A Novel Nomogram Integrating Systemic Immune-Inflammation Index and Serum Prealbumin for Predicting Unplanned Readmission in Male Patients with Coexisting Lung Cancer and Chronic Obstructive Pulmonary Disease
Zhenjue Qian, Cuixia Niu, Jian Yang, Xingran Du, Yuting Wen, Li Wang, Hai Zhong, Xiuwei Zhang, Bing Wan, Zhangmin Ke

TL;DR
This study created a tool to predict unplanned hospital readmissions in men with both lung cancer and COPD using inflammation, nutrition, and cancer stage data.
Contribution
A novel nomogram integrating SII and prealbumin for predicting unplanned readmission in male patients with lung cancer and COPD.
Findings
The nomogram achieved good predictive accuracy with an AUC of 0.809.
SII and advanced cancer stage were significant independent risk factors for unplanned readmission.
The tool showed excellent calibration and clinical net benefit via Decision Curve Analysis.
Abstract
Patients with coexisting lung cancer and chronic obstructive pulmonary disease (COPD) face a disproportionately high risk of unplanned readmission. This study developed and internally validated a user-friendly nomogram based on the “inflammation-nutrition-tumor” framework, using routinely available clinical parameters—specifically age, cancer stage, the Systemic Immune-Inflammation Index (SII), and serum prealbumin. SII is a composite marker derived from standard complete blood counts, reflecting systemic inflammation, while prealbumin serves as a sensitive indicator of nutritional status. The nomogram demonstrated good predictive accuracy (AUC = 0.809) and clinical utility in our male cohort, outperforming simpler models based on age and cancer stage alone. This tool may empower clinicians to identify high-risk patients and implement targeted, cost-effective interventions—such as…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
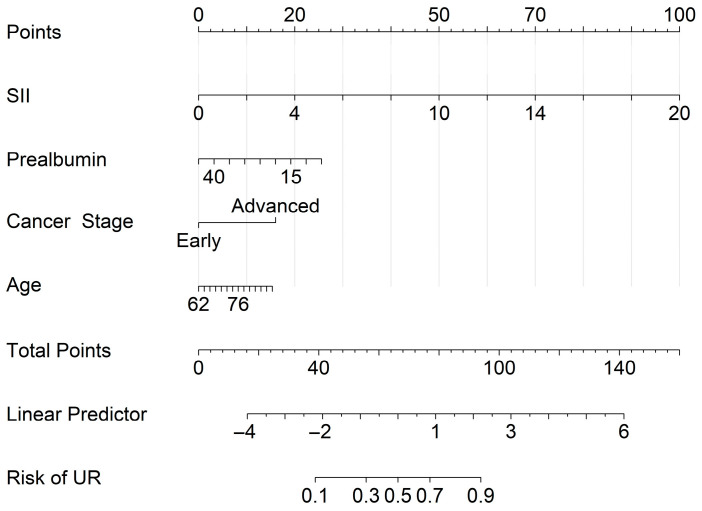 Figure 1
Figure 1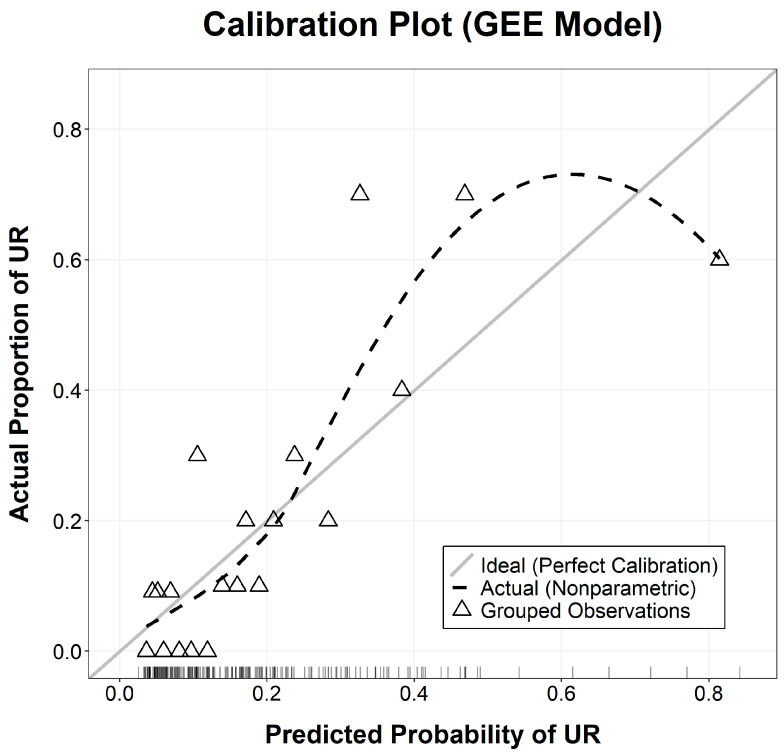 Figure 2
Figure 2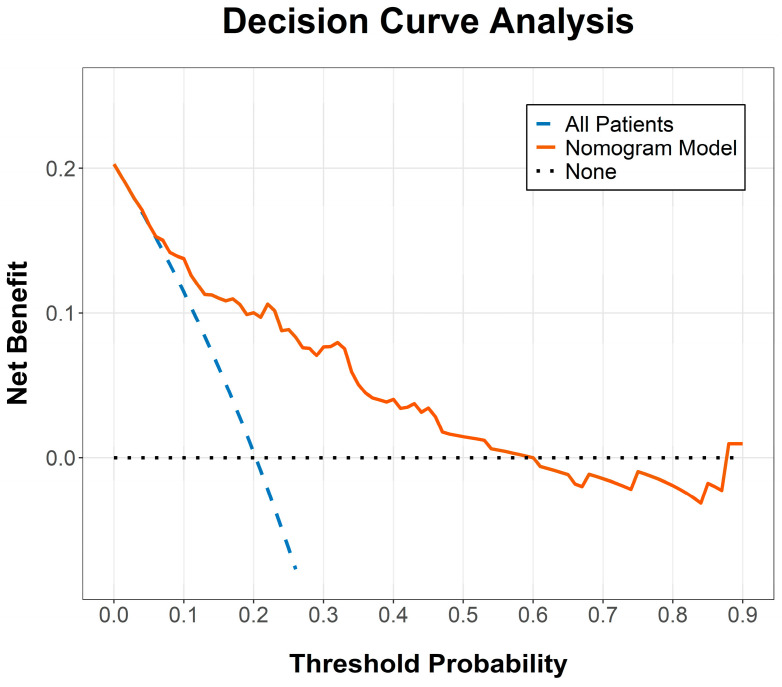 Figure 3
Figure 3- —Nanjing Medical University Science and Technology Development Fund Project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Biomarkers in Disease Prognosis · Lung Cancer Diagnosis and Treatment · Chronic Obstructive Pulmonary Disease (COPD) Research
1. Introduction
Lung cancer [1] and chronic obstructive pulmonary disease (COPD) [2,3] are the leading causes of respiratory-related mortality and disability worldwide. These two conditions are not only epidemiologically linked through shared risk factors such as tobacco smoking and environmental pollutants but are also pathophysiologically intertwined, forming a complex “lung cancer-COPD coexistence” [4]. Reports indicate that approximately 40–70% of lung cancer patients have comorbid COPD [5]. This coexistence creates a synergistic negative effect, which is associated with more severe clinical symptoms, limited treatment options, and significantly worsened prognosis compared to either disease alone. Notably, unplanned readmission has emerged as a critical negative indicator for healthcare quality and patient outcomes in this population [6,7,8].
Research suggests that nearly one-fifth of COPD patients are readmitted during the “vulnerable window” following discharge [9,10]. In patients where lung cancer and COPD coexist, this clinical management challenge is further amplified, as comorbid COPD is a significant risk factor for poor outcomes in lung cancer patients [11,12]. Frequent readmissions not only signal unsuccessful disease management but also impose heavy physical, psychological, and financial burdens on patients and their families while straining healthcare systems. Currently, clinical decisions regarding discharge readiness often rely on subjective experience or limited indicators, lacking quantified and personalized risk stratification tools for this specific comorbidity.
Traditionally, risk prediction has relied on comprehensive scoring systems such as the Charlson Comorbidity Index (CCI) or the Elixhauser Comorbidity Index [13,14,15]. However, these indices have notable limitations when applied to the unplanned readmission risk of lung cancer-COPD patients. The CCI, for instance, summarizes respiratory conditions as a binary “chronic pulmonary disease” category, failing to account for the severity of COPD (e.g., GOLD grades) or the dynamic exacerbation frequency [16,17]. Moreover, these static diagnostic counts cannot capture the acute pathophysiological changes occurring during the peri-discharge period.
Recent trends in precision medicine have shifted focus toward quantifiable biomarkers and pathophysiological indicators. Systemic inflammation and malnutrition are now recognized as pivotal factors influencing the prognosis of lung cancer patients [18,19]. Peripheral blood-derived inflammatory markers, such as the systemic immune-inflammation index (SII), offer a low-cost and highly accessible means of risk assessment [20]. Furthermore, integrating inflammatory markers with nutritional indicators like serum albumin and prealbumin has demonstrated superior prognostic value [21,22]. While nomograms have been utilized to visualize complex regression models for individualized risk assessment in various cancers [23,24,25,26,27,28,29], a specialized tool for predicting unplanned readmission in the lung cancer-COPD comorbid population remains scarce.
Therefore, the present study aimed to retrospectively evaluate the correlation between “inflammation-nutrition” axis indicators and unplanned readmission risk in patients with lung cancer and COPD. We sought to construct and internally validate a practical, visualized nomogram to facilitate identification and precise intervention for high-risk individuals, ultimately improving patient prognosis and optimizing healthcare resource allocation.
2. Materials and Methods
2.1. Study Design and Participant Selection
This retrospective study was conducted at Affiliated Jiangning Hospital of Nanjing Medical University. We identified patients diagnosed with both lung cancer and Chronic Obstructive Pulmonary Disease (COPD) between 1 January 2021 and 31 December 2025. Lung cancer was confirmed by pathological or cytological evidence, while COPD was diagnosed according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria. The inclusion criteria were: (1) aged ≥ 18 years; (2) histologically confirmed lung cancer; (3) concomitant COPD. Exclusion criteria included: (1) major missing baseline clinical data; (2) presence of other active malignancies; (3) acute infections or systemic inflammatory diseases unrelated to lung cancer or COPD. A total of 207 (n = 207) qualified clinical episodes were finally recorded for analysis, with small amounts of missing prealbumin data handled through algorithmic imputation. Because this study investigates readmission, the first hospitalization for each patient was excluded from the analysis. Thus, all 207 episodes represent true readmission events. Notably, all patients identified during this period were male, thus the analysis was conducted on this male-specific cohort.
The study protocols adhered strictly to the ethical principles outlined in the Declaration of Helsinki and were approved by the Institutional Ethics Committee of Affiliated Jiangning Hospital of Nanjing Medicine University (Ethics Approval Number 2026-03-003-K01). Given the retrospective nature of the study, the requirement for informed consent was waived.
2.2. Data Acquisition and Variable Definitions
Comprehensive clinical data were systematically retrieved from the institutional electronic medical record (EMR) system. Demographic parameters included age and tobacco exposure history. Clinical and oncological variables encompassed cancer stage (classified according to the 8th edition of the American Joint Committee on Cancer TNM staging system), histological subtype, and COPD severity, graded per the GOLD criteria.
To ensure consistency and minimize the influence of acute perioperative inflammation or treatment-related fluctuations, all laboratory parameters were obtained from fasting venous blood samples collected during the initial clinical assessment within 24 h of admission, prior to any surgical intervention or systemic therapy. Systemic inflammatory biomarkers include absolute neutrophil count (ANC), absolute lymphocyte count (ALC), platelet count, and C-reactive protein (CRP). Nutritional and biochemical indices include serum albumin, serum prealbumin, and hemoglobin levels.
Specifically, the SII value was calculated using the standardized formula: , where P0, N, and L represent platelet, ANC, and ALC (all expressed as 10^9^/L), respectively. Body Mass Index (BMI) was excluded from the final analysis due to a high proportion of inconsistent measurements and potential inter-observer variability during repeated admissions, which could compromise the stability and reliability of the predictive model. Prealbumin levels were missing in 9.7% (20/207) of cases. To assess the missing data pattern, we compared the clinical characteristics and primary outcomes between the missing group (n = 20) and the non-missing group (n = 187) for prealbumin. The results showed no significant difference in the primary outcome between the two groups (p = 0.973). Similarly, no significant differences were observed in cancer stage (p = 0.074), SII (p = 0.199), or serum albumin (p = 0.079). These findings suggest that the data are missing at random (MAR). Given the low proportion of missing data and its random nature, missing prealbumin values were handled using a median imputation algorithm. This sensitivity analysis confirmed that missing data were unlikely to introduce significant bias, as complete-case and imputed datasets yielded consistent results.
2.3. Definition of the Outcome
The primary outcome was unplanned readmission (UR), defined as any non-elective admission to our hospital within 90 days of discharge from the index hospitalization. We utilized an all-cause unplanned readmission definition to capture the overall clinical burden. A post hoc review indicated that the majority of these readmissions (approximately 90%) were directly attributable to acute exacerbations of COPD or complications from lung cancer (e.g., obstructive pneumonia, pleural effusion, or cancer-related pain). Conversely, planned readmissions (PR) were defined as scheduled, elective admissions for staged procedures or planned treatments and were excluded from the primary outcome analysis. Two clinicians independently reviewed the electronic health records to classify the nature of the readmissions, with a third senior oncologist acting as an adjudicator in cases of disagreement.
2.4. Statistical Analysis
Statistical processing was performed using R software version 4.5.2. Data normality was assessed for continuous variables using the Shapiro–Wilk test and visual inspection of Q-Q plots. Normally distributed continuous variables (e.g., hemoglobin, albumin) were reported as mean ± standard deviation (SD) and compared using Independent-samples t-test. Non-normally distributed data (e.g., SII, prealbumin) were expressed as medians and interquartile ranges Median (IQR) and analyzed using the Mann–Whitney U test. Categorical data were presented as frequencies (%) and analyzed using the test.
To identify robust predictors of readmission while accounting for the dependency among repeated observations from the same patient (207 episodes from 22 unique patients, with a median of 7 episodes per patient), univariate Generalized Estimating Equations (GEE) with a logit link function and an exchangeable working correlation structure were initially conducted. Variables exhibiting p < 0.10 were considered candidates for multivariable analysis. Adhering to the principle of parsimony and the clinical “inflammation-nutrition-tumor” hypothesis, a final multivariable GEE model comprising age, cancer stage, SII, and prealbumin was constructed. To evaluate the predictive value of the integrated biomarkers, a baseline model included only age and cancer stage was also built. A sensitivity analysis excluding the patient with the highest number of episodes (34 episodes) was also performed to assess the robustness of the findings.
A nomogram was subsequently developed based on the GEE model. Model performance was evaluated in terms of discrimination and calibration. Discriminative capacity was assessed using the Area Under the Receiver Operating Characteristic Curve (AUC). The difference in AUC between the proposed model and the baseline model was compared using the DeLong test. Model calibration was evaluated via calibration curves, where 207 episodes were divided into groups based on their predicted probabilities to compare the mean predicted probability with the actual observed readmission rate. Clinical utility was quantitatively assessed via Decision Curve Analysis (DCA). All statistical tests were two-sided, with p < 0.05 denoting statistical significance.
3. Results
3.1. Baseline Characteristics
A total of 207 clinical episodes with coexisting lung cancer and COPD were enrolled, comprising 165 (79.7%) in the PR group and 42 (20.3%) in the UR group. The number of episodes per patient ranged from 1 to 34, with a median of 7 (IQR: 3.25–14). The first hospitalization for each patient was excluded, consistent with this study’s focus on readmission. The comparative analysis of baseline clinical and laboratory parameters is detailed in Table 1. The median age of the entire cohort was 75 years [IQR: 69.0–78.0] in the PR group and 77 years [IQR: 71.0–78.3] in the UR group (p = 0.096).
Episodes in the UR group demonstrated a significantly heightened systemic inflammatory profile, characterized by markedly elevated SII levels [1474.5 (1110.1–1939.8) vs. 504.9 (344.9–712.5), p < 0.001] and CRP concentrations [19.7 (10.9–34.1) vs. 4.9 (2.1–10.4), p < 0.001]. Furthermore, nutritional depletion was more pronounced in the UR cohort, as evidenced by significantly lower serum albumin (34.3 ± 4.2 vs. 38.5 ± 3.9 g/L, p < 0.001) and prealbumin levels [159.5 (130.8–202.3) vs. 201.0 (161.0–246.0) mg/L, p = 0.002]. Oncologically, the UR group presented a higher prevalence of advanced-stage disease (Stage III–IV: 64.3% vs. 39.4%, p = 0.018) and increased COPD severity (GOLD III–IV: 35.7% vs. 20.0%, p = 0.031). Other parameters, including smoking history, histological subtype, and hemoglobin levels, showed no statistically significant disparities between the two groups (p > 0.05).
3.2. Predictor Selection and GEE Analysis Results
3.2.1. Selection Strategy: Balancing Statistical Rigor and Clinical Utility
To develop a predictive model that is both statistically robust and clinically interpretable, we implemented a three-stage selection strategy focused on the “inflammation-nutrition” axis. First, all candidate covariates were initially evaluated using univariable GEE to identify potential predictors associated with the target outcome (p < 0.10), considering that a portion of patients experienced repeated readmissions. Second, for variables representing overlapping biological pathways, selection was guided by clinical sensitivity and physiological relevance. Specifically, between the inflammatory markers SII and CRP, SII was prioritized as it provides a more comprehensive reflection of the immune-inflammatory balance by integrating neutrophils, lymphocytes, and platelets. Similarly, prealbumin was favored over albumin due to its shorter half-life, making it a more sensitive indicator of acute nutritional fluctuations. Third, we compared the stability of models using different combinations of these indices. Variance Inflation Factors (VIF) were calculated to ensure the absence of significant multicollinearity among the final predictors.
3.2.2. Results of Univariable and Multivariable GEE Analysis
Univariable GEE analysis identified several factors potentially associated with the outcome, including age (p = 0.055), cancer stage (p = 0.067), SII (p = 0.003), CRP (p < 0.001), prealbumin (p = 0.050), and albumin (p < 0.001). In the multivariable GEE analysis, when all six variables (age, cancer stage, SII, CRP, albumin, and prealbumin) were included, the p-values for SII and prealbumin were 0.384 and 0.369, respectively, with an AUC of 0.867. However, for the four variable model (age, cancer stage, SII, and prealbumin), the p-values for SII and prealbumin were <0.001 and 0.087, respectively. This sensitivity analysis confirms that CRP and albumin masked the independent contributions of SII and prealbumin, supporting our decision to retain the more clinically relevant markers in the final model. Consequently, the final model was constructed using age, cancer stage, SII, and prealbumin. The VIF values for age, cancer stage, SII, and prealbumin are 1.259, 1.112, 1.048, and 1.186, respectively, indicating no significant multicollinearity. The multivariable results demonstrated that higher age, advanced cancer stage, and elevated SII were independent risk factors, while higher prealbumin levels were associated with reduced risk. Detailed statistics are presented in Table 2. SII was treated as a continuous variable in increments of 500 units to facilitate a more clinically meaningful interpretation of the risk estimates. Consequently, the odds ratios (ORs) presented in Table 2 represent the change in the risk of UR for every 500-unit increase in the baseline SII level.
3.3. Construction and Performance Internal Validation of the Nomogram
Based on the independent predictors identified via multivariable GEE analysis, a visual predictive nomogram was developed (Figure 1). This tool translates the regression coefficients of age, cancer stage, SII, and prealbumin into a point-based scoring system. By summing the individual scores, clinicians can derive a personalized probability of unplanned readmission for each patient.
The model’s discriminative ability to distinguish between different outcomes was internally assessed using the AUC. In this cohort, the nomogram achieved an AUC of 0.809 (95% CI: 0.733–0.885), indicating strong discriminative performance. This was significantly higher than the baseline model (age and cancer stage only), which had an AUC of 0.677 (DeLong’s test, p = 0.0016). This sensitivity analysis demonstrates the incremental value of incorporating SII and prealbumin into the predictive model, confirming that the full nomogram provides superior risk stratification compared to basic clinical variables alone. Via the maximum Youden Index, the optimal cut-off value for the nomogram was determined as 0.210, yielding a sensitivity of 73.8% and a specificity of 79.3%. Another sensitivity analysis excluding the patient with the highest number of episodes (34 episodes) was conducted to assess the robustness of our findings. The results remained consistent: SII remained a strong independent predictor (OR = 1.548, 95% CI: 1.183–2.025, p = 0.001), and the model AUC improved slightly to 0.817 (95% CI: 0.737–0.896), confirming that our conclusions are not driven by a single outlier.
The calibration of the GEE-based model was evaluated using a calibration curve (Figure 2), where the 207 episodes were categorized into 20 nearly equal-sized groups based on their predicted probabilities. This approach ensured that each group contained approximately 10 to 11 cases. The curve demonstrated high agreement between the predicted probabilities and actual observed frequencies, with grouped data points closely aligning with the 45-degree Ideal line, indicating excellent calibration. Furthermore, DCA underscored the clinical utility of the model, demonstrating a superior net clinical benefit across a broad range of threshold probabilities (Figure 3). In this context, the threshold probability represents the level of risk at which a clinician would deem the benefits of an intervention (e.g., intensified monitoring) to outweigh the potential harms or costs. For instance, a threshold of 20% implies that the clinician considers the cost of a missed readmission to be four times greater than the cost of an unnecessary preventative intervention for a patient who would not have been readmitted. These findings confirm that the integrated nomogram is a reliable tool for identifying high-risk patients who may benefit from preemptive clinical management.
4. Discussion
4.1. The “Inflammation-Nutrition-Tumor” Axis in LC-COPD Coexistence
The current study successfully developed and internally validated a clinical nomogram aimed at predicting the risk of unplanned readmission in male patients with concurrent lung cancer and COPD. By integrating systemic inflammatory, nutritional, and oncological indices, we established a predictive tool with a good discriminative capacity (AUC = 0.809). Our findings underscore the pivotal role of the “inflammation-nutrition-tumor” axis in driving clinical instability in this specific patient population.
4.2. The Dominant Role of Systemic Inflammation (SII)
The most profound observation in our study was the strong predictive significance of SII. As a composite biomarker integrating neutrophil, lymphocyte, and platelet counts, SII provides a holistic perspective on the host’s immune-inflammatory equilibrium. In patients with lung cancer and COPD, elevated SII levels may reflect underlying chronic systemic inflammation—a common pathological substrate for both diseases. Neutrophils are known to play a role in tumor invasion and airway remodeling through the release of proteolytic enzymes, while lymphopenia has been associated with impaired anti-tumor immunity. Our multivariable analysis demonstrated that SII serves as a highly significant independent risk factor (p < 0.001), suggesting that intensified inflammatory monitoring could be instrumental in identifying patients prone to acute post-discharge deterioration.
4.3. Nutritional Vulnerability and the Significance of Prealbumin
Nutritional status, represented here by serum prealbumin, emerged as another critical component of our predictive framework. Although prealbumin did not meet the conventional threshold for statistical significance in the multivariable GEE model (p = 0.087), it was retained due to its clinical relevance and its role within the “inflammation-nutrition” framework. Unlike albumin, prealbumin possesses a shorter half-life, making it a more sensitive indicator of acute changes in nutritional reserves. In our UR group, significantly lower prealbumin levels likely signify a reduced physiological reserve, leaving patients vulnerable to infections and COPD exacerbations—the primary catalysts for unplanned readmissions.
4.4. Oncological Burden and Rationale for Model Selection
Oncological factors, specifically cancer stage, proved indispensable for accurate risk assessment. Stage III–IV disease was a significant predictor in the final GEE model (OR = 3.59, p = 0.014), underscoring its substantial clinical impact. Advanced-stage lung cancer is frequently associated with a higher tumor burden and necessitates more aggressive therapeutic regimens, which can exacerbate underlying COPD symptoms.
A critical consideration in this study was the selection of the final predictive model. While a model incorporating CRP and albumin yielded a higher statistical AUC, we prioritized the “age + cancer stage + SII + prealbumin” model. This decision was based on biological plausibility, as the coexistence of lung cancer and COPD involves a profound metabolic shift leading to “cancer-COPD cachexia.” Including prealbumin ensures the nomogram captures the “nutritional reserve” component, which is essential for identifying patients at risk of physiological decline. Furthermore, the statistical difference between the models was marginal when considering the holistic value. The chosen model also demonstrated good sensitivity (73.8%) and specificity (79.3%), offering a balanced tool for patient management.
4.5. Clinical Utility and Limitations
The proposed nomogram offers several practical advantages for clinical application. Firstly, it relies on laboratory parameters (SII and prealbumin) that are routinely obtained during standard admission, ensuring high feasibility without additional economic burden. Secondly, clinicians can use the nomogram at discharge to identify high-risk patients who may benefit from proactive strategies, such as personalized pulmonary rehabilitation, nutritional optimization, and more frequent post-discharge monitoring. For instance, a high-risk score could trigger a “Transition of Care” protocol, including a nutritional consult and an early post-discharge multidisciplinary clinic visit.
The proposed risk cutoff (e.g., a total score corresponding to a 25% predicted risk of UR) is intended as a clinical triage tool rather than a definitive diagnostic threshold. Patients identified as “High Risk” based on this cutoff could warrant the initiation of a multidisciplinary intervention bundle prior to discharge. This may include intensified pulmonary rehabilitation, optimization of bronchodilator therapy, and a mandatory follow-up teleconsultation within 72 h of discharge. While a lower threshold would increase sensitivity to capture more potential readmissions, the trade-off involves a higher burden on outpatient resources. Thus, the specific cutoff should be adaptable, allowing individual institutions to calibrate it based on their capacity for post-discharge monitoring and intervention.
Several limitations of this study warrant consideration. First, the cohort consisted exclusively of male cohort, reflecting the epidemiological reality that the prevalence of coexisting lung cancer and COPD is significantly higher in males within our specific regional demographic. However, the exclusion of female patients inherently limits the generalizability of our findings. Hormonal differences and varying smoking patterns between genders may influence both inflammatory profiles and respiratory outcomes; therefore, these results should be extrapolated to female populations with caution. Second, while median imputation was used for the minor missing prealbumin data (9.7%), and a sensitivity analysis suggested the data were missing at random, potential bias cannot be entirely excluded. Third, although the data are clustered within 22 patients, the use of GEE appropriately accounts for intra-patient correlation. A sensitivity analysis excluding the most extreme patient yielded consistent results (e.g., SII OR = 1.548, p = 0.001; AUC = 0.817), supporting the robustness of our model. Nonetheless, the small number of unique patients limits the generalizability, and external validation in larger cohorts is essential. Fourth, and most importantly, this study represents a model development and internal validation phase. Although internal validation via calibration plots and DCA demonstrated robust performance, these methods only assess model optimism within the derivation cohort. External validation in independent, multi-center cohorts is essential to confirm the model’s generalizability, predictive precision, and clinical utility across diverse geographic regions, ethnic populations, and clinical settings. Furthermore, as a single-center [30] retrospective study, the developed nomogram may be influenced by local clinical practices and patient demographics. To address this limitation, we are planning a prospective multi-center validation study across multiple institutions in different geographic regions. This will allow us to assess the model’s generalizability, evaluate its performance across diverse patient populations, and refine the nomogram based on heterogeneous clinical practices before considering its broader clinical implementations.
5. Conclusions
In summary, this study identified SII as a strong independent predictor of unplanned readmission in male patients with coexisting lung cancer and COPD. The developed nomogram, integrating age, SII, serum prealbumin, and cancer stage, provides a reliable and individualized risk-assessment tool during this model development phase. This “inflammation-nutrition-tumor” framework may help clinicians identify high-risk individuals for targeted interventions, with the goal of reducing readmission rates. External validation in prospective, multi-center cohorts is required before this tool can be recommended for widespread clinical implementation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hendriks L.E.L. Remon J. Faivre-Finn C. Garassino M.C. Heymach J.V. Kerr K.M. Tan D.S.W. Veronesi G. Reck M. Non-small-cell lung cancer Nat. Rev. Dis. Primers 2024107110.1038/s 41572-024-00551-939327441 · doi ↗ · pubmed ↗
- 2de Oca M.M. Perez-Padilla R. Celli B. Aaron S.D. Wehrmeister F.C. Amaral A.F.S. Mannino D. Zheng J. Salvi S. Obaseji D. The global burden of COPD: Epidemiology and effect of prevention strategies Lancet Respir. Med.20251370972410.1016/S 2213-2600(24)00339-440684784 · doi ↗ · pubmed ↗
- 3Aaron S.D. Vandemheen K.L. Whitmore G.A. Bergeron C. Boulet L. CôtéA. Mclvor R.A. Penz E. Field S.K. Lemière C. Early diagnosis and treatment of COPD and asthma—A randomized, controlled trial N. Engl. J. Med.20243902061207310.1056/NEJ Moa 240138938767248 · doi ↗ · pubmed ↗
- 4Qi C. Sun S.W. Xiong X.Z. From COPD to lung cancer: Mechanisms linking, diagnosis, treatment, and prognosis Int. J. Chron. Obstruct. Pulmon. Dis.2022172603262110.2147/COPD.S 38073236274992 PMC 9586171 · doi ↗ · pubmed ↗
- 5Zhou C. Qin Y. Zhao W. Liang Z. Li M. Liu D. Bai L. Chen Y. Chen Y. Cheng Y. International expert consensus on diagnosis and treatment of lung cancer complicated by chronic obstructive pulmonary disease Transl. Lung Cancer Res.2023121661170110.21037/tlcr-23-33937691866 PMC 10483081 · doi ↗ · pubmed ↗
- 6Zumbrunn A. Bachmann N. Bayer-Oglesby L. Joerg R. SIHOS Team Social disparities in unplanned 30-day readmission rates after hospital discharge in patients with chronic health conditions P Lo S ONE 202217 e 027334210.1371/journal.pone.027334236137092 PMC 9499293 · doi ↗ · pubmed ↗
- 7Kan S.W. Yen H.Y. Chi M.J. Huang H.Y. Influence of physical function and frailty on unplanned readmission in middle-aged and older patients discharged from a hospital Sci. Rep.2025151000310.1038/s 41598-025-94945-840122992 PMC 11930979 · doi ↗ · pubmed ↗
- 8Sharma Y. Mangoni A.A. Rao S. Batuwaththagamage I.K. Kaambwa B. Woodman R. Horwood C. Thompson C. Prevalence and characteristics of potentially avoidable unplanned readmissions: A retrospective cohort study Aust. Health Rev.202549 AH 2426110.1071/AH 2426140588225 · doi ↗ · pubmed ↗