Artificial Intelligence in Orthopaedics: Clinical Performance, Limitations, and Translational Readiness—A Review
Wojciech Michał Glinkowski, Antonina Spalińska, Agnieszka Wołk, Krzysztof Wołk

TL;DR
This review explores how AI is being used in orthopedics, highlighting its potential in imaging, surgery, and rehabilitation, while noting challenges in validation and implementation.
Contribution
The paper provides a comprehensive synthesis of AI applications in orthopedics and identifies translational gaps for ethical and equitable implementation.
Findings
AI achieves expert-level performance in detecting bone fractures and identifying implants with high accuracy.
AI-based surgical planning improves accuracy and reduces intraoperative corrections and surgery time.
Predictive models for complications and outcomes show promise but lack external validation.
Abstract
Background/Objectives: Musculoskeletal disorders and their surgical treatment significantly affect global disability, healthcare utilization, and costs. Artificial intelligence (AI) is a key enabler of data-driven musculoskeletal care. Their applications include diagnostic imaging, surgical planning, risk prediction, rehabilitation, and digital health ecosystems. This narrative review synthesizes current evidence on the use of AI in orthopaedics and musculoskeletal care across five areas: diagnostic imaging, surgical planning and intraoperative augmentation, predictive analytics and patient-reported outcomes, rehabilitation intelligence and teleorthopaedics, and system-level management. An additional task is to identify translational gaps and priorities for safe, ethical, and equitable implementation of AI. Methods: A structured narrative review was conducted using targeted searches in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
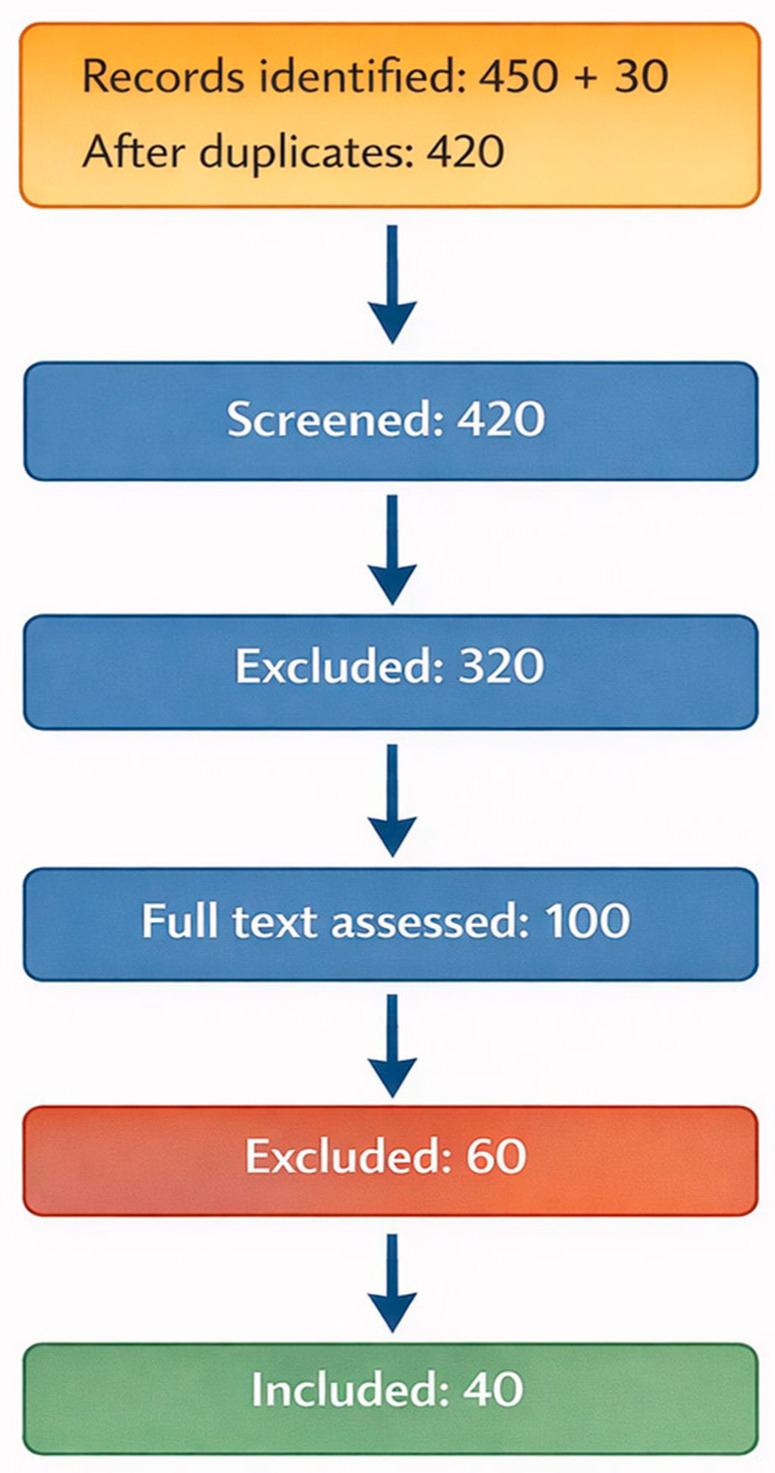 Figure 1
Figure 1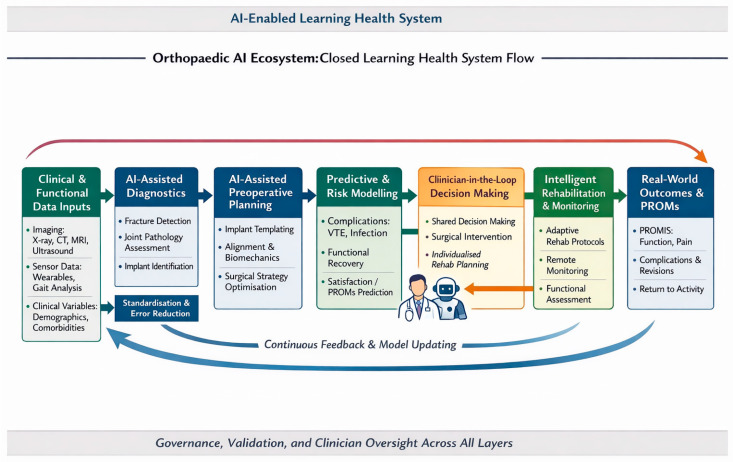 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsArtificial Intelligence in Healthcare and Education · Medical Imaging and Analysis · Radiomics and Machine Learning in Medical Imaging
1. Introduction
Musculoskeletal disorders and injuries are among the leading causes of pain and disability worldwide, leading to a significant demand for imaging services for urgent and elective surgeries and rehabilitation, thereby placing a considerable burden on healthcare systems [1,2,3,4,5]. Clinical decision-making in this field involves comprehensive radiological assessment, determination of surgical indications, postoperative observation, and long-term functional monitoring. The increased interest in data-driven tools for the digital transformation process stems from their potential to improve the consistency, scalability, and decision support throughout the orthopedic care process [6,7,8,9]. Orthopaedics is a unique field because of the importance of visual data (X-rays, CT scans, and MRIs) and biomechanical measurements. This makes it ideal for computer vision applications that use deep learning models to automatically extract features from pixel data, unlike traditional machine learning methods that require manual feature definition.
It has been observed that artificial intelligence (AI), especially deep learning and other machine learning-based methods, is advancing rapidly from theoretical concepts to practical applications in orthopaedics [8,10,11,12,13,14,15,16,17,18,19,20]. It has already been demonstrated that convolutional neural networks can achieve high accuracy in fracture detection, comparable to that of musculoskeletal radiology specialists, with overall sensitivities and specificities of approximately 90% and 92%, respectively [21,22,23,24,25]. Systems supporting elective orthopedic surgery with implant placement achieve 97–99% accuracy and can significantly speed up the planning of complex revision arthroplasty procedures [26,27,28]. AI-assisted arthroplasty planning improves implant sizing compared to conventional two-dimensional templating (manual or digital “overlaying” of implant templates onto standard two-dimensional radiographs to estimate the size and positioning of components before surgery) [29,30,31]. Compared with traditional methods, this results in a more efficient procedure, shorter operating times, reduced blood loss during surgery, and fewer intraoperative corrections in hip and knee arthroplasty [32,33,34,35]. In addition to imaging and templating, AI-based predictive models are increasingly used to assess the risks of venous thromboembolism, dislocation, readmission, and patient-reported satisfaction [36,37,38]. Integrating imaging, clinical data, signals from wearable sensors, and patient-reported outcomes (PROMs) to support personalized treatment pathways creates opportunities for multimodal structures [39,40]. The simultaneous use of teleorthopaedics and AI-assisted rehabilitation tools aims to extend specialized care to patients’ homes through remote monitoring, automatic motion analysis, and adaptive exercise guidance [41,42,43]. Despite this promising progress, clinical implementation of AI-based systems remains inconsistent. Many such systems are trained on data from a single center or demographically homogeneous datasets [44,45,46,47], lack robust multicenter external validation, exhibit algorithmic opacity, undermine clinician trust, and raise concerns regarding fairness and accountability. Workflow integration with picture archiving and communication systems (PACS), electronic health records, and surgical planning platforms is often incomplete [44,46]. Regulatory and ethical frameworks for adaptive data-driven tools are still under development. Existing reviews typically focus on single domains, such as fracture detection or arthroplasty planning, and rarely combine diagnostic, surgical, prognostic, rehabilitation, and systemic perspectives into a unified picture of orthopedic healthcare [22,23,48,49,50,51,52].
Technical Foundations of AI in Orthopaedics
To enhance the understanding, it is essential to outline the core AI techniques that are relevant to this field. Deep learning (DL), a subset of ML, uses neural networks with multiple layers to learn hierarchical features from data and has driven major advances in medical image analysis [53]. In imaging, convolutional neural networks (CNNs) are predominant for tasks such as fracture detection because they excel in processing grid-like data such as radiographs [54]. For the predictive analytics of tabular clinical data, models such as random forests or gradient boosting machines (e.g., XGBoost) are employed for risk stratification and effectively handle structured inputs [55]. These techniques typically require large labeled datasets for training, which are often augmented via transfer learning to mitigate data scarcity in orthopaedics.
In addition to these established model families, emerging architectures such as vision transformers (ViT) and hybrid CNN–transformer pipelines are increasingly employed for image classification and segmentation, particularly when long-range contextual relationships or multiview integration are crucial [56,57,58,59]. In practice, the selection of architecture involves trade-offs between data requirements, robustness, and interpretability [60,61]. CNNs typically excel in tasks characterized by high contrast and well-defined geometry (e.g., implant identification) [62,63], whereas osteoarthritis grading often entails subtle, spatially heterogeneous changes that benefit from precisely constrained regions of interest, multiscale feature extraction, and rigorous external validation [64,65,66]. For structured clinical datasets, gradient-boosting models frequently remain competitive owing to their efficacy with tabular inputs, superior calibration of uncertainty, and more accessible feature attribution than deep neural networks [67]. However, they may underperform when the predictive signal is embedded in high-dimensional imaging or multimodal data [67,68].
This structured narrative review synthesizes current evidence on AI in orthopedic and musculoskeletal practice across diagnostic imaging, surgical planning and intraoperative augmentation, predictive analysis and precision stratification, rehabilitation intelligence and teleorthopaedics, and system-level management using digital ecosystems. This study aimed to characterize the technological maturity and clinical utility of current applications, identify key translational gaps, and outline a research and implementation agenda to support the safe, ethical, equitable, and patient-centered implementation of AI in modern musculoskeletal healthcare.
2. Materials and Methods
2.1. Study Design
This study was a structured narrative review that combined a targeted literature database search with expert interpretation in the clinical and methodological domains. The synthesis was based on two complementary streams of evidence: (1) a targeted set of clinical studies on AI in orthopedic imaging, surgical planning, and predictive modeling, and (2) a thematic analysis of emerging areas, including PROM–AI integration, teleorthopaedics, and digital rehabilitation.
2.2. Search Strategy
This expert review synthesizes current evidence on the clinical applications of AI in orthopaedics and the broad treatment of musculoskeletal disorders. The search covered the period from January 2019 to December 2025, during which deep learning techniques matured into clinically applicable tools and the first regulatory approval for AI-based imaging systems was obtained [69]. This timeframe was deliberately chosen to include studies that reflected actual translational readiness rather than early concept verification.
A comprehensive literature search was conducted using PubMed, Scopus, and Web of Science databases. To increase coverage and minimize database bias, targeted semantic- and citation-based searches were performed using Semantic Scholar, OpenAlex, and Google Scholar databases. The search strategies combined controlled vocabulary and text terms related to AI, machine learning, deep learning, orthopaedics, musculoskeletal disorders, fracture detection, osteoarthritis, arthroplasty, spine surgery, outcome prediction, patient-reported outcome measures (PROMs), PROMIS, telemedicine, teleorthopaedics, and digital rehabilitation.
2.3. Eligibility Criteria and Study Selection
Eligible articles comprised original research evaluating AI-based tools or models with direct applicability to clinical practice in orthopaedics, including diagnostic imaging, preoperative planning, risk prediction, rehabilitation, and outcome assessment. Both retrospective and prospective clinical studies were deemed eligible for inclusion. Exclusions were made for conference abstracts, editorials, articles focused solely on algorithm development without clinical validation, and publications in languages other than English. Titles and abstracts were screened to exclude studies outside the scope of clinical orthopaedics and musculoskeletal patient care. Animal studies, investigations focused purely on engineering without a clinical framework, studies on robotics or navigation systems lacking elements pertinent to clinical decision-making, and image-processing studies without clinical validation were excluded from the review. Some included articles, particularly review articles, were used to inform contextual synthesis but were not subjected to primary quantitative data extraction.
The main reasons for full-text exclusion after eligibility assessment are summarised in Supplementary Table S1. The categorisation in Supplementary Table S1 reflects the dominant reason for excluding each full-text article; when multiple exclusion criteria were applied, studies were assigned to the most clinically relevant category.
The reference lists of the included articles and recent high-quality reviews were manually screened to identify additional relevant studies not captured by the electronic search. Full-text articles were assessed for conceptual relevance, availability of quantitative performance data, and translational implications of the results. Rather than applying rigid eligibility thresholds, a priority-based approach was adopted that emphasized clinical relevance. Preference was given to studies reporting diagnostic performance metrics (e.g., sensitivity, specificity, area under the curve), benefits in surgical planning compared with conventional methods, predictive differentiation of outcomes or complications, measurable impact on clinical workflow, or conceptually robust frameworks for rehabilitation and precision medicine. The included studies demonstrated broad geographical representation, with research conducted in the United States, Europe, and Asia (including Sweden, Austria, France, The Netherlands, China, Thailand, India, Japan, and Singapore). Sample sizes varied widely, ranging from small proof-of-concept cohorts (n = 12) to large-scale systematic reviews encompassing more than one million implants. Study quality was assessed using the modified Methodological Index for Non-Randomized Studies (MINORS) or the Newcastle–Ottawa Scale for non-randomized studies [70]. These instruments were applied qualitatively to contextualize the strength of evidence and recurrent sources of bias across study designs rather than to generate pooled scores or exclude studies based on numerical thresholds. From the pool of eligible publications, 40 studies were selected as the evidence base for a detailed narrative synthesis.
2.4. Data Extraction and Synthesis
Each selected study was analyzed in terms of the area of AI application (diagnostic imaging, surgical planning, predictive analytics, rehabilitation, or system-level), orthopedic specialty, anatomical area, basic AI methodologies, data modality, study design and validation level, quantitative performance metrics, and patient-reported clinical outcomes or workflow impact. A structured organization of predefined data elements was used. All collected information was verified by the authors and placed in context to ensure the clinical accuracy and interpretability of the data.
In this study, it was not possible to combine quantitative data due to significant heterogeneity in model architectures, datasets, and endpoints. The results were synthesized in narrative form, with greater interpretive weight given to empirically verified clinical trials and feasibility studies than to other studies. Simultaneously, new and rapidly evolving ideas, such as integrating patient-reported outcomes (PROMs) with AI, developing tele-orthopedic teaching systems, modeling biological responses, and using digital twin technologies, have been considered preliminary or exploratory. In other words, these concepts were treated as areas that generated hypotheses that required further research and validation before being translated into clinical practice.
2.5. Organization and Evaluation of Evidence
The results were categorized into five thematic areas to facilitate coherent synthesis and identify translational gaps: (1) AI-based diagnostic imaging; (2) surgical planning and intraoperative augmentation; (3) predictive analytics and precision stratification; (4) rehabilitation intelligence and remote monitoring; and (5) system-level management, ethics, and future research directions. The study identification, selection, and inclusion processes are summarized in a PRISMA-inspired flow diagram (Figure 1).
No formal quantitative grading of evidence (e.g., GRADE or AMSTAR) was conducted because the primary objective was comparative clinical interpretation rather than effect-size aggregation. Instead, studies were qualitatively assessed based on the strength of their clinical signals, with a clear distinction between empirical outcome studies, feasibility studies supported by empirical results, and conceptual or framework-based contributions to the literature.
A formal meta-analysis was not performed due to substantial heterogeneity across study designs, data sources, AI architectures, outcome measures, and validation strategies. Consequently, the results were synthesized narratively, with an emphasis on clinical performance indicators, validation levels, generalizability, and implementation readiness.
The main reasons for excluding full texts are summarized in Supplementary Table S1.
Because this work is a structured narrative review, the flow diagram is intended to increase transparency in the identification and selection of studies. However, the review did not claim formal PRISMA compliance and did not provide a quantitative meta-analytic synthesis.
Grammarly and PaperPal were used for grammatical and stylistic corrections.
3. Results
3.1. Evidence-Based Review
A narrative synthesis of 40 studies was conducted to reflect the current scope, maturity, and complexity of artificial intelligence applications in orthopaedics. Qualitative assessment using the modified Methodological Index for Non-Randomized Studies (MINORS) and Newcastle–Ottawa Scale revealed that the overall methodological quality of the included studies was predominantly moderate. Approximately two-thirds of the studies met the basic criteria for internal validity, whereas only seven of 40 (17.5%) satisfied the key criteria for a prospective design or external multicenter validation. A qualitative overview of the recurrent methodological strengths and limitations identified using these tools is presented in Supplementary Table S2.
Regarding study design, seven studies (17.5%) utilized prospective or multicenter validation approaches, including randomized controlled trials and clinical trials. The remaining evidence was predominantly composed of retrospective, single-center studies, and development or internal validation cohorts. Common methodological limitations included small sample sizes, lack of prospective validation, incomplete reporting of model calibration, uncertainty, and failure modes.
The evidence base comprised systematic reviews and meta-analyses, cohort and validation studies, randomized controlled trials, and clinically oriented feasibility studies. As summarized in Table 1, most studies have focused on diagnostic imaging and surgical planning, with a small but growing body of evidence on predictive modeling, rehabilitation, and system-level applications.
3.2. Diagnostic Imaging Using AI
The most mature and clinically relevant evidence concerns the use of AI in musculoskeletal imaging, particularly in the radiographic detection of fractures [25,47,49,51,52,54,55], implant identification [56,57,58], and osteoarthritis classification [105,106]. In many studies, deep learning systems have achieved a fracture detection sensitivity of approximately 90% and specificity of approximately 92%, with area under the curve values approaching 0.97, matching those of experienced clinicians, outperforming less experienced specialists, and providing millisecond-level inference times [107].
The differences in results across individual studies can be attributed to several factors, including differences in image acquisition and preprocessing protocols, case diversity, and disease prevalence, the method used to determine objective truth (whether through expert consensus or clinical observation/CT), and discrepancies in external validation strategies.
AI algorithms for orthopaedic implant identification demonstrate even higher performance, with reported accuracies of 97–99%, and can substantially accelerate the planning of complex revision arthroplasty procedures [73,108]. In contrast, AI-based classification of knee osteoarthritis, which is clinically useful and associated with improved inter-observer agreement compared with manual assessment, generally achieves lower performance, with reported accuracies of up to 93% [105,109,110]. However, deep learning models must be trained in the selected areas of interest. Otherwise, they lack precision and struggle to identify significant changes that are indicative of osteoarthritis [111]. This discrepancy seems to stem not from the sophistication of the algorithms but from the fundamental differences in image characteristics and task structure. Orthopedic implants are characterized by smooth, well-defined edges, high signal contrast, and a limited set of repetitive shapes, which closely match the strengths of convolutional neural networks in detecting high-contrast global patterns [112]. In addition, image preprocessing strategies, such as contrast enhancement, may further improve recognition in challenging scenarios, including cases of cement adhering to implant surfaces [113]. In contrast, osteoarthritic changes are spatially heterogeneous, gradually evolving, and lack clear geometric boundaries, rendering reliable classification inherently more complex and sensitive to disease stage and imaging variability [114]. Notably, many imaging models continue to rely on single-center datasets and have limited external multicenter validation, further limiting their generalizability.
3.3. Surgical Planning and Intraoperative Augmentation
Evidence confirms the significant benefits of AI-assisted planning for hip and knee arthroplasties and their early application in spinal deformity surgeries. In total hip arthroplasty, AI-based preoperative templates and segmentation improved component sizing and positioning compared to manual planning, increasing the acetabular component fit from approximately 30 to 57% to 66% to 90% and enabling the prediction of tibial and femoral components in total knee arthroplasty with an accuracy of approximately 92.9% compared to approximately 45% for manual planning [31,81,115]. AI-assisted planning is associated with shorter operating times (approximately 12 min), reduced blood loss during surgery (approximately 50 mL), and a 40% reduction in intraoperative revisions, with a slight improvement in postoperative functional outcomes [115,116]. In contrast, preliminary data on spinal surgery suggest a potential reduction in blood loss and length of hospital stay in these patients.
3.4. Predictive Analysis and Precise Stratification
Predictive models in orthopaedics address postoperative complications, readmissions, eligibility for arthroplasty, and patient-reported outcomes, such as satisfaction and return to functional fitness [117,118,119]. The reported area under the curve values for venous thromboembolism (VTE) after endoprosthesis replacement range from approximately 0.71 to 0.982, indicating moderate to excellent discriminatory ability [95,120]. Models predicting the risk of dislocation after hip arthroplasty achieved approximately 95% accuracy, while eligibility models achieved approximately 87.8% accuracy, with AUC values of 0.97–0.98 [76,121]. Despite these promising indicators, most predictive models have been developed and validated internally in single-center cohorts with limited external validation, and virtually no prospective impact studies have been conducted. The conceptual framework for predicting biological responses in regenerative orthopaedics remains in the hypothesis-generation phase.
3.5. Rehabilitation Intelligence and Teleorthopaedics
The applications of AI in rehabilitation [14,41,122] and teleorthopaedics demonstrate that orthopedic care can extend beyond hospitals to patients’ homes and communities [123]. Computer vision systems applied to video recordings can quantify gait asymmetry and joint range of motion [124]. Platforms based on wearable sensors and AI algorithms are being explored for adaptive rehabilitation planning, adherence monitoring, and early detection of suboptimal recovery [125,126,127]. However, the current evidence is limited, largely due to the small number of pilot studies with limited links to long-term outcomes. Teleconsultation platforms that integrate simple AI-based tools to measure range of motion or medical segregation may improve access to care in underserved regions but raise concerns about digital exclusion, data security, and clinical accountability for remotely supervised programs [128,129]. The feasibility of thermal imaging applications is still in its early stages of development.
3.6. System-Level Governance, Ethics, and Future Trajectories
In addition to individual applications, the literature highlights significant system-level barriers related to data quality, interoperability, regulatory oversight, and clinician trust. Many orthopedic AI systems have been developed using data from a single center or homogeneous datasets, which limits their overall utility and may exacerbate bias if underrepresented populations are not adequately included [130,131]. The lack of explainability and the “black box” nature of algorithms often constitute significant barriers to their acceptance in high-risk decision-making environments. In addition, the implementation of such solutions is hampered by fragmented clinical workflows, changing regulations on software as a medical device, and insufficient systematic postmarket surveillance. This highlights the need for multicenter training datasets, methods that are easy to explain to clinicians, implementation of science research, and long-term concepts, such as learning teleorthopedic systems and “digital twins” of patients [12,132]. Table 1 summarizes the study types, primary AI applications, and anatomical regions of the 40 included studies.
Systematic reviews were included for contextual synthesis, and primary quantitative extraction focused on original clinical studies.
A summary of diagnostic AI applications in orthopaedics is presented in Table 2.
AI-assisted-surgical planning and intraoperative augmentation are shown in Table 3.
The predictive analytics and precision stratification in orthopaedics are presented in Table 4.
AI-enabled rehabilitation and teleorthopaedics are listed in Table 5.
Table 6 presents the system-level, governance, and implementation frameworks for orthopaedic AI.
The future research agenda derived from expert synthesis is presented in Table 7 below.
Table 8 presents a comparative analysis of outcomes from conventional image interpretation and those enabled by AI support. The data in Table 8 indicate that AI contributes to enhanced performance, improved accuracy, training standardization, and expedited workflows. Nevertheless, the implementation of AI remains dependent on its validation and integration. The reported time metrics correspond to values observed under study-specific or experimental conditions and should not be misconstrued as representing the total duration of clinical workflows.
It is essential to differentiate between the inference time and the entire clinical workflow duration, which includes image transfer, result evaluation, management of false positives, and subsequent clinical decision-making.
4. Discussion
4.1. Key Findings and Maturity of Evidence
The key message of this review is that AI in orthopaedics can provide the greatest clinical value when applied to well-defined, standardized tasks with clear validation pathways, thereby augmenting physicians [156]. By contrast, performance and reliability decline as clinical complexity, contextual variability, and the diffusion of responsibility across care processes increase in the healthcare system. This narrative review indicates that AI in orthopaedics is the most clinically mature in diagnostic imaging [8,45,52,98,131,157,158,159,160,161] and arthroplasty planning [11,35,74,115,162,163], where deep learning systems consistently achieve expert-level performance in fracture detection [25,50,52,88,159,160,164,165,166], implant identification [73,167,168,169,170,171], and component template creation [29,30,31]. AI can reduce diagnostic delays [161], planning errors [147,161,169], and perioperative burdens [130]. In contrast, predictive analytics [93,112,172,173], rehabilitation intelligence [116,122,174,175,176], and digital ecosystem concepts (Figure 2), such as learning systems [173,177] or digital twins [157,178], remain at an earlier stage of development, supported mainly by proof-of-concept studies with limited multicenter validation or prospective impact data.
4.2. Comparison with Previous Works
Previous reviews have typically focused on individual elements of the orthopedic care pathway, such as radiographic analysis [61,127,132,141,142], knee or hip arthroplasty planning [26,91,124,143,144,145], and general machine-learning-based predictive models [179]. In contrast, this review integrates AI applications in diagnostic imaging [8,48,180,181], surgical planning [12,28,35,44,84,182], risk prediction [173,174,183,184,185], rehabilitation [5,14,41,43,181], and system-level management. It explicitly links these to PROM integration [7,14,153], teleorthopaedics [154,186], and new concepts in learning-based healthcare systems, thereby highlighting the maturity of each area. Many previous reviews have focused on the application of AI in various orthopedic subspecialties. In contrast, this synthesis emphasizes the degree of translational readiness, which is influenced more by task structure and validation feasibility than algorithmic complexity.
4.3. Technical Challenges in AI Implementation
Despite significant advances, several technical hurdles impede the translation of AI into routine orthopaedic practice. One major issue is overfitting owing to relatively small or biased datasets, underscoring the need for approaches such as federated learning to pool data across institutions without sharing sensitive patient information [156,157]. Additionally, the “black-box” nature of many AI models raises concerns; explainable AI (XAI) techniques (e.g., SHAP value analysis or LIME) are required to interpret model decisions, thereby enhancing clinician trust in AI outputs [187].
4.4. Clinical and Healthcare System Implications
For clinicians, the most immediate opportunities arise from implementing AI to streamline existing processes in radiology and arthroplasty planning [20], where tools can standardize templates [29], prioritize cases, and support less-experienced readers without replacing human judgment.
AI-based teleorthopedic pathways can improve remote medical triage [188,189], range-of-motion assessment [155], and rehabilitation monitoring [41,189,190]. However, implementing these systems requires establishing a robust governance and accountability framework to ensure data security and support digital inclusion [171,172,173], thereby mitigating the risk transferred from institutions to patients and physicians [191,192].
From a healthcare perspective, AI-based risk stratification [148] and PROM-based prediction models [159] may ultimately support personalized thromboprophylaxis [36,37,109], joint decision-making regarding arthroplasty candidates [20,193,194], and more efficient resource allocation. In contrast, teleorthopedic and rehabilitation applications remain constrained by limited validation, contextual variability, and unresolved questions regarding digital equity, data security, and clinical responsibility in remote care models [161,179]. The results emphasize that the effective use of AI in orthopaedics depends not only on the sophistication of the algorithms themselves, but also on clearly defined tasks, robust validation strategies, and effective integration of these tools into existing clinical and organizational frameworks. Even more important than the “sophistication” of the models is whether we know exactly what they are supposed to be used for, how reliably we check their performance, and how we fit them into a real-world workflow. Expanding the use of AI beyond narrowly defined tasks without adequate validation and oversight can undermine physician trust in these systems and ultimately harm the quality of care. Although quantitative data pooling (meta-analysis) was infeasible owing to study heterogeneity, we deliberately prioritized the qualitative synthesis of AI model architectures and use cases. This approach provides technical insights that are often missing from clinical reviews.
4.5. Economic and Implementation Considerations
Current evidence on the cost-effectiveness of artificial intelligence (AI) in orthopaedics remains limited and highly context-dependent [195,196,197]. Although imaging triage and arthroplasty planning tools have the potential to mitigate delays, reduce rework, and decrease planning variability, the overall economic impact is influenced by the local baseline performance [198,199], case volume, and degree of workflow integration, including PACS/EHR [112], reporting, and liability pathways [79,195]. Initial costs, such as licensing, integration, cybersecurity, and staff training, as well as ongoing maintenance expenses, including monitoring, model updates, and post-market surveillance, are often underreported, thereby constraining comprehensive health technology assessments [26,79,195,200,201,202].
From an institutional standpoint, the business case for AI is generally most compelling when it demonstrably alleviates bottlenecks, such as radiology turnaround time and revision planning time, or standardizes performance for less-experienced practitioners [74,196,201,203,204]. However, financial incentives may be misaligned if cost savings benefit one stakeholder while another incurs implementation costs. Consequently, future evaluations should incorporate economic endpoints alongside clinical outcomes, encompassing resource utilization, time-to-decision, complication-related costs, and patient-reported values [205,206].
4.6. Strengths and Limitations of This Review
The structured narrative, broad thematic scope covering the entire spectrum of orthopedic patient care from imaging, surgery planning, prognosis, rehabilitation, and treatment within a single coherent structure, and the adoption of clear performance indicators and clinically relevant endpoints can be considered strengths of our review.
However, this was not a formal systematic review and did not constitute exhaustive or quantitative synthesis. The evidence base remains dominated by retrospective single-center studies based on carefully selected datasets with limited demographic and institutional diversity. The review was based solely on English-language literature and did not consider studies from gray literature or other languages. Consequently, residual selection and classification biases cannot be excluded. The impact of incomplete consideration of relevant evidence, particularly in areas with heterogeneous imaging protocols, variable annotation standards, and limited external validation, cannot be ruled out.
Several additional limitations of this study should be considered when interpreting these results. Studies vary considerably in terms of the input data, reference standards, outcome definitions, and reporting practices. Image acquisition parameters, real-world annotation strategies, and performance metrics have not been analyzed in sufficient detail, making it difficult to compare models and meaningfully aggregate results. In many areas, the reported accuracy likely reflects optimization for specific tasks rather than the actual clinical performance. Few studies have included rigorous external validation, prospective evaluation, or direct comparison with established clinical processes. It can also be assumed that high algorithm performance does not necessarily translate into better patient outcomes, greater efficiency, or better decision quality. This gap is particularly evident in predictive analytics, rehabilitation intelligence, and teleorthopaedic applications, where long-term outcomes and contextual factors are critical. In addition, many studies have provided limited information on transparency, explainability, fairness, and other ethical issues. Despite growing regulatory and ethical expectations, there is a lack of systematic assessment of bias, interpretability, and failure modes, making it difficult to predict unintended consequences and potentially undermining clinicians’ trust in AI. This may be particularly relevant when AI systems are deployed outside of narrowly defined use cases. Overall, the current literature reflects an evolving, methodologically heterogeneous field, and the reported results should be interpreted with caution when extrapolating to routine clinical practice.
Another concern is the apparent optimism in many early-stage studies, often authored by the same teams that developed the evaluated algorithms. Although these studies often demonstrate high performance under controlled conditions, they may be biased by optimism resulting from the favorable selection of datasets, task formulation, or evaluation protocols tailored to the strengths of the proposed methods. Consequently, the actual performance in heterogeneous clinical settings with unknown data distribution and daily workflow constraints may be significantly lower than previously reported. This highlights the need for independent validation, external replication, and prospective evaluation to distinguish true clinical utility from proof-of-concept results and to avoid overestimating the capabilities of current AI systems that can be safely delivered in practice.
4.7. Generative AI
Emerging Generative AI tools warrant consideration in orthopaedics. Although current applications are dominated by discriminative models (for classification or segmentation), generative approaches, including large language models (LLMs), are beginning to assist with clinical documentation and decision support. For example [207], preliminary studies have shown that LLMs can draft discharge summaries and operative reports significantly faster than clinicians, while maintaining comparable quality. These models could reduce administrative burdens and improve patient communication, although issues such as content ‘hallucinations’ and the need for rigorous validation currently limit their clinical deployment [208].
4.8. Directions for the Future
Future research should prioritize the prospective multicenter validation of imaging and preoperative planning algorithms. However, the current body of evidence has been limited by insufficient external validation. Therefore, future studies should employ pragmatic designs, such as stepped-wedge cluster-randomized trials or multicenter prospective cohort studies, to assess the real-world clinical impact of routine workflows.
The evaluation should extend beyond the diagnostic accuracy. Key outcomes include patient-reported outcome measures, complications and safety endpoints, time-to-decision, workflow efficiency, downstream healthcare utilization (e.g., additional imaging or re-consultations), and economic outcomes relevant to hospitals and payers.
Validation should not rely solely on a single test. Regular local reevaluation at individual centers is necessary to account for dataset shifts, evolving practice patterns, and changes in the patient population. Research should transition from isolated case reports to implementation-focused studies that assess the impact of AI on treatment outcomes, clinician behavior, and resource utilization.
In the fields of rehabilitation and teleorthopedics, robust prospective studies are required to determine whether remote monitoring and AI-supported adaptive therapy can enhance clinical outcomes and improve patient safety. At the health-system level, future work should address regulatory adaptation, transparent and interpretable model design, continuous post-market oversight, and the integration of patient-reported outcomes and real-world evidence into learning health systems to ensure the safe, ethical, and equitable deployment of AI technologies.
At the system level, it is critical to adapt to changing regulations; develop transparent and understandable models; conduct ongoing oversight after innovations are introduced to the market; and integrate patient-reported outcomes (PROMs) and real-world evidence into health education systems to ensure the safe, ethical, and equitable implementation of these solutions.
5. Conclusions
AI in orthopaedics and in the care of patients with musculoskeletal disorders has reached clinical maturity in terms of diagnostic imaging and arthroplasty planning. In these areas, algorithms can consistently achieve expert-level results, leading to measurable improvements in efficiency and perioperative decision-making. In contrast, areas such as predictive analytics, rehabilitation intelligence, and teleorthopaedic applications are still at an early stage of translational readiness. However, their development is hampered by limited external validation, biased or narrowly representative datasets, and a lack of transparency in algorithmic decision-making processes. The transition from proof-of-concept implementations to reliable clinical services will rely, to some extent, on further improvements in the algorithm performance. However, to a large extent, implementation will require robust multicenter prospective evaluations, repeatable local validations, systematic assessments of fairness and explainability, and clinically meaningful integration of PROM and sensor data. Under these conditions, AI is well-positioned to complement, rather than replace, orthopedic knowledge, thereby supporting more consistent, patient-centered, and value-based musculoskeletal care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nguyen A. Lee P. Rodriguez E.K. Chahal K. Freedman B.R. Nazarian A. Addressing the growing burden of musculoskeletal diseases in the ageing US population: Challenges and innovations Lancet Healthy Longev.2025610070710.1016/j.lanhl.2025.10070740381641 · doi ↗ · pubmed ↗
- 2Malik K.M. Beckerly R. Imani F. Musculoskeletal Disorders a Universal Source of Pain and Disability Misunderstood and Mismanaged: A Critical Analysis Based on the U.S. Model of Care Anesth. Pain Med.20188 e 8553210.5812/aapm.8553230775292 PMC 6348332 · doi ↗ · pubmed ↗
- 3Kumar R. Marla K. Sporn K. Paladugu P. Khanna A. Gowda C. Ngo A. Waisberg E. Jagadeesan R. Tavakkoli A. Emerging Diagnostic Approaches for Musculoskeletal Disorders: Advances in Imaging, Biomarkers, and Clinical Assessment Diagnostics 202515164810.3390/diagnostics 1513164840647646 PMC 12248478 · doi ↗ · pubmed ↗
- 4Gill T.K. Tabish M. Global, regional, and national burden of other musculoskeletal disorders, 1990–2020, and projections to 2050: A systematic analysis of the Global Burden of Disease Study 2021 Lancet Rheumatol.20235 e 670e 68210.1016/S 2665-9913(23)00232-137927903 PMC 10620749 · doi ↗ · pubmed ↗
- 5Lee Y.K. Yoon E.-J. Kim T.H. Kim J.-I. Kim J.-H. Musculoskeletal Digital Therapeutics and Digital Health Rehabilitation: A Global Paradigm Shift in Orthopedic Care JCM 202514846710.3390/jcm 1423846741375770 PMC 12693369 · doi ↗ · pubmed ↗
- 6Meara J.G. Leather A.J.M. Hagander L. Alkire B.C. Alonso N. Ameh E.A. Bickler S.W. Conteh L. Dare A.J. Davies J. Global Surgery 2030: Evidence and solutions for achieving health, welfare, and economic development Lancet 201538656962410.1016/S 0140-6736(15)60160-X 25924834 · doi ↗ · pubmed ↗
- 7Zarghami A. Role of Artificial Intelligence in Surgical Decision-Making: A Comprehensive Review: Role of AI in SDM Galen Med. J.202413 e 333210.31661/gmj.v 13i.3332 · doi ↗
- 8Zhang X. Yang Y. Shen Y.W. Zhang K.R. Jiang Z.K. Ma L.T. Ding C. Wang B.Y. Meng Y. Liu H. Diagnostic accuracy and potential covariates of artificial intelligence for diagnosing orthopedic fractures: A systematic literature review and meta-analysis Eur. Radiol.2022327196721610.1007/s 00330-022-08956-435754091 · doi ↗ · pubmed ↗