Dye Localization Extended Segmentectomy vs. Lobectomy for Deep Intersegmental Early-Stage Lung Cancer
Wen-Yao Lee, Ting-Fang Kuo, Hsiao-Hung Lu, Yu-Sen Huang, Min-Shu Hsieh, Hsao-Hsun Hsu, Jin-Shing Chen

TL;DR
This study compares extended segmentectomy with lobectomy for early-stage lung cancer, finding similar survival but better short-term outcomes with segmentectomy.
Contribution
Demonstrates that dye-guided extended segmentectomy offers comparable cancer control with better perioperative outcomes than lobectomy for deep intersegmental lung tumors.
Findings
Extended segmentectomy had shorter operation time, less blood loss, and shorter hospital stays compared to lobectomy.
Patients who underwent segmentectomy had smaller lung volume reductions at 6 months.
Comparable 5-year survival rates were observed despite fewer lymph nodes harvested in segmentectomy cases.
Abstract
Background: Computed tomography-guided dye localization facilitates extended segmentectomy with reliable oncologic margins for deep intersegmental early-stage lung cancer. This study evaluated perioperative and long-term outcomes in comparison with those of lobectomy. Methods: We retrospectively reviewed patients with early-stage lung adenocarcinoma ≤ 2 cm who underwent computed tomography-guided dye localization extended segmentectomy between 2013 and 2019 and compared them with those who underwent lobectomy between 2011 and 2016. After 1:1 propensity score matching based on demographic and clinical variables, 30 matched pairs were included in the analysis. Results: Compared with lobectomy, extended segmentectomy with computed tomography-guided dye localization was associated with shorter operative time (102 ± 34 vs. 181 ± 42 min, p < 0.001), less blood loss (0 [0–0] vs. 0 [0–62.5] mL,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
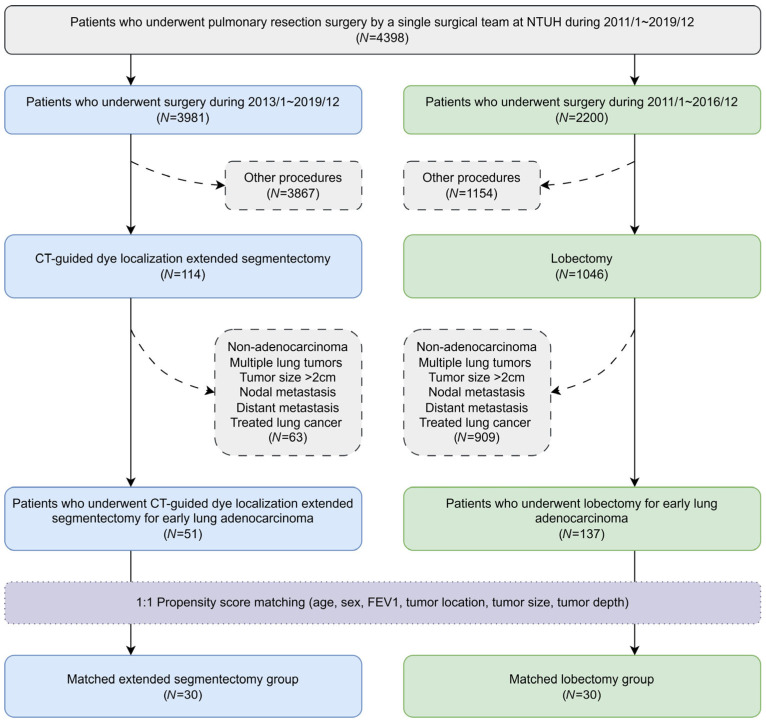 Figure 1
Figure 1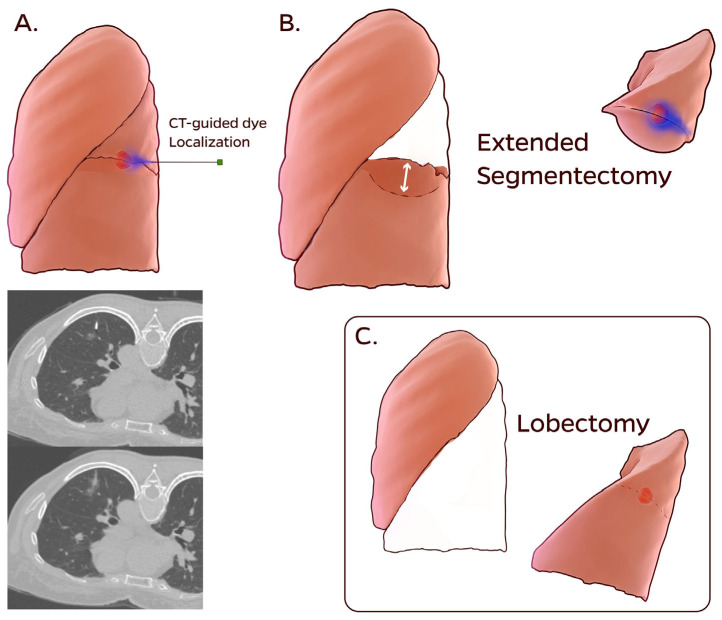 Figure 2
Figure 2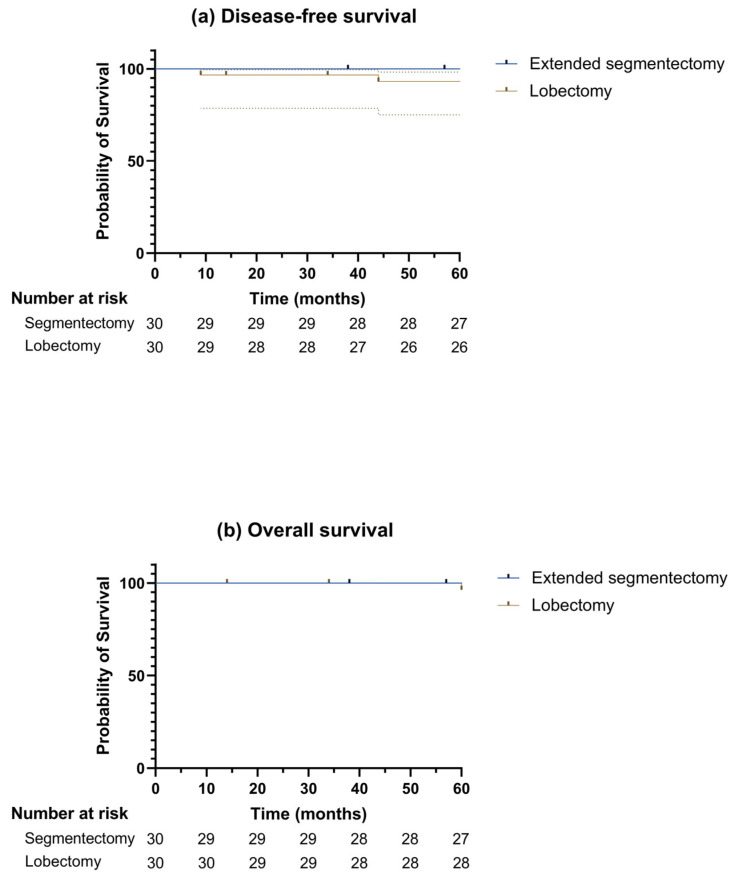 Figure 3
Figure 3- —National Taiwan University Hospital, Taipei, Taiwan
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Diagnosis and Treatment · Radiomics and Machine Learning in Medical Imaging · Lymphadenopathy Diagnosis and Analysis
1. Introduction
The incidence of pulmonary nodules has increased with the widespread use of low-dose computed tomography (CT), leading to earlier lung cancer diagnosis [1]. Recent randomized controlled trials have demonstrated that sublobar resection offers oncologic outcomes equivalent to those of lobectomy for early-stage lung cancer, as long as adequate resection margins can be obtained [2,3,4,5]. For lesions located near the intersegmental plane, extended segmentectomy, in which an additional margin from the adjacent segment is obtained using a non-anatomical resection, can be considered [6,7,8,9,10,11]. However, segmentectomy is technically more demanding than lobectomy, and determining the optimal resection line for small, nonpalpable lesions located deep within the pulmonary parenchyma remains challenging.
We developed a CT-guided patent blue vital (PBV) dye localization system for pulmonary nodules and demonstrated its feasibility, safety, and accuracy [12,13,14]. The technique was initially used in wedge resections and then applied to determine the resection line for extended segmentectomy, showing satisfactory results [10]. Nevertheless, the overall surgical outcomes remain unclear. This study aimed to compare the perioperative and long-term outcomes of CT-guided dye localization extended segmentectomy and lobectomy for early-stage lung adenocarcinoma.
2. Materials and Methods
2.1. Ethical Statement
This study was approved by the Research Ethics Committee of the National Taiwan University Hospital, Taipei, Taiwan (202502124RINE, 7 March 2025) and was conducted in accordance with the ethical principles of medical research involving human subjects outlined in the Declaration of Helsinki (2024), as amended by the World Medical Association. The requirement for informed consent was waived due to the retrospective nature of this study.
2.2. Study Population
The flowchart of the patient inclusion process is shown in Figure 1. Patients who underwent pulmonary resection surgery by a single surgical team at the National Taiwan University Hospital between 1 January 2011 and 31 December 2019 were retrospectively reviewed. For stage IA lung cancer, segmentectomy was indicated for tumors ≤ 2 cm, as well as for tumors > 2 cm in patients with impaired cardiopulmonary function who were not considered suitable for lobectomy. Since early 2013, extended segmentectomy under CT-guided dye localization has been adopted for deep or intersegmental lesions in which adequate margins could not be confidently achieved using conventional segmentectomy. After excluding patients with non-adenocarcinoma, multiple lung tumors, tumor size > 2 cm, nodal metastasis, distant metastasis, or a history of treated lung cancer, 51 consecutive patients with early-stage lung adenocarcinoma who underwent CT-guided dye localization extended segmentectomy between 1 January 2013 and 31 December 2019 were included in the extended segmentectomy group. Similarly, another 137 patients with early-stage lung adenocarcinoma who underwent lobectomy between 1 January 2011 and 31 December 2016 were included in the lobectomy group.
2.3. Primary and Secondary Outcomes
The primary outcome was postoperative hospital stay. Secondary outcomes included perioperative outcomes (operative time, blood loss, chest tube duration, and resection margin) and long-term outcomes (lung volume reduction at 6 months, disease-free survival, and overall survival rates).
2.4. Surgical Techniques
As shown in Figure 2 and Supplementary Video S1, the CT-guided dye localization extended segmentectomy technique has been previously described in detail [10,12,13,14].
The patients were transported to the CT suite on the day of the surgery. An initial CT scan was performed to confirm the most recent finding of a pulmonary nodule. Under local anesthesia and CT guidance, a 22-Gauge Chiba needle was advanced to the nodule or an adjacent site, and 0.1–0.3 mL of PBV dye (patent blue V 2.5%; Guerbet, Aulnay-sous-Bois, France) was injected into the nodule. For deep-seated nodules, when the dye was not visible on the pleural surface, an additional 0.2 mL injection was administered along the localization tract into the subpleural area. A repeat CT scan was then performed to evaluate the dye distribution and potential complications. The patients were subsequently transferred back to the ward to await surgery.
Extended segmentectomy was performed using video-assisted thoracoscopic surgery. Segmental arteries and veins were divided using curved-tip endovascular staplers (Johnson & Johnson Institute, Cincinnati, OH, USA), and the segmental bronchus and lung parenchyma were divided using endoscopic staplers (Johnson & Johnson Institute; Medtronic, Minneapolis, MN, USA). The dye markings and pinholes on the pleura guided tumor orientation, whereas the deeper dye facilitated precise localization. Together, these findings determined the resection line beyond the virtual intersegmental plane for extended segmentectomy to ensure adequate margins. Mediastinal lymph node dissection was performed in all patients.
2.5. Postoperative Management and Follow-Up
Intravenous analgesics were administered as required during the immediate postoperative period. Once patients resumed oral intake, additional analgesics, such as celecoxib and acetaminophen, were administered. Postoperative chest radiography was performed the following morning. The chest tube was removed when no air leak was detected and the drainage volume was <200 mL/d. Complications were classified using the extended Clavien–Dindo classification [15].
The endpoint of this study was all-cause mortality. Patients underwent CT and tumor-marker surveillance every 6 months for 5 years, and annually thereafter, until death or study termination (16 February 2025).
2.6. Data Collection and Statistical Analysis
Patient characteristics and perioperative and long-term outcomes were obtained from medical records. A five-factor modified Frailty Index (mFi-5) was used to assess frailty, which may influence postoperative outcomes. Preoperative and postoperative lung volumes were calculated from CT scans using AVIEW software version 1.1 (Coreline Soft, Seoul, Republic of Korea) [16].
Propensity score matching was used to balance baseline covariates, including age, sex, forced expiratory volume in the first second, and tumor location, size, and depth. The lobectomy group was 1:1 matched to the extended segmentectomy group using the greedy nearest-neighbor algorithm with a caliper of 0.02.
Statistical analyses were performed using SPSS Statistics (version 27.0; IBM, Armonk, NY, USA). Categorical data are presented as numbers (%) and were analyzed using Fisher’s exact or chi-square tests. Continuous data are presented as the median [interquartile range] or mean ± standard deviation. Normality was evaluated using the Shapiro–Wilk test. The Student’s t-test was used for normally distributed variables and the Mann–Whitney U test for non-normal distributions. Differences between the groups were reported using the Hodges–Lehmann estimator with 95% confidence intervals (CIs). Statistical significance was set at two-sided p < 0.05. Disease-free and overall survival were estimated using the Kaplan–Meier method and compared using the log-rank test.
3. Results
Patients in both groups were propensity score-matched at a 1:1 ratio, and 30 matched pairs were analyzed. The patient characteristics of the two matched groups are summarized in Table 1 and were comparable.
The perioperative outcomes are shown in Table 2. The median localization time for CT-guided dye localization extended segmentectomy was 19 min, with no localization-related complications greater than Clavien–Dindo grade II. The operative time was shorter (102 ± 34 vs. 181 ± 42 min, p < 0.001), and the blood loss was lower (0 [0–0] vs. 0 [0–62.5] mL, p < 0.001) in the extended segmentectomy group than in the lobectomy group. However, both the number of lymph node retrieval stations (3 [2–4] vs. 5 [5–6], p < 0.001) and the total number of lymph nodes retrieved (4 [3–8] vs. 12 [8–15], p < 0.001) were lower in the extended segmentectomy group than in the lobectomy group. Postoperatively, the extended segmentectomy group had a shorter chest tube duration (1 [1–2] vs. 2 [2–3] d, p = 0.002) and shorter postoperative hospital stay (3 [3–4] vs. 5 [4–6] d, p < 0.001). The resection margins were negative in both groups. The median pathological resection margin in the extended segmentectomy group was 1.0 cm. The 90-d morbidity rate did not differ significantly between the groups, and no 90-d mortality was observed.
The functional outcomes are summarized in Table 3. At 6 months, both ipsilateral and total lung volume reduction were significantly smaller in the extended segmentectomy group than in the lobectomy group (10.4 [1.9–15.7] vs. 20.0 [10.0–26.2] %, p = 0.004; and 1.3 [−3.5–6.4] vs. 6.5 [1.4–12.9] %, p = 0.022, respectively).
Figure 3 shows the overall and disease-free survival. The 5-year disease-free survival rates were 100% and 93.1% in the extended segmentectomy and lobectomy groups, respectively (p = 0.539). The 5-year overall survival rates were 100% and 96.4%, respectively (p = 0.837).
4. Discussion
CT-guided dye localization extended segmentectomy achieved shorter operative time, less blood loss, and shorter chest tube duration and hospital stay than lobectomy for deep intersegmental early-stage lung adenocarcinoma, with smaller lung volume reduction and comparable oncologic outcomes.
The non-inferiority of segmentectomy to lobectomy for stage IA1 and IA2 non-small cell lung cancer has been demonstrated in recent randomized trials [2,3,4,5]. Most of these studies included patients with peripheral lung lesions who underwent conventional segmentectomy to obtain adequate resection margins. However, segmentectomy for deep-seated nodules without compromising oncologic outcomes has also been reported in observational studies [17,18,19,20,21]. In real-world practice, intersegmental plane lesions are not uncommon, and determining the optimal parenchymal resection line for such lesions remains challenging, particularly when they are located deep within the pulmonary parenchyma [22]. Extended segmentectomy for these lesions has been facilitated in some centers by virtual-assisted lung mapping, intraoperative cone-beam CT-guided dye localization, or electromagnetic navigation bronchoscopy-guided radiofrequency identification marker placement to ensure adequate resection margins [8,9,10,11]. In addition to other emerging localization techniques, we developed a CT-guided dye localization method performed under local anesthesia in the CT suite to mark both the pleural and deep sites of the lesions. During extended segmentectomy, the inflation-deflation method and visible dyes delineate the resection line beyond the virtual intersegmental plane, ensuring adequate margins. Compared with other approaches, our cohort demonstrated short localization and operative times, and a 100% complete resection rate, indicating that the technique is simple yet effective [10].
The efficacy of new technology-assisted extended segmentectomy for deep intersegmental early-stage lung cancer, in terms of perioperative and long-term outcomes compared with lobectomy, has not been previously reported. Similar to prior studies comparing segmentectomy and lobectomy for small lung nodules, the 5-year overall and disease-free survival rates were comparable between the groups [2,3,4,5]. Although perioperative outcomes vary across the literature, most reports have shown that more lymph nodes are harvested in lobectomies than in segmentectomies, which is consistent with our findings. In contrast, our study demonstrated less blood loss and shorter operative time in the extended segmentectomy group, whereas previous reports have described comparable blood loss and longer operative times in the segmentectomy group. Chest tube duration and hospital stay were also shorter after extended segmentectomy than after lobectomy in our study, whereas they were generally comparable in a prior series. This may be attributed to the accurate CT-guided localization and stapler division of the intersegmental planes. Postoperative morbidity and mortality rates were not significantly different between the two groups, consistent with earlier reports [5,23,24,25,26]. We used CT-derived lung volume reduction as a surrogate for postoperative pulmonary function, as spirometric assessments were not routinely performed, particularly during the pandemic period [27,28]. At 6 months, both total and ipsilateral lung volume reductions were smaller in the extended segmentectomy group than in the lobectomy group, indicating that despite a slightly larger resection than conventional segmentectomy, extended segmentectomy effectively preserved lung function.
Our study had several limitations. First, the sample size in both groups was relatively small, which may have limited statistical power. Second, this was a retrospective study with comparisons based on historical controls. Although propensity score matching was applied to minimize selection bias and confounding factors, unmeasured or time-varying confounders may still exist. Finally, data on resection margins were incomplete due to the retrospective design; however, all available specimens had negative margins, and no local recurrence occurred in the extended segmentectomy group during follow-up.
5. Conclusions
CT-guided dye localization extended segmentectomy provides favorable perioperative and functional outcomes and achieves comparable oncologic control in selected patients with deep intersegmental early-stage lung adenocarcinoma, representing a potential alternative to lobectomy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hendrix W. Rutten M. Hendrix N. van Ginneken B. Schaefer-Prokop C. Scholten E.T. Prokop M. Jacobs C. Trends in the incidence of pulmonary nodules in chest computed tomography: 10-year results from two Dutch hospitals Eur. Radiol.2023338279828810.1007/s 00330-023-09826-337338552 PMC 10598118 · doi ↗ · pubmed ↗
- 2Altorki N. Wang X. Kozono D. Watt C. Landrenau R. Wigle D. Port J. Jones D.R. Conti M. Ashrafi A.S. Lobar or sublobar resection for peripheral stage IA non–small-cell lung cancer N. Engl. J. Med.202338848949810.1056/NEJ Moa 221208336780674 PMC 10036605 · doi ↗ · pubmed ↗
- 3Saji H. Okada M. Tsuboi M. Nakajima R. Suzuki K. Aokage K. Aoki T. Okami J. Yoshino I. Ito H. Segmentectomy versus lobectomy in small-sized peripheral non-small-cell lung cancer (JCOG 0802/WJOG 4607 L): A multicentre, open-label, phase 3, randomised, controlled, non-inferiority trial Lancet 20223991607161710.1016/S 0140-6736(21)02333-335461558 · doi ↗ · pubmed ↗
- 4Stamatis G. Leschber G. Schwarz B. Brintrup D.L. Flossdorf S. Passlick B. Hecker E. Kugler C. Eichhorn M. Krbek T. Survival outcomes in a prospective randomized multicenter Phase III trial comparing patients undergoing anatomical segmentectomy versus standard lobectomy for non-small cell lung cancer up to 2 cm Lung Cancer 202217210811610.1016/j.lungcan.2022.08.01336058174 · doi ↗ · pubmed ↗
- 5Wang L. Zhou J. Jing S. Liu B. Fang J. Xue T. Sublobar or lobar resection in early-stage peripheral non-small cell lung cancer less than 2cm: A meta-analysis for randomized controlled trials Am. J. Surg.202524111606910.1016/j.amjsurg.2024.11606939522446 · doi ↗ · pubmed ↗
- 6Tsubota N. Ayabe K. Doi O. Mori T. Namikawa S. Taki T. Watanabe Y. Ongoing prospective study of segmentectomy for small lung tumors. Study Group of Extended Segmentectomy for Small Lung Tumor Ann. Thorac. Surg.1998661787179010.1016/S 0003-4975(98)00819-49875790 · doi ↗ · pubmed ↗
- 7Yoshikawa K. Tsubota N. Kodama K. Ayabe H. Taki T. Mori T. Prospective study of extended segmentectomy for small lung tumors: The final report Ann. Thorac. Surg.200273105510591055–1058, discussion 1058–105910.1016/S 0003-4975(01)03466-X 11996240 · doi ↗ · pubmed ↗
- 8Sato M. Kuwata T. Kitamura A. Misawa K. Imashimizu K. Yamanashi K. Ikeda M. Koike T. Kobayashi M. Fukai R. The role of virtual-assisted lung mapping in the resection of ground glass nodules J. Thorac. Dis.2018102638264710.21037/jtd.2018.05.1329997925 PMC 6006076 · doi ↗ · pubmed ↗