HER2 Alterations in Non-Small Cell Lung Cancer: Emerging Perspectives on the Therapeutic Landscape
Paola Muscolino, Elena Fassi, Diego Signorelli, Francesca Colonese, Diego Luigi Cortinovis, Giuseppe Lo Russo, Giulia Pasello, Carla Infurna, Giuliana Ciappina, Massimiliano Berretta, Vanesa Gregorc, Chiara Lazzari, Mariacarmela Santarpia

TL;DR
This paper reviews the role of HER2 alterations in non-small cell lung cancer and the emerging targeted therapies showing promise in treating these specific cancer subtypes.
Contribution
The paper provides a comprehensive review of HER2-targeted therapies and their clinical outcomes in non-small cell lung cancer.
Findings
HER2 alterations in NSCLC include protein overexpression, gene amplification, and activating mutations.
Trastuzumab deruxtecan and selective tyrosine kinase inhibitors show robust efficacy and intracranial penetration.
Further research is needed to understand resistance mechanisms and optimize treatment strategies for HER2-mutant NSCLC.
Abstract
Over the past decade, significant achievements in elucidating the molecular pathogenesis of non–small cell lung cancer (NSCLC) have catalyzed a paradigm shift from empiric therapies to precision oncology. In this context, HER2 alterations, including protein overexpression, gene amplification, and activating mutations, constitute distinct molecular subsets within NSCLC. In the past few years, targeted therapeutic modalities such as antibody–drug conjugates (ADCs), particularly trastuzumab deruxtecan (the first agent to be granted FDA approval for HER2-mutant NSCLC), alongside selective tyrosine kinase inhibitors (TKIs), including zongertinib and sevabertinib, have demonstrated robust systemic efficacy and notable intracranial penetration. This comprehensive review delineates the molecular landscape and clinical phenotypes of HER2-altered NSCLC, synthesizes interim and mature data from…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
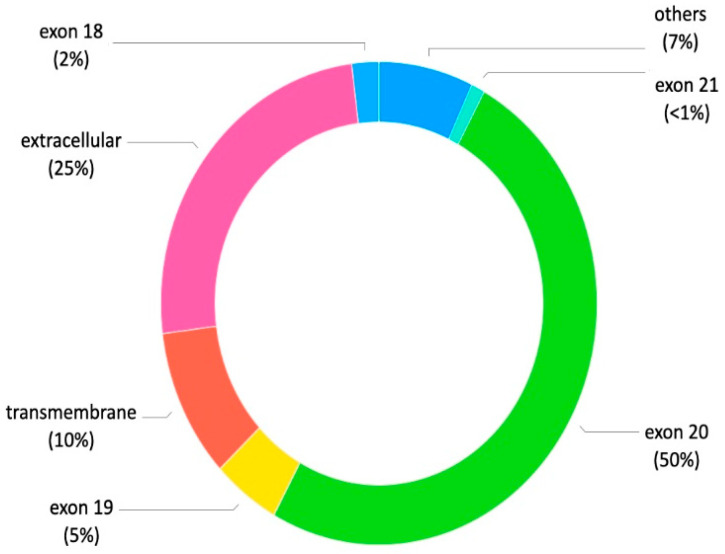 Figure 1
Figure 1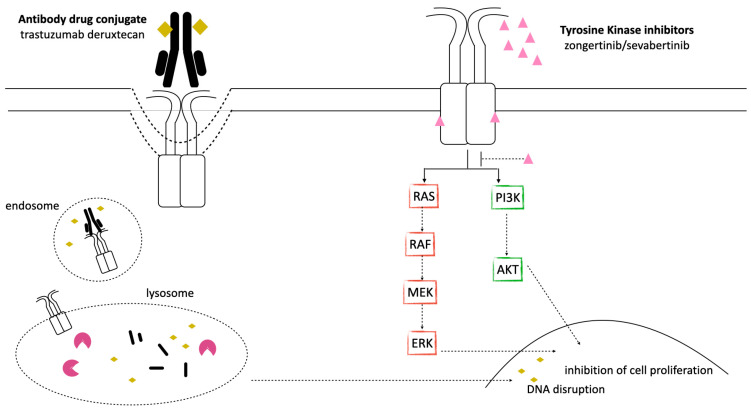 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · HER2/EGFR in Cancer Research · Lung Cancer Research Studies
1. Introduction
Lung cancer is the leading cause of cancer-related deaths, with the majority of cases attributable to cigarette smoking [1]. Non-small cell lung cancer (NSCLC) constitutes about 85% of lung cancer cases, and represents a highly heterogeneous disease, including multiple histological types, such as adenocarcinoma, squamous cell carcinoma, and large cell carcinoma. In recent decades, identifying several actionable genetic changes has revolutionized treatment approaches. The introduction of targeted therapies has shifted treatment from a “one size fits all” model to strategies based on specific molecular features, resulting in unprecedented advances in managing lung tumors [2,3]. Targeted drugs have significantly improved objective response rates (ORRs) and survival outcomes in patients with defined molecular profiles, usually with manageable side effects. The human epidermal growth factor receptor (HER) family consists of four related proteins: the epidermal growth factor receptor (EGFR, also known as HER1 or ErbB1), HER2 (ErbB2 or Neu), HER3 (ErbB3), and HER4 (ErbB4). Both EGFR and HER2 are key drug targets, especially in NSCLC as well as breast and gastroesophageal cancers [4]. Each HER family receptor includes three main regions: an extracellular ligand-binding domain, a single α-helical transmembrane segment, and an intracellular tyrosine kinase domain.
HER2 preferentially undergoes heterodimerization with other ErbB family members upon ligand binding to these receptors. The formation of HER2-containing dimers triggers receptor autophosphorylation and activates key downstream signaling cascades, predominantly the phosphatidylinositol-3-kinase (PI3K)/protein kinase B (AKT) and mitogen-activated protein kinase (MAPK) pathways, which play central roles in the regulation of cell proliferation, differentiation, and migration [4,5]. Different types of HER2 alterations have been found in NSCLC, such as gene mutations (1–6.7%), gene amplifications (2–22%), and protein overexpression (7.7–23%). These alterations are often associated with poorer outcomes [6,7].
Therapeutic strategies targeting HER2 in lung cancer have been under investigation for decades, with unsatisfactory results. Trastuzumab deruxtecan (T-DXd), approved in August 2022 by the Food and Drug Administration for patients with HER2-mutant NSCLC after prior systemic therapy, was the first agent to show significant benefit in this population [8]. Currently, platinum-based chemotherapy combined with immune checkpoint inhibitors (ICIs) remains the standard initial treatment for NSCLC patients with HER2 mutations, providing an ORR of about 43% and median progression-free survival (PFS) of six months [9,10]. Despite this, new therapeutic options are emerging. Ongoing phase III trials in treatment-naïve HER2-mutant NSCLC may soon redefine current management strategies. This review discusses the latest developments and future directions in treating HER2-altered NSCLC.
A literature search was conducted using main medical research databases and on international cancer meetings websites: PubMed, Scopus, and Web of Science, and abstracts from the European Society for Medical Oncology (ESMO), American Society of Clinical Oncology (ASCO), and International Association for the Study of Lung Cancer (IASLC). The search included articles published between from 2004 to February 2026. Original research articles and relevant review articles published in English were considered eligible. The search strategy included combinations of the following keywords: (“HER2” OR “ERBB2”) AND (“non-small cell lung cancer” OR “NSCLC”) AND (“mutation” OR “amplification” OR “overexpression” OR “signaling pathways” OR “targeted therapy” OR “tyrosine kinase inhibitor” OR “antibody–drug conjugate”). The review specifically focused on prospective clinical trials and systematic reviews to synthesize the most relevant evidence.
2. HER2 Alterations in NSCLC
2.1. HER2 Mutations
The HER2 gene, located on chromosome 17 (17q21), encodes a transmembrane growth factor receptor with intrinsic tyrosine kinase activity [5]. HER2 mutations, found in about 4% of NSCLC cases, cause constitutive activation of its kinase domain (see Figure 1). These mutations can be identified trough different methodologies, including Sanger sequencing, next-generation sequencing (NGS), amplification refractory mutation system PCR (ARMS-PCR), or droplet digital PCR (ddPCR) [11]. However, NGS is recommended for HER2 mutation testing due to its high sensitivity and ability to simultaneously analyze millions of DNA fragments while requiring limited input material. An optimal NGS platform should reliably detect the full spectrum of clinically relevant HER2 alterations, including exon 20 YVMA and non-YVMA insertions, missense mutations, copy number variations, and gene amplification, with low DNA input requirements, rapid turnaround time, and high reproducibility. Furthermore, HER2 mutations can be detected on circulating tumor DNA (ctDNA) through plasma NGS. A recent analysis of the DESTINY-Lung01 and DESTINY-Lung02 studies demonstrated the analytical and clinical validity of the approved (United States and Japan) plasma-based Guardant360 companion diagnostic (CDx) HER2-mutated NSCLC for T-DXd treatment [12]. These mutations are more common in female patients, non-smokers, and with adenocarcinoma histology, similar to EGFR mutations. Generally, HER2 mutations do not co-occur with other oncogenic drivers. The most frequent HER2 mutation (about 34%) is a 12-base pair insertion in exon 20 (ex20ins) of the tyrosine kinase domain, adding YVMA between residues A775 and G776. Other recurrent exon 20 insertions affecting the kinase domain include G776delinsVC and G778_P780insGSP, accounting for 5.7% and 3.4%, respectively. Some mutations, like I655V (4.5%), P122L (2.3%), and G222C (1.1%), occur within the extracellular domain, while S310F (5.1%) affects the transmembrane domain [13]. The YVMA insertion variant, in particular, has been correlated with an increased incidence of brain metastases and poorer outcomes after chemotherapy compared to non-YVMA variants [5]. HER2 mutations are key drivers in NSCLC and may contribute to acquired resistance during EGFR TKI therapy [5]. Figure 1 classifies the type and frequency of HER2 mutations that may be observed in patients with NSCLC. Approximately 30% of patients develop brain metastatses [14]. A higher proportion of males was observed in the exon 20 group (41.9% vs. 75.0%, p = 0.025) compared with non-exon 20 mutations. Moreover patients carrying exon 20 mutations have a higher risk of lung and lymph gland metastasis. On the other hand, those with non-exon 20 mutations have a higher probability of developing metastasis to multiple organs [15].
2.2. HER2 Amplification
HER2 amplification occurs in about 3% of NSCLCs. It is typically defined as a HER2/CEP ratio ≥ 2 or HER2 gene copy number > 6, measured using fluorescence in situ hybridization (FISH) [13]. HER2 copy number changes can be detected using various techniques, including NGS, real-time quantitative PCR (qRT-PCR), and FISH, with NGS being the most common in clinical practice due to its high resolution and the ability to analyze multiple genes at once and distinguish focal amplifications from broader chromosomal gains. qRT-PCR does not offer significant advantages over NGS, while FISH remains recommended in clinical studies [11].
Interpretation of FISH results in NSCLC generally follows breast cancer criteria: (i) HER2/CEP17 ratio ≥ 2.0, positive for HER2 amplification; (ii) HER2/CEP17 ratio < 2.0, with HER2 copy number ≥ 6.0 indicating positive amplification, <4.0 indicating negative, and 4.0–5.9 considered indeterminate; (iii) the presence of clustered HER2 signals is considered unequivocally positive [11,16].
HER2 amplification appears to occur more frequently in males and in patients with a smoking history, and it is associated with aggressive disease features, such as larger tumors, increased pleural spread and more lymphovascular invasion. Beyond its role as a primary oncogenic driver, HER2 amplification also acts as an acquired resistance mechanism in EGFR-mutant NSCLC treated with EGFR TKIs, appearing in roughly 15% of patients who develop resistance [13].
2.3. HER2 Overexpression
HER2 overexpression has been identified in various solid tumors, including NSCLC. In lung cancer, studies have linked HER2 overexpression to certain clinicopathological features such as male gender, adenocarcinoma histology (including papillary types), a history of smoking, and generally poorer prognosis [13,17].
The prevalence of HER2 overexpression ranges from 2.4% to 38%, commonly determined by immunohistochemistry (IHC) [18]. However, the relationships among HER2 gene amplification, mutation, and protein overexpression in lung cancers remain controversial, indicating that these changes may constitute distinct clinical subtypes. The mechanism of overexpression is mainly associated with increased copy number from chromosome duplication and polysomy (HER2 gene copy number higher than 5 or 6, but HER2/CEP17 < 2) [19]. HER2 protein levels are assessed through IHC using various scoring systems, such as those developed by the ASCO/College of American Pathologists (CAP) guidelines for breast cancer. These assign scores from 0 to 3+ based on membrane staining intensity. Scores of 0 and 1+ are considered HER2-negative, while 3+ denotes overexpression. A score of 2+ is considered equivocal in breast cancer and requires confirmation by in situ hybridization (ISH). In lung cancer, the proportion of IHC 2+ cases among FISH-positive tumors is relatively low, and an IHC score of 2+ shows limited sensitivity for identifying HER2 amplification. Companion diagnostic criteria of HER2 expression in NSCLC are based on IHC scoring. An IHC score of 0 is defined as HER2-negative. A score of 1+ is currently also classified as negative; however, in the context of the expanding clinical application of ADCs and emerging evidence, further validation is needed to clarify whether IHC 1+ should continue to be considered negative or instead be reclassified as HER2-low expression. In contrast, IHC scores of 2+ and 3+ are defined as HER2-positive [11].
3. HER2 Status and Therapeutic Strategies
Over the past decade, the landscape of HER2-altered NSCLC management has changed considerably with the introduction of HER2-targeted therapies. Despite these therapeutic advances, the current standard first-line treatment for HER2-altered NSCLC is similar to the treatment for non-oncogene-addicted NSCLC and it usually consists of platinum-based chemotherapy combined with immune checkpoint inhibitors (ICIs) [20], although the impact of immunotherapy is controversial.
3.1. Immunotherapy
Immunotherapy represents a standard treatment option for patients with advanced NSCLC without actionable oncogenic drivers. However, their effectiveness is notably reduced in patients whose tumors harbor oncogenic alterations, such as EGFR mutations and ALK rearragements. This reduced efficacy is thought to result from a less inflamed tumor microenvironment and a generally lower tumor mutational burden (TMB) observed in this subgroup of patients. In particular, HER2 mutations correlate with both low TMB and low PD-L1 expression, further limiting the response to ICIs in these patients [21]. Clinical studies evaluating the use of single-agent immunotherapy in HER2-mutant NSCLC have shown lower response rates, which range from 7.4% to 28.9%, according to various retrospective analyses [22,23,24,25,26]. Similarly, in unresectable stage III NSCLC following chemoradiation, consolidation durvalumab in HER2-mutants NSCLC was associated with less clinical benefit [27]. Furthermore, the combination of chemotherapy and immunotherapy in HER2-mutant NSCLC has yielded outcomes that are comparable to those seen in other NSCLC subgroups. Reported results include an ORR of 52%, a median PFS of six months, and an overall survival (OS) rate at one year of 88% [28]. Because of these findings, current guidelines from the European Society for Medical Oncology (ESMO) recommend the use of chemotherapy, with or without immunotherapy, as the first-line treatment for patients with HER2-mutant NSCLC [3].
3.2. HER2-Targeted Treatments
Recent years have seen significant progress in the development and evaluation of various compounds targeting HER2 alterations in NSCLC. These therapies include HER2 Tyrosine Kinase Inhibitors (TKIs), monoclonal antibodies, and antibody–drug conjugates (ADCs). Each category encompasses different agents that have been investigated for their efficacy and safety in patients with HER2-altered NSCLC, as outlined in Table 1 and Figure 2.
3.2.1. Monoclonal Antibodies (mAbs)
Trastuzumab, a humanized monoclonal antibody targeting the HER2 receptor, has been investigated in various chemotherapy combinations for the treatment of advanced, HER2-positive NSCLC. Despite these efforts, the outcomes have been largely disappointing. In a phase II trial assessing the combination of trastuzumab with carboplatin and paclitaxel in advanced NSCLC, selected according to HER2 positivity (1+ to 3+ by Herceptest [Dako Corp, Carpinteria, CA], an ORR of 24.5% (95% confidence interval [CI], 13.8 to 38.3) was reported. The median PFS and median OS were 3.3 months and 10.1 months, respectively [32]. Additionally, the strategy of dual blockade using trastuzumab and pertuzumab was investigated in 15 patients carrying HER2 mutations and 12 harboring HER2 amplification who had previously received standard treatment. This approach resulted in an ORR of only 11% [33]. Given these limited benefits, HER2 alterations in NSCLC were, for a long time, considered as an undruggable target, and further development of these treatment strategies was discontinued.
3.2.2. Antibody–Drug Conjugates (ADCs) and Bispecific Antibodies (BsAbs)
Antibody–drug conjugates (ADCs) represent a novel class of antitumor agents designed to enhance the delivery of cytotoxic chemotherapy directly to cancer cells. These agents are composed of a monoclonal antibody, specifically targeting a tumor-associated antigen, chemically linked to a potent chemotherapy payload. The conjugation is achieved through a stable chemical linker, ensuring that the cytotoxic drug remains attached to the antibody until it reaches the targeted tumor cell. Upon binding to the tumor antigen, the ADC is internalized by the cancer cell. This facilitates the localized release of the cytotoxic agent, thus allowing a higher concentration of the chemotherapy drug to be delivered specifically to cancer cells, thereby minimizing exposure and potential toxicity to normal tissues. In addition to direct cytotoxicity, ADCs can stimulate immune cell effector functions and disrupt receptor dimerization, further contributing to their antitumor activity [34,35]. Among the ADCs developed for NSCLC harborig HER2 alterations, trastuzumab emtansine and trastuzumab deruxtecan have demonstrated the first evidence of efficacy. Figure 2 summarizes the mechanism of action of ADCs.
3.2.3. Trastuzumab Emtansine
Trastuzumab emtansine (T-DM1) is an ADC that combines the HER2-targeted monoclonal antibody trastuzumab with the cytotoxic microtubule inhibitor emtansine (DM1). The clinical efficacy of T-DM1 has been evaluated in a phase II study including pretreated populations selected for HER2 overexpression. In one study, patients were included if they exhibited HER2 expression by IHC 2+ with FISH positivity, or IHC 3+ status. The results demonstrated limited effectiveness, with an ORR of only 7% (1 out of 15 patients). Notably, the only patient who responded carried a HER2 mutation within exon 20 [36]. The efficacy of T-DM1 was explored in another phase II clinical trial, which enrolled 49 patients with advanced HER2-overexpressing NSCLC, previously treated with platinum-based chemotherapy. Of these patients, 29 had IHC 2+ tumors and 20 had IHC 3+ tumors. No objective responses were observed in the IHC 2+ cohort. In contrast, the IHC 3+ cohort achieved an ORR of 20%, with responses particularly noted among patients harboring HER2 gene amplification [37].
A phase II basket trial including HER2-mutant NSCLC showed more promising results, with partial responses observed in 8 out of 18 patients, median duration of response (DoR) of 4 months (range, 2 to 9 months), and a median PFS of 5 months (95% CI, 3 to 9 months). Treatment-related adverse events were generally grade 1 and 2. The most common were transaminase elevation (44%), thrombocytopenia, fatigue, and nausea (33%) [38]. Updated data from 28 pretreated patients reported an ORR of 50%. In HER2-amplified NSCLC, the ORR observed was 55% [39].
3.2.4. Trastuzumab Deruxtecan
Trastuzumab deruxtecan (T-DXd) is an ADC consisting of the humanized monoclonal antibody trastuzumab covalently linked to the topoisomerase I inhibitor deruxtecan through a tetrapeptide cleavable linker. Initially developed in patients with HER2-amplified breast cancer, it is the first approved HER2-directed therapy for patients with previously treated, advanced, HER2-mutated NSCLC. Encouraging results were reported in a phase I trial enrolling 11 pretreated patients carrying HER2 mutations, with an ORR of 72.7% (95% CI 39–94), a median PFS of 11.3 months (95% CI 5.5–14.3), and median DoR of 9.9 months (95% CI 6.9–11.5) [40].
During the dose escalation phase, no dose-limiting toxicities (DLTs) were observed, and the dose-expansion phase evaluated T-DXd in patients with HER2-positive breast or gastric cancer at the dose of 5.4 or 6.4 mg/kg intravenously once every 3 weeks. In the other cohorts, the maximum tolerated dose (MTD) was defined at 6.4 mg/kg and was therefore selected for the subsequent drug development [41].
DESTINY-Lung01 was an open-label, two-cohort, phase II study, designed to evaluate the efficacy and safety of T-DXd in previously treated NSCLC patients carrying HER2 mutations. T-DXd was administered at the dose of 6.4 mg/kg. Ninety-one HER2-mutant NSCLC patients were enrolled. Results showed an ORR of 55% (95% CI 44–65), a median PFS of 8.2 months (95% 6.0–11.9), and a median OS of 17.8 months (95% 13.8–22.1). However, 41% of patients reported grade ≥ 3 treatment-related adverse events (TRAEs), including hematologic and gastrointestinal toxicities. Interstitial lung disease (ILD) occurred in approximately 26% of patients. Of these, four cases of grade ≥ 3 ILD were observed, two of which were fatal [42].
In order to reduce the risk of ILD, the phase II DESTINY-Lung02 trial was designed to compare the safety and efficacy of T-DXd when administered at the dose of 6.4 mg/kg over 5.4 mg/kg in 152 previously treated HER2-mutant NSCLC. Results demonstrated that the dose of 5.4 mg/kg determined an ORR of 49.0% (95% 39–59.1), a median PFS of 9.9 months (95% 7.4-NE), and a median OS of 19.5 months. The incidence of T-DXd-induced ILD/pneumonitis was significantly lower at the dose of 5.4 mg/kg (12.9%) compared to a 6.4 mg/kg dose (28.0%) [8]. The updated analysis of the study confirmed the T-DXd activity in patients receiving 5.4 mg/kg dosage, with a median PFS of 10.0 months (CI 95%, 7.7 to 15.2) and a median OS 19.0 months (CI 95%, 14.7-NE) [40]. Drug-related ILD occurred at a higher frequency in the higher dose arm (14.9% vs. 32.0% in the 5.4 mg/mg and 6.4 mg/kg arms, respectively), although most of these events were grade 1 or 2, with one grade 5 in each arm. Of note, health-related quality of life was preserved for the duration of T-DXd treatment [43].
In a post hoc secondary pooled analysis of the DESTINY-Lung01 and DESTINY-Lung02 trials, Jänne et al. evaluated the efficacy and safety of T-DXd according to the dose (5.4 mg/kg vs. 6.4 mg/kg) in patients with previously treated HER2-mutant NSCLC with or without untreated or previously treated stable brain metastases (BMs) (Table 1). Patients with and without BMs who received T-DXd at the dose of 5.4 mg/kg (102 pts) had confirmed ORR of 47% (95% CI, 29–65%) and 50% (95% CI, 38–62%), respectively, and an intracranial confirmed ORR of 50% (95% CI, 23–77%). An ORR of 50% (95% CI, 36–64%) and 59% (95% CI, 48–69%) was observed in patients receiving T-DXd at the dose of 6.4 mg/kg with and without BMs, respectively, with an intracranial confirmed ORR of 30% (95% CI, 15–49%). These data suggest that T-DXd, at the approved dose of 5.4 mg/kg, is an effective treatment option for patients previously treated, with or without BMs [44]. Based on comparable efficacy and a reduced risk of ILD, the 5.4 mg/kg dosage was selected for the ongoing phase III DESTINY-Lung 04 study (NCT 05048796), designed in treatment-naïve, HER2-mutant patients. Four hundred fifty nine metastatic patients have been randomized between T-DXd and cisplatin/carboplatin, pemetrexed, and pembrolizumab. Primary endpoint is PFS. Results from this trial may establish T-DXd as the new first-line therapeutic standard for this molecular subset of NSCLC [45]. To improve its antitumor efficacy, several studies are evaluating the combination of T-DXd with ICIs or platinum-based chemotherapy.
Planchard et al., in a phase Ib trial, DESTINY-Lung03, evaluated T-DXd as monotherapy or in combination with durvalumab and platinum-based chemotherapy in patients with pretreated, metastatic HER2-overexpressing NSCLC. Part 1 evaluated T-DXd 4.4 or 5.4 mg/kg plus durvalumab (1120 mg) and cisplatin (60 or 75 mg/m^2^; Arm 1A)/carboplatin (AUC 4 or 5; Arm 1B); or T-DXd 5.4 mg/kg monotherapy (Arm 1D). The primary endpoints included DLTs and AEs (Arms 1A and 1B), while safety (Arm 1D) and efficacy (all arms) were secondary endpoints. On April 1, 2024, at the data cutoff, 11, 24, and 36 patients had received treatment in the cisplatin-based combination arm, the carboplatin-based combination arm, and the T-DXd monotherapy arm, respectively. Combination regimens were associated with a high incidence of DLTs, primarily hematologic, such as febrile neutropenia reported in Arm 1A: (n = 1; Grade [G]5; 4.4 mg/kg/1120 mg/60 mg/m^2^ doses) versus febrile neutropenia observed in Arm 1B: (n = 1; G3; 4.4 mg/kg/1120 mg/AUC 5 doses; n = 1; G4; 4.4 mg/kg/1120 mg/AUC 4 doses) with the occasional occurrence of severe and fatal events. Drug-related serious AEs occurred in 63.6%, 37.5%, and 16.7% of Arms 1A, 1B, and 1D, respectively. Confirmed ORR were 37.5% (95% CI: 18.8–59.4) in Arm 1B and 44.4% (95% CI: 27.9–61.9) in Arm 1D, demonstrating the substantial clinical activity of single-agent T-DXd, and suggesting that the combination regimens are not recommended for this population [46]. Novel agents are currently under investigation, including trastuzumab rezetecan or zanidatamab.
3.2.5. Trastuzumab Rezetecan (SHR-A1811)
Trastuzumab rezetecan is an ADC consisting of the humanised HER2-trastuzumab, linked to the DNA topoisomerase I inhibitor SHR169265 via a tetrapeptide-based cleavable linker. The phase II HORIZON-Lung trial, conducted in China in 94 patients with previously treated locally advanced or metastatic NSCLC carrying an activating HER2 mutation, demonstrated an ORR of 73% (95% CI, 63.3–82.0) and a median PFS of 11.5 months (95% CI 9–9 not reached). Data on OS are not yet mature. Treatment was effective also in patients with brain metastases (ORR: 87.5%) [47].
3.2.6. Zanidatamab (ZW25)
Zanidatamab (ZW25) is a humanized bispecific monoclonal antibody (bsAb) targeting two HER2 extracellular domains: the dimerization domain (ECD2) and the juxtamembranous one (ECD4). In a phase 1 dose escalation and expansion study, including patients with locally advanced or metastatic HER2-expressing or HER2-amplified solid tumours, ZW25 showed a good safety profile. The most common adverse events were diarrhea (43%) and infusion-related reactions (34%), and only 3% of toxicities were grade 3/4. In Part 2, enrolling 86 patients with HER2 overexpression or amplification, the ORR was 37%, with a DOR of 8.5 months in the biliary tract cancer group, 5.6 months in the colorectal cancer group, and 9.7 months in the group of other cancers. The median PFS for all patients was 5.4 months (95% CI 3.7–7.3) [48].
Novel ADCs are under evaluation in phase I/II clinical trials for NSCLC, including BL-M17D1 (NCT06114511), TQB2102 (NCT06496490), and MRG002 (NCT05141786). Additional ADCs are being assessed in phase I trials across multiple solid tumors, including NSCLC, such as DB-1303/BNT323 (NCT05150691), XMT-2056 (NCT05514717), and GQ1001 (NCT04450732) [49].
3.2.7. Tyrosine Kinase Inhibitors
Several pan-HER TKIs have been extensively tested in HER2-altered NSCLC patients, including afatinib, neratinib, dacomitinib, and poziotinib, with disappointing results, probably due to DLTs or suboptimal potency [23,50,51,52,53].
In contrast with pan-HER inhibitors, novel mutant-selective TKIs have been developed with the aim of improving activity against HER2 mutations, while reducing off-target side effects. Zongertinib and sevabertinib represent the first HER2-selective TKIs that have demonstrated significant clinical activity in this setting (Table 1). Figure 2 summarizes the mechanism of action of HER2 TKIs.
3.2.8. Zongertinib
Zongertinib is an oral, irreversible TKI that selectively inhibits HER2 while sparing wild-type receptors. Preclinical data suggest its activity against HER2-dependent human cancer cells resistant to trastuzumab deruxtecan and in KRAS G12C mutant NSCLC cell lines resistant to KRAS inhibitors [54]. This agent was evaluated in the Beamion LUNG-1 study, a multicohort, phase Ia/Ib trial enrolling 200 naïve or previously treated patients with metastatic NSCLC carrying TKD and non-TKD HER2 mutations. The primary endpoint was ORR, assessed by blinded independent central review (cohorts 1 and 5) or by investigator review (cohort 3). Secondary endpoints included DoR and PFS. Zongertinib achieved a confirmed ORR of 71% (CI 95% 60–80) in 75 previously treated patients carrying TKD mutations (cohort 1), with a median DoR of 14.1 months (CI 95% 6.9—not estimable) and a median PFS of 12.4 months (CI 95% 8.2—not estimable). The ORR in 31 patients previously treated with HER2-directed ADCs (cohort 5) was 48% (CI 95% 32–65), while that in those with non-TKD mutations (cohort 3) was 30%. Data from thr 74 naïve patients (cohort 4) demonstrated an ORR of 77% (CI 95% 66- 85), with a median DoR of 9.7 months (CI 95% 7.1–9.9) and a median PFS of 11 months (CI 95% 9.7–12.4) [55]. Twenty seven patients had brain lesions. An intracranial response of 41% (95% CI 25–59) and an intracranial disease control rate of 81% (95% CI 63–92) were reported, thus demonstrating the notable intracranial activity of zongertinib. Treatment was generally well tolerated. Grade ≥ 3 adverse events were reported in 17%, 3%, and 25% of patients in cohorts 1, 5, and 3, respectively. No cases of drug-related interstitial lung disease were observed [56].
On August 8, 2025, the Food and Drug Administration granted accelerated approval to zongertinib for adults with unresectable or metastatic NSCLC whose tumors harbor HER2 TKD-activating mutations, as detected by an FDA-approved test, and who have received prior systemic therapy [30]. The phase III ongoing Beamion LUNG 2 study (NCT06151574) is currently evaluating the efficacy and safety of zongertinib in treatment-naïve NSCLC carrying TKD HER2 mutations. Two hundred seventy patients, stratified according to the type of mutations, are randomized between zongertinib or platinum pemetrexed pembrolizumab combinations. The primary end point is PFS. Zongertinib is also under evaluation in the adjuvant setting in the phase 3 trial Beamion-LUNG 3 (NCT07195695).
3.2.9. Sevabertinib
Sevabertinib is an oral, reversible TKI that potently inhibits tumors with EGFR and HER2 mutations, including ex20ins, while sparing wild-type EGFR. Preclinical data demonstrate that activities of sevabertinib and zongertinib are comparable in cancer cell lines carrying HER2 alterations, while zongertinib has no activity against exon 20 EGFR insertions [57]. Clinical efficacy and safety of sevabertinib was tested in the phase I-II SOHO-01 trial in 209 treatment-naïve and previously treated NSCLC patients carrying TKD and non-TKD mutations. Patients were stratified into three cohorts based on prior therapy. Cohort D included those who had received prior treatment, but not HER2-targeted therapy. Cohort E included those who had received HER2-directed ADCs. Cohort F included treatment-naïve patients. The median follow-up was 13.8 months in cohort D, 11.7 months in cohort E, and 9.9 months in cohort F. In cohort D (n = 81), an ORR of 64% (CI 95% 53–75), a median DOR of 9.2 months (CI 95% 6.3–13.5), and a PFS of 8.3 months (CI 95% 6.9–12.3) were reported. In cohort E (n = 55), sevabertinib demonstrated an ORR of 38% (CI 95% 25–52), with a median DOR of 8.5 months (CI 95% 5.6–16.4) and median PFS of 5.5 months (CI 95% 4.3–8.3). In cohort F (n = 73), ORR was 71% (CI 95% 59–81), median DOR was 11.0 months (CI 95% 8.1-not estimable), and median PFS was not reached. In 22%, 27%, and 12% of patients enrolled in cohorts D, E, and F, respectively, BMs were present. In cohort D, ORRs were 61% in patients with brain metastases and 65% in those without. In cohort E, ORRs were 27% in patients with BMs and 43% among those without, whereas in cohort F, ORRs reached 78% and 70% in patients with and without BMs, respectively. In patients with BMs at baseline, post-baseline intracranial progression was observed in 22% of cohort D, 20% of cohort E, and 0% of cohort F. In contrast, in patients without BMs at baseline, post-baseline brain progression occurred in 6% of cohort D, 5% of cohort E, and 3% of cohort F. Diarrhea was the most common adverse event (reported in 84–91% of patients), with grade ≥ 3 events observed in 5–23% of patients [58]. An exploratory analysis from the SOHO-1 trial revealed activity across HER2 variant classes. Higher response rates were observed in tumors harboring TKD mutations, particularly the Y772_A775dup (YVMA) mutation versus patients with HER2 non-TKD mutations. On November 19 2025, the FDA granted accelerated approval to sevabertinib [31]. The Oncomine Dx Target Test (Life Technologies Corporation) as a companion diagnostic test to detect HER2 TKD activating mutations in patients with non-squamous NSCLC was also approved.
The ongoing phase III SOHO-02 study (NCT06452277) is evaluating the efficacy of sevabertinib in 278 patients with naïve advanced NSCLC harboring TKD HER2 mutations. Patients are randomized between sevabertinib over platinum pemetrexed pembrolizumab and the primary end point is PFS.
4. Mechanisms of Acquired Resistance to HER2 Inhibitors
Little is known about the acquired mechanisms of resistance to HER2 inhibitors. Data from HER2-mutant tumor cell lines, patient-derived xenografts, and tumor tissues were collected to identify acquired resistance mechanisms to T-DXd [59]. Alterations of the deruxtecan payload, mediated by loss of Schlafen Family Member 11 (SLFN11), a DNA/RNA helicase, or copy number gain in ABCC1, responsible for the transcription of the efflux pump, MRP1, or the blockade of MRP1, have been described as some of the acquired mechanisms to T-DXd. Furthermore, secondary HER2 mutations determining a steric hindrance to trastuzumab binding were observed. Data from liquid biopsy performed in HER2 mutant NSCLC patients progressing on T-DXd showed the activation of alternative signaling pathways, including MET, FGFR2 mutation, and EGFR and BRAF amplifications. Preclinical data indicate that these mechanisms do not affect the sensitivity to HER2 TKIs, as zongertinib, thus suggesting that this class of drugs might be effective to overcome acquired resistance to T-DXd.
5. Perspectives and Conclusions
HER2 mutations, amplifications, and overexpression display distinct biological characteristics and variable responses to treatments, highlighting the importance of an accurate molecular diagnostics. Platinum-based chemotherapy and immunotherapy remain standard first-line options. However, the emergence of novel HER2-targeted therapies, including zongertinib and sevabertinib, and potent ADCs such as trastuzumab deruxtecan has led to meaningful durable responses and survival benefits in patients with HER2-mutant NSCLC, thus changing the treatment paradigm for this subset of oncogene-driven tumors. The recent approval of anti-HER2 targeted agents supports the use of a comprehensive molecular profiling with NGS techniques in routine clinical practice to identify these mutations and tailor treatment strategies at the time of tumor diagnosis. In addition, HER2 overexpression identifies a subset of patients that might benefit from T-DXd-based therapies, and currently ongoing studies will provide definitive conclusions on the efficacy of this strategy.
Increasing evidence suggests the clinically meaningful intracranial activity of anti-HER2 agents. However, the optimal treatment algorithm still remains to be defined. How to combine these agents with loco-regional treatments needs to be further explored. The efficacy observed in the phase I/II clinical trials, exploring the anti-tumor activity of T-DXd, zongertinib, and sevabertinib in patients with HER2-mutant NSCLC has opened new questions regarding the therapeutic strategy to use (first T-XDd followed by HER2 TKIs or HER2 TKIs followed by T-XDd). Considering the different safety profile of these agents and the different mechanisms of action, a sequential use might be possible and currently ongoing studies will provide additional evidence.
Multiple biological mechanisms of acquired resistance to T-XDd have been identified. Based on preclinical evidences, HER2-mutated cancer cells progressing to T-XDd might retain sensitivity to HER2 TKIs. Data from phase I/II clinical trials suggest the efficacy of zongertinib and sevabertinib following T-XDd, but further research is warranted in order to achieve maximal clinical benefit and improve patients’ outcomes.
With the advent of new targeted therapies specifically targeting HER2 mutations, the prognosis for patients with HER2-mutant NSCLC, historically considered dismal, is remarkably improving. However, active areas of research include the discovery of genetic alterations underlying resistance and the optimal management of anti-HER2 toxicities, more pronounced for the ADCs compared to the TKIs, in the clinical setting.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siegel R.L. Kratzer T.B. Wagle N.S. Sung H. Jemal A. Cancer Statistics, 2026 CA Cancer J. Clin.202676 e 7004310.3322/caac.7004341528114 PMC 12798275 · doi ↗ · pubmed ↗
- 2Tan A.C. Tan D.S.W. Targeted Therapies for Lung Cancer Patients with Oncogenic Driver Molecular Alterations J. Clin. Oncol.20224061162510.1200/JCO.21.0162634985916 · doi ↗ · pubmed ↗
- 3Hendriks L.E.L. Cortiula F. Martins-Branco D. Mariamidze E. Popat S. Reck M. ESMO Guidelines Committee Updated Treatment Recommendations for Systemic Treatment: From the ESMO Oncogene-Addicted Metastatic NSCLC Living Guideline Ann. Oncol.2025361227123110.1016/j.annonc.2025.06.00740571160 · doi ↗ · pubmed ↗
- 4Friedlaender A. Subbiah V. Russo A. Banna G.L. Malapelle U. Rolfo C. Addeo A. EGFR and HER 2 Exon 20 Insertions in Solid Tumours: From Biology to Treatment Nat. Rev. Clin. Oncol.2022195169 Correction in Nat. Rev. Clin. Oncol. 2022, 19, 70. https://doi.org/10.1038/s 41571-021-00571-410.1038/s 41571-021-00558-134561632 · doi ↗ · pubmed ↗
- 5Jebbink M. de Langen A.J. Boelens M.C. Monkhorst K. Smit E.F. The Force of HER 2—A Druggable Target in NSCLC?Cancer Treat. Rev.20208610199610.1016/j.ctrv.2020.10199632135383 · doi ↗ · pubmed ↗
- 6Takezawa K. Pirazzoli V. Arcila M.E. Nebhan C.A. Song X. de Stanchina E. Ohashi K. Janjigian Y.Y. Spitzler P.J. Melnick M.A. HER 2 Amplification: A Potential Mechanism of Acquired Resistance to EGFR Inhibition in EGFR-Mutant Lung Cancers That Lack the Second-Site EGFRT 790M Mutation Cancer Discov.2012292293310.1158/2159-8290.CD-12-010822956644 PMC 3473100 · doi ↗ · pubmed ↗
- 7Loeffler E. Ancel J. Dalstein V. Deslée G. Polette M. Nawrocki-Raby B. HER 2 Alterations in Non-Small Cell Lung Cancer: Biologico-Clinical Consequences and Interest in Therapeutic Strategies Life 2023146410.3390/life 1401006438255679 PMC 10820545 · doi ↗ · pubmed ↗
- 8Goto K. Goto Y. Kubo T. Ninomiya K. Kim S.-W. Planchard D. Ahn M.-J. Smit E.F. de Langen A.J. Pérol M. Trastuzumab Deruxtecan in Patients with HER 2-Mutant Metastatic Non-Small-Cell Lung Cancer: Primary Results from the Randomized, Phase II DESTINY-Lung 02 Trial J. Clin. Oncol.20234148524863 Erratum in J. Clin. Oncol. 2024, 42, 3635. https://doi.org/10.1200/JCO-24-0188310.1200/JCO.23.0136137694347 PMC 10617843 · doi ↗ · pubmed ↗