Seizure Clusters: Current Concepts in Definition and Treatment
Gemma Bassani, Elena Pasini, Barbara Mostacci, Lidia Di Vito, Lorenzo Ferri, Lorenzo Muccioli, Francesca Bisulli

TL;DR
Seizure clusters are sudden increases in seizure frequency and require prompt treatment, but managing them is complicated by inconsistent definitions and treatment approaches.
Contribution
The paper reviews current definitions and treatments for seizure clusters across different clinical settings and highlights the need for standardized protocols.
Findings
Outpatient treatments like diazepam nasal spray and midazolam nasal spray show similar efficacy but lack head-to-head comparisons.
Inpatient management aligns more closely with status epilepticus protocols, emphasizing intravenous benzodiazepines.
Geographic drug availability differences hinder universal treatment guidelines for seizure clusters.
Abstract
Seizure clusters (SCs) are an acute and transient increase in seizure frequency relative to an individual patient’s baseline and are associated with an increased risk of injury, morbidity, and potentially mortality if not promptly and adequately treated. Despite their clinical importance, the management of SCs remains highly heterogeneous, primarily due to the absence of a universally accepted definition, which is determined also by the wide variability in seizure semiology and baseline individual burden;, as well as by differences in care settings. Outpatient treatment relies largely on caregivers’ ability to recognize SCs and administer rescue medication, whereas inpatient management may also involve invasive routes of administration. We conducted a literature review identifying 32 original articles addressing the treatment of SCs. The analysis focused on definitions, efficacy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
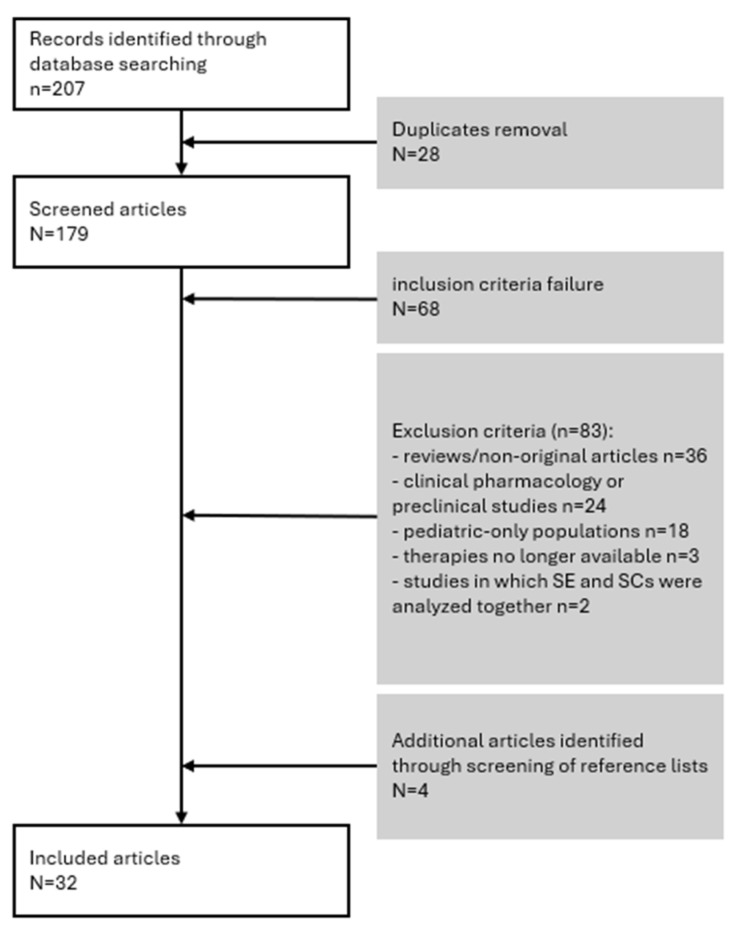 Figure 1
Figure 1| Treatment | Study | Study Design | N. Patients | N. Treated SCs | SC Definition | Seizure Type |
|---|---|---|---|---|---|---|
| MDZ-NS (5 mg, ±second 5 mg dose) | Wheless et al. [ | Open-label extension trial (single arm) | 161 | 1998 *: 1291 with single dose; 797 with a second dose | ≥2 seizures/6 h | focal or generalized |
| Detyniecki et al. [ | Phase 3 RCT double blind (vs. placebo 2:1) | 67 in placebo, 133 in MDZ | NA | ≥2 seizures/6 h | focal or generalized | |
| DZP-NS (5, 10, 15 or 20 mg depending on age and weight, ±second dose) | Wheless et al. [ | Phase 3, open-label, repeat-dose safety study | 163 * (NA, 23.1 years); 54.6% females | 3853 * | NA | NA |
| Liow et al. [ | Post hoc cohort analysis 3 | NS [ | 485 | ≥2/24 h | NA | |
| Jarrar et al. [ | Post hoc cohort analysis 3 | NA | 727 | Prolonged seizures | NA | |
| DZP-NS (5–20 mg according to age and weight) and MDZ-NS (5 mg) | Li et al. [ | Retrospective | 39 in DZP-NS, 38 in MDZ-NS (NA, median 25 and 27 years for DZP and MDZ respectively), and 46–58% females | NA | NA | NA |
| LZP oral solution 0.5–2 mg/dose (65% 1 mg, 29% 2 mg) | Lelis et al. [ | Retrospective, single centre | 48 (100%; 37.8 years); 40% females. 32 sublingual, 11 buccal, and 5 oral administration. | NA | Individual definition: | NA |
| BZD real world use | Chiang et al. [ | Retrospective from Seizure Tracker database | 220 (NA, 14.4 years); 52.7% females | 10,889 rescue medication administrations | ≥2/4 h or ≥2/6 h or ≥2/24 h | Focal impaired awareness seizures and bilateral tonic–clonic seizures |
| DZP rectal gel | Fakhoury et al. [ | Retrospective, single centre | 50 (100%; 34.7 years); 52% females | NA | NA | NA |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEpilepsy research and treatment · Pharmacological Effects and Toxicity Studies · Neuroscience and Neuropharmacology Research
1. Introduction
A seizure cluster (SC), also referred to as acute repetitive seizures (ARS), is generally defined as a sudden increase in seizure frequency compared with an individual patient’s baseline, with recovery of the usual neurological status during the interictal period. Despite this general definition, and although SCs are frequently encountered in both outpatient and acute care settings, standardized diagnostic criteria are lacking.
SCs represent a substantial clinical and societal burden. For people with epilepsy (PWE) and their caregivers, their occurrence is often associated with significant psychological distress, anxiety, and a reduced sense of control over the disease. These factors negatively affect quality of life, daily functioning and productivity [1]. In particular, epidemiological data indicate that PWE with a history of SC are at significantly higher risk of developing status epilepticus (SE) than those without such a history (44% vs. 13%) [2]. Moreover, another interesting study underlies a strong association between SCs and a previous history of convulsive SE [3]. This association has also raised concerns about potential increase in mortality and the risk of sudden unexpected death in epilepsy (SUDEP) [4,5,6].
A history of SCs has been significantly associated with seizure-related hospitalization, independently of convulsive SE [3], whereas the use of rescue medication was significantly associated with fewer injuries and Emergency Department visits [7].
Several risk factors for SC have been consistently identified. These include drug-resistant epilepsy, a prior history of SE, and high baseline seizure frequency [8,9]. Additional factors—such as sleep deprivation, concomitant systemic disease, medication non-adherence, and hormonal influences—have also been implicated; however, the supporting evidence remains inconsistent [10]. The association between SC occurrence and the localization of the seizure onset zone in focal epilepsies is still unclear, as the literature reports conflicting or inconclusive findings [3,10,11].
The reported prevalence of SC varies widely, ranging from approximately 3% among PWE in large population-based studies to 46% in tertiary epilepsy centres [7,11,12,13,14]. This variability reflects differences in studies’ designs, patient populations, and clinical settings, as well as heterogeneity in the operational definitions of SC. A major challenge in both research and clinical practice is the absence of a universally accepted definition. So-called “empirical” or “clinical” criteria differ substantially across studies with regard to the number of seizures required to define a cluster and the time interval considered [9,10,13]. The commonly adopted empirical/clinical criteria include the following:
- Two or more seizures within 24 h;
- Two or more seizures within 6 h [15,16];
- Two to four seizures within 48 h;
- Two generalized tonic–clonic seizures or three focal seizures with impaired awareness within 4 h [9,10].
Alternatively, “statistical definitions” are based on deviations from an individual patient’s baseline seizure frequency [10].
A recent expert consensus on the outpatient management of SCs and prolonged seizures proposed defining SCs as an “abnormal increase in seizure frequency compared with the individual patient’s usual seizure pattern,” explicitly rejecting time-based definitions [17]. Clinicians are therefore encouraged to develop personalized treatment strategies, commonly referred to as Acute Seizure Action Plans (ASAPs) [18,19,20,21,22]. An ASAP is a written document developed in collaboration with the patient and caregivers. It describes the individual seizure pattern, specifies situations requiring rescue treatment and clarifies when emergency medical assistance should be sought [23]. In addition to improving clinical management, ASAPs may provide significant economic benefits [7].
The consensus also distinguished two therapeutic strategies. The first, termed ACT (Acute Cluster Treatment), aims to prevent additional seizures within a cluster. The second, termed REST (Rapid and Early Seizure Termination), is intended to stop an ongoing seizure. This distinction enables the categorization of medications according to their time to peak plasma concentration and duration of action, and supports the selection of the most appropriate route of administration for specific clinical scenarios. REST medications should exert their effect within approximately 2 min to achieve seizure termination [17].
Benzodiazepines (BZDs) remain the cornerstone of acute treatment, because of their rapid antiseizure activity and well-established efficacy. However, their pharmacokinetic profiles differ according to the specific molecule and formulation. Some BZDs (e.g., clobazam and clonazepam) are commonly used for the treatment of SCs despite lacking a specific regulatory indication. The availability of benzodiazepines and their routes of administration vary considerably across regions and healthcare systems (see Table 1). Consequently, the real-world management of SCs is highly heterogeneous. This variability is further driven by the abovementioned absence of a standardized definition. Additional factors, including caregiver education, patient comorbidities, disease severity, and access to healthcare services, also contribute to differences in treatment approaches.
In hospital settings, including Emergency Departments (ED) and Epilepsy Monitoring Units (EMU), treatment decisions are also influenced by the availability of intravenous access, monitoring capabilities, and local institutional protocols. The absence of standardized approaches may delay effective intervention and increase the risk of progression to SE.
In light of these challenges, a comprehensive and critical synthesis of the available evidence is essential to guide clinical decision-making. This review analyzes the current literature on the treatment of SCs in adult patients, with particular emphasis on pharmacological rescue therapies. Specific attention is given to differences between outpatient and inpatient settings, including EDs and EMUs, in order to address setting-specific issues related to drug availability, feasibility, and clinical priorities.
2. Methods
2.1. Search Strategy and Eligibility Criteria
A PubMed search was conducted in April 2025 using the following search strings: “(acute repetitive seizures [Title/Abstract]) NOT (veterinary)” and “(seizure cluster [Title/Abstract]) NOT (veterinary)”. The aim was to identify original studies reporting treatment options for SCs. Only articles published in English from 2005 onward were included to capture contemporary treatment strategies. The following exclusion criteria were applied:
- Review articles and other non-original contributions;
- Clinical pharmacology or preclinical studies;
- Studies exclusively involving pediatric populations, as the present review focuses on adult patients. Studies including both adults and pediatric patients were considered eligible; in such cases, the mean age of the overall study population was reported;
- Studies investigating therapies no longer available;
- Studies in which status epilepticus and SCs were analyzed as a single combined group.
2.2. Article Selection
The articles’ eligibility was assessed by a single reviewer (GB) through a two-step process: (1) the screening of the title and abstract and (2) full-text evaluation. Studies that clearly did not meet the inclusion criteria or clearly fulfilled any exclusion criteria were removed during the initial screening. The remaining articles underwent full-text review. The reasons for exclusion were documented and independently verified by a second reviewer (EP) to ensure accuracy. The reference lists of included studies were also examined to identify additional relevant publications. The final set of studies included in the analysis was reviewed and approved by all authors.
2.3. Data Analysis
Each study was assessed according to the following variables: study design, sample size, sex distribution, age, clinical setting (outpatient, Emergency Department, or Epilepsy Monitoring Unit), definition of SCs, seizure type, the inclusion of SE or other seizure emergencies, etiology, the inclusion of patients in whom SCs represented the first manifestation of epilepsy, baseline seizure frequency, SC treatment strategy, the number and type of antiseizure medications (ASMs), hospitalization, and diagnostic investigations.
Efficacy outcomes included all reported measures, such as time to drug administration, time to seizure cessation, seizure recurrence at 6, 12, and 24 h, need for a second dose within 6, 12, or 24 h, progression to SE, hospitalization, and drug-related adverse events (AEs).
3. Results
3.1. Study Selection
The PubMed search identified 207 articles. After removing 28 duplicates, 179 abstracts were screened. Of these, 68 were excluded as they did not meet the inclusion criteria, and 83 were excluded based on the predefined exclusion criteria: 36 were reviews or non-original articles, 24 were clinical pharmacology or preclinical studies, 18 involved pediatric-only populations, 3 investigated therapies no longer available, and 2 analyzed SE and SCs together.
The screening of reference lists identified four additional eligible publications [17,28,29,30]. Following the full-text review, a total of 32 articles were included in the analysis. Figure 1 illustrates the studies selection process.
3.2. Outpatient Management
Of the 32 selected studies, 22 (68.8%) focused on the outpatient setting. In these studies, medications were administered primarily by caregivers, and less frequently were self-administered by patients. All the studies evaluated BZDs, and diazepam (DZP) was evaluated in 15 studies and midazolam (MDZ) in 5 studies. In 19 of the 22 studies, BZDs were delivered via the intranasal (IN) route. The studies’ characteristics —including the design, sample size, and SC definition—are summarized in Table 2, organized by treatment strategy. Only one study was a double-blind randomized controlled trial (RCT) whereas the majority of evidence was derived from open-label trials or retrospective studies.
Four medications were prescribed in outpatient studies: MDZ-NS (nasal spray), DZP-NS, lorarepam (LZP) oral solution, and DZP rectal gel.
MDZ-NS was administered at a fixed 5 mg dose, regardless of age or weight, for episodes, lasting ≥ 10 min, of ≥2 seizures (focal or generalized) within 6 h. A second 5 mg dose was allowed 10 min to 6 h later [15,16,31,32,33].DZP-NS was administered at 5–20 mg, depending on age and weight. A second dose was permitted 4–24 h later. Indication was broadly defined (“seizures that might require benzodiazepine intervention”) [28].LZP oral solution was prescribed at 0.5–2 mg (65% of the cohort received 1 mg; 29% 2 mg) for two or more seizures in 24 h (73% of patients) or prolonged seizures > 5 min (21%) [34].DZP rectal gel was evaluated in a single-centre retrospective study of 50 patients (mean age 34.7 years) for SCs (>2 seizures) or prolonged seizures. The doses ranged from 10 to 20 mg, adjusted according to weight [35].
Males and females were generally equally represented (detailed in Table 2). Ages ranged from 6 to 75 years, with younger patients included in DZP studies [28,33], whereas the LZP cohort comprised only adults [34].
Over 50% of patients had drug-resistant epilepsy. The baseline seizure frequency was reported in only one study [34]. MDZ-NS trials enrolled patients with high SC frequency (mean 7.97 episodes/year) [15,16]. Etiology was often unspecified, although the 40–66% of patients had encephalopathy or were dependent in daily activities [28,33,34].
The seizure types varied across studies. Tonic–clonic seizures in MDZ-NS and DZP-NS trials ranged between 40 and 70%. LZP oral solution was used to target mainly focal seizures with impaired awareness [34]. Notably, 6% of patients used LZP to prevent seizures following auras [34]. DZP-NS was administered “at the first sign of a seizure” by 8.8% of caregivers and 48% of self-administering patients; only 24% of self-administrations targeted SCs [46]. The reasons for these types of prescriptions were not specified. Data on SC precipitating factors were not available.
Efficacy outcomes were variably defined. Seizure freedom at 24 h ranged from 62.7 in a double-blind RCT (with a statistically significant difference from placebo) [15] to 63.1% in an open-label trial [16] with MDZ-NS treatment. Seizure freedom at 24 h reached 66% with LZP oral solution, and was higher (78%) when administered sublingually [34]. Data on seizure recurrence with DZP-NS were unavailable; 12.6% of patients required a second dose within 24 h [28,42,49]. No differences were observed in the number of second doses of DZP-NS in the case of chronic use of BZDs or concomitant cannabidiol use [42,49].
The return to baseline function occurred within 1 h in ~45% of MDZ-NS patients in an open-label study [31] and in 60% of DZP-NS patients [46]. The progression to SE was rare: 0–1.2% with MDZ-NS [15,16] and 4.3% with DZP-NS in another study [28].
No data were available regarding hospitalization reduction. Two studies reported that effective SC treatment may prevent subsequent clusters by prolonging the inter-cluster interval [37,39].
Overall AEs were reported in 18.4% of DZP-NS patients [28]. For MDZ-NS, AE rates ranged from 26.4% (versus 23.1% in the placebo group) [15] to 31.7% in an open-label single-arm study [16]. The overall safety profile was comparable across medications. Acute Central Respiratory Depression (ACRD) occurred in 0.7% of MDZ-NS patients during the test phase [15]. No serious drug-related AEs were reported with DZP-NS or LZP [28,34].
The efficacy outcomes and AEs reported in the selected outpatient studies are summarized in Table 3. Heterogeneity in the outcomes—including seizure cessation, seizure recurrence at various time points, the use of a second dose, and the return to full baseline functionality—is evident.
3.3. In-Hospital Management
Nine studies (28.1%) evaluated in-hospital SC management, including five studies conducted in the ED [50,51,52,53,54] and four in EMU [30,55,56,57].
The medications assessed included intranasal midazolam (IN-MDZ, referring to the intranasal atomization of the intramuscular MDZ formulation, and MDZ-NS) [30,55,57], intravenous LZP [56,57], and intravenous non-benzodiazepine ASMs—brivaracetam, lacosamide, valproic acid, and phenobarbital [50,51,52,53,56].
3.3.1. Emergency Department (ED)
The studies’ characteristics—including the design, sample size, and SC definition—are summarized in Table 4. Only one study was an open-label RCT, whereas most of the evidence comes from retrospective or ambispective observational studies.
Within the selected time frame, all identified studies evaluated ASMs as add-on therapy after benzodiazepine failure or as first-line treatment in patients with contraindications to benzodiazepines.
Intravenous brivaracetam (IV-BRV) was administered for the treatment of ≥2 seizures occurring within 6–24 h (depending on the study), considered infrequent for the patient [50,51]. A loading dose of ≥1.82 mg/kg was used, based on previous studies investigating IV-BRV for SE, followed by the maintenance therapy of 100–200 mg/day in 74% of patients [50]. IV-BRV was used as first-line therapy in 17–41.8% of cases and as second-line therapy in 35.8–49% [50,51].Intravenous lacosamide (IV-LCM) was added to standard ASMs for the treatment of ≥2 seizures occurring within 1 h, with the complete recovery to baseline between events. This presentation was considered atypical for the individual patient. The median loading dose was 200 mg [52].Intravenous valproic acid (IV-VPA, 30 mg/kg) and intravenous phenytoin (IV-PHT; 18 mg/kg) were evaluated as first-line therapy (without prior BZD administration) in patients experiencing ≥2 seizures over 5–6 h. These events differed from the patient’s usual seizure pattern in both frequency and severity. No maintenance doses were administered [53].
Males and females were generally equally represented, except in the IV-VPA and IV-PHT groups, which included a higher proportion of male patients [53]. The mean age of patients presenting to the ED for SCs ranged from 51 to 62.3 years [50,51,52,53], with higher mean ages reported in studies evaluating IV-BRV [50,51].
A total of 42.9–76.0% of patients had pre-existing epilepsy [50,51,52], whereas in the remaining cases, the SC represented the first epileptic manifestation. The most common etiology was structural [50,51,52], followed by unknown causes. Prior seizure frequency in PWE was not reported, nor was the proportion of drug-resistant cases. However, in one IV-BRV study, the mean number of concomitant ASMs was 2.3 [51].
ASM withdrawal, treatment non-adherence, or subtherapeutic drug levels accounted for 9.5–16.2% of cases across different subgroups [50,52,53]. Other frequent provoking factors included acute systemic illness (e.g., fever) and sleep deprivation. Nevertheless, most cases were classified as unprovoked [50]. Most treated seizures were focal in the IV-BRV [50,51] and IV-LCM [52] studies. In contrast, in the IV-VPA/IV-PHT group, the majority of patients were treated for tonic–clonic seizures [53].
Direct comparisons of efficacy are not possible because the outcome definitions varied across studies. The reported outcomes are summarized in Table 5. Seizure freedom within 24 h was reported in two studies: 58% with IV-BRV [50] and 67% with IV-LCM (83% when used as first-line therapy) [52]. Following IV-BRV administration, seizure freedom was significantly higher in PWE than in patients without a prior history of epilepsy. Moreover, SCs provoked by systemic factors were associated with a lower probability of seizure freedom and a higher risk of progression to SE in PWE [50].
The efficacy of IV-BRV and IV-LCM was not influenced by the seizure type in two studies [50,51,52]. Favourable outcomes were associated with a shorter time to treatment and earlier drug administration (first or second line) for both IV-BRV [50,51] and IV-LCM [52]. Rapid IV-BRV infusion (1–5 min) was also associated with improved outcomes [51]. No significant differences were observed between higher (>200 mg) and lower (<200 mg) IV-LCM loading doses [52].
Clinical response was confirmed electrographically in all patients treated with IV-LCM [52] and in at least 58% of those treated with IV-BRV [50,51,52]. In the study evaluating IV-VPA and IV-PHT [53], EEG was performed only when non-convulsive SE was suspected. The progression from SC to SE (17% of patients) was reported only in IV-BRV studies [50], as was subsequent hospitalization (92.9% of patients), with a mean length of stay of 15 days [51].
AEs were reported in fewer than 15% of the IV-BRV-treated patients in two studies [50,51,52] and in 16% of the IV-LCM-treated patients in another study [52]. The most common AEs included somnolence/drowsiness, dizziness, nausea, vomiting, fatigue and blurred vision. No serious AEs were reported with IV-BRV or IV-LCM. The efficacy outcomes and AEs from the ED studies are summarized in Table 5. As noted above, there is considerable variability in outcome definitions across studies.
3.3.2. Epilepsy Monitoring Unit (EMU)
In the EMU setting, three of four studies evaluated benzodiazepine efficacy (MDZ-NS [55], IN-MDZ [30,57], or IV-LZP [57]), whereas one study compared the efficacy and safety of IV-BRV versus IV-LZP [56].
The studies’ characteristics, including their design, sample size, and SC definition, are summarized in Table 6. Only one study was a double-blind RCT; the remaining evidence derives from open-label or retrospective/ambispective observational studies.
As-needed therapy for increased seizure frequency, including SCs, was prescribed under the following conditions: ≥2 seizures within 6 h, ≥3 seizures within 24 h, or any generalized tonic–clonic seizure requiring treatment at the clinician’s discretion [55,56,57]. The main exclusion criteria were chronic benzodiazepine use (>3 times per week) in the MDZ-NS study [55] and recent (<28 days) initiation of BRV or use of chronic BZDs in the IV-BRV study [56].
Males and females were generally equally represented. The mean age of patients in the EMU ranged from 32.7 to 43.9 years [30,55,56,57].
When reported, most patients treated with MDZ, IV-LZP or IV-BRV were drug resistant, as expected in this population [42]. The baseline (out-of-cluster) seizure frequency was not reported. No data were available on seizure etiology. When specified, tonic–clonic seizures occurred in 60–93% of patients across the studies [30,55,56,57].
Efficacy was defined as the absence of seizure recurrence within 12 h: 20% with IV-BRV and 40% with IV-LZP in one study [56], and 42.6% with IN-MDZ in another [30]. In a double-blind RCT, seizure freedom at 6 h was achieved in 54.8% of patients treated with MDZ-NS, with no significant difference compared with placebo [55]. EEG monitoring, confirming electrographic seizure cessation, was performed in all patients [30,56,57].
AEs occurred in 42–60.9% of patients receiving MDZ-NS or IN-MDZ [55,57], 25–55.6% of those treated with IV-LZP [56,57], and in 13.0% of patients treated with IV-BRV. Nasal discomfort and throat irritation were the most common with MDZ-NS/IN-MDZ, whereas phlebitis or drug extravasation occurred in 7.4% of IV-LZP treated patients [57]. No cases of respiratory depression or other severe AEs were reported with any treatment. Progression to SE occurred in 0–4.3% of MDZ-treated patients [30,55,57] and in 0–14.8% of patients treated with IV-LZP studies [56,57], whereas no progression to SE was reported in the IV-BRV study [56]. No data were available regarding prolonged hospitalization due to SCs or increased seizure activity in the EMU.
The efficacy outcomes and AEs reported in EMU studies are summarized in Table 7. The variability in the definition of efficacy outcomes is noted.
4. Discussion
SCs represent a transient increase in seizure frequency. Currently, no universally accepted definition exists, and the literature is affected by heterogeneous criteria (summarized in the “SC definition” columns of Table 2, Table 4 and Table 6). “Clinical”/“empirical” definitions—based on the number of seizures within a specific time frame (e.g., ≥2 seizures within 24 h)—are convenient and easily applied in ED settings, where detailed knowledge of a patient’s seizure history may be lacking. However, in patients with a high baseline seizure frequency, there is a risk of overestimating the diagnosis of SC. To address this limitation, some studies have proposed a “statistical definition”, based on deviations from a patient’s baseline seizure frequency. For example, an increase by a factor of 3–4 over a 3-day period has been suggested as a valid criterion [10]. The clinical setting also critically influences the choice of antiseizure medication and the urgency of intervention. Patients presenting to the ED with recurrent seizures over the preceding hours typically require rapid treatment to terminate the cluster and reduce the risk of progression to SE. In contrast, patients experiencing predictable seizure exacerbations, such as during the menstrual cycle, may require preventive therapy over subsequent hours, with a different tolerance for side effects and acceptable seizure frequency.
Clinicians further emphasize the need to differentiate SC definitions based on patients’ characteristics and seizure types (focal vs. generalized, and with or without impaired awareness), which further limits the generalizability of a standardized approach. Additionally, the availability of medications across settings and differences in drug formulations between countries (e.g., USA vs. Europe) reduce the feasibility of developing universally applicable treatment algorithms or protocols (see Table 1).
This literature review aimed to analyze current evidence to guide medication prescription. The limitations of this study include that a formal bias assessment of the included studies was not performed. High-quality evidence—such as double-blind randomized controlled trials and head-to-head comparisons—remains scarce. Moreover, SCs and efficacy outcomes have been variably defined across different studies, in both outpatient and inpatient settings, which hampers comparison among different medications.
For outpatients, a recent expert consensus has recommended the use of an individualized SC definition for management [17]. Clinicians should develop ASAPs (Acute Seizure Action Plans) and prescribe rescue treatment following ACT or REST purpose (Table 8). Under this framework, the consensus recommends offering ACT prophylactically to all patients with a history of SCs to prevent further episodes, while REST should be prescribed to patients with a history of myoclonic or absence seizures known to progress to tonic–clonic seizures, those with prolonged seizures or SE, or patients with focal seizures without impaired awareness that evolve into seizures with impaired awareness or bilateral tonic–clonic seizures [17].
We concur that for outpatients an ASAP should be developed [18] collaboratively with the patient and caregiver for all individuals at risk of SCs or prolonged seizures. This plan should be tailored to the patient’s characteristics, including their independence in activities of daily living, occupational status, seizure type, and cluster duration.
Our literature review suggests that DZP-NS, MDZ-NS and LZP oral solution may exhibit a similar efficacy and safety profile, despite several limitations:
- Efficacy was defined using different criteria across studies;
- Studies’ designs varies considerably;
- No head-to-head comparisons are available.
Specifically, DZP-NS has not been evaluated in randomized controlled trials; available data derive from an open-label safety study and its post hoc analysis. MDZ-NS was assessed against placebo and, subsequently, in an open-label extension trial. The LZP data originates from a single-centre retrospective study. The discrepancy in second dose use (31.3–37.3% at 6 h with MDZ-NS vs. 12.6% with DZP-NS) may reflect the broader use of DZP-NS beyond SCs. However, the lack of availability of MDZ-NS and DZP-NS in some countries (see Table 1) limits their clinical use. Consequently, the off-label use of oral BZDs (i.e., clobazam and clonazepam, as well as the above-mentioned lorazepam) still remains common when oral therapy is feasible, despite limited supporting evidence.
Interestingly, cluster prevention may exert a long-term benefits by increasing the interval to the next cluster, suggesting that, at least in some patients, a self-perpetuating mechanism underlies SC recurrence [37,39]. The safety profile showed overall mild AEs.
Regarding SC management in EDs, the literature indicates substantial heterogeneity. In a significant proportion of cases, SCs represent the first epileptic manifestation [50,51,52]. Currently, no specific guidelines exist for managing this neurological emergency. Based on our review, there is a general consensus supporting the application of the same first-line treatment paradigm used for SE: initial IV benzodiazepine administration, followed—if seizures recur—by the IV loading of ASMs such as brivaracetam [50,51] or lacosamide [52]. Existing studies on intravenous ASMs raise the question of whether tolerability and the route of administration outweigh therapeutic indication. This conceptual limitation has also been noted in prior observational studies of SE and has been hypothesized as a factor contributing to worse prognostic outcomes [58]. While some findings suggest a potential advantage of brivaracetam over benzodiazepines in terms of reducing the risk of progression to SE, these observations require further investigation, particularly in patient populations with diverse seizure aetiologies. Prospective studies comparing the efficacy of rapid-acting benzodiazepines—potentially including intranasal formulations—versus ASMs in SC management are warranted.
The EMU setting presents distinct challenges. The rapid tapering of ASMs to facilitate seizure recording while minimizing hospitalization duration increases the risk of cluster seizures. Shih et al. (2025) surveyed over 20 experts from a dedicated Epilepsy Education Council and reported significant variability in cluster definitions, ranging from two seizures in 1 h to three seizures within 24 h [29]. This variability reflects both baseline patient characteristics and seizure semiology, with tonic–clonic seizures occurring more frequently during rapid medication tapering. According to the International League Against Epilepsy’s clinical practice guidelines, a fast taper (30–50%) or slow taper (15–30%) is considered safe for patients without a history of SE or frequent daily seizures during EMU hospitalization [59]. Rescue medications are typically predetermined by the supervising neurologist. Most experts reported preferring IV-LZP if available; otherwise, intranasal MDZ is used [29]. These choices largely depend on drug availability in different countries. In Europe, for example, buccal midazolam is commonly used both at home and in the hospital. Often, reloading the patient’s previous therapy—sometimes intravenously—may suffice to terminate the cluster in this setting.
The treatment objectives and strategies identified in this review, across different clinical settings, are summarized in Table 8.
5. Conclusions
Seizure clusters (SCs) are defined as an abnormal increase in seizure frequency relative to an individual patient’s baseline. However, the lack of standardized temporal criteria contributes to substantial heterogeneity in clinical practice. Furthermore, the existing literature employs heterogeneous definitions, which complicates inter-study comparisons. Management strategies vary according to the clinical setting, drug properties, patients’ characteristics and clinicians’ experience.
A more streamlined, setting-oriented approach may improve care. In outpatient settings, insufficient patient and caregiver education and the underuse of rescue therapies remain major limitations. Individualized action plans should be prioritized to enable timely intervention, empowering patients or caregivers to terminate prolonged seizures (REST) or ongoing seizure clusters (ACT). Currently available medications include diazepam nasal spray, midazolam nasal spray, and, although lacking a specific indication for SCs, lorazepam oral solution. Direct comparisons of efficacy and safety are limited by variable outcome definitions. In the Emergency Department, SCs can be managed with prompt benzodiazepine administration and the correction of reversible precipitants, consistent with early SE protocols. During long-term video EEG monitoring, treatment decisions must balance diagnostic objectives with patient safety. Early, context-specific intervention and the routine use of individualized rescue protocols are essential to reduce complications and the risk of progression to status epilepticus.
The unification of SC and efficacy definitions is needed to improve comparability in future studies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Penovich P.E. Buelow J. Steinberg K. Sirven J. Wheless J. Burden of Seizure Clusters on Patients With Epilepsy and Caregivers: Survey of Patient, Caregiver, and Clinician Perspectives Neurologist 20172220721410.1097/NRL.000000000000014029095321 · doi ↗ · pubmed ↗
- 2Haut S.R. Shinnar S. MoshéS.L. O’Dell C. Legatt A.D. The association between seizure clustering and convulsive status epilepticus in patients with intractable complex partial seizures Epilepsia 1999401832183410.1111/j.1528-1157.1999.tb 01607.x 10612353 · doi ↗ · pubmed ↗
- 3Haut S.R. Shinnar S. MoshéS.L. Seizure clustering: Risks and outcomes Epilepsia 20054614614910.1111/j.0013-9580.2005.29004.x 15660781 · doi ↗ · pubmed ↗
- 4Bauman K. Devinsky O. Seizure Clusters: Morbidity and Mortality Front. Neurol.20211263604510.3389/fneur.2021.63604533664705 PMC 7920959 · doi ↗ · pubmed ↗
- 5Ochoa-Urrea M. Lacuey N. Vilella L. Zhu L. Jamal-Omidi S. Rani M.R.S. Hampson J.P. Dayyani M. Hampson J. Hupp N.J. Seizure Clusters, Seizure Severity Markers, and SUDEP Risk Front. Neurol.20211264391610.3389/fneur.2021.64391633643216 PMC 7907515 · doi ↗ · pubmed ↗
- 6Morris G.L. Eads P. Tryfon M. Ems D. Seizure clusters, treatment patterns, and healthcare resource utilization in patients with epilepsy: A Wisconsin-based claims analysis Epilepsy Behav.202415710986710.1016/j.yebeh.2024.10986738824751 · doi ↗ · pubmed ↗
- 7Detyniecki K. O’Bryan J. Choezom T. Rak G. Ma C. Zhang S. Bonito J. Hirsch L.J. Prevalence and predictors of seizure clusters: A prospective observational study of adult patients with epilepsy Epilepsy Behav.20188834935610.1016/j.yebeh.2018.09.03530344026 · doi ↗ · pubmed ↗
- 8Zhong R. Chen Q. Zhang X. Lin W. The Occurrence of Seizure Clusters in Patients with Epilepsy Is Partly Determined by Epilepsy Severity: A Single-Center Retrospective Observational Study Front. Neurol.20211279408610.3389/fneur.2021.79408634956069 PMC 8695898 · doi ↗ · pubmed ↗