West Nile Virus Lineage 2 Neuroinvasive Infection Presenting as Intraparenchimal Cerebral Hemorrage
Antonio Mastroianni, Simone Malagò, Valeria Vangeli, Giuliana Guadagnino, Luciana Chidichimo, Maria Vittoria Mauro, Francesca Greco, Robert Tenuta, Lavinia Berardelli, Antonio Mori, Sonia Greco, Concetta Castilletti

TL;DR
This study reports on nine adult cases of neuroinvasive West Nile virus infection in Italy, highlighting cerebral hemorrhage and other severe neurological complications.
Contribution
The paper presents new clinical and phylogenetic data on West Nile virus lineage 2 in Southern Italy, including rare manifestations like cerebral hemorrhage.
Findings
Nine WNDD cases showed severe neurological symptoms, including cerebral hemorrhage and Guillain–Barré syndrome.
Phylogenetic analysis grouped Italian WNV strains with Central–Southern–Eastern European sequences, distinct from northern Italian strains.
The study identified sub-lineage 2a of WNV-2, clustering mainly with Hungarian sequences.
Abstract
Objective: The aim of this retrospective study was to evaluate clinical and laboratory characteristics in adult patients with neuroinvasive West Nile virus (WNDD). We also studied the phylogeny and molecular characteristics of some of the WNV strains. Methods: A retrospective analysis was conducted at “Annunziata” Hub Hospital, a secondary referral facility in Calabria region, in Southern Italy. Sample pre-processing, sequencing and bioinformatic analyses were carried out at IRCCS Sacro Cuore Don Calabria Hospital in Negrar di Valpolicella, Verona, Veneto region in North-East Italy. Results: Nine cases of WNDD were analyzed, involving eight males and one female, with a mean age of 70.33 years (range 60–85). The overall average hospital stay was 20.6 days (range 6–46). Six patients made a full recovery after a mean of 35.3 days of acute care. Thirty-day mortality rate was 23%. VNDD in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
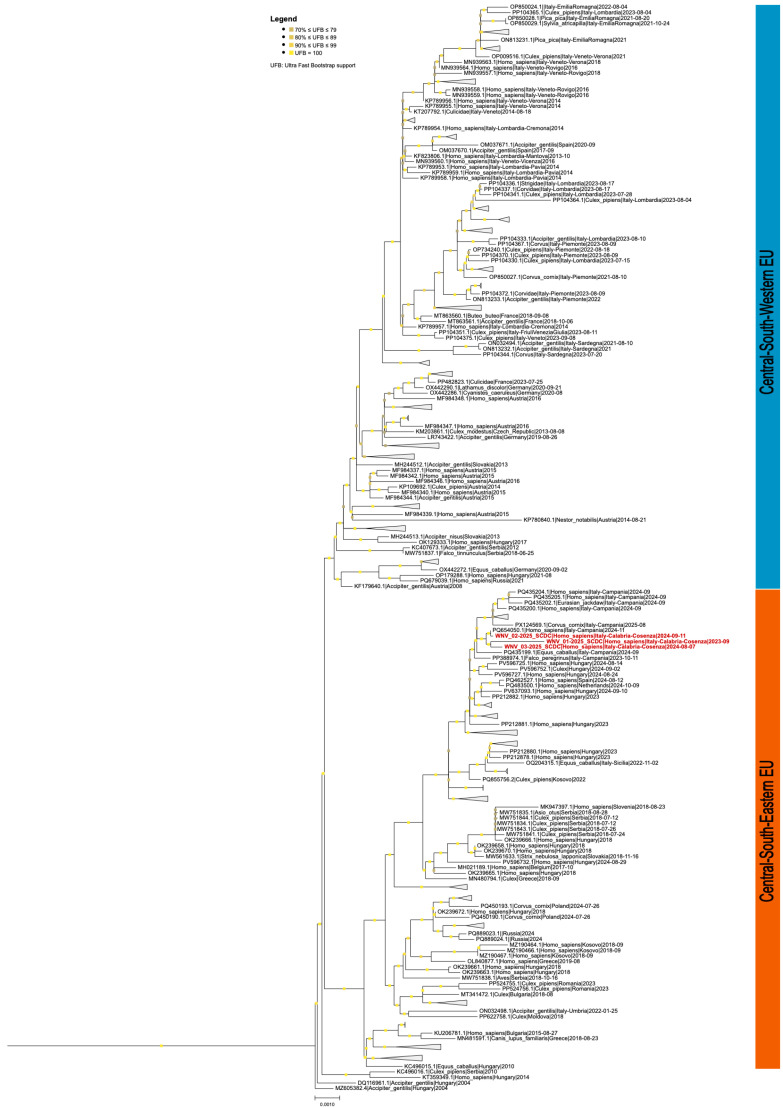 Figure 1
Figure 1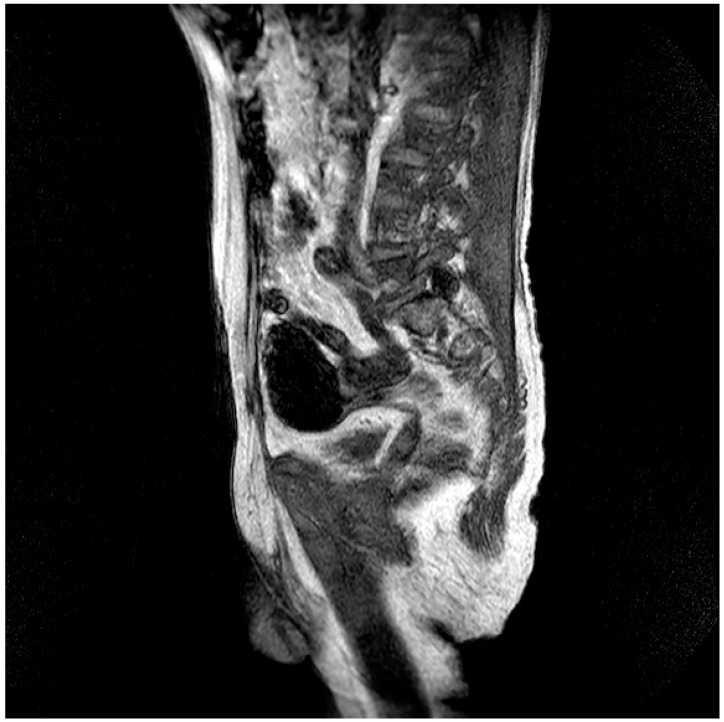 Figure 2
Figure 2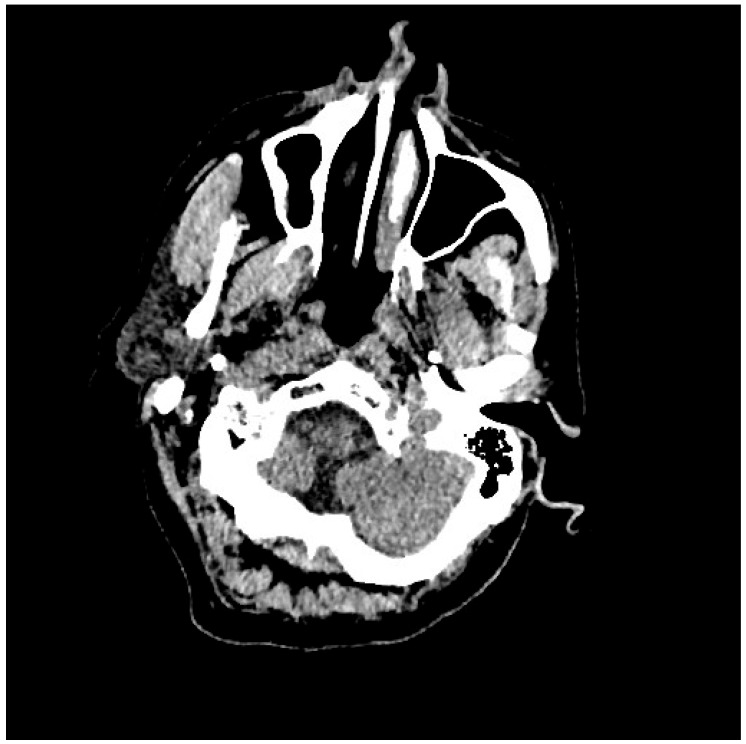 Figure 3
Figure 3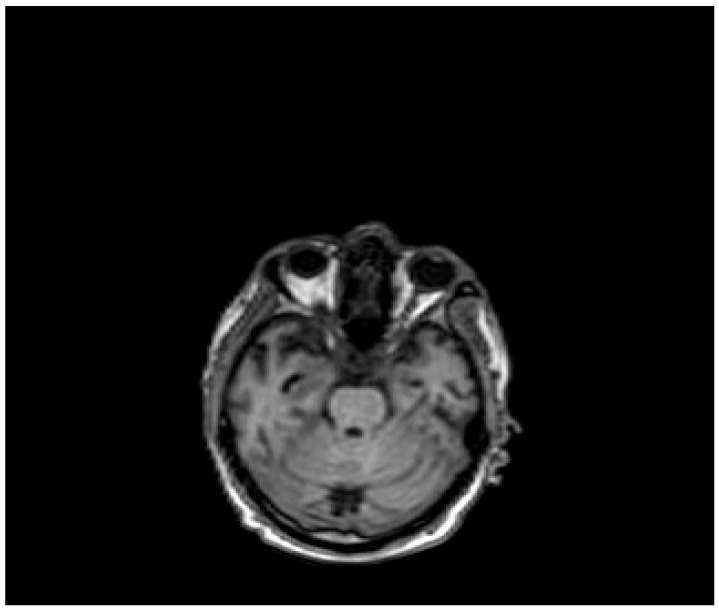 Figure 4
Figure 4| Patient (Pt), Sex, Age (Years, y) | Comorbidity | Symptoms | WNV Serology, IgG /IgM | Blood WNV Viremia, | Urinary WNV Viremia, | WNV CSF Viremia, Copies/mL | EEG | Head Tc | Head MRI | Treatment | Complications | Outcome (Days) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pt 1, F, 71, 2024 | HHD, dyslipidemia | Abdominal pain, fever, diarrhea, vomiting, headache | +/+ | <500 | 3028 | Neg | NR | UNR | NR | DEX | None | Cured, discharged after 16 d |
| Pt 2, M, 74, 2024 | HHD | High fever, confusion, disorientation, sensory clouding, headache | +/+ | Neg | Neg | Neg | Slowing of cerebral bioelectrical activity with additional bursts of spike waves over the left frontotemporal regions | Thin extraaxial hemorrhagic collections along the bilateral fronto-temporo-parietal convexities | Thin bilateral frontoparietal subdural hemorrhagic layers | DEX, Igs | Left hemiparesis, progressively worsening coma | Exitus, 21 days after hospital admission |
| Pt 3, M, 60,2024 | None | High fever, headache, confusion | −/+ | 67.067 | Neg | >50,000,000 | NR | UNR | Weak cerebellar leptomeningeal venular enhancement | DEX, Igs | None | Cured, discharged after 21 d |
| Pt 4, M, 75, 2024 | CVE, H | High fever, headache, confusion, dysarthria | +/+ | Neg | Neg | Neg | NR | UNR | CVE, cerebral atrophy | DEX, Igs | None | Cured, discharged after 9 d |
| Pt 5, M, 63, 2023 | DM2, CHHD | In the days preceding hospital admission he had suffered; upon arrival at the emergency room he was found to be in a coma (Glasgow Coma Scale 6), with severe weakness of the limbs and high fever | +/+ | Neg | Neg | <500 | Delta waves spread mainly over the anterior regions | UNR | Hyperintensity in the middle cerebellar peduncles, the splenium of the corpus callosum, | DEX, Igs, plasmapheresis | Global clinical worsening with irreversible tetraparesis and mechanical ventilation through tracheostomy | Transferred to a rehabilitation facility 46 days after hospital admission. Exitus after 3 week because of respiratory failure. |
| Pt 6, M, 84, 2024 | Previous right nephrectomy for cancer, prostate cancer undergoing radiotherapy | High fever, headache, confusion | +/+ | 842.845 | 9454 | Neg | Slowing of cerebral bioelectrical activity | UNR | UNR | DEX, Igs | None | Cured, discharged after 6 d |
| Pt 7, M, 71, 2025 | HHD, cognitive involutional syndrome | High fever, headache, confusion, worsening motor difficulty with lower limb weakness | +/+ | Neg | Neg | Neg | ICH of the occipital horns of the lateral ventricles ( | Diffuse meningoencephalitis, with involvement of the cauda extremity roots. | DEX, Igs | Gradual clinical improvement, however lower limb weakness persisted | Transferred to a rehabilitation facility 34 days after hospital admission. | |
| Pt 8, M, 66, 2025 | DM2, CHHD, CVE | High fever, vomiting, peripheral paresis of the VII right cranial nerve | +/+ | Neg | Neg | Neg | Mild diffuse encephalic suffering with slowed background electrical activity and bursts of generalized slow activity | CVE | CVE | DEX, Igs | None | Cured, discharged after 20 d |
| Pt 9, M, 68, 2025 | DM2, | High fever, soporific state, poor verbal, tactile and pain reactivity | +/+ | Neg | Neg | 1072 | Slow activity in the theta and delta bands, low voltage, | Bilateral frontal lobe subdural hemorrage, ICH in the right frontotemporal lobe | NR | DEX, Igs | Overall worsening of clinical conditions and comatose state | Exitus, 13 d after hospital admission |
| References, Country, Type of Article | Age (y), Sex | Comorbidity | Clinical Features | Head CT | EMG | Head MRI | Clinical Diagnosis | Autopsy Findings | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| Smith R.D. et al. [ | 43, M | Renal allograft, end-stage | A 2-day history of nausea, vomiting, diarrhea, and chills | Bilateral thalamic edema extending to the midbrain and | NR | Extensive edema involving the pons, | A severe, bilateral, necrotizing and hemorrhagic encephalitis | Acyclovir | Died | |
| Whitney E.A. et al. [ | 68, F | Recurrent transient | High fever, | Non-revealing | NR | Unremarkable | Community-acquired pneumonia, atrial fibrillation, | Oral antibiotics, carbamazepine. | Discharged on the 7th day | |
| Peters S. & Brown K. [ | 57, M | None | Pharyngitis and a descending | “T” occlusion of the distal left internal carotid artery | NR | Patchy infarction in the left insula, basal ganglia, and | Acute cryptogenic stroke | Intravenous thrombolysis, | Discharged with no residual neurologic deficits and no recurrence after two | |
| Kulstad E.B., Wichter M.D. [ | 70, M | Chronic lymphocytic leukemia | Mental confusion, | Mild atrophy consistent with | NR | Mild chronic ischemic demyelination | Stroke | Oxygen, fluid hydration, | Death | |
| Alexander J.J. et al. [ | 9, F | Environmental exposure to mosquitoes | Intermittent right arm and leg weakness. She fell from her bicycle and developed | A small hypodense area in the left anterior temporal lobe | NR | Increased T 2- | Stroke Associated With Central Nervous System | She was initially treated with hydration, low-dose | Discharged. Clinical | |
| Castaldo N. et al. [ | 57, M | Autoimmune glomerulonephritis in immunosuppressive treatment | Fever, confusion, diplopia, opsoclonus, multifocal myoclonus and generalized tremor | Massive intraparenchymal hemorrhage, fourth ventricle compression and tonsillar herniation | Slow bilateral diffuse slow waves | Unremarkable | Rhombencephalitis, | Macroscopic examination of the brain showed diffuse malacia | Empirical therapy with ampicillin, ceftriaxone, acyclovir and dexamethasone. Therefore, IVIGs and steroids | Died 5 days after admission |
| Jacob S. et al. [ | 67, F | None. Significant history of pigeon exposure | Right-sided facial droop, right-sided weakness, low back pain, fever and lethargy | Unremarkable | N.A. | Medial left frontal acute infarct | Stroke with encephalopathy | IVIG | Her | |
| Harroud A. et al. [ | 73, F | A remote history of renal cell and breast carcinomas, both in complete remission and no | Confusion, high fever; decreased level of | Unremarkable | Severe slowing but no epileptic activity | Extensive | Encephalitis with | Supportive treatment including neurointensive | On discharge, the | |
| Hingorani K. et al. [ | 70, F | None | Depressed level of consciousness, | Bilateral corona radiata strokes | Mild generalized delta slowing | Bilateral corona radiata strokes | Stroke | NR | Discharged | |
| Tangella N et al. [ | 74, M | ESRD, T2DM, | 3–4 days of nausea, vomiting, diarrhea, fever and chills | NR | Diffuse | Acute ischemic stroke and SAH | NR | Empiric meningitis treatment. Therefore, | NR | |
| Lowe L.H. et al. [ | 7, F | None | Headache, right hemiparesis, | Unremarkable | NR | Acute left middle cerebral artery | Primary cerebral vasculitis | Aspirin, steroids, cyclophosphamide | Discharged, without recurrent stroke after 36 months | |
| Lowe L.H. et al. [ | 12, F | None | Headache, slurred speech, | Abnormality in the left | NR | Abnormality in the left | Primary cerebral vasculitis | Aspirin, steroids, | Discharged, without recurrent stroke | |
| Lowe L.H. et al. [ | 9, F | None | Headache, | Acute left middle | NR | Acute left middle | Primary cerebral vasculitis | Aspirin, steroids, and cyclophosphamide | Discharged, without recurrent stroke |
| References, Country, Type of Article | Age (y), Sex | Comorbidity | Clinical Features | CT Scan of the Brain | EMG | MRI of the Brain/Spine | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|
| Ashkin A. et al., 2023 [ | 67, M | CAD, hyperlipidemia | Fever, nausea, vomiting, and right lower quadrant abdominal pain | NA | Nonrecordable nerve conduction velocity in bilateral peroneal nerve, a slowing of the right tibial nerve conduction velocity | Not remarkable | 3-day course of IVIG, 1 g of methylprednisolone daily for of 5 days | Residual lower extremity weakness |
| Sciturro M. et al., 2022 [ | 64, M | Asthma, diverticulitis, | Generalized bilateral upper and lower extremity | NA | NA | Not remarkable | IVIG and plasmapheresis, with no improvement | Died |
| Beshai R. et al., 2020 [ | 65, F | NA | Progressive ascending paralysis | Normal | Acute sensorimotor axonal and demyelinating peripheral neuropathy | NA | 10-day course of IVIG | Improved, but lower extremity weakness unchanged |
| Paphitou N.I. et al. [ | 75, M | CAD, prostate cancer | Reduced muscle strength | Not remarkable | Nonspecific findings of peripheral neuropathy | Not remarkable | 5-day course of IVIG | Recovered |
| Walid M.S. et al., 2009 [ | 55, M | Diabetes mellitus, hypothyroidism | Muscle weakness | Not remarkable | Sensorimotor mixed polyneuropa- | Not remarkable | Plasma- | Recovered |
| Sejvar J.J. et al., 2006 [ | 4 pts | NA | Ascending weakness with | NA | Demyelinating sensorimotor neuropathy | NA | NA | 1 pt lost to follow-up. |
| Ahmed S. et al., 2000 [ | 69, M | Hypertension | Progressive weakness, quadriparesis | Not remarkable | Demyelinating polyneuritis with secondary motor axon | Not remarkable | 5 cycles of plasmapheresis with no improvement; 2 courses of IVIG, with only minimal improvement | Transferred to a nursing home with a tracheostomy and a |
| Joseph N. et al., 2019 [ | 40, M | Hypertension | Progressive muscle | NA | Demyelinating sensorimotor polyneuropathy | NA | 5-day course of IVIG | Recovered |
| Abraham A. et al., 2011 [ | 67, F | None | Shoulder and back pain, generalized | Occipital lobes hypodensities | Demyelinating polyneuropathy | PRES | 5-day course of | Recovered |
| References (First Author, Year, Country) | Age (Years, y), Sex | Medical History | Clinical Features | Cranial Nerves | Treatment | Outcome |
|---|---|---|---|---|---|---|
| Flaherty M.S. et al., 2003 [ | 34, M | CD | Non-specific viral illness, tinnitus, facial palsy | VII, XI | Systemic antibiotics | Partial recovery |
| Rosenheck M.L. et al., 2022 [ | 40, F | CD | Facial palsy, | VII | Systemic antivirals, steroids and antibiotics | Cured |
| EL-Dokla A.M. et al., 2018 [ | 48, M | NA | Facial palsy, weakness in extremities | VII | Systemic antivirals snd steroids | Cured |
| EL-Dokla A.M. et al., 2018 [ | 49, F | NA | Non-specific viral illness, | VII | Systemic antivirals and steroids | Cured |
| Sejvar J.J. et al., 2003 [ | 57, M | CD | Facial palsy | VII | Supportive therapy | No recovery |
| Li J. et al., 2003 [ | 45, M | Healthy | Facial palsy | VII | Immunoglobulins | No recovery |
| Li J. et al., 2003 [ | 27, M | CD | Non-specific viral illness, facial palsy, | VII, XI | NA | No recovery |
| Al-Hashimi I. et al., 2024 [ | 68, F | CD | Non-specific viral illness, facial palsy, | II, VII, XI | Systemic antivirals and antibiotics | Cured |
| Cunha B.A. et al., 2006 [ | 47, M | NA | Vision problems | VI, VII | NA | Cured |
| Nikolic N. et al., 2024 [ | 65, F | CD | Non-specific viral illness, | VII | Systemic antivirals and antibiotics | Cured |
| Ostapchuk Y.O. et al., 2020 [ | 28, M | NA | Non-specific viral illness, | VII | Supportive therapy | Cured |
| Ostapchuk Y.O. et al., 2020 [ | 19, F | NA | Non-specific viral illness, facial palsy, | VII | Systemic antivirals and | Cured |
| Jhunjhunwala K. et al., 2018 [ | 28, F | Healthy | Non-specific viral illness, facial palsy, | VII | Systemic antibiotics | Cured |
| This case series | 66, M | CD | High fever, vomiting, peripheral paresis of the VII right cranial nerve | VII | Steroids, Igs | Cured |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMosquito-borne diseases and control · Vector-borne infectious diseases · Viral Infections and Vectors
1. Introduction
Most West Nile Virus (WNV) infections are asymptomatic, mild, or undiagnosed; however, severe cases of WNV neuroinvasive disease (WNND) are incresingly reported, probably related to WNV’s specific affinity for the nervous system, both central and peripheral. West Nile encephalitis (WNE) presents as severe neuroinvasive disease after a flu-like prodrome, featuring rapid progression to neurological issues, like acute flaccid paralysis, movement disorders, altered mental status, seizures, and neck stiffness, affecting under 1% of WNV-infected individuals [1].
WNE involves brain inflammation, but it can also trigger cerebrovascular issues like vasculitis and strokes, both ischemic and/or hemorrhagic, making it mimic a stroke or cause stroke-like symptoms. This neuroinvasive form (<1% of cases) damages blood vessels, leading to these serious complications, even causing intracranial cerebral hemorrage (ICH), expanding the range of severe WNV neurological impacts beyond typical clinical features [2].
ICH is a leading cause of death worldwide and an important health issue. Although common causes predominantly affect the elderly, there exists a spectrum of uncommon etiologies that contribute to the overall incidence of ICH [3].
Infectious causes of ICH may involve organisms like bacteria (Streptococcus pneumoniae, Treponema pallidum), viruses (HIV, VZV, HSV, COVID-19), fungi (Aspergillus, Cryptococcus), and parasites, leading to inflammation (vasculitis), ruptured aneurysms, or clotting issues (coagulopathy) that damage blood vessels, causing them to leak or burst, as seen in tuberculous meningitis, endocarditis, or invasive fungal infections [3].
During the summer of 2025, we consecutively followed two patients with WNE complicated by ICE (Table 1, patient 7 and 9), among other patients. This occurrence raised our clinical suspicion of a potential correlation between WNE and the risk of ICH, also considering a case of WNE complicated by ICH observed in 2024 (Table 1, patient 2). For this reason, we decided to reevaluate the clinical features of the WNE cases observed in our department and compare our results with an extensive literature review.
2. Methods
We conducted a descriptive study of cases of WNDD occurred between 2023 and 2025 in the province of Cosenza, which covers a large territory in Calabria, a region of Southern Italy, in order to evaluate unusual clinical presentations. Nine cases of WNND were analyzed, involving 8 males and 1 female, with a mean age of 70.33 years (range 60–85) (Table 1). WNE was confirmed by the demonstration of specific IgM and IgG antibodies in serum using routine serological screening tests.
Laboratory diagnosis of WNDD was carried out at the “Annunziata” Hub Hospital, Cosenza. Cerebrospinal fluid (CSF) and blood sample were analyzed for WNV infection using the one-step real time RT-PCR (kit WNV ELITe MGB® Kit (ELITechGroup SAS, Puteaux, France), following the manufacturer’s instructions. All patients had specific IgM antibodies at admission and IgG antibodies were present in 90%.
We investigated the phylogeny and molecular characteristics on the complete genome sequence of the GBS case, identified in September 2023 (WNV-2-Cal/2023), as well as the complete genome sequences of two of the patient with ICH ascociated WNE in August 2024.
The analysis included sequences from the GenBank database, ranging from the first European/African sequences deposited up to September 2025. The majority of sequences originate from Italy (n = 124), Greece (n = 112), Germany (n = 99), Russia (n = 87), and Hungary (n = 76), primarily associated with mosquito (~36%), humans (~29%), and birds (~27%) hosts.
Sample pre-processing, sequencing and bioinformatic analyses were carried out at IRCCS Sacro Cuore Don Calabria hospital in Negrar di Valpolicella, Verona. All the analyses were performed on the same whole blood samples used for the laboratory diagnosis.
The whole blood samples’ nucleic acid content was extracted via Qiagen EZ1 Advanced XL, with the EZ1 ^®^ DSP Virus kit, from 200 uL into 60 uL (Qiagen, Hilden, Germany). RNA was quantified using the Qubit RNA HS assay kit (Invitrogen, Thermo Fisher Scientific, Inc., Waltham, MA, USA) and the High Sensitivity RNA ScreenTape on the 4200 TapeStation System (Agilent Technologies Inc., Santa Clara, CA, USA).
Full-length WNV genome sequences were obtained using two different approaches: (i) the Illumina RNA prep kit with enrichment, with Viral Surveillance Panel (VSP) hybridization capture probes (Illumina, San Diego, CA, USA), following the manufacturer’s instructions; and (ii) a panel of tiled amplicons of 400 bp in length. Amplicons underwent Illumina DNA prep kit processing, as per manufacturer instructions. Libraries were loaded on Illumina P1 flow cells (Illumina, San Diego, CA, USA), running 2 × 150 bp, on a NextSeq1k. Each library was evaluated via qubit DNA HS and High Sensitivity DNA ScreenTape 5000 prior to loading on the appropriate flow cell.
3. Results
The overall average hospital stay was 20.6 days (range, 6–46). Six patients made a full recovery with no neurological sequelae after a mean of 35.3 days of acute care. Thirty-day mortality rate was 23%.
Three male patients with a median age of 71 years (range 68–74), presented ICH associated with WNE (Table 1, patient 2, 7, 9). Two male patients, the first 74-year-old (Table 1, patient 2) suffering from arterial hypertension and the second 68-year-old (Table 1, patient 9) suffering from diabetes mellitus and post-ischemic dilated heart disease, died after 13 and 21 days, while the third patient (Table 1, patient 7) was transferred to a neuromotor rehabilitation facility after 34 days of hospitalization. This patient, before admission to the hospital, presented age-related brain involution symptoms and suffered from chronic hypertensive heart disease. The reasons for admission to the emergency room were worsening motor difficulties with weakness in the lower limbs, a rapidly worsening state of confusion, high fever, and an episode of hypertensive peak. Repeated studies of the brain and spinal cord, using computed tomography (CT) scans and magnetic resonance imaging (MRI), have documented a very complex picture, characterized by diffuse meningoencephalitis, with a diffuse flogistic involvement of the pachy-leptomeninges and the equine cauda roots, blood deposits in the occipitopolar and bihemispheric mid-posterior cingulate sulci, the left temporoparietal carrefour, the fourth ventricle and occipital horns and the pericerebellar cistern. There was also evidence of a diffuse posterior dorso-lumbo-sacral, anterior dorso-lumbar (up to L1) and sacral spinal cord epidural hematoma. Diffuse hemosiderin coating was present on the dural surface in the dorso-distal posterior lumbo-sacral and anterior lumbo-sacral regions, as well as at the anterior 8th-10th level. Serology for WNV was positive, while WNV RNA testing in CSF, blood, and urine was negative. Treatment included two 5-day cycles of high-dose immunoglobulins and the use of dexamethasone (Table 1, patient 7).
The second patient was a 68-year-old man with diabetes mellitus and post-ischemic dilated heart disease, admitted to the emergency room for a syncope in absence of cardiac arrhythmias (Table 1, patient 9).
The patient appeared drowsy, but initially arousable. A spinal tap was not performed urgently due to concomitant aspirin therapy. A brain CT scan documented an increase in the volume of the subarachnoid spaces of the vault and skull base, thin, hygromatous subdural hypodense layers in the bilateral frontal lobe, and a blood hyperdensity within the right subdural collection in the right frontotemporal parietal lobe. An EEG revealed slow background activity in the theta and delta bands, with low voltage, and slightly asymmetric (right greater than left). Serology for WNV was positive and urine WNV-RNA testing was positive with a titer of 1072 copies/mL The patient received both high-dose immunoglobulin for seven days and dexamethasone, but his clinical condition did not change, resulting in death 13 days after hospital admission.
The third patient was a 74-year-old male (Table 1, patient 2) suffering from hypertensive heart disease, hospitalized for high fever, worsening spatial-temporal disorientation and mental confusion, associated with dysarthria. There was evidence of a left upper limb paresis. An EEG revealed a widespread slowing of brain bioelectrical activity to 4–5 c/s, interspersed with additional bursts of spike waves over the left frontotemporal regions, which spread to the contralateral hemisphere. Both a CT scan and a brain MRI documented subdural hygromatous collections along the bilateral fronto-temporo-parietal convexities. Despite treatment with high-dose immunoglobulin for 5 days and dexamethasone, the clinical conditions worsened, resulting in death 21 days after hospital admission. Four patients (Table 1, patient 3, 4, 5, 6) presented with moderate severity of WNE, responded positively to treatment with immunoglobulins and dexamethasone and were discharged with complete recovery.
In our small cohort, we observed two other cases of patients with an unusual presentation. A 66-year-old male patient presented with severe right Bell’s palsy, which gradually regressed over approximately two months. This patient was treated with both steroids and immunoglobulins, leaving no neurological deficits and without relapse at the six-month follow-up. Steroid treatment was continued with tapering doses for approximately six weeks. This is the first patient with WNV-related facial palsy to be treated simultaneously with steroids and immunoglobulins, with a complete clinical response.
A 63-year-old man (Table 1, patient 5) developed a fulminant Guillain–Barré syndrome (GBS) responsible for a severe tetraparesis and a respiratory failure, requiring a tracheostomy and intubation. He was transferred to a rehabilitation long-term care facility 46 days after hospital admission, but he died after approximately two months, because of severe respiratory complications.
Phylogenetic analysis showed that the WNVIRCCS-SCDC_01/2025 strain (WNV2-Cal/2023) and the other two strains analyzed belonged to the sub-lineage 2a of the WNV-2, clustering with sequences from the Central–South–Eastern clade (Figure 1). The neighboring branches reported sequences from the Southern and Eastern Europe, such as Greece, Hungary, Serbia, Russia, Romania, Slovakia, Poland and Kosovo. In particular, the most closely related sequences could be traced back mainly the WNV Hungary 578/10 strain (GenBank accession ID KC496015.1). The polyprotein sequence analysis of the WNV-2 strains from Calabria region identified non-synonymous substitutions that were representative signatures in the genome-based phylogenetic analysis of Hungarian clade of WNV-2 Central–South–Eastern cluster. In particular, the WNV-2 genomes detected in the Calabria region were characterized by amino acid residues (NS2B-V119I, NS3-H249P, NS4B-S14G, and NS4B-T49A) that were not present in other sequences of the Central–North–Western Europe (including them from NC–Italy). These observed residues were shared with the Central–South–Eastern European WNV reference strain (Hungary 578/10), isolated in 2010 (NS2B-119I, NS3-249P, NS4B-14G, and NS4B-49A). Moreover, among these substitutions, the Proline at NS3-249 was previously associated with higher neuro-virulence.
Phylogenetic analysis of WNV lineage 2 whole-genome sequences. In this sub-selection only European sequences were included. Red-colored labels refer to clinical cases collected at out hospital. Colored bars on the right delineate the separation between Central–Western European (blue) and Central–Southern–Eastern (red) sequences. Bootstrap values are reported where ≥90. The original tree comprises European and African sequences from the first deposited whole-genome sequence up to August 2025. For visualization constraint, clades that contain either multiple records of the same country or low bootstrap values were collapsed. To inspect the full phylogenetic tree see microreact.
Evidence of an extensive epidural spinal cord hematoma on spinal MRI (Table 1, patient 7).
Evidence of ICH on brain CT scan (Table 1, patient 7).
Evidence of ICH on brain MRI (Table 1, patient 7).
4. Discussion
A comprehensive search was conducted across the PubMed, Scopus, Web of Science, and Embase databases to extract relevant published data existing about ICH and WNE, up to November 2025. This retrospective analysis reveled only three reported cases of ICH in WNE patients (Table 2).
A case of severe, bilateral necrotizing and hemorrhagic encephalitis was reported in a 43-year-old man, undergoing mycophenolate mofetil therapy for a renal transplant due to diabetes mellitus. He died 12 days after hospital admission. Autopsy revealed predominantly inflammatory involvement of motor neurons and a positive immunohistochemical staining for WNv antigen [4].
Castaldo N et al. [5] documented in 2020 a 57-year-old male patient suffering from autoimmune glomerulopathy, treated with immunosuppressive therapy, with rhombencephalitis and massive intraparenchymal hemorrhage, fourth ventricle compression and tonsillar herniation. He died 5 days after admission [4].
Harroud A. et al. [2] described a 73-year-old female patient with lymphocytic encephalitis and subarachnoid hemorrhage. She was treated with supportive care and he was discharged in improved clinical condition, able to walk without support, but with chronic cognitive deficits.
Our review highlighted nine cases of ischemic and hemorragic stroke associated with WNV infection reported in the literature [6,7,8,9,10,11,12,13] (Table 2).
Seven patients were female and two were male, with a median age of 49.22 years (range, 7–74). The outcome was favorable, being all but one patient discharged, with no residual neurological findings and no recurrences in subsequent follow-up. Only one patient died due to severe acute respiratory failure during the ICU stay. Comorbidities were varied; only one of these patients had a confirmed history of recurrent cerebral ischemic episodes. Tangella N et al. reported a case of acute ischemic stroke and subaracnoid hemorrage (SAH) [12], while Lowe LH et al. [7] described three pediatric cases of primary idiopathic cerebral vasculitis complicated by stroke. These cases were observed in three girls aged 7, 9, and 12 years and were followed by complete recovery with a regimen of aspirin, steroids, and cyclophosphamide. In all three of these children, during follow-up to 36 months, 19 months, and 18 months, respectively, no recurrence of stroke was detected, and the neurological condition was stable [7].
A recent systematic review [14] of case reports on WNV infection-associated cranial nerve (CN) neuropathy reported 13 cases of facial palsy related to WNV infection. Thus, facial palsy represented 31.0% of 42 cases of cranial nerve neuropathies as an outcome of WNV infection, reported in 30 case reports. The mean time until onset of signs and symptoms of facial palsy was 1–16 days [14].
Complete recovery was significantly associated with absence of comorbidities, while it is difficult to establish the role of the use of antivirals, steroids and antibiotics, variously used in combination without a precise criterion. However, it is also true that three male patients aged 57, 45, and 27 who did not receive antivirals did not achieve resolution of facial palsy. Furthermore, a 34-year-old man with involvement of the VII and XI cranial nerves, treated with antibiotics, achieved only partial improvement.
A 63-year-old man developed a GBS unresponsive to steroids, immunoglobulins and plasmapheresis. This patient died after approximately two months after hospital admission because of severe respiratory complications.
WNDD presenting as GBS or Guillain–Barré-like syndrome (GBLS) has been increasingly reported [15,16,17,18,19,20,21,22,23,24] (Table 3 and Table 4).
A polio-like syndrome with paralysis involving one (monoparesis) to four limbs (tetraparesis), with or without brainstem involvement and respiratory failure, has been described. This syndrome of acute flaccid paralysis may occur without overt fever or meningoencephalitis. Although involvement of the anterior horn cells of the spinal cord and motor neurons of the brainstem are the main sites of pathology responsible for neuromuscular signs, inflammation may also involve the skeletal and/or cardiac musculoskeletal system (myositis, myocarditis), motor axons (polyradiculitis), and peripheral nerves (GBS), or present as brachial plexopathy. Furthermore, involvement of spinal sympathetic neurons and ganglia provides an explanation for the autonomic instability observed in some patients. Many patients also experience prolonged subjective generalized weakness and disabling fatigue. The long-term outcome of WNE polio-like syndrome appears to be more heterogeneous than preliminary data may have suggested, with some patients showing little neurologic and functional improvement and others showing substantial improvement. The degree of initial weakness appears to be a predictor of subsequent long-term outcome. The Centers for Disease Control and Prevention (CDCs) report that 13% of WNV infections manifest as GBS [25].
In most of the cases reported from the current literature through a PUBMED/MEDLINE search summarized in Table 4, gradual and slow improvement occurred, often with residual neurologic deficits of varying severity. Treatment includes supportive care and consideration of the use of intravenous immunoglobulin and, if unsuccessful, plasmapheresis [15,16,17,18,19,20,21,22,23,24,25].
5. Conclusions
Preliminary data do not allow us to determine whether our strains presented an increased neurovirulence, potentially attributable to some amino acid substitutions located in the Envelope protein. However, additional investigations and data consolidation are necessary to clarify this point. Most WNV infections are asymptomatic, mild, or undiagnosed; however, severe cases of WNDD are increasingly reported, probably related to WNV’s specific affinity for the nervous system, both central and peripheral. WNV infection can rarely cause cerebral vasculitis, a serious inflammation of brain blood vessels, leading to complications like ischemic or hemorrhagic stroke and severe neurological issues [2]. This viral vasculitis may involve direct viral infection of endothelial cells, causing vessel damage, rupture, and subsequent bleeding or blockage. Clinicians should suspect WNE in ischemic and hemorragic stroke cases during summer and mosquito season, especially with cerebral hemorrhagic signs. We suggest that clinicians should be vigilant for vasculitic complications in WNE patients, including ICH.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Solomon T. Ooi M.H. Beasley D.W. Mallewa M. West Nile encephalitis BMJ 200332686586910.1136/bmj.326.7394.86512702624 PMC 1125772 · doi ↗ · pubmed ↗
- 2Harroud A. Almutlaq A. Pellerin D. Paz D. Linnell G.J. Gendron D. West Nile virus-associated vasculitis and intracranial hemorrhage Neurol. Neuroimmunol. Neuroinflamm.20197 e 64110.1212/NXI.000000000000064131757817 PMC 6935842 · doi ↗ · pubmed ↗
- 3Chutinet A. Charnnarong C. Suwanwela N.C. Stroke from Infection Cerebrovasc. Dis. Extra.20251511812910.1159/00054498640068656 PMC 12237291 · doi ↗ · pubmed ↗
- 4Smith R.D. Konoplev S. De Courten-Myers G. Brown T. West Nile virus encephalitis with myositis and orchitis Hum. Pathol.20043525425810.1016/j.humpath.2003.09.00714991545 · doi ↗ · pubmed ↗
- 5Castaldo N. Graziano E. Peghin M. Gallo T. D’Agaro P. Sartor A. Bove T. Cocconi R. Merlino G. Bassetti M. Neuroinvasive West Nile Infection with an Unusual Clinical Presentation: A Single-Center Case Series Trop. Med. Infect. Dis.2020513810.3390/tropicalmed 503013832878269 PMC 7558676 · doi ↗ · pubmed ↗
- 6Kulstad E.B. Wichter M.D. West Nile encephalitis presenting as a stroke Ann. Emerg. Med.20034128310.1067/mem.2003.6712572565 · doi ↗ · pubmed ↗
- 7Lowe L.H. Morello F.P. Jackson M.A. Lasky A. Application of transcranial Doppler sonography in children with acute neurologic events due to primary cerebral and West Nile vasculitis AJNR Am. J. Neuroradiol.2005261698170116091517 PMC 7975159 · pubmed ↗
- 8Whitney E.A. Heilpern K.L. Woods C.W. Bahn C.C. Franko E.A. Del Rio C. Silk B.J. Ratcliff J.J. Bryant K.A. Park M.M. West Nile virus among hospitalized, febrile patients: A case for expanding diagnostic testing Vector Borne Zoonotic Dis.20066424910.1089/vbz.2006.6.4216584326 · doi ↗ · pubmed ↗