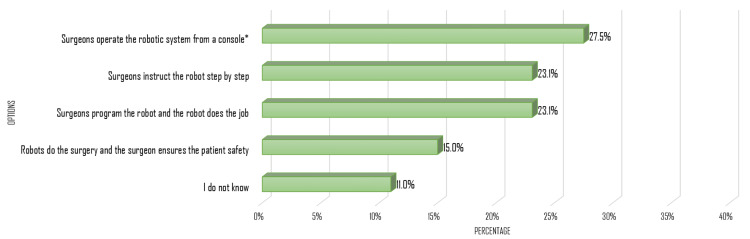 Figure 1
Figure 1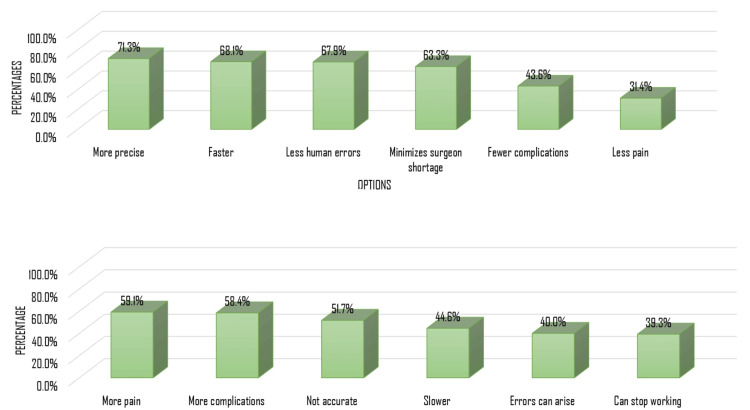 Figure 2
Figure 2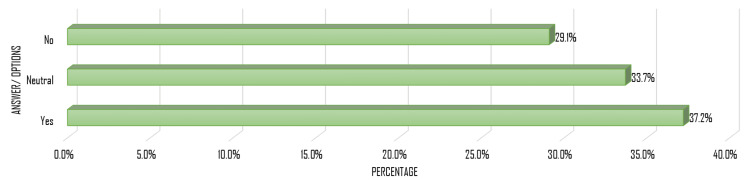 Figure 3
Figure 3| Category | Number of participants (n) | Percentage of participants (%) |
| Sex | ||
| Female | 258 | 59.6% |
| Male | 175 | 40.4% |
| Age | ||
| 18-30 years | 261 | 60.6% |
| 31-40 years | 64 | 14.8% |
| 41-50 years | 65 | 15.1% |
| >50 years | 41 | 9.5% |
| Residence | ||
| Abu Dhabi | 113 | 26.1% |
| Dubai | 135 | 31.2% |
| Sharjah | 157 | 36.3% |
| Other Emirates | 28 | 6.5% |
| Nationality | ||
| Emirati | 200 | 46.2% |
| Non-Emirati | 207 | 47.8% |
| Non-Arab | 26 | 6.0% |
| Education | ||
| School | 113 | 26.1% |
| College/ diploma degree | 77 | 17.8% |
| Bachelor's degree | 197 | 45.5% |
| Postgraduate degree | 46 | 10.6% |
| Profession | ||
| Non-medical | 265 | 61.2% |
| Medical related | 54 | 12.5% |
| Medical | 114 | 26.3% |
| Employment status | ||
| Employed | 188 | 43.4% |
| Unemployed | 37 | 8.5% |
| Student | 208 | 48.0% |
| Education level | Adequate awareness (n, %) | Inadequate awareness (n, %) | p-value | OR (95% CI) |
| School | 26 (23.0%) | 87 (77.0%) | 0.177 | 0.673 (0.379-1.198) |
| Some college/diploma degree | 9 (11.7%) | 68 (88.3%) | 0.296 | 1.520 (0.690-3.348) |
| Bachelor’s degree | 33 (16.8%) | 164 (83.2%) | Reference | 1.00 (reference) |
| Postgraduate degree | 14 (30.4%) | 32 (69.6%) | 0.034 | 2.174 (1.047-4.516) |
| Occupation field | Adequate awareness (n, %) | Inadequate awareness (n, %) | p-value | OR (95% CI) |
| Medical | 29 (25.4%) | 85 (74.6%) | 0.028 | 0.552 (0.323-0.943) |
| Non-medical | 42 (15.8%) | 223 (84.2%) | Reference | 1.00 (reference) |
| Medical-related | 11 (20.4%) | 43 (79.6%) | 0.416 | 1.258 (0.648-2.846) |
| Technological literacy | Adequate awareness (n, %) | Inadequate awareness (n, %) | p-value | OR (95% CI) |
| Below basic | 3 (23.1%) | 10 (76.9%) | 0.493 | 0.624 (0.161-2.421) |
| Basic | 27 (15.8%) | 144 (84.2%) | Reference | 1.00 (reference) |
| Intermediate | 25 (15.2%) | 140 (84.8%) | 0.872 | 0.952 (0.527-1.721) |
| Proficient | 27 (32.1%) | 57 (67.9%) | 0.003 | 2.526 (1.365-4.674) |
| Likelihood to undergo RAS | Adequate awareness (n) | Inadequate awareness (n) | p-value | OR (95% CI) |
| Extremely unlikely | 3 | 49 | 0.613 | 1.408 (0.371-5.338) |
| Unlikely | 5 | 75 | 0.65 | 1.293 (0.425-3.932) |
| Neutral/unsure | 10 | 116 | Reference | 1.00 (reference) |
| Likely | 49 | 99 | <0.001 | 5.741 (2.764-11.927) |
| Extremely likely | 15 | 12 | <0.001 | 14.500 (5.352-29.287) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical Simulation and Training · Soft Robotics and Applications · Artificial Intelligence in Healthcare and Education
Introduction
Robotic-assisted surgery (RAS) represents a major advancement in modern surgical practice and has been increasingly adopted worldwide across multiple surgical specialties. Since the introduction of robotic surgical platforms, most notably the da Vinci® Surgical System (Intuitive Surgical, Inc., Sunnyvale, CA, USA), RAS has transformed minimally invasive surgery by enhancing surgical precision, improving visualization through three-dimensional imaging, and increasing dexterity via articulated instruments [1]. These technological advantages have been associated with reduced blood loss, shorter hospital stays, faster postoperative recovery, and, in selected procedures, improved surgical outcomes compared to conventional techniques [2,3]. As a result, RAS has become an integral component of surgical care in many high-income countries and continues to expand globally.
Despite its growing clinical utilization, public understanding and awareness of RAS remain limited. Existing literature has predominantly focused on the perspectives of surgeons, medical trainees, and patients already undergoing surgical care, with relatively fewer studies assessing awareness and perceptions within the general population [4,5]. Previous international studies have demonstrated that misconceptions regarding the surgeon's role, system autonomy, safety, and cost are common, and that awareness levels are strongly influenced by educational background, occupational exposure, and technological literacy [6].
In the Middle East, and particularly in the United Arab Emirates (UAE), the adoption of RAS systems has expanded rapidly in both public and private healthcare institutions as part of national strategies aimed at advancing healthcare innovation [7]. However, data on public awareness, knowledge, and perceptions toward RAS within the UAE remain scarce. Understanding public perceptions is essential, as patient acceptance and informed decision-making are critical to the successful integration of emerging surgical technologies.
This cross-sectional study aims to examine public awareness, knowledge, and perceptions of RAS among adults in the UAE and to explore factors influencing these attitudes, including demographics, technological literacy, and media exposure.
This article was previously presented at the 6th American University in the Emirates (AUE) student research competition on September 11, 2023, and as a poster presentation at the 5th Internal Medicine Update (IMU) conference 2023 in October 2023.
Materials and methods
Study design
This cross-sectional study was conducted between September 2021 and March 2023 to assess public awareness, knowledge, and attitudes toward RAS among adults residing in the UAE. The study was designed and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies. The University of Sharjah Research Ethics Committee issued approval REC-22-02-16-05-S.
Study sample
Cochran's formula \begin{document} N = \frac{4P(1 - P)}{ME^2} \end{document} was used to calculate the sample size [8], assuming an awareness prevalence of 36.8%, a 95% confidence level, and a 5% margin of error, resulting in a minimum required sample size of 358 participants. To account for potential incomplete responses, the target sample size was increased to 376. A total of 462 participants were recruited, of whom 433 completed the questionnaire fully and were included in the final analysis.
Study population
Adults aged ≥18 years residing in the UAE and able to complete the questionnaire in Arabic or English were eligible to participate. Individuals who submitted incomplete questionnaires were excluded. Participants were recruited using convenience sampling through social media platforms, including WhatsApp (Meta Platforms, Inc., Menlo Park, CA, USA), Instagram (Meta Platforms, Inc., Menlo Park, CA, USA), and Telegram (Telegram FZ-LLC, UAE).
Research instrument and data collection
Data were collected using a 20-item self-administered online questionnaire adapted from a previously validated instrument developed by Buabbas et al. [6]. The questionnaire comprised three domains: demographics (seven items: gender, age, nationality, place of residence, educational level, employment status, and profession), awareness of RAS (six items), and attitudes toward RAS (seven items). Awareness and attitude items were assessed using a five-point Likert-scale response format (1 = strongly disagree to 5 = strongly agree), with higher scores indicating greater awareness and more favorable attitudes toward RAS.
The questionnaire was distributed electronically as an online survey. Participation was voluntary and anonymous, and informed consent was obtained electronically prior to participation. A copy of the distributed questionnaire is provided in the Appendices.
The questionnaire was administered in both Arabic and English. A forward-backward translation process was employed to ensure linguistic and conceptual equivalence. The questionnaire was translated from English into Arabic and independently back-translated into English by bilingual authors. Any discrepancies were reviewed and resolved through consensus to ensure semantic consistency between versions. Although the questionnaire was adapted from a previously validated instrument, a formal pilot study was not conducted. This limitation was acknowledged and considered when interpreting the findings.
Reliability
Internal consistency of the awareness domain was assessed using Cronbach’s alpha ( \begin{document}\alpha = \frac{k}{k - 1} \times \left[ 1 - \frac{\sum \text{item variances}}{\text{total score variance}} \right]\end{document} ), which demonstrated acceptable reliability (α = 0.753) [9,10].
Statistical analysis
Data were analyzed using SPSS Statistics version 22 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.). Descriptive statistics were used to summarize participant characteristics. Associations were assessed using Pearson’s chi-square test or Fisher’s exact test, as appropriate, and odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Awareness and attitude scores were analyzed as continuous variables. For descriptive purposes, attitude scores were further categorized into low, moderate, and high levels to facilitate interpretability. Awareness and knowledge were categorized as adequate or inadequate. A two-tailed p-value of < 0.05 was considered statistically significant.
Results
Sociodemographic data
A total of 433 participants were included in the study; sociodemographic data are represented in Table 1. Females comprised 59.6% (n = 258) of the sample. Participants’ ages ranged from 18 to 64 years, with a median age of 23 years. Most respondents resided in Sharjah (36.3%, n = 157) and Dubai (31.2%, n = 135). Nearly half of the sample were Non-Emirati Arabs (47.8%, n = 207), followed by Emiratis (46.2%, n = 200) and non-Arabs (6.0%, n = 26). Regarding education, 45.5% (n = 197) held a bachelor’s degree. Students represented 48.0% (n = 208) of participants, and 61.2% (n = 265) reported working in non-medical fields.
Awareness of RAS
Awareness scores were generally low, with only 18.9% of participants meeting the predetermined cutoff for adequate awareness. Education level was significantly associated with awareness (p = 0.038). Participants with postgraduate degrees were over twice as likely to have adequate awareness compared with those holding a bachelor’s degree (30.4% vs. 16.8%; OR = 2.174, 95% CI: 1.047-4.516), as shown in Table 2.
Occupation also influenced awareness (p = 0.028). Individuals working in non-medical professions were significantly less likely to have adequate awareness than those in medical fields (15.8% vs. 25.4%; OR = 0.552, 95% CI: 0.323-0.943). Nonetheless, there was no significant difference in awareness between individuals within non-medical and medical-related fields (OR = 1.258, 95% CI: 0.648-2.846), as shown in Table 3.
In the multivariable logistic regression analysis, participants identifying as proficient in technology were 2.5 times more likely to have adequate awareness compared with those reporting only basic technological literacy (32.1% vs. 15.8%; adjusted OR = 2.526, 95% CI: 1.365-4.674). In contrast, there was no significant difference in the proportion of individuals with adequate awareness between those with intermediate literacy and those with basic literacy (15.2% vs. 15.8%; OR = 0.952, 95% CI: 0.527-1.721). Similarly, individuals with below-basic literacy did not differ significantly from those with basic literacy (23.1% vs. 15.8%; OR = 0.624, 95% CI: 0.161-2.421), as shown in Table 4.
Knowledge of RAS principles
When asked to identify the correct definition of RAS, only 27.5% selected that RAS involves a surgeon operating the robotic system from a console. The majority (61.2%) selected incorrect responses, indicating substantial misunderstanding of RAS fundamentals, as shown in Figure 1.
Participants’ responses to the definition of RASCorrect response is marked by an asterisk ().RAS: robotic-assisted surgery*
Regarding participants’ perceptions of the advantages of RAS (Figure 2A), awareness was moderate. Most participants recognized improved surgical precision (71.3%), shorter operative times (68.1%), reduced human error (67.9%), and reduced surgeon shortages (63.3%) as benefits. Fewer participants identified reductions in complications (43.6%) or postoperative pain (31.4%) as advantages, indicating partial understanding of clinical benefits.
Participants’ perceptions of the (A) advantages and (B) disadvantages of RASRAS: robotic-assisted surgery
Knowledge of potential disadvantages (Figure 2B) was similarly limited. While many participants acknowledged increased pain (59.1%), higher complication rates (58.4%), and potential inaccuracy (51.7%) as risks, a substantial proportion were less aware of slower procedures (44.6%), possible errors (40.0%), or technical malfunctions (39.3%), reflecting gaps in awareness of RAS limitations.
Attitudes toward RAS
Although awareness was low, attitudes toward RAS were generally moderate. Based on the predefined attitude categories, 47.6% of participants demonstrated a high attitude, reflected by a willingness to undergo RAS; 34.2% showed a moderate attitude (unsure); and 18.3% exhibited a low attitude (unwilling).
Participants with adequate awareness had significantly higher odds of a high attitude toward RAS than those with inadequate awareness (adjusted OR = 14.5, 95% CI: 5.35-29.29), as shown in Table 5. Regarding the recommendation of RAS, 37.2% indicated they would recommend it to others, 29.1% would not, and 33.7% remained unsure (Figure 3).
Participants’ willingness to recommend RASRAS: robotic-assisted surgery
Discussion
This study reveals that public awareness of RAS in the UAE remains low, with fewer than one in five participants demonstrating adequate knowledge. Findings indicate that education level, occupation, and technological literacy are key determinants of awareness and acceptance, highlighting the need for targeted public education initiatives and improved access to reliable information tailored to the UAE context [11,12].
Higher levels of education, particularly postgraduate study, were associated with greater awareness of RAS. This aligns with existing literature indicating that individuals with higher levels of education are more likely to be exposed to scientific innovations and possess greater health and technology literacy [13,14]. In contrast, participants with only a bachelor’s degree demonstrated lower levels of knowledge, suggesting gaps in public dissemination of information about RAS. In the UAE, where higher education is expanding but not universally health- or technology-focused, integrating medical and technological literacy across diverse programs may be critical for fostering public understanding.
Consistent with previous research, healthcare workers exhibited significantly higher awareness of RAS than those in non-medical careers. Their direct exposure to surgical technologies likely contributes to their greater familiarity. Limited awareness among non-medical participants suggests unequal access to information and emphasizes the need for broader community education efforts [15]. Public health campaigns tailored to non-medical audiences may help bridge this gap and promote equitable understanding of emerging medical technologies.
Technological proficiency appeared to influence awareness. Participants with higher digital literacy were significantly more knowledgeable about RAS. This reflects global trends, indicating that individuals who are comfortable with technology are more open to innovations in healthcare and better able to understand complex technological systems [16]. Given the UAE’s rapidly digitizing healthcare sector, initiatives to improve general digital literacy could enhance both awareness and acceptance of RAS. Notably, social media was the predominant source of RAS information, underscoring the importance of optimizing digital platforms to ensure accurate, accessible, and culturally relevant health communication.
Despite generally positive attitudes toward RAS, participants expressed notable concerns regarding the reliability and safety of robotic systems. Many reported fears of potential malfunctions, findings consistent with studies conducted in other regions. These concerns may stem from limited public understanding of RAS safeguards and intraoperative control mechanisms. Cost was also a frequently cited concern. Participants perceived RAS as more expensive than traditional surgical approaches, echoing prior research suggesting that cost remains a major barrier to the broader adoption of RAS [15,16]. Addressing these concerns through targeted public education, particularly by emphasizing system safety, clinical outcomes, and long-term benefits, such as reduced complications and faster recovery, can strengthen public trust and acceptance.
A strong relationship was observed between participants’ knowledge levels and their willingness to undergo RAS. In the present study, individuals with adequate knowledge were markedly more likely to consider RAS than those with inadequate knowledge. This reinforces the existing literature showing that informed patients are more likely to choose advanced medical technologies when they understand their safety, effectiveness, and potential benefits [17,18]. As public understanding of RAS's precision, minimal invasiveness, and shorter recovery periods improves, acceptance and demand for RAS are likely to increase.
Recommendations
The findings of this study highlight the critical importance of expanding public education to improve awareness and acceptance of RAS. Although RAS offers many advantages, persistent misconceptions related to safety, reliability, and cost continue to limit public confidence. To address these gaps, healthcare institutions and policymakers should prioritize digital outreach, including social media campaigns that provide accurate, accessible information. Additionally, community education programs are advisable to address common misconceptions, particularly when combined with collaboration with educational institutions to enhance technological and health literacy. These efforts will play a vital role in enhancing public understanding and supporting the effective integration of robotic technology into healthcare systems [19,20].
Strengths and limitations
This study’s strengths include a large, geographically diverse sample across multiple Emirates, providing a broad overview of public awareness of RAS in the UAE. Additionally, it features a structured questionnaire with acceptable reliability and enables standardized data collection and comparison with the existing literature.
Limitations include convenience sampling via social media, which may limit generalizability, introduce recruitment bias, and favor tech-literate participants, thereby inflating awareness scores. The absence of a formal pilot study limits the ability to confirm the questionnaire’s reproducibility. Additionally, the extended data collection period (2021-2023) may have introduced temporal variation, as public awareness could have shifted due to new hospital marketing campaigns or government health initiatives. Furthermore, the association between attitudinal status toward RAS and participants’ demographic backgrounds was not analyzed in this study. Examining these relationships in future research would provide valuable insights for understanding factors influencing attitudes toward RAS. Despite these limitations, the findings provide valuable insight into public knowledge and perceptions of RAS in the UAE, offering a foundation for targeted education and outreach initiatives.
Conclusions
This cross-sectional study demonstrates that public awareness of RAS among adults in the UAE remains limited, despite generally positive attitudes toward its use. Awareness was significantly influenced by educational attainment, professional background, and technological literacy, highlighting persistent disparities in access to and understanding of advanced surgical technologies. Importantly, individuals with adequate knowledge were substantially more willing to undergo RAS, underscoring the critical role of public education in shaping acceptance and informed decision-making.
As robotic technologies continue to expand within the UAE healthcare system, targeted public education initiatives are essential to address misconceptions regarding safety, reliability, and cost. Improving technological and health literacy may enhance patient trust, autonomy, and readiness to adopt innovative surgical options. Future studies employing probability-based sampling and longitudinal designs are recommended to assess causal relationships better and evaluate the impact of educational interventions on public awareness and acceptance of RAS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Role of robotic-assisted surgery in public health: its advantages and challenges Cureus Handa A Gaidhane A Choudhari SG 6295816202410.7759/cureus.62958 PMC 1126595439050344 · doi ↗ · pubmed ↗
- 2Robot-assisted urological surgery in the Middle East: where are we and how far can we go?Arab J Urol Azhar RA Elkoushy MA Aldousari S 1061131720193128592110.1080/2090598 X.2019.1601003 PMC 6600062 · doi ↗ · pubmed ↗
- 3Impacts of robotic assisted surgery on hospital’s strategic plan Procedia Soc Behav Sci Platis C Zoulias E 3213261472014
- 4Robotic surgery: current perceptions and the clinical evidence Surg Endosc Ahmad A Ahmad ZF Carleton JD Agarwala A 2552633120172719426410.1007/s 00464-016-4966-y · doi ↗ · pubmed ↗
- 5Gender differences in understanding and acceptance of robot-assisted surgery J Robot Surg Mc Dermott H Choudhury N Lewin-Runacres M Aemn I Moss E 2272321420203104977510.1007/s 11701-019-00960-z PMC 7000495 · doi ↗ · pubmed ↗
- 6An exploratory study of public' awareness about robotics-assisted surgery in Kuwait BMC Med Inform Decis Mak Buabbas AJ Aldousari S Shehab AA 1402020203261140710.1186/s 12911-020-01167-1PMC 7329483 · doi ↗ · pubmed ↗
- 7Robotic assisted surgery in the United Arab Emirates: healthcare experts' perceptions J Robot Surg Barkati N Ntefeh N Okasha A Takshe AA El Khatib R Chelli S 279928061720233773321010.1007/s 11701-023-01716-6PMC 10678779 · doi ↗ · pubmed ↗
- 8How to choose a sampling technique and determine sample size for research: a simplified guide for researchers Oral Oncol Rep Ahmed SK 100662122024