Pancreatic Head Cancer Masquerading as Distal Cholangiocarcinoma: Diagnostic Challenges, Tumor Characteristics, and Oncologic Outcomes
Kenta Aso, Ryuji Yoshioka, Atsushi Takahashi, Shoichi Irie, Yoshinori Takeda, Yoshihiro Hirata, Takaaki Kato, Hirofumi Ichida, Yoshihito Kotera, Yoshihiro Mise, Yuki Fukumura, Akio Saiura

TL;DR
This study shows that some pancreatic cancers initially mistaken for bile duct cancer have better survival rates, suggesting they may be a less aggressive type.
Contribution
The study identifies a potentially less aggressive subtype of pancreatic cancer that mimics distal cholangiocarcinoma.
Findings
Patients with pancreatic cancer misdiagnosed as bile duct cancer had survival rates comparable to typical pancreatic cancer cases.
These misdiagnosed pancreatic cancers were associated with better overall survival in multivariable analysis.
The findings suggest a need for improved diagnostic methods to distinguish these cancers preoperatively.
Abstract
Accurately distinguishing between pancreatic head cancer and distal cholangiocarcinoma before surgery is difficult because they occur in the same area and share similar symptoms. This distinction is critical because treatment plans differ, especially regarding the use of neoadjuvant chemotherapy before surgery. Our study analyzed patients who were initially thought to have distal cholangiocarcinoma but were later diagnosed with pancreatic head cancer after surgery. We found that although these cases often required more complex surgery, the patients had comparatively better survival outcomes than those typical for pancreatic head cancer. This suggests that pancreatic cancers that mimic distal cholangiocarcinoma might be a biologically less aggressive subtype. These findings highlight the need for better diagnostic methods to ensure each patient receives the most effective treatment plan…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
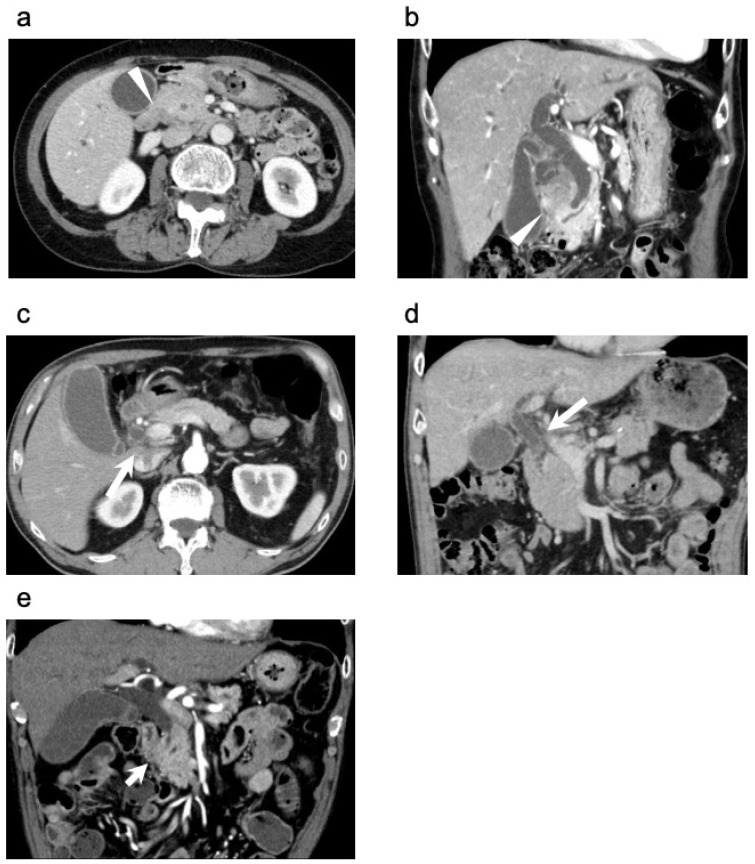 Figure 1
Figure 1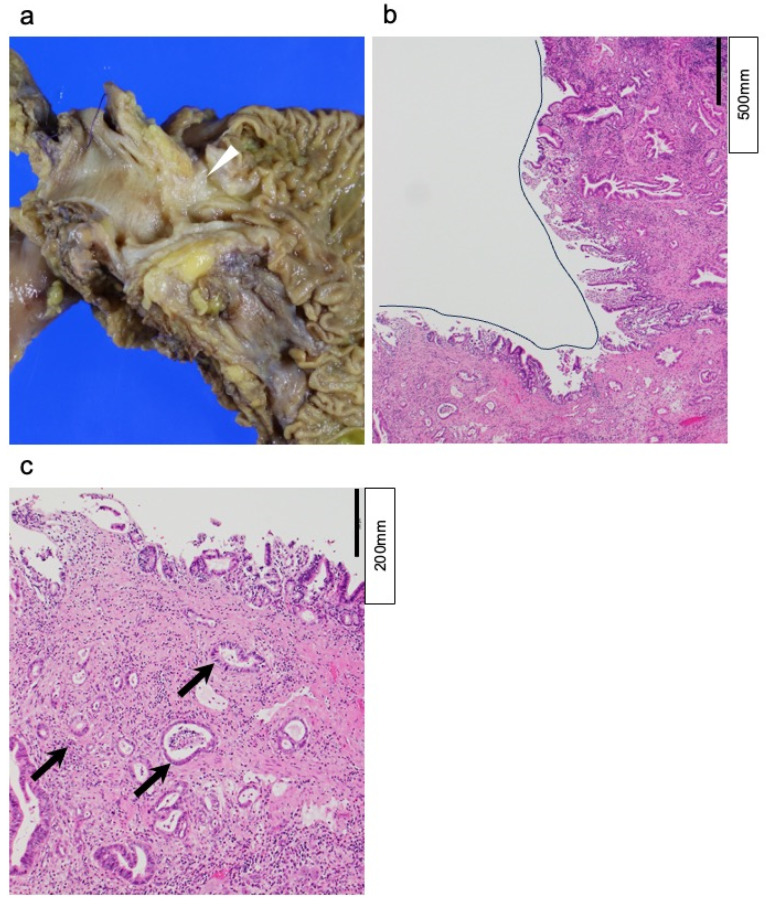 Figure 2
Figure 2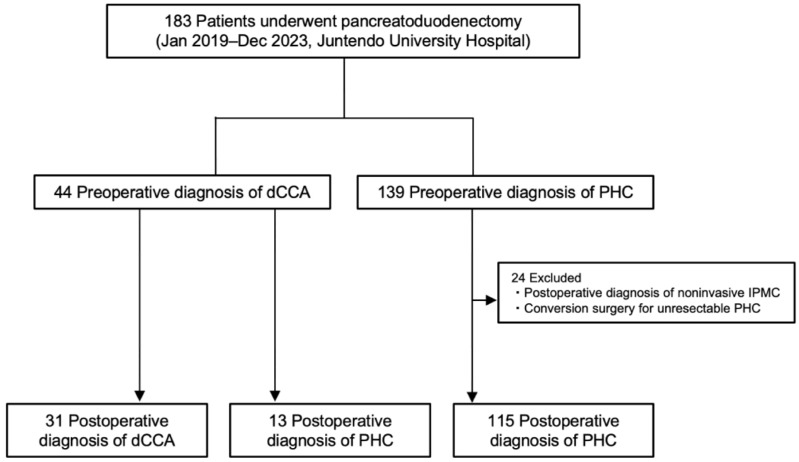 Figure 3
Figure 3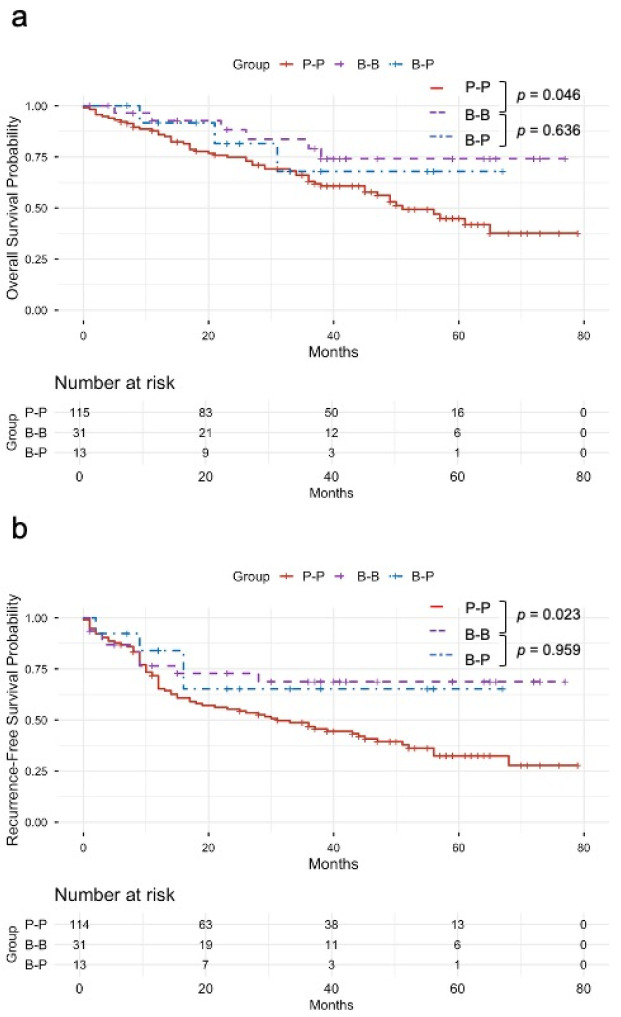 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Pancreatic and Hepatic Oncology Research · Gallbladder and Bile Duct Disorders
1. Introduction
Accurately differentiating pancreatic head cancer (PHC) from distal cholangiocarcinoma (dCCA) poses a persistent challenge in clinical practice. These tumors are anatomically contiguous and frequently share nonspecific symptoms and overlapping radiologic features, while reliable tumor-specific biomarkers remain unavailable [1]. As a result, the preoperative distinction between the two entities is often difficult, even for experienced clinicians. Diagnosis typically relies on a combination of clinical findings, laboratory data, and imaging modalities, including contrast-enhanced computed tomography (CE-CT), magnetic resonance imaging, and endoscopic ultrasound (EUS). However, most prior investigations have focused on the diagnostic utility of these modalities in staging or assessing resectability rather than on their capacity to differentiate PHC from dCCA before surgery [2,3,4,5,6,7].
Despite the frequency of this diagnostic dilemma, few studies have systematically compared patients preoperatively diagnosed with dCCA who were ultimately found to have pancreatic ductal adenocarcinoma (PDAC) on final pathology, in contrast to those accurately diagnosed with PDAC both pre- and postoperatively [8,9]. In particular, such comparative studies from high-volume institutions in Japan remain highly limited. Clarifying these distinctions’ clinical, surgical, and oncologic implications may help improve preoperative diagnostic strategies and optimize treatment selection. In Japan, neoadjuvant chemotherapy (NAC) is the standard treatment strategy for pancreatic cancer, even in resectable cases [10]. By contrast, dCCA is managed with upfront surgery followed by adjuvant S-1 therapy [11]. These divergent treatment strategies mean that an incorrect preoperative diagnosis may substantially affect long-term postoperative outcomes. The aim of this study was to elucidate real-world data from a Japanese high-volume center regarding the diagnostic accuracy of preoperative differentiation between dCCA and PHC, and to investigate whether discrepancies in preoperative diagnosis influence the clinicopathological characteristics and oncologic outcomes.
2. Materials and Methods
2.1. Patients
This study included consecutive patients who were preoperatively diagnosed with PHC, or dCCA, and who underwent either open or robot-assisted pancreatoduodenectomy at Juntendo University Hospital between January 2019 and December 2023. Patients with a final pathological diagnosis of noninvasive intraductal papillary mucinous carcinoma (IPMC) and those who underwent conversion surgery for unresectable PHC were excluded. We retrospectively reviewed medical records retrieved from a prospectively maintained database, including baseline characteristics, demographic data, preoperative imaging findings, surgical procedures and details, histopathological findings, postoperative outcomes, and prognoses. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Juntendo University Hospital (approval number: E25-0209).
2.2. Treatment Strategy
NAC was administered to patients who were assessed as having PHC based on preoperative imaging. For patients with resectable disease, the NAC regimen consisted of two cycles of gemcitabine plus S-1, in accordance with the Prep-02/JSAP05 trial [10,12]. For patients with borderline resectable tumors, gemcitabine plus nab-paclitaxel or modified FOLFIRINOX, comprising oxaliplatin, irinotecan, fluorouracil, and leucovorin, were administered [13]. Following NAC, tumor resectability was reassessed using CE-CT, and radical resection was performed in appropriate candidates. In contrast, patients who were preoperatively diagnosed with dCCA did not routinely receive NAC. Therefore, these patients proceeded directly to surgery without preoperative systemic treatment. Postoperative adjuvant chemotherapy was administered using S-1 in accordance with the ASCOT trial [11,14]. During the follow-up period, tumor markers (carcinoembryonic antigen, carbohydrate antigen 19-9 [CA19-9], or Duke pancreatic monoclonal antigen type 2) and imaging studies with CE-CT were performed every 3 months for the first 3 years and every 6 months thereafter up to 5 years.
2.3. Surgery
All patients in this study underwent pancreatoduodenectomy, primarily via an open approach. Subtotal stomach-preserving pancreatoduodenectomy was the standard procedure performed. In selected cases diagnosed with invasive IPMC or dCCA preoperatively, robot-assisted pylorus-preserving pancreatoduodenectomy was also performed. The choice of surgical approach was based on the preoperative diagnosis, tumor characteristics, and the general condition of the patient. Conventional lymph node dissection was performed in all cases, following standard oncological principles without excess or omission. In PHC patients where tumor attachment or involvement to portal vein were observed in CT before chemotherapy, portal vein resection (PVR) was performed as previously reported [15,16].
2.4. Image Analysis
Preoperative imaging evaluation was routinely performed using CE-CT and EUS. EUS was performed using standard echoendoscopes under conscious sedation, and contrast agents were administered when considered appropriate. When PHC was suspected preoperatively, we generally obtained a histological diagnosis by EUS-guided fine-needle aspiration (FNA) prior to NAC. In contrast, when dCCA was suspected, we prioritized tissue diagnosis (or cytology) during endoscopic retrograde cholangiopancreatography (ERCP) over histological confirmation by EUS-FNA. If vascular invasion within the hepatoduodenal ligament was suspected, intraductal ultrasonography was performed. Rapid on-site evaluation was not available for these procedures during this study period.
The diagnosis of either dCCA or pancreatic cancer was made by a multidisciplinary team based on preoperative imaging findings, clinical presentation and assessment. In this study, a preoperative diagnosis of dCCA was defined as a lesion primarily located within the bile duct, without obvious evidence of pancreatic involvement. Conversely, PHC was suspected when the lesion was considered to originate from the pancreatic parenchyma or the peripancreatic region, even in cases where no distinct mass was visualized in the pancreatic head. Several imaging features on dynamic CT were considered suggestive of PHC. These included cases in which the main lesion appeared to extend beyond the bile duct (Figure 1a,b), lesions with prominent lateral growth, particularly those spreading along the hepatoduodenal ligament (Figure 1c,d); obstruction of the main pancreatic duct (Figure 1e); and clear signs of local invasiveness into surrounding structures [7,17,18,19]. Bile duct wall thickening, although frequently observed, was not used as a discriminating feature between the two disease entities. Preoperative imaging findings were independently reviewed by two board-certified radiologists, including one with subspecialty expertise in hepatopancreatobiliary imaging, as well as at least two hepatopancreatobiliary surgeons. In cases of disagreement, a consensus was reached through discussion.
2.5. Pathological Evaluation
Pathological findings were independently assessed by two or more board-certified pathologists specializing in HBP diseases at our institution. Specimen processing and diagnostic evaluation were performed in accordance with the General Rules for the Study of Pancreatic Cancer, eighth edition (Japan Pancreas Society) [20], and the General Rules for Clinical and Pathological Studies on Cancer of the Biliary Tract, seventh edition (Japan Biliary Association) [21]. Briefly, the pancreas and the bile duct specimens were cut at 5 mm intervals, and all were processed for pathologic examination. The final diagnosis was determined by consensus following a comprehensive review of histological findings [22]. The pathologists presented a mapped overlay of tumor invasion on photographs of the macroscopic cut surfaces. Tumors were classified as dCCA when (1) carcinoma in situ or high-grade intraepithelial neoplasm was observed at bile duct mucosa, (2) invasive carcinoma involved bile duct wall circumferentially for at least one section, (3) no high-grade intraepithelial neoplasm was observed at pancreatic ducts, (4) tumor progression along the long axis of the bile duct (>2 continuous sections) was observed, and (5) no cancerous involvement of duodenal ampullary region was detected. In contrast, those were classified as PHC when (1) no carcinoma in situ or high-grade intraepithelial neoplasm was present, whereas benign bile duct epithelia were lining the bile duct mucosa (Figure 2). When cases did not satisfy either of the dCCA and PHC criteria, as written above, they were excluded from this study. The histological grade of ductal adenocarcinoma was determined according to the current WHO classification, which is based on combined assessment of glandular differentiation, mucin production, mitotic activity, and nuclear features. In cases with intratumoral heterogeneity, the higher grade was assigned, even if the high-grade component constituted less than 50% of the tumor [23,24].
2.6. Statistical Analysis
Overall survival (OS) was defined as the time from the date of diagnosis, based on initial radiological or pathological evaluation, to the date of death from any cause. Recurrence-free survival (RFS) was defined as the time from the date of surgery to the date of first documented recurrence or death. Continuous variables with a normal distribution were compared using the independent Student’s t-test and are presented as means with standard deviations. For variables that did not follow a normal distribution, the Mann–Whitney U test was applied, with results expressed as medians and interquartile ranges. Multivariable analysis was performed using Cox proportional hazards regression with stepwise variable selection. OS and RFS were initially evaluated using the log-rank test, followed by univariate Cox proportional hazards regression analysis to estimate hazard ratios (HRs) and 95% confidence intervals (CIs). Statistical analyses were performed using R (version 4.3.2 for macOS; R Foundation for Statistical Computing, Vienna, Austria) and JMP^®^ Pro 18.1.2 (SAS Institute Inc., Cary, NC, USA).
3. Results
A total of 183 patients underwent pancreatoduodenectomy for PHC or dCCA between January 2019 and December 2023. Twenty-four were excluded (postoperative diagnosis of noninvasive IPMC and conversion surgery for initially unresectable PHC), leaving 159 patients for analysis (Figure 3). Preoperatively, 44 were assigned as dCCA and 139 as PHC. The patient baseline characteristics according to pre- and postoperative diagnoses in three groups are shown in Table 1.
3.1. Preoperative Comparison Between Three Groups
Among the 44 patients preoperatively diagnosed with dCCA, 31 were confirmed postoperatively as dCCA (B-B group) and 13 as PDAC (B-P group). In addition, of the 128 patients with postoperative PHC, 115 were preoperatively concordant (P-P group) and 13 were initially assigned as dCCA (B-P group). The proportion of diagnostic discrepancy between prior and after surgery in patients with preoperative dCCA was 29.5%. Conversely, there were no cases in which a preoperative diagnosis of PDAC was revised to a postoperative diagnosis of dCCA. The median age was 74 years in the B-P group and 80 years in the B-B group (p = 0.104). Preoperative biliary drainage was performed in all B-P patients and in 90.3% of B-B patients (p = 0.138). The median total bilirubin level was slightly lower in the B-P group (12 μmol/L) than in the B-B group (17 μmol/L, p = 0.149). The main pancreatic duct diameter was significantly larger in the B-P group (2.8 mm vs. 2.1 mm, p = 0.038), and portal vein contact was more frequent (46.1% vs. 6.4%, p = 0.002). No significant differences were observed in other preoperative variables. Between the P-P and B-P cohorts, B-P patients were significantly older (p = 0.036), were more likely to have received preoperative biliary drainage (p < 0.001) and had higher amylase (p = 0.020) and lower C reactive protein levels (p = 0.001). In contrast, the P-P group showed a larger main pancreatic duct diameter (p < 0.001), a higher rate of portal vein contact (p < 0.001), and more frequent NAC (p < 0.001). No other preoperative variables differed significantly.
3.2. Postoperative Comparison Between Two Groups with Postoperative Diagnosis of PHC
Detailed postoperative comparisons are summarized in Table 2. The maximum tumor diameter was larger in B-P (38 vs. 25 mm, p = 0.009). The lymph node ratio was higher (0.142 vs. 0, p = 0.006), the number of metastatic lymph nodes was greater (median 4 vs. 0, p = 0.003), and lymph node metastasis was more frequent (76.9% vs. 46.9%, p = 0.036). Station 12b lymph node metastasis occurred more often in the B-P (38.4% vs. 3.5%, p < 0.001). Bile-duct invasion was present in 100% vs. 41.2% (p < 0.001). Soft pancreatic texture was more common in the B-P (76.9% vs. 28.7%, p < 0.001). R0 resection was less frequently achieved in B-P (61.5% vs. 84.3%, p = 0.043). Portal vein resection was performed in 46.1% vs. 59.1% (p = 0.369), while unplanned portal vein resection was conducted only in the B-P (30.7% vs. 0%, p < 0.001). Operative time, intraoperative blood loss, 90-day mortality, severe complications (Clavien–Dindo ≥ IIIa), and adjuvant chemotherapy were comparable.
3.3. Long-Term Outcomes
Recurrence patterns differed significantly between the two groups (p = 0.013). Local recurrence was observed more frequently in the B-P group (30.7% vs. 10.5%), while distant metastases occurred only in the P-P group (38.6% vs. 0%). No lymph node recurrences were reported in either group (Table 3).
OS did not differ between the P-P and B-P groups (p = 0.363; Figure 4a). 5-year OS was 44.8% in the P-P and 67.9% in the B-P; median OS was 51 months in the P-P group and not reached in B-P group. RFS was also comparable (p = 0.183; Figure 4b). 1- and 3-year RFS were 65.3% and 46.7% in the P-P, and 83.9% and 65.3% in the B-P group. In multivariable Cox analysis for OS, the B-P group was associated with a lower risk of death than the P-P (HR 0.137, 95% CI 0.026–0.735, p = 0.020). Additional independent predictors of worse OS were higher CA19-9 (HR 1.18, p = 0.015), larger tumor size (HR 1.03, p = 0.024), and higher lymph node ratio (HR 2.10, p < 0.001), while older age was associated with a lower risk of death (HR 0.965, p = 0.001). For RFS, B-P showed a favorable but non-significant association (HR 0.228, 95% CI 0.046–1.118, p = 0.068). Independent predictors of shorter RFS were higher CA19-9 (HR 1.20, p = 0.006) and higher lymph node ratio (HR 1.62, p = 0.004), whereas older age was associated with a lower risk of recurrence (HR 0.966, p < 0.001).
4. Discussion
This study demonstrated the persistent difficulty in achieving accurate preoperative differentiation between dCCA and PHC, highlighting that a subset of PHC remains indistinguishable from dCCA before surgery (B-P group). We compared the B-B with the B-P groups preoperatively and the P-P with the B-P groups postoperatively. We demonstrated that, despite incorporating multidisciplinary imaging assessment and established diagnostic criteria, preoperative identification of B-P cases remains inherently challenging, with a subset inevitably exhibiting pre- to postoperative diagnostic discordance. Notably, the B-P group underwent upfront surgery without NAC and exhibited a higher burden of lymph node metastases yet achieved OS and RFS rates comparable to the P-P group. This paradox, more advanced nodal disease but equivalent prognosis, together with significant differences in histological grade between groups, suggests that distinct tumor biology may underlie the observed outcomes. Furthermore, in multivariable analysis for OS, the B-P group remained an independent prognostic factor associated with a lower risk of death. By integrating detailed preoperative imaging analysis, comprehensive pathological mapping, and survival assessment within a single high-volume institutional cohort, our findings address a persistent diagnostic blind spot in HPB oncology and open new avenues for refining preoperative risk stratification and treatment selection.
Differentiating between PDAC and dCCA, especially in periampullary tumors, remains challenging, with approximately 16% of cases ultimately reclassified at definitive pathology [9,18,25]. Both entities share overlapping clinical features and imaging characteristics [7]. When stratified by disease type, the accuracy of preoperative diagnosis was 84% for pancreatic cancer, 71% for dCCA, 73% for ampullary cancer, and 73% for duodenal cancer [9]. These figures highlight the particular diagnostic challenge associated with dCCA. Notably, despite a standardized preoperative diagnostic algorithm combining CE-CT and EUS, with ERCP or magnetic resonance imaging as indicated, we observed no diagnostic discordance among cases preoperatively assigned as PHC. This underscores the high specificity and reliability of our preoperative assessment, particularly when compared to previous reports of a 12–13% misdiagnosis rate in this direction [26]. In contrast, approximately 30% of patients assigned preoperatively as dCCA were postoperatively confirmed as PHC. Despite the integration of multiple diagnostic modalities, including CE-CT, EUS, and intraductal ultrasonography, preoperative differentiation between dCCA and PHC remains inherently challenging. This diagnostic dilemma persists because both tumors originate in close proximity within the pancreatic head and often share overlapping imaging characteristics. In the comparison of preoperative factors between the B-P and B-B cohorts, main pancreatic duct diameter differed statistically (median 2.8 vs. 2.1 mm, p = 0.038), although the absolute difference was small, which might indicate limited discriminatory value of preoperative imaging for distinguishing PHC from dCCA. To overcome these diagnostic hurdles, meticulous diagnostic EUS and thorough EUS-guided tissue sampling might be instrumental, particularly for cases of dCCA diagnosed on preoperative CE-CT [27,28]. Clinical consideration of these diagnostic approaches may be required, as accurate preoperative diagnosis has significant clinical implications.
Treatment strategies for PHC and dCCA differ substantially. For PDAC, NAC is now regarded as a standard of treatment as endorsed by major international guidelines [29], even for resectable status [20]. NAC improves the likelihood of achieving R0 resection and allows early treatment of micrometastases [30,31]. Furthermore, surgical planning is influenced by whether the tumor is PHC or dCCA. When PHC is suspected preoperatively and radiologic findings suggest portal vein contact or involvement, PVR can be proactively incorporated into the surgical strategy [15,16]. In such cases, surgeons avoid dissecting near the tumor and instead plan for en-bloc resection, thereby minimizing intraoperative complications and optimizing oncologic outcomes. In addition, perioperative treatment strategies continue to diversify for both pancreatic and biliary tract cancers, accurate preoperative diagnosis has become increasingly critical [32,33,34]. This divergence in treatment approach underscores the importance of correct preoperative diagnosis. Compared with the P-P group, the B-P group exhibited a higher rate of unplanned PVR (30.7% vs. 0%, p < 0.001) and a lower R0 rate (61.5% vs. 84.3%, p = 0.043), along with a higher local recurrence rate (30.7%). These patterns might reflect the impact of NAC and an en-bloc resection policy that includes PVR.
Reports specifically addressing the preoperative distinction between PHC and dCCA are limited. A diagnostic scoring system incorporating CA19-9 > 230 U/mL, C-reactive protein > 10 mg/dL, and main pancreatic duct dilatation > 3 mm has been proposed, with a score > 1 suggesting PDAC (Area Under the ROC curve 0.74, p < 0.001) [18]. In addition, Roessel et al. identified clinical predictors of PDAC in cases initially diagnosed as dCCA, including >10% weight loss, CA19-9 > 160 U/mL, vascular invasion on imaging, tumor size > 20 mm, and positive EUS-guided fine-needle aspiration [9]. Notably, in PDAC cases initially classified as dCCA and subsequently confirmed as PDAC, the median OS was comparable to that of preoperatively concordant PDAC managed without neoadjuvant therapy (21.5 vs. 19.4 months), indicating no evident impact of diagnostic discordance on short-term survival. Relatedly, pancreatic groove cancer, a periampullary tumor that is particularly difficult to differentiate from distal cholangiocarcinoma, has been reported to exhibit well-differentiated histology in 43% of cases, with perineural invasion present in 90% and both lymphovascular invasion and lymph node metastasis identified in 83%. Moreover, well-differentiated tumors have been reported to be associated with better survival outcomes than moderately or poorly differentiated tumors [8].
Molecular subtype classification of PDAC, particularly the Moffitt classification, may partly explain these findings. This system stratifies tumors into Classical and Basal-like subtypes, with the Basal-like subtype associated with poor prognosis [35,36,37]. The Classical subtype shows higher tumor differentiation, consistent with the significantly better differentiation observed in the B-P group than in the P-P group. Although molecular subtyping was not performed, subtype-related tumor biology might have contributed to the observed prognostic differences. These observations suggest that the B-P group might represent a biologically distinct subgroup of pancreatic cancer with a less aggressive clinical course. While these biological characteristics could mitigate the impact of unfavorable surgical results, future large-scale studies are necessary to fully elucidate the relationship between tumor biology and diagnostic discordance in these patients.
This study has several limitations. First, it is a retrospective single-center study, subject to inherent biases in patient selection and data collection. Second, the total number of patients with a preoperative diagnosis of dCCA was small (n = 44), and specifically, the B-P group consisted of only 13 patients. This small sample size, especially when compared with the P-P group (n = 115), represents a major limitation in achieving robust statistical comparisons and may have introduced potential biases. Third, although two pre-dCCA patients received preoperative systemic treatment for suspected advanced disease, these were not standardized protocols. Fourth, our pathological classification of P-P and B-P is histology-based, and not molecular-based. Molecular or genomic characteristics could further clarify tumor origin or subtype classification. Fifth, 29.5% of patients who were preoperatively diagnosed with dCCA were ultimately found to have PDAC, suggesting a substantial rate of diagnostic discrepancy. One contributing factor may be the tendency to classify tumors with extensive longitudinal spread along the bile duct as cholangiocarcinoma with extensive biliary involvement, which could have reduced the number of cases specifically diagnosed as dCCA. Lastly, the substantial difference in neoadjuvant chemotherapy use between groups (67.8% vs. 15.3%) may have introduced residual confounding that could have influenced survival outcomes. Therefore, the present findings should be considered hypothesis-generating and require validation in larger, multi-institutional cohorts.
5. Conclusions
In conclusion, a proportion of cases assigned as dCCA preoperatively may represent PDAC. PDAC presenting with a dCCA-like phenotype may constitute a biologically more indolent subset, and in our cohort, this pre- to postoperative diagnostic discordance was not associated with inferior survival. Complete preoperative discrimination remains difficult, underscoring the need for refined diagnostic pathways and integrated clinicopathological assessment to optimize treatment selection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Macias R.I. Muñoz-Bellvís L. Sánchez-Martín A. Arretxe E. Martínez-Arranz I. Lapitz A. Gutiérrez M.L. La Casta A. Alonso C. González L.M. A novel serum metabolomic profile for the differential diagnosis of distal cholangiocarcinoma and pancreatic ductal adenocarcinoma Cancers 202012143310.3390/cancers 1206143332486461 PMC 7352809 · doi ↗ · pubmed ↗
- 2Harder F.N. Jung E. Mc Tavish S. Van A.T. Weiss K. Ziegelmayer S. Gawlitza J. Gouder P. Kamal O. Makowski M.R. High-Resolution, high b-Value computed diffusion-weighted imaging improves detection of pancreatic ductal adenocarcinoma Cancers 20221447010.3390/cancers 1403047035158737 PMC 8833466 · doi ↗ · pubmed ↗
- 3Horvat N. Ryan D.E. La Gratta M.D. Shah P.M. Do R.K. Imaging for pancreatic ductal adenocarcinoma Chin. Clin. Oncol.201866210.21037/cco.2017.11.0329307202 · doi ↗ · pubmed ↗
- 4Elbanna K.Y. Jang H.-J. Kim T.K. Imaging diagnosis and staging of pancreatic ductal adenocarcinoma: A comprehensive review Insights Imaging 20201111310.1186/s 13244-020-00861-y 32335790 PMC 7183518 · doi ↗ · pubmed ↗
- 5Corallo C. Al-Adhami A.S. Jamieson N. Valle J. Radhakrishna G. Moir J. Albazaz R. An update on pancreatic cancer imaging, staging, and use of the PACT-UK radiology template pre-and post neoadjuvant treatment Br. J. Radiol.202598132610.1093/bjr/tqae 21739460945 PMC 11652714 · doi ↗ · pubmed ↗
- 6Bowman A.W. Bolan C.W. MRI evaluation of pancreatic ductal adenocarcinoma: Diagnosis, mimics, and staging Abdom. Radiol.20194493694910.1007/s 00261-018-1686-x 29967986 · doi ↗ · pubmed ↗
- 7Lv T.-R. Wang J.-M. Ma W.-J. Hu Y.-F. Dai Y.-S. Jin Y.-W. Li F.-Y. The consistencies and inconsistencies between distal cholangiocarcinoma and pancreatic ductal adenocarcinoma: A systematic review and meta-analysis Front. Oncol.202212104249310.3389/fonc.2022.104249336578941 PMC 9791204 · doi ↗ · pubmed ↗
- 8Ku Y.-H. Chen S.-C. Shyr B.-U. Lee R.-C. Shyr Y.-M. Wang S.-E. Pancreatic groove cancer Medicine 201796 e 564010.1097/MD.000000000000564028079795 PMC 5266157 · doi ↗ · pubmed ↗