Oncological Feasibility of Conservative Axillary Surgery (Opinion Article): Tailored Axillary Surgery vs. Axillary Reverse Mapping-Guided Axillary Lymph Node Dissection
Masakuni Noguchi, Yusuke Haba, Emi Morioka, Masafumi Inokuchi

TL;DR
This paper reviews the cancer safety of less invasive axillary surgery techniques and their potential to reduce side effects without increasing recurrence risk.
Contribution
The paper evaluates the oncological feasibility of tailored axillary surgery and ARM-guided ALND based on current literature.
Findings
ALND after TAS found additional involved nodes in 60–70% of patients.
ARM nodes were involved in 15.7–64.7% of patients after conventional ALND.
Postoperative radiotherapy may prevent recurrence in patients with microscopic residual disease.
Abstract
Conventional axillary lymph node dissection (ALND) is associated with postoperative morbidities, including arm lymphedema, seroma, reduced shoulder mobility and local sensory dysfunction. Sentinel lymph node (SLN) biopsy has been introduced for assessing axillary nodal status in clinically node-negative (cN0) patients. However, ALND continues to be indicated for staging purposes and regional control in clinically node-positive (cN+) patients. Tailored axillary surgery (TAS) and axillary reverse mapping (ARM)-guided ALND have been developed to avoid arm lymphedema without increasing a risk of axillary recurrence. However, because TAS and ARM-guided ALND are much less radical than conventional ALND, their oncological feasibility remains a crucial consideration. For conventional ALND performed after TAS, additional involved nodes were found in 60–70% of patients. ARM nodes also were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
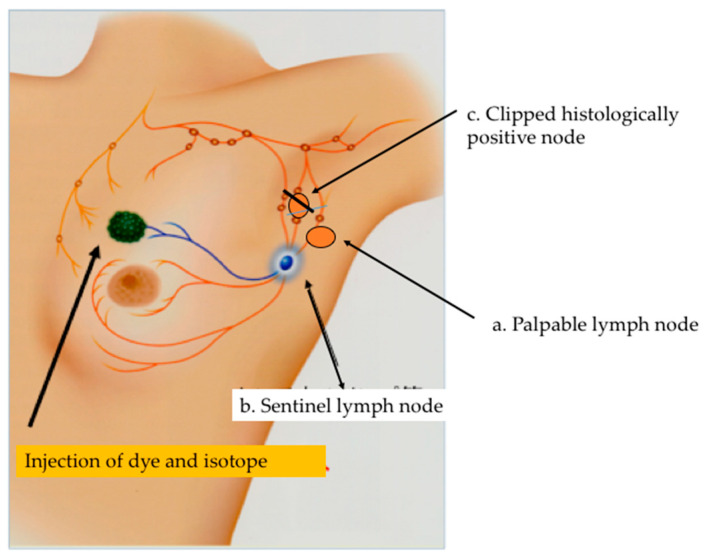 Figure 1
Figure 1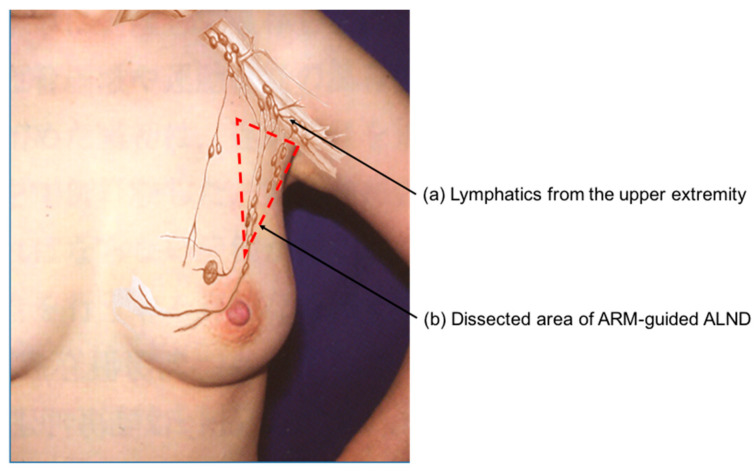 Figure 2
Figure 2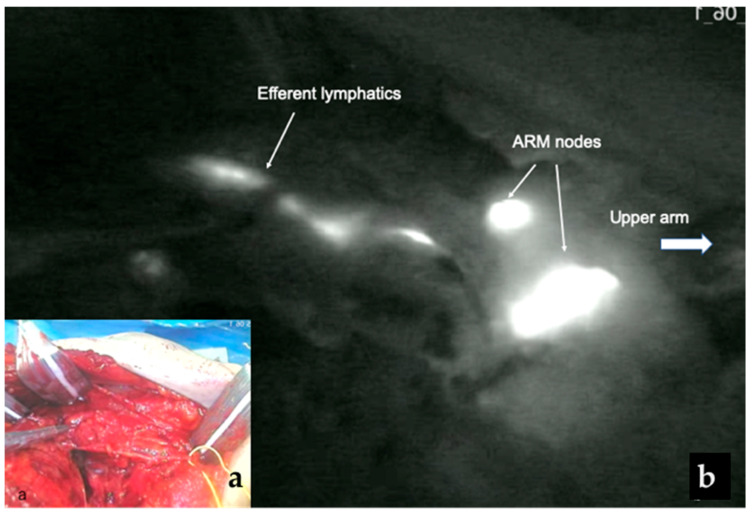 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphatic System and Diseases · Breast Cancer Treatment Studies · Breast Implant and Reconstruction
1. Introduction
Axillary surgery is a key component of breast cancer surgery for staging and treatment. However, ALND is postoperatively associated with several morbidities, including arm lymphedema, seroma, reduced shoulder mobility and local sensory dysfunction. Notably, the risk of arm lymphedema after ALND was reported to be 25% in a recent review [1]. This has often been used as an argument against ALND. Sentinel lymph node (SLN) biopsy has been performed for assessing axillary nodal status in clinically node-negative (cN0) patients [2,3]. Since its introduction, axillary surgery for breast cancer patients has changed tremendously over the past few decades. Currently, ALND can be avoided not only in cN0 patients with negative SLNs [4,5] but also in cN0 patients with fewer than three positive SLNs receiving breast radiation or axillary radiation [6,7]. Furthermore, ALND may be avoided in clinically node-positive (cN+) patients whose nodal status becomes SLN-negative following neoadjuvant chemotherapy (NAC) [8]. However, ALND continues to be indicated for staging purposes and for the treatment of regional disease in a significant number of cN+ patients [9,10]. Recently, various forms of conservative axillary surgery such as TAS and ARM-guided ALND have been developed to replace or supplement conventional ALND. In the era of effective multimodality therapy, completion ALND removing all microscopic axillary disease may be not necessary in both cN0 patients and cN+ patients. However, there remains a lack of consensus among surgeons regarding conservative axillary surgery. Therefore, in this article, we evaluated the oncological feasibility of conservative axillary surgery including TAS and ARM-guided ALND.
2. Conservative Axillary Surgery
Conservative axillary surgery has been developed to avoid arm lymphedema without increasing a risk of axillary recurrence. It includes conservative axillary regional excision (CARE) [11], tailored axillary surgery (TAS) [12,13], partial lower ALND [14] and ARM-guided ALND [15,16] (Table 1). Conservative axillary surgery is conceptually divided into two groups. The first group includes TAS and CARE, which commonly remove SLNs and other palpable suspicious nodes, although TAS may optionally be performed with image-guided localization of the histologically involved clipped node. The second group includes ARM-guided ALND and partial lower ALND, which aim to preserve upper-extremity lymphatic drainage. Partial lower ALND preserves the axillary lymph nodes and lymphatics located between the second intercostobrachial nerve and axillary vein [14], whereas ARM-guided ALND is performed in a personalized fashion to preserve the lymphatics of the upper extremity [17,18]. In this article, we evaluate the oncological feasibility of TAS and ARM-guided ALND.
3. Tailored Axillary Surgery (TAS)
TAS was developed as an alternative to ALND for cN+ patients [12]. This procedure removes all palpable suspicious lymph nodes together with SLNs, and may be optionally performed with image-guided localization of the clipped node to achieve optimal results. TAS aims to convert a cN+ axilla into a cN0 one, mainly by palpation-guided selective removal of grossly involved nodal disease [19] (Figure 1). Postoperative radiotherapy is routinely used to achieve local control in patients with low-volume remaining nodal disease. However, the value of this procedure with respect to long-term regional control and survival needs to be investigated in a prospective randomized trial.
A randomized clinical TAXIS trial comparing TAS in combination with axillary irradiation to conventional ALND has been performed in NAC and upfront surgery settings. Although the selective removal of clipped nodes by image-guided localization is not a mandatory part of TAS, clipped nodes were removed in 94.3% of patients. All patients either undergo adjuvant whole-breast irradiation after breast-conserving surgery (BCS) or chest-wall irradiation after mastectomy. The ongoing TAXIS trial will determine whether axillary treatment with TAS and radiotherapy is oncologically non-inferior and associated with improved quality of life compared to conventional ALND in cN+ patients [12]. A total of 1500 patients was randomized and accrual completion was expected in 2025. An analysis of the primary endpoint will be published in 2030 [13,19].
However, for ALND performed after TAS in a phase II TAXIS trial, additional involved nodes were found in 70% of upfront surgery patients and 60% of NAC patients [12]. Although all these patients received postoperative irradiation after TAS, the incidence of additional involved nodes was much higher compared with corresponding rates from the Z0011 and AMAROS trials [6,7]. The incidence of additional involved nodes after SLN biopsy was 27.4% in the Z0011 trial and 33% in the AMAROS trial, in which most patients in the SLN biopsy-alone group did not develop axillary recurrence [20] (Table 2). Nevertheless, these trials are not directly comparable because they involved fundamentally different patient populations (cN+ in the TAXIS trial vs. cN0 in the Z0011 and AMAROS trials).
The landmark NSABP B-04 trial serves as a reference with relevant data. In its observation arm (no ALND or axillary radiation), ipsilateral axillary nodes were the first site of failure in only 18% of cN0 patients, despite an expected histological nodal positivity rate of 40% in cN0 patients. The rate of axillary recurrence was reduced to 3% after axillary radiotherapy in cN0 patients. On the other hand, the rate of axillary recurrence was reduced to 12% after radiotherapy in cN+ patients, despite an expected histological nodal positivity rate of 73% [21] (Table 2). When a cN+ axilla becomes cN0 after TAS, postoperative radiotherapy would reduce the axillary recurrence rate. It has been suggested that outcomes will be favorable in the TAXIS trial [12].
The TAXIS phase III trial is being conducted to test the hypothesis that TAS with axillary radiotherapy is non-inferior to conventional ALND in terms of disease-free survival of cN+ patients at first presentation in the era of effective systemic therapy and regional nodal irradiation [22]. We await the results of the TAXIS trial involving a large number of cN+ patients as they will help determine the benefit of TAS. Oncological non-inferiority is hypothetical until mature results from TAXIS phase III are available. Moreover, tumor biology should be considered when omitting ALND [23]. The biological and systemic therapy landscape has evolved significantly in the current cN+ population.
4. Axillary Reverse Mapping (ARM)–Guided ALND
The occurrence of arm lymphedema is mainly due to the unnecessary sacrifice of upper extremity lymphatics. ARM-guided ALND was developed to delineate and preserve the lymphatic drainage pathways of the arm during ALND, thereby minimizing arm lymphedema (Figure 2) [15,16]. The ARM technique is based on the hypothesis that arm lymphatics are distinct from breast lymphatics, and thus axillary nodes and lymphatics from the upper extremity are theoretically not involved. The ARM approach has the potential to reduce the incidence of arm lymphedema [24,25]. A meta-analysis including 1696 patients favored ALND with ARM compared with conventional ALND alone for preventing arm lymphedema occurrence (4.8% vs. 18.8% respectively; p < 0.0001) [26]. However, there have been concerns about the oncological feasibility of ARM due to the involvement of ARM nodes [24,25,27,28,29,30]. Anatomically, there are lymphatic interconnections between nodes draining from the upper extremity and nodes draining from the breast [31,32].
The ARM procedure was originally performed using blue dye [15,16]. A meta-analysis of studies using blue dye alone to identify ARM nodes reported ARM node and/or lymphatics identification rates ranging from 47% to 89% and metastatic involvement rates for ARM nodes ranging from 0% to 27% [33]. In contrast, when indocyanine green (ICG) fluorescence was used, identification rates of ARM node and/or lymphatics were found to range from 81% to 96%, with metastatic involvement rates for ARM nodes ranging from 3% to 22% [33]. Thus, fluorescence provides better intraoperative visualization of lymphatic vessels and nodes than blue dye [34,35,36,37,38].
The FARM trial was recently conducted to evaluate the utility of fluorescence ARM-guided ALND in breast cancer. In this study, fluorescent ARM nodes were successfully found and removed within the ALND field in 95% of patients (95/100) and were involved with metastases in 18.9% of patients. The rate of involved ARM nodes was not significantly different between the upfront surgery patients and the NAC patients [39] (Table 3). In our previous study using ICG fluorescence-guided ARM, however, fluorescent ARM nodes were involved in 35.4% of NAC patients and 64.7% of upfront surgery patients [40]. Because the fluorescence method is highly sensitive in visualizing ARM nodes and lymphatics, it may identify a greater number of involved ARM nodes. These finding suggest that lymphatics from the ARM are not entirely independent. Prolonged diffusion times may cause the ICG to spread to additional axillary lymph nodes, which might increase the identification of involved ARM nodes [41]. Nevertheless, it is not necessary to preserve all ARM nodes because ARM lymph nodes and lymphatics are multiple. Ortega-Exposito et al. [41] divided patients into two cohort based on ICG migration patterns: standard technique (removal of all ARM nodes) and targeted technique (selective preservation of ARM nodes in contact with the axillary vein). With selective preservation of ARM nodes closest to the axillary vein (targeted technique), the incidence of involved ARM nodes and lymphatics can be significantly reduced from 47.1% with the standard technique to 15.7% with the targeted technique (p = 0.026) [41] (Table 3). Thus, it is important to preserve ARM nodes around the axillary vein to prevent arm lymphedema (Figure 3).
Several randomized clinical trials have been conducted to compare conventional ALND and ARM-guided ALND [24,25,27,28,29,30]. Yuan et al. [24] developed a modified ARM approach called iDEntification and Preservation of ARm lymphaTic system (DEPART). In this DEPART study, fluorescent dye (ICG) and methylene blue were used to identify the ARM nodes and lymphatics. A total of 874 cN+ patients and 480 SLN-positive patients were randomized into two groups: 648 patients underwent conventional ALND and 543 patients underwent ARM-guided ALND with preservation of ARM nodes and lymphatics. In the ARM-guided ALND group, ARM nodes and lymphatics were preserved unless they coincided with SLNs and palpable suspicious nodes. Palpable suspicious ARM nodes were histologically examined by partial frozen sections in 59 patients and involved ARM nodes were removed in 38 patients (38/558, 6.8%). More than 60% of tumors were hormone receptor-positive in either group. After surgery, regional nodal radiation was administered to 60.6% of the conventional ALND group and to 56.5% of the ARM-guided group, and patients in both groups received adjuvant chemotherapy. Within a median follow-up period of 37 months, arm lymphedema was observed in 99 patients (15.3%) in the conventional ALND group and in 18 patients (3.3%) from the ARM-guided ALND group (p < 0.001), but the incidence of axillary recurrence did not differ significantly between the two groups (1.4% vs. 1.2%) [24].
Given these findings, intraoperative nodal palpation must be regarded as an essential component rather than an optimal adjunct in ARM-guided ALND [42,43,44,45]. Moreover, postoperative radiotherapy is necessary for preventing axillary recurrence in high-risk patients after ARM-guided ALND. If it is not possible to spare fluorescent ARM lymphatics, these patients could be treated with lympho-lymphatic or lympho-venous anastomosis at the time of surgery to reduce a risk of arm lymphedema [46,47]. However, the follow-up duration was insufficient to evaluate axillary recurrence after ARM-guided ALND. Since the majority of breast cancer is hormone receptor-positive, which recurs over a longer period of time [48,49], a longer follow-up is needed to confirm the oncological feasibility of ARM-guided ALND.
5. Conclusions
TAS and ARM-guided ALND have been developed to reduce the incidence of arm lymphedema without increasing a risk of axillary recurrence. However, there have been concerns about the oncological feasibility of these procedures. TAS and ARM-guided ALND remained much less radical than conventional ALND. Nevertheless, postoperative radiotherapy may be effective for preventing axillary recurrence in patients with low-volume additional nodal disease. If palpably suspicious axillary lymph nodes are found during surgery, therefore, these nodes should be removed not only in TAS but also in ARM-guided ALND. However, since conservative axillary surgery lacks prospective studies with sufficient follow-up periods, it should be considered an investigational approach. Ultimately, we await the long-term results of prospective randomized clinical trials comparing TAS and ARM-guided ALND with conventional ALND to establish the oncological feasibility of these procedures. Ideally, direct comparative studies between TAS and ARM-guided ALND would be of great interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bakri N.A.C. Kwasnicki R.M. Khan N. Ghandour O. Lee A. Grant Y. Dawidziuk A. Darzi A. Ashrafian H. Leff D.R. Impact of axillary lymph node dissection and sentinel lymph node biopsy on upper limb morbidity in breast cancer patients. Systemic review and meta-analysis Ann. Surg.202327757258010.1097/SLA.000000000000567135946806 PMC 9994843 · doi ↗ · pubmed ↗
- 2Krag D.N. Weaver D.L. Alex L.C. Fairbank J.T. Surgical resection and radiolocalization of the sentinel lymph node in breast cancer using a gamma probe Surg. Oncol.1993233533910.1016/0960-7404(93)90064-68130940 · doi ↗ · pubmed ↗
- 3Giuliano A.E. Kirgan D.M. Guenther J.M. Morton D.L. Lymphatic mapping and sentinel lymphadenectomy for breast cancer Ann. Surg.199422039139810.1097/00000658-199409000-000158092905 PMC 1234400 · doi ↗ · pubmed ↗
- 4Krag D.N. Anderson S.J. Julian T.B. Brown A.M. Harlow S.P. Costantino J.P. Ashikaga T. Weaver D. Mamounas E.P. Jalove L.M. Sentinel –lymph-node resection compared with conventional axillary-lymph-node resection in clinically node-negative patients with breast cancer: Overall survival findings from the NSABP B-32 randomised phase 3 trial Lancet Oncol.20101192793310.1016/S 1470-2045(10)70207-220863759 PMC 3041644 · doi ↗ · pubmed ↗
- 5Veronesi U. Viale G. Paganelli G. Zurrida S. Luini A. Galimberti V. Veronesi P. Intra M. Maisonneuve P. Zucca F. Sentinel lymph node biopsy in breast cancer. Ten-year results of a randomized controlled study Ann. Surg.201025159560010.1097/SLA.0b 013e 3181 c 0e 92a 20195151 · doi ↗ · pubmed ↗
- 6Giuliano A.E. Mc Call L. Beitsch P. Whitworth P.W. Blumencranz P. Leitch A.M. Saha S. Hunt K.K. Morrow M. Ballman K. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases. The American College of Surgeons Oncology Group Z 0011 randomized trial Ann. Surg.201025242643210.1097/SLA.0b 013e 3181 f 08f 3220739842 PMC 5593421 · doi ↗ · pubmed ↗
- 7Donker M. van Tiernhoven G. Straver M.E. Meijnen P. van de Velde C.J.H. Mensel R.E. Cataliotti L. Westenberg A.H. Klinkenbijl J.H.G. Orzalesi L. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): A randomized, multicenter open-label, phase 3 non-inferiority trial Lancet Oncol.2014151303131010.1016/S 1470-2045(14)70460-725439688 PMC 4291166 · doi ↗ · pubmed ↗
- 8Mamtani A. Barrio A.V. King T.A. Van Zee K.J. Plitas G. Pilewskie M. El-Tamer M. Gemignani M.L. Heerdt A.S. Sclafani L.M. How often does neoadjuvant chemotherapy avoid axillary dissection in patients with histologically confirmed nodal metastases: Results of a prospective study Ann. Surg. Oncol.2016263467347410.1245/s 10434-016-5246-8PMC 507065127160528 · doi ↗ · pubmed ↗