Post-COVID-19 Outcomes of Patients with Autosomal Dominant Polycystic Kidney Disease: A Multicenter Controlled Study
Serhat Karadag, Savas Ozturk, Nimet Aktas, Sinan Trabulus, Zeki Aydin, Hamad Dheir, Tolga Kuzu, Fatih Yilmaz, Yavuz Ayar, Irem Pembegul, Taner Basturk, Ruya Mutluay, Egemen Cebeci, Metin Ergul, Esra Akcali, Tuba Elif Ozler, Alper Azak, Mahmud Islam, Mustafa Arici, Kenan Ates

TL;DR
This study found that ADPKD patients who survived COVID-19 had similar short-term outcomes as those who never had the virus.
Contribution
The study provides new evidence on the short-term post-COVID-19 outcomes specifically in ADPKD patients.
Findings
No deaths occurred in either the COVID-19 or control group during the first and third months of follow-up.
Urinary tract infections were more common in the non-COVID-19 group in the third month.
No significant differences were found in respiratory symptoms or kidney replacement therapy initiation between the groups.
Abstract
Background: Patients with chronic kidney disease (CKD), including autosomal dominant polycystic kidney disease (ADPKD), have been reported to be at higher risk for adverse outcomes during the COVID-19 pandemic. We aimed to obtain the characteristics and outcome data obtained in the follow-up of patients with ADPKD who survived COVID-19 and to compare these data with a control group with ADPKD who were COVID-19 naive. Methods: In this national, multicenter observational study, adult ADPKD patients who survived COVID-19 were included, and ADPKD patients without a history of COVID-19 from the same outpatient clinics were selected as a control group. Baseline characteristics and post-COVID-19 first- and third-month data were recorded. Results: In this study, a total of 72 ADPKD patients from 16 centers were included in the study (COVID-19 group, n: 40, non-COVID-19 control group, n: 32).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
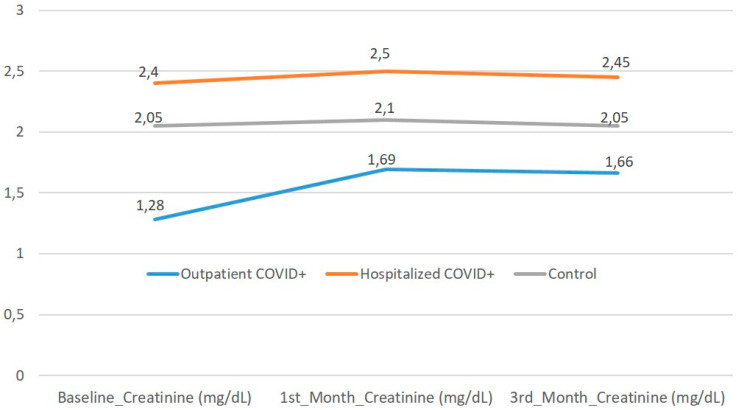 Figure 1
Figure 1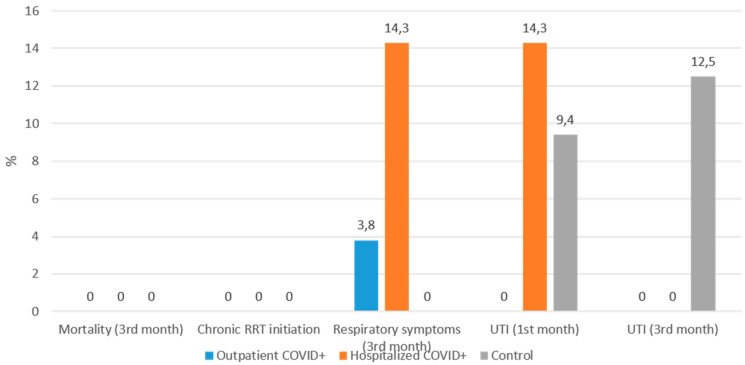 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic and Kidney Cyst Diseases · COVID-19 Clinical Research Studies · Renal Diseases and Glomerulopathies
1. Introduction
Autosomal dominant polycystic kidney disease (ADPKD) is the most common genetic kidney disease, affecting approximately 1 in 1000 live births worldwide [1]. ADPKD forms cysts in the kidneys, leading to a range of complications, including hypertension, chronic kidney disease (CKD), and end-stage renal disease [2]. During the coronavirus disease 2019 (COVID-19) pandemic, patients with chronic diseases such as CKD were reported to have more adverse outcomes, including hospitalization, need for intensive care support, and death [3,4,5,6]. Few data are available in the literature on the importance of having ADPKD during the COVID-19 pandemic. Although some studies indicate that having ADPKD is an elevated risk of COVID-19 complications, there are also studies showing that ADPKD patients with COVID-19 do not result in different outcomes than non-COVID-19 ADPKD patients [7,8]. These studies include data during the active COVID-19 period. There are no published data that we can find on the outcome of ADPKD patients who have had COVID-19.
The pathogenesis of ADPKD is not directly related to immune disorders; thus, it may not be expected to cause more severe consequences in the post-COVID-19 period. However, outcomes may be worse in patients with advanced renal impairment. While prior studies have primarily examined the acute phase, the post-COVID recovery period may reveal persistent renal or systemic effects that remain under-characterized in ADPKD. Therefore, we aimed to evaluate the clinical characteristics and short-term outcomes of ADPKD patients who survived COVID-19 and to compare these findings with a COVID-19-naïve ADPKD control group.
2. Materials and Methods
This retrospective cohort study followed the Strengthening Reporting of Observational Studies in Epidemiology (STROBE) statement [9]. Ethical approval of the study was obtained from the Health Sciences University, Haseki Training and Research Hospital Ethics Committee (Date: 28 April 2021, protocol number: 12-2021).
2.1. Population and Setting
This study was designed as a retrospective controlled cohort study. The index date for the COVID-19 group was defined as the date of reverse transcriptase-polymerase chain reaction (RT-PCR) confirmation. For the control group, the index date was defined as the outpatient visit occurring in the same calendar month as the corresponding COVID-19 case to ensure temporal alignment of follow-up. COVID-19 cases were identified through the Turkish Society of Nephrology web-based registry, which prospectively collects national data on COVID-19 from voluntary nephrology centers. Patients included in the registry were known ADPKD patients followed in participating nephrology clinics who developed RT-PCR-confirmed SARS-CoV-2 infection and were subsequently reported by the treating nephrologist. COVID-19 infection was confirmed by a positive SARS-CoV-2 nasopharyngeal RT-PCR test. Patients diagnosed only by clinical or radiological findings without a confirmatory RT-PCR test were excluded from the COVID-19 group. Both symptomatic and asymptomatic RT-PCR-positive patients were eligible for inclusion. Data were collected from April 2021 to September 2021. A control group consisting of ADPKD patients without COVID-19 was formed from the same centers. COVID-19-free status was determined based on the absence of documented RT-PCR positivity and no recorded clinical diagnosis of COVID-19 in hospital electronic medical records at the time of selection. The first COVID-19-free ADPKD patient who came to the outpatient clinic of the participating centers after an ADPKD patient with COVID-19 was selected as the Control group, regardless of serum creatinine and glomerular filtration rate (GFR) values. To minimize selection bias, control patients were chosen from the same outpatient clinics and during the same time frame as the COVID-19 cases, ensuring comparable access to healthcare and follow-up frequency. Although individual matching was not performed, the two groups were similar in terms of age, sex, and major comorbidities, as shown in Table 1. All patients in both groups were followed with the same post-evaluation schedule (baseline, first month, and third month visits), using identical laboratory and clinical data collection procedures. The diagnosis, disease severity, and treatment of patients who had COVID-19 were managed with the guidelines recommended by the Ministry of Health [10].
The study excluded patients with end-stage renal disease, kidney transplant recipients, individuals under 18 years of age, and those with known kidney diseases other than ADPKD—such as diabetic nephropathy, hypertensive nephrosclerosis, glomerulonephritis, or NSAID-induced nephropathy. Additionally, within the COVID-19 group, patients without a confirmed positive nasopharyngeal SARS-CoV-2 reverse transcriptase-polymerase chain reaction (RT-PCR) test were also excluded. We also excluded patients with missing third-month outcome data after COVID-19. Potential control patients with documented COVID-19 infection during the study period or missing follow-up data were also excluded from analysis.
COVID-19 vaccination status was not consistently available in the registry database. During the study period (April–September 2021), vaccination in Turkey had begun with priority groups, including healthcare workers and older adults, but was not yet widespread across the general population; therefore, vaccination data could not be analyzed.
2.2. Measurements and Definitions
We gathered baseline characteristics, comorbidities and medications, blood pressure, height, weight, basic laboratory test results including glucose, urea, creatinine, albumin, C reactive protein (CRP), hemoglobin, proteinuria, urinalysis, and hemogram parameters from hospital records at the last outpatient clinic visit of the relevant center before the development of COVID-19. The same laboratory tests were recorded after the first and third months. All laboratory measurements were performed in the clinical laboratories of participating centers, each accredited by the Turkish Ministry of Health. Laboratory methods and reference ranges were consistent across centers. COVID-19-related outcomes were recorded from electronic hospital systems and verified by the treating nephrologist at each center to ensure data accuracy. Proteinuria was recorded both qualitatively, as measured by dipstick, and quantitatively by deriving from spot urine protein creatinine ratio or measured from 24-h collected urine protein amount. Hematuria was defined as the presence of 5 or more erythrocytes per high-power field. Leukocyturia was defined as 5 or more leukocytes per high-power field. In addition, information about the active period of COVID-19 [symptoms, chest computed tomography (CT), treatments for COVID-19, clinical severity of the disease according to the Ministry of Health guideline [10], inpatient or outpatient treatment, need for ICU, dialysis, and the duration of the hospitalization] was obtained. The data of patients included in the non-COVID group were obtained in the same month (including baseline visits) as the equivalent patient in the COVID-19 group.
For subgroup analysis, COVID-19-positive ADPKD patients were further divided into two categories according to their management during the acute infection: hospitalized and outpatient. A third group consisted of ADPKD patients without a history of COVID-19 (controls). All three subgroups were followed with the same post-COVID evaluation protocol, and laboratory parameters were obtained at baseline, first, and third months. These subgroup analyses according to hospitalization status were exploratory and conducted post hoc, as they were not prespecified in the original study design.
2.3. Follow-Up and Outcome
Primary endpoints were all-cause mortality, initiation of chronic kidney replacement therapy (KRT), and persistent respiratory symptoms at 1 and 3 months. Secondary endpoints included hospitalization during follow-up, urinary tract infection (UTI), lower respiratory tract infection, thromboembolic events, and laboratory parameters. We collected clinical data, including mortality, initiation of chronic Kidney replacement therapy (KRT), ongoing respiratory symptoms (cough and/or shortness of breath), hospitalization, need for home oxygen therapy, lower respiratory tract infection, and UTI development in our patient group at the 1st and 3rd months post-COVID-19. In addition, patients’ weight, blood pressure, creatinine, albumin, CRP, hemoglobin, proteinuria (qualitative and quantitative), hematuria and leukocyturia values in the urine sediment were obtained at 1 and 3 months. The same data were also obtained for the non-COVID-19 control group. In this control group, the data of each patient were obtained from the data in the same month as the patient with COVID-19 control. Ongoing respiratory symptoms were defined as the persistence of cough and/or dyspnea beyond 4 weeks after acute infection. UTI was recorded only in the presence of both compatible symptoms and either positive urine culture or physician-documented antibiotic prescription. All-cause mortality, new initiation of chronic KRT, and rehospitalization were recorded within the first and third months.
2.4. Statistical Analyses
In descriptive statistics, we presented numbers and percentages for categorical variables, and median and interquartile ranges (25–75%) for numerical variables. The normality of the variables was analyzed using Kolmogorov–Smirnov tests. The chi-square test was used to compare categorical variables in two or multiple groups. We used the independent t-test or the Mann–Whitney U test as appropriate to compare numerical variables. In multi-group comparisons of numerical variables, the analysis of variance (ANOVA) test was used for normally distributed numerical variables, and the Kruskal–Wallis test was used for numerical variables that were not normally distributed. The significance level was accepted as p < 0.05. Given the limited sample size, no multivariable adjustments were applied. Therefore, the analyses should be interpreted as exploratory and hypothesis-generating. Effect sizes (median differences and proportions) were examined to identify clinically meaningful trends even when statistical significance was not achieved. IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis.
3. Results
3.1. Demographic and Baseline Characteristics
A total of 74 patients’ data were obtained from 16 centers for the study. Two patients were excluded because third-month outcome data were missing. In the final, 72 patients (40 ADPKD patients who survived COVID-19, and 32 ADPKD patients without a COVID-19 control group) were included in the study. The main characteristics of both groups were almost similar (Table 1). Age, gender, ADPKD duration, extrarenal organ involvement, comorbidities, medications, and baseline laboratory tests were not different between the groups, except CRP [median: 6 (IQR: 2–36) mg/L) vs. 3 (IQR: 3–6) mg/L, p < 0.05] and hematuria [n (%): 14 (41.2) vs. 6 (18.8), p < 0.05], which were significantly higher in the COVID-19 group than COVID-19 free group.
3.2. The Acute Phase of COVID-19
The clinical severity of patients who had COVID-19 at the time of first admission to the hospital was as follows: asymptomatic disease 3 (7.5%), mild disease 27 (67.5%), moderate-severe disease 10 (25.0%). None of the patients had severe critical illness. Fourteen (33.3%) of them were treated as inpatients. The length of stay at the hospital was 10 (8–13) days. Acute kidney injury developed in 9 (64.2%) of the hospitalized patients (7 patients KDIGO stage 1, 2 patients stage 3). Nine (64.2%) patients were given glucocorticoids for COVID-19 in addition to symptomatic treatments. No patient was admitted to the intensive care unit.
3.3. Comparison of First and Third-Month Laboratory Values and Outcomes
There were no significant differences in laboratory parameters between the COVID-19 and non-COVID-19 groups at the first and third months (Table 2). During the first and third months after COVID-19, none of the patients died in either group. Only UTI was significantly higher in the non-COVID-19 group than in the COVID-19 group in the third month (0% vs. 12.5%, p = 0.021). All other follow-up outcomes, including initiation of chronic KRT, were not different between the groups in the first and third months.
3.4. Comparison of First and Third-Month Laboratory Values and Outcomes According to Hospitalization of COVID-19 Group
When the COVID-19 group was divided into two groups according to outpatient (26 patients) or inpatient (14 patients) treatment and compared with the COVID-19-free group (Supplementary Table S1); age and presence of recurrent urinary infection were higher in the inpatient group. All inpatient-treated patients had pneumonia on chest CT, and had a higher rate of dyspnea, cough, and moderate-severe illness than the outpatient-treated group at presentation. Baseline creatinine, CRP levels, rate of hematuria, and proteinuria were significantly higher in the inpatient group than in the other groups. When the outcomes of these groups were compared in the first and third months, there was no significant difference between these groups (Supplementary Table S2).
3.5. Additional Subgroup Analyses
Supplementary Table S1 summarizes baseline demographic and laboratory findings of outpatients, hospitalized COVID-19-positive ADPKD patients, and non-COVID controls. Hospitalized patients had significantly higher creatinine and CRP levels than both outpatients and controls (p < 0.05). Other parameters, including blood pressure, albumin, and proteinuria, were comparable among groups. Supplementary Table S2 shows short-term outcomes across the three subgroups. No mortality or chronic KRT initiation was observed during follow-up. UTI at the third month was more frequent in the control group (p = 0.02), while other outcomes showed no significant differences. Figure 1 demonstrates that serum creatinine levels remained stable from baseline to the third month among all three subgroups. Although hospitalized COVID-19-positive patients had slightly higher baseline creatinine levels, no progressive deterioration was observed during follow-up. The distribution of post-COVID events—including respiratory symptoms, UTIs, and need for hospitalization—was similar across all subgroups, with no mortality or chronic KRT observed in any group (Figure 2). A higher frequency of UTIs was noted in the control group at the third month (12.5%), which reached statistical significance (p = 0.02). These findings are consistent with the overall observation that ADPKD patients recovering from COVID-19 do not experience worsened short-term outcomes compared with COVID-naïve counterparts.
4. Discussion
The results of this study provided important insights into the outcomes of ADPKD patients who survived COVID-19 in the post-acute period. Our study found that mortality, initiation of chronic KRT, and respiratory symptoms were not significantly different in ADPKD patients COVID-19 survivors compared to non-COVID-19 ADPKD patients in the first three months of the post-COVID-19 period. Importantly, both groups were comparable in demographic and clinical characteristics at baseline, and follow-up evaluations were performed under identical conditions, which supports the internal validity of our findings. Moreover, subgroup analyses revealed that hospitalized COVID-19-positive ADPKD patients had higher baseline creatinine and CRP levels compared to outpatients and controls, reflecting greater inflammation and renal burden during acute disease. Nevertheless, post-COVID outcomes were similar among all groups, suggesting preserved renal function and a favorable short-term prognosis in ADPKD patients who recover from COVID-19. Although data specifically examining COVID-19 outcomes in ADPKD are limited, existing reviews suggest that while CKD disease in general increases the risk of adverse outcomes, patients with ADPKD do not appear to have substantially higher COVID-19-related mortality compared with CKD cohorts, supporting our findings of preserved short-term outcomes post-infection [8]. Given the reduced sample size within subgroups, these findings should be interpreted cautiously. The absence of significant differences during follow-up does not exclude potential clinically relevant effects, and the subgroup analyses should be considered exploratory and hypothesis-generating.
Recent longitudinal data by Lai et al. have provided additional insights into the long-term renal impact of COVID-19 among patients with ADPKD [11]. In that multicenter retrospective cohort of 103 patients, ADPKD individuals exhibited a more pronounced decline in renal function—reflected by increased serum creatinine and decreased eGFR—one year after COVID-19 infection compared to patients with CKD alone, particularly among those with baseline eGFR below 60 mL/min/1.73 m^2^. This observation suggests that while short-term outcomes appear similar between ADPKD and non-ADPKD CKD patients, long-term follow-up may reveal subtle but progressive kidney function deterioration in ADPKD following SARS-CoV-2 infection. Our findings, which demonstrate no significant renal worsening within the first three months, are therefore complementary to these long-term data and highlight the need for extended follow-up in this population.
While some numerical differences were observed in baseline characteristics and clinical outcomes, none reached statistical significance. This may be attributed to the limited sample size, which could have reduced the statistical power to detect modest but clinically meaningful differences.
Nevertheless, the overall absence of adverse post-COVID outcomes in the ADPKD group is consistent with previous reports suggesting that ADPKD does not inherently increase the risk of COVID-19-related complications. Our findings, therefore, support and extend the existing literature by providing new data from the post-acute recovery period. Cui et al. showed that in patients with ADPKD who were positive for COVID-19, the rates of hospitalization, ICU admission, ventilator requirement, and death were comparable with those of patients with other cystic kidney disease and cystic liver-only disease in a study including 61 veteran patients [7]. In a large cohort of patients hospitalized for COVID-19 previously published by our group, none of the 19 patients with ADPKD (4 kidney transplant patients, 2 predialysis CKD patients and 13 hemodialysis patients) died. However, these studies evaluated the outcomes during the active COVID-19 period, whereas our study evaluated the post-acute period outcomes [6]. A narrative review by Kutky [8] et al. found no evidence that patients with ADPKD are at higher risk for SARS-CoV-2 infection. Also, according to this study, people with renal dysfunction among those who develop COVID-19 have an increased risk of hospitalization, intensive care unit admission, and death, but ADPKD does not seem to specifically change the risk. However, none of these studies specifically evaluate the outcomes of ADPKD patients in the post-COVID-19 period. Consistent with broader COVID-19 literature, elevated CRP has been linked to adverse outcomes and organ dysfunction in infected patients. Smilowitz et al. demonstrated that higher CRP levels correlate with acute kidney injury, critical illness, and mortality among hospitalized COVID-19 patients, supporting the role of systemic inflammation in disease progression [12]. Furthermore, meta-analytic data indicate that higher CRP concentrations are significantly associated with greater disease severity and lower survival rates in COVID-19 [13]. These findings align with our observation that hospitalized ADPKD patients had higher CRP levels, though this did not translate into worse short-term renal outcomes in our cohort.
Our study also found that UTI was significantly higher in the non-COVID-19 group than in the COVID-19 group in the third month. No significant difference was observed in the first month. Although antibiotic exposure during acute COVID-19 could theoretically influence subsequent UTI incidence, antibiotic type and duration were not systematically recorded; therefore, this explanation remains speculative. Alternative explanations include differences in healthcare utilization patterns during the pandemic, variation in diagnostic intensity, or the possibility of a chance finding given the small number of events. Baseline prevalence of recurrent urinary infection and sex distribution were similar between groups; however, due to the limited sample size, these results should be interpreted cautiously and considered hypothesis-generating. Further studies are needed to confirm this finding and to evaluate the long-term effects of COVID-19 on UTIs in ADPKD patients. The lack of significant differences in laboratory data and the absence of statistically significant differences in the incidence of hematuria and leukocyturia ratios between the groups suggest that COVID-19 did not exacerbate ADPKD’s underlying pathophysiology.
This study has several limitations. First, the relatively small sample size and absence of major clinical events such as mortality or initiation of chronic kidney replacement therapy limit statistical power and increase the possibility of type II error. Therefore, modest but clinically meaningful differences between groups may not have been detected, and the findings should be interpreted as exploratory. Second, the follow-up period was limited to three months, which restricts the assessment of long-term renal progression in ADPKD. Although no significant short-term deterioration was observed, these results do not exclude the possibility of medium- or long-term renal consequences following SARS-CoV-2 infection, as suggested by recent longitudinal studies. Third, renal outcomes were primarily assessed using serum creatinine and proteinuria. Because ADPKD is a structural kidney disease, progression is more accurately reflected by longitudinal eGFR trajectories and imaging parameters such as total kidney volume (TKV), which were not systematically available in our dataset. Subtle structural progression or early decline in kidney function may therefore not have been fully captured. Fourth, despite temporal alignment and center-based control selection, residual selection bias cannot be entirely excluded. Differences in healthcare-seeking behavior during the pandemic and the possibility of unrecognized asymptomatic SARS-CoV-2 infection among controls may have influenced group comparability. Finally, vaccination status and prior SARS-CoV-2 infection history were not systematically recorded. During the study period (April–September 2021), COVID-19 vaccination in Turkey had primarily been administered to healthcare workers and high-risk groups and was not yet widespread in the general population. In addition, circulating SARS-CoV-2 variants evolved over time. These factors may limit the generalizability of our findings to later phases of the pandemic, characterized by higher vaccination coverage and different variant distributions. In conclusion, our findings suggest that ADPKD patients who survive COVID-19 do not appear to experience worse short-term (up to three months) post-acute outcomes compared with COVID-19-naïve ADPKD patients. Nevertheless, longer-term studies with larger cohorts are warranted to fully assess the long-term implications of COVID-19 in this vulnerable patient group.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Davies F. Coles G.A. Harper P.S. Williams A.J. Evans C. Cochlin D. Polycystic kidney disease re-evaluated: A population-based study Q. J. Med.1991794774851946928 · pubmed ↗
- 2Gabow P.A. Autosomal Dominant Polycystic Kidney Disease N. Engl. J. Med.199332933234210.1056/NEJM 1993072932905088321262 · doi ↗ · pubmed ↗
- 3Wu Z. Mc Googan J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Center for Disease Control and Prevention JAMA 20203231239124210.1001/jama.2020.264832091533 · doi ↗ · pubmed ↗
- 4Wang L. He W. Yu X. Hu D. Bao M. Liu H. Zhou J. Jiang H. Coronavirus disease 2019 in elderly patients: Characteristics and prognostic factors based on 4-week follow-up J. Infect.20208063964510.1016/j.jinf.2020.03.01932240670 PMC 7118526 · doi ↗ · pubmed ↗
- 5Guo W. Li M. Dong Y. Zhou H. Zhang Z. Tian C. Qin R. Wang H. Shen Y. Du K. Diabetes is a risk factor for the progression and prognosis of COVID-19Diabetes/Metab. Res. Rev.202036 e 331910.1002/dmrr.331932233013 PMC 7228407 · doi ↗ · pubmed ↗
- 6Ozturk S. Turgutalp K. Arici M. Odabas A.R. Altiparmak M.R. Aydin Z. Cebeci E. Basturk T. Soypacaci Z. Sahin G. Mortality analysis of COVID-19 infection in chronic kidney disease, haemodialysis and renal transplant patients compared with patients without kidney disease: A nationwide analysis from Turkey Nephrol. Dial. Transplant.2020352083209510.1093/ndt/gfaa 27133275763 PMC 7716804 · doi ↗ · pubmed ↗
- 7Cui X. Gallini J.W. Jasien C.L. Mrug M. Autosomal Dominant Polycystic Kidney Disease Does Not Significantly Alter Major COVID-19 Outcomes among Veterans Kidney 3602021298398810.34067/KID.000728202035373094 PMC 8791380 · doi ↗ · pubmed ↗
- 8Kutky M. Cross E. Treleaven D.J. Alam A. Lanktree M.B. The Impact of COVID-19 on Patients with ADPKD Can. J. Kidney Health Dis.202182054358121105647910.1177/2054358121105647934777845 PMC 8586165 · doi ↗ · pubmed ↗