Patient, Physician, and Caregiver Preferences for Lung Cancer Treatment: A Systematic Review of Discrete Choice Experiments
Sida Wang, Yun Liu, Mengyu Yang, Linning Wang, Jie Yu, Xiaoxi Xie, Feng Chang, Yun Lu

TL;DR
This study reviews how patients, doctors, and caregivers prioritize lung cancer treatment options based on their preferences.
Contribution
The paper systematically synthesizes discrete choice experiments to compare preferences across different stakeholders in lung cancer treatment.
Findings
Preferences for lung cancer treatment differ among patients, physicians, and caregivers.
Attributes related to treatment outcomes, processes, and costs were most commonly evaluated.
Study quality was generally high, but there were limitations in population coverage and experimental design.
Abstract
Objectives: This systematic review aimed to synthesize evidence from discrete choice experiments to explore the preferences of patients, physicians, and caregivers regarding lung cancer treatment. Methods: A systematic literature search was conducted utilizing the PubMed, Web of Science, Embase, and Scopus databases, encompassing publications up to 12 July 2024. We included published discrete choice experiment (DCE) studies that assessed preferences for lung cancer treatment among patients, physicians, or caregivers, with no restrictions on country, language, publication date, or disease stage. Two researchers independently conducted the literature screening and data extraction. The included studies were assessed for quality using the PREFS checklist. Results: Among the 1086 studies identified, 18 studies met the eligibility criteria. A total of 115 attributes were extracted and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
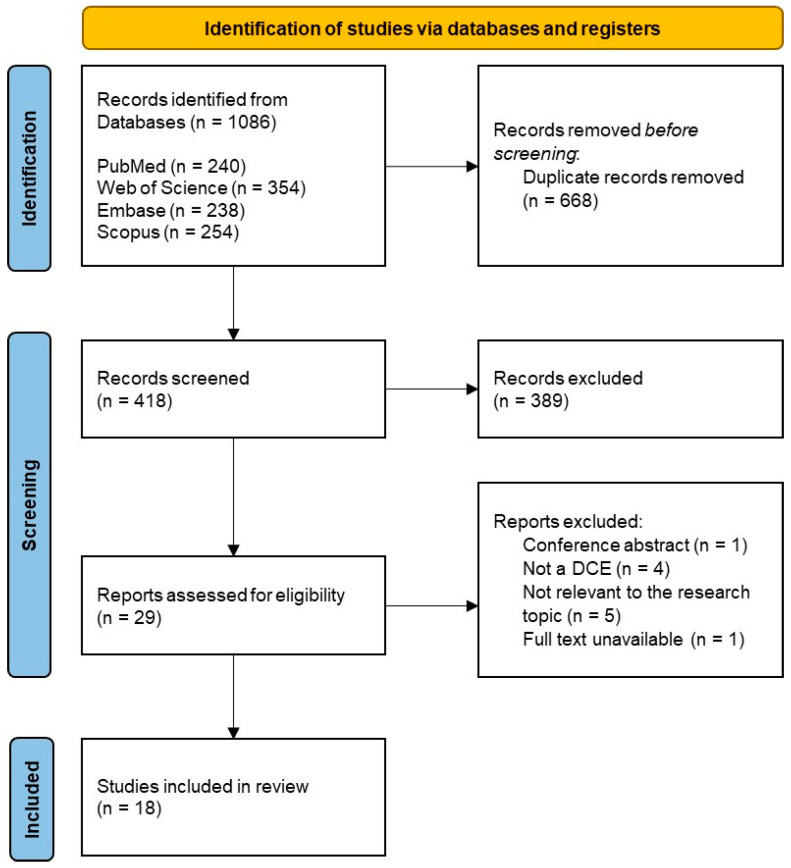 Figure 1
Figure 1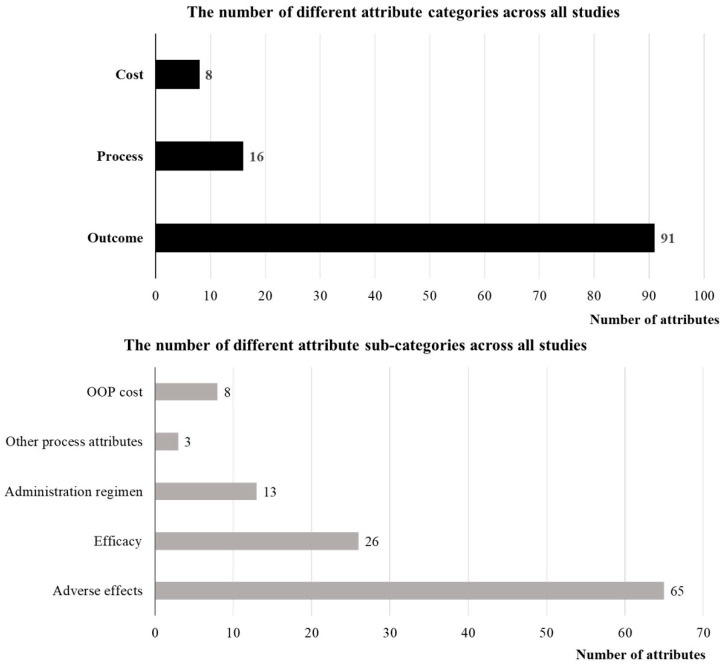 Figure 2
Figure 2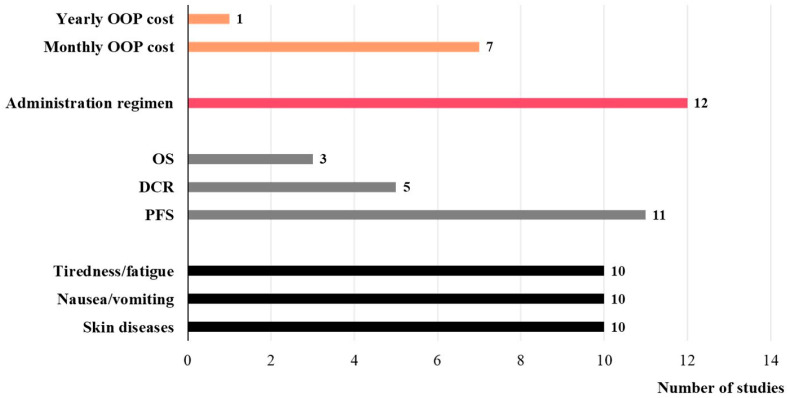 Figure 3
Figure 3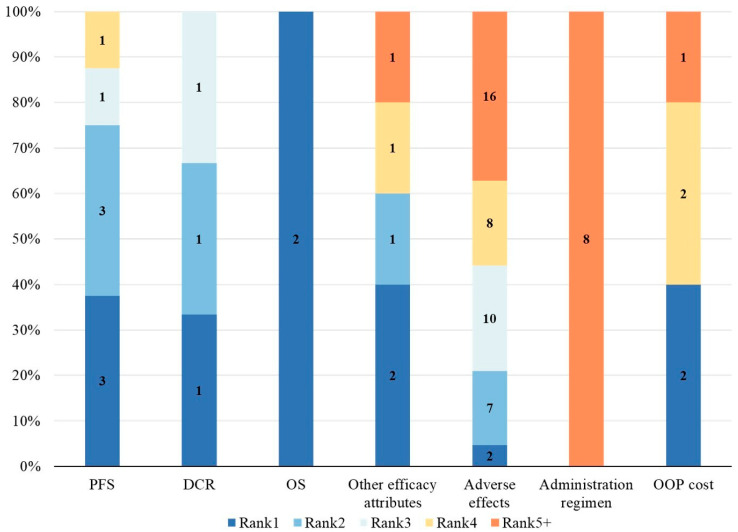 Figure 4
Figure 4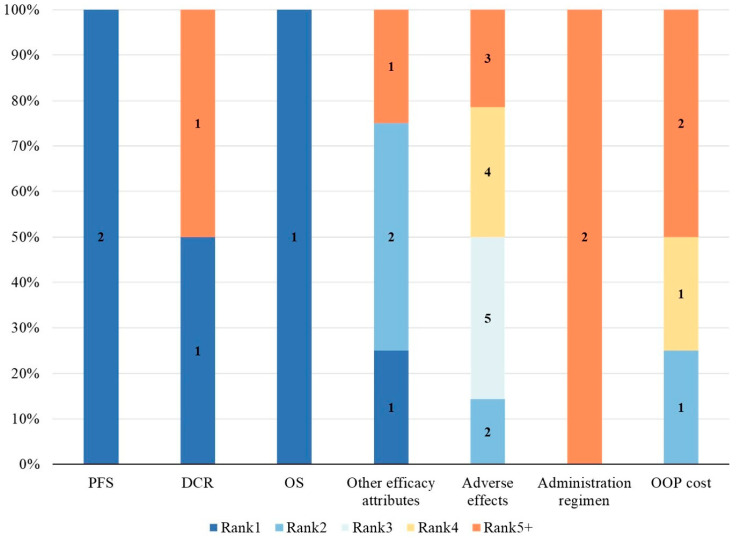 Figure 5
Figure 5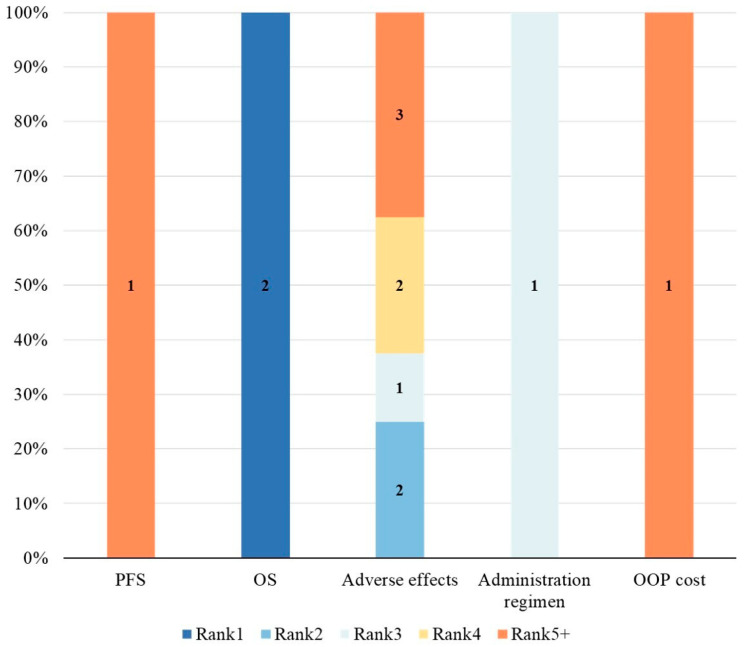 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEconomic and Environmental Valuation · Patient-Provider Communication in Healthcare · Lung Cancer Diagnosis and Treatment
1. Introduction
Cancer presents a major global public health concern and remains one of the leading causes of mortality and disease burden worldwide [1]. According to the latest global cancer burden data from the International Agency for Research on Cancer (IARC) of the World Health Organization (WHO), an estimated 20 million new cancer cases and 9.7 million cancer deaths occurred globally in 2022 [2]. With 2.5 million new cases and 1.8 million deaths [2], lung cancer stands as the cancer type with the highest incidence and mortality rates globally, imposing substantial psychological and economic burdens not only on patients but also on their families and society. Lung cancer is classified into two main types based on pathological characteristics: non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC), with NSCLC being the most prevalent, accounting for approximately 80% to 85% of all lung cancer cases [3,4]. With continuous advancements in medical technology, treatment options for lung cancer have expanded to encompass not only traditional methods such as surgery, chemotherapy, and radiotherapy, but also various emerging therapies like molecular targeted therapy, photothermal therapy, and immunotherapy [5,6,7]. However, this diversity may increase the complexity of treatment decisions, requiring a comprehensive assessment of various factors, including the patient’s clinical condition, treatment expectations, quality of life, and potential side effects. In this context, patients, physicians, and caregivers (the latter used here as an umbrella term for individuals involved in supporting patients and/or participating in treatment decisions) may exhibit diverse preferences when selecting treatment options. Physicians rely on their expertise to formulate a rational and personalized treatment strategy for the patient. Unlike patients, caregivers do not directly experience treatment benefits and harms, but their preferences may reflect caregiving burden and practical considerations. Meanwhile, patients and caregivers need to weigh the different treatment options in alignment with their actual condition and expectations regarding quality of life to select the most appropriate treatment. Therefore, it is essential to conduct an in-depth exploration of the differences in treatment preferences among patients, physicians, and caregivers in the management of lung cancer.
Preferences can be categorized into 2 types based on the method of measurement: revealed preferences and stated preferences. Specifically, revealed preferences involve analyzing actual observed behaviors, reflecting individuals’ authentic decision-making processes. In contrast, stated preferences are based on feedback collected through surveys to assess respondents’ preferences for specific options or scenarios under hypothetical conditions [8,9]. In recent years, Discrete Choice Experiments (DCE) have become a popular tool for assessing stated preferences and have been widely used in the field of health economics [10,11,12], increasingly to quantify the preferences of patients, physicians, and other stakeholders [13]. In DCE, a series of choice scenarios simulating real-life decision-making contexts is designed by combining different attributes and levels, prompting respondents to select their most favored option from two or more alternatives. Subsequently, appropriate statistical models are employed to quantitatively analyze respondents’ choices and estimate their underlying preferences for various attributes and levels [13,14]. DCEs infer preferences by analyzing respondents’ choice behaviors. The choice scenarios closely resemble real-world decision-making contexts, enabling reliable preference measurement in practical applications. In contrast, simple ratings/rankings or qualitative interviews alone are less suited to producing directly comparable trade-off estimates. Therefore, to comprehensively understand the preferences of different stakeholders regarding lung cancer treatment, it is essential to review and analyze existing DCE studies systematically.
Previous systematic reviews on preferences for lung cancer treatment have primarily focused on the patient’s perspective [15,16]. However, as treatment decisions involve multiple stakeholders, relying solely on patient preferences fails to capture the complexity of real-world clinical decisions and may overlook critical barriers to implementation. Despite numerous studies exploring the preferences of physicians and caregivers in lung cancer treatment, the differences in preferences between them and patients are still lacking. Therefore, this study aims to conduct a systematic review of DCEs and compare the preferences of patients, physicians, and caregivers regarding lung cancer treatment. The findings of this study will not only deepen the understanding of the decision-making process in lung cancer treatment among various stakeholders but also provide vital insights for personalized lung cancer treatment planning.
2. Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines established by Moher et al. [17]. The study protocol was registered with PROSPERO (CRD42024623604). No deviations from the registered protocol occurred.
2.1. Search Strategy
The literature search for this systematic review was conducted across four relevant databases: PubMed, Web of Science, Embase, and Scopus. The search timeframe covered the period from each database’s inception to 12 July 2024. The search terms included two categories: those related to discrete choice experiments (DCEs) and those related to lung cancer. The DCE-related search terms were derived from previous systematic reviews on DCEs, including terms such as “conjoint experiment”, “conjoint analysis”, “conjoint measurement”, “conjoint study”, “paired comparison”, “discrete choice”, and “stated preference” [11,12,18]. The lung cancer-related search terms were formulated using a combination of MeSH terms and free-text terms. The complete electronic search strategies for all databases were provided in Supplementary Materials Table S1.
2.2. Eligibility Criteria
The review question was structured using the PICO framework: patients with lung cancer and other key stakeholders involved in treatment decisions (patients, physicians, and caregivers) (P); preferences elicited in DCEs comparing alternative profiles defined by attributes and levels (I/C); and stakeholder preferences such as attribute importance or reported preference weights (O). Studies were included if they employed a DCE design to investigate the preferences of patients, physicians, or caregivers regarding lung cancer treatment. No restrictions were applied to country, language, publication date, or disease stage.
Studies meeting any of the following criteria were excluded: (1) studies not using a DCE design; (2) studies unrelated to the topic of this review; (3) studies that did not measure preferences; (4) studies assessing preferences for multiple cancer treatments simultaneously; (5) duplicate publications; (6) studies for which full-text information was unavailable; and (7) reviews, commentaries, reports, conference abstracts, dissertations, books, or other forms of grey literature. We excluded grey literature to focus on peer-reviewed DCE studies for consistent extraction and analysis.
2.3. Study Identification and Selection
The identification and selection of studies were conducted in stages by two researchers (S.D.W. and M.Y.Y.). First, the search results from each database were imported into the reference management software NoteExpress (version 4.1.0.10030), and duplicates were removed. Second, the titles and abstracts of the studies were preliminarily screened based on pre-defined eligibility criteria. Finally, the full texts of studies identified during the initial screening were evaluated to confirm their eligibility for inclusion. If a potentially eligible study was not in English, it would be translated for eligibility assessment and data extraction. At each stage, the screening results of the two researchers were compared, and any discrepancies or disagreements during the study identification and selection process were resolved through discussion and consultation with a third researcher (Y.L.).
2.4. Data Extraction and Analysis
Data extraction was independently conducted by two researchers (M.Y.Y. and Y.L.), followed by collation and verification by a third researcher (S.D.W.). The extracted information primarily included the following aspects: (1) basic information of the included studies: first author, publication year, country/region of the study, disease condition, treatment type, respondent type, sample size, response rate, and survey administration method; (2) DCE choice task design: the process of determining attributes and levels, descriptions and number of attributes, descriptions and number of levels, experimental design software, number of choice sets, use of block designs, number of choice tasks answered per respondent, number of alternatives, use of labeled designs, inclusion of opt-out/status quo options, and whether a pilot study was conducted; (3) DCE statistical analysis: econometric models used, types of variable coding, data analysis software, and common metrics for comparing relative attribute effects; (4) relative attribute importance (RAI) (extracted as reported; when not explicitly reported, attributes were ranked within each study based on the coefficient range for each attribute); (5) study conclusions and recommendations.
2.5. Quality Assessment
This study used the PREFS checklist developed by Joy et al. to assess the quality of the included studies [19]. The PREFS checklist is concise, easy to use, and widely applied for quality assessment in DCE studies [20,21,22,23,24,25]. It focuses on five key aspects: purpose, respondents, explanation, findings, and significance. These aspects correspond to the core reporting elements needed to interpret DCE methods and results. Each aspect is scored dichotomously, with a score of 1 if the criterion is met and 0 otherwise. The total score for each study is the sum of scores across these five aspects, ranging from 0 to 5. The primary quality assessment process was independently conducted by two researchers (L.N.W. and M.Y.Y.) using the checklist. Any unresolved disagreements were addressed through discussion or consultation with a third researcher (Y.L.). However, PREFS does not fully capture DCE-specific methodological features (e.g., attribute development, experimental design efficiency, or econometric models). Therefore, PREFS scores were interpreted as an indicator of reporting quality rather than a formal risk of bias assessment.
3. Results
3.1. Search Results
Through the electronic database search, a total of 1086 records were retrieved, with 668 duplicate records removed. Of the remaining 418 records, 389 were excluded after title and abstract screening for not meeting the eligibility criteria. Consequently, 29 records were selected for full-text screening. After full-text screening, 18 studies met the inclusion criteria and were included in this systematic review [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43]. Among the 11 full-text studies excluded, the main reasons were ineligible study design (n = 9) and inability to extract relevant data (n = 2). The study selection process is illustrated in Figure 1, following the PRISMA guidelines.
3.2. General Characteristics of Included Studies
Table 1 summarizes the key characteristics of the included studies. These studies were published between 2012 and 2024, with 14 studies (78%) published after 2020 [30,31,32,33,34,35,36,37,38,39,40,41,42,43]. The included studies involved respondents from 8 countries. The largest number of studies came from the United States and China, each contributing 6 studies (33%). Japan accounted for 2 studies (11%) [37,43]. The United Kingdom [26], Germany [27], and Brazil [35] each contributed 1 study (6%), and one study (6%) was a multicenter survey involving Italy and Belgium [41].
The target populations of the included studies comprised patients, physicians, and caregivers. Studies targeting only patients accounted for 11 studies (61%) [26,27,28,29,30,34,35,36,37,41,42]. Studies targeting only physicians accounted for 2 studies (11%) [31,39]. Additionally, 5 studies (28%) included multiple respondent groups, involving patients and physicians (n = 2, 11%) [33,43], patients and caregivers (n = 2, 11%) [32,38], and patients, physicians, and caregivers (n = 1, 6%) [40].
Across included studies, 11 studies (61%) did not report response rates, and only 2 studies had a response rate higher than 50%. Regarding the survey administration method, 8 studies (44%) collected preference data exclusively online, while 7 studies (39%) used interviewer-administered/in-person methods. Most studies did not explicitly specify the type of treatment assessed (n = 8, 44%) [26,32,33,34,35,36,38,40], but 3 studies (17%) examined preferences for lung cancer chemotherapy [28,31,37], and 2 studies (11%) investigated preferences for traditional Chinese medicine treatments [39,42]. Sample sizes ranged from 24 to 466, with a median of 175. Notably, 13 studies (72%) had sample sizes exceeding 100 [27,28,30,31,33,34,36,37,38,39,40,41,42]. Response rates varied from 5.2% to 99.2%; however, the majority of studies did not explicitly report response rates. Regarding the administration methods of DCE surveys, 9 studies (50%) utilized online surveys [26,29,30,32,36,37,38,41,43], 7 studies (39%) conducted face-to-face interviews [27,28,31,34,39,40,42], and 2 studies (11%) did not explicitly specify the survey administration method [33,35].
3.3. Choice Task Design and Analysis
3.3.1. Choice Task Design
Table 2 summarizes the choice task designs in the studies reviewed. All studies reported the process used to determine the attributes and their respective levels, with the literature review being the most commonly used approach. 17 studies (94%) identified attributes and levels through literature reviews [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,42,43], 11 studies (61%) employed qualitative methods such as respondent interviews and focus groups [27,28,29,32,34,35,36,38,40,41,43], and 9 studies (50%) used expert consultations [26,28,29,31,33,34,35,39,42]. 4 studies (22%) combined all three methods [28,29,34,35]. The number of attributes in the studies typically ranged from 4 to 7, although three studies included 8 [26], 9 [38], and 10 attributes [37], respectively. Each attribute usually had between 2 and 4 levels, with a maximum of 6 levels [43]. The total number of DCE choice sets varied from 13 to 96 [32,40], with 12 studies (67%) using blocking techniques to reduce cognitive burden [27,29,30,33,35,36,37,39,40,41,42,43], randomly assigning respondents to different versions of the choice tasks. More than half of the studies (n = 13, 72%) involved 10 to 14 choice tasks per respondent [26,27,29,30,31,32,33,35,36,37,38,40,41,43], with an average of 12 tasks. However, only 2 studies (11%) included three options per choice task [36,43], offering an opt-out alternative in addition to the two primary options. This indicated that most studies required respondents to choose between two alternatives. The majority of studies (n = 16, 89%) utilized a generic design [26,27,28,29,30,31,32,33,34,35,36,37,39,40,41,42], while only 1 study (6%) implemented a label-based design [43], distinguishing between “Oral treatment” and “Intravenous treatment”. Additionally, 10 studies (56%) conducted pretests with the target population before the formal DCE surveys to assess the validity and clarity of the choice task design and questionnaire [26,28,30,31,33,34,35,39,41,42].
3.3.2. Analysis Procedure
Table 3 summarizes the analytical approaches used in the included studies. Among the econometric models, the mixed logit model was the most frequently applied (n = 10, 56%) [26,28,31,32,33,34,36,39,40,42], followed by the latent class model (n = 4, 22%) [27,30,40,41]. 1 study (6%) employed a mixed multinomial logit model [43], an extension of the multinomial logit model, which accounts for preference heterogeneity among respondents. Regarding variable coding, 6 studies (33%) used categorical variable coding (dummy coding or effect coding) for all attributes [26,27,29,36,37,38], while 11 studies (61%) combined categorical and continuous variable coding [28,30,31,33,34,35,39,40,41,42,43]. Due to the potential confounding between attribute parameter estimates and underlying subjective utility scales, direct comparisons of relative attribute effects based on parameter size and significance are not feasible. Consequently, parameter estimates typically need to be converted into a comparable common scale [44,45]. A total of 15 studies (83%) used a common metric to compare the relative effects of different attributes [26,27,28,29,30,31,32,33,34,35,36,38,40,41,43]. Among these, relative attribute importance (RAI) was the most commonly used metric (n = 8, 44%) [26,28,31,33,38,40,41,43], followed by willingness to pay (WTP) (n = 5, 28%) [28,30,31,34,40], with only a subset of studies incorporating cost variables.
3.4. Attribute Classification, Frequency, and Relative Attribute Importance
3.4.1. Attribute Classification
Figure 2 summarizes the classification of attributes across the included studies. To facilitate comparison, attributes were grouped into three main categories: outcome attributes, process attributes, and cost attributes [23,46,47]. Among the 18 studies included, a total of 115 attributes were reported, comprising 91 outcome attributes (79%), 16 process attributes (14%), and 8 cost attributes (7%). Each main category was further divided into distinct subcategories: outcome attributes were classified into treatment efficacy and adverse effects; process attributes included administration regimen (e.g., route of administration, frequency, duration) and other process-related factors; and cost attributes were subdivided into out-of-pocket costs and work-related losses, among others. Within the outcome attributes, 26 attributes (29%) were related to treatment efficacy, while 65 attributes (71%) concerned adverse effects. For process attributes, 13 attributes (81%) were related to the administration regimen, while 3 attributes (19%) fell under other process-related factors. All the attributes in the cost category were related to out-of-pocket costs. A detailed classification of attributes across all studies is provided in Supplementary Materials Table S2.
3.4.2. Attribute Frequency
Figure 3 illustrates the frequency of occurrence of each attribute category across all studies. Nearly half of the studies (n = 8, 44%) considered both outcome and process attributes [26,27,29,35,36,37,38,41], while 5 studies (28%) included all three attribute categories [28,30,31,34,43]. 2 studies (11%) focused exclusively on outcome attributes [32,33]. The most common process attribute across all studies was the administration regimen, appearing in 12 studies (67%) [26,27,28,29,31,34,35,36,37,38,41,43]. Among the outcome attributes, “Progression-Free Survival” (PFS) was the most frequently considered attribute in the domain of treatment efficacy, featured in 11 studies (61%) [26,27,28,29,31,32,34,36,37,38,43], followed by “Disease Control Rate” (DCR) (n = 5, 28%) [28,31,34,39,42] and “Overall Survival” (OS) (n = 3, 17%) [37,38,40]. In the domain of adverse effects, the most common attributes were “Skin Diseases”, “Tiredness/Fatigue”, and “Nausea/Vomiting”, each appearing in 10 studies (56%). A total of 8 studies (44%) included cost attributes [28,30,31,34,39,40,42,43], all of which pertained to out-of-pocket treatment expenses, with 7 studies reporting monthly costs and 1 study reporting annual costs.
3.4.3. Relative Attribute Importance
In different studies and stakeholder groups, the relative importance rankings of attributes were not fully consistent. To assess the relative importance of attributes across studies, we utilized Relative Attribute Importance (RAI) or level coefficients. Figure 4, Figure 5 and Figure 6 present the distribution of relative attribute importance rankings in studies reporting patient, physician, and caregiver preferences. Among the studies included in the analysis, over 70% (n = 14) directly reported RAI or provided the level coefficients necessary to compute the relative importance of attributes [26,27,28,29,31,33,34,36,38,39,40,41,42,43]. However, 4 studies were excluded from the analysis due to missing key data or the presence of significant errors in the data, which hindered the calculation of attribute relative importance.
From the patients’ perspective, 10 studies identified outcome attributes as the most important [26,27,29,33,36,38,40,41,42,43], while 2 studies prioritized cost attributes [28,34]. Process attributes were never considered the most important in any of the studies. Among the most important attributes, PFS was the most commonly cited, followed by OS, other efficacy-related attributes, adverse effects, and out-of-pocket costs. Furthermore, the second most important attributes were also predominantly outcome-related. From the physicians’ perspective, all 5 studies considered outcome attributes as the most important [31,33,39,40,43]. Among them, PFS remained the most frequently cited, followed by OS, DCR, and other efficacy-related attributes. The second most important attributes were mainly outcome-related, with only one study categorizing cost attributes as secondary in importance [31]. Studies on caregiver preferences were relatively limited. In the two relevant studies [38,40], OS was considered the most important attribute, followed by adverse effects as the second most important. Out-of-pocket treatment costs were regarded as relatively less important from the caregivers’ perspective.
3.5. Quality Assessment
Table 4 presents the quality assessment results of all included studies based on the PREFS checklist. The PREFS scores ranged from 2 to 5 across the 18 studies, with an average score of 3.8. Only 1 study (6%) achieved a perfect score [41]. The majority of studies (n = 13, 72%) received a score of 4 [26,27,28,29,31,32,34,35,36,39,40,42,43], while 3 studies (17%) scored 3 [30,33,37], and 1 study (6%) scored 2 [38]. Specifically, all studies reported the research objectives and outcomes, but only 1 study (6%) reported the differences between responders and non-responders [41]. Although almost all studies provided a detailed and clear explanation of the methods used to assess preferences, one study failed to do so [38]. Additionally, the majority of studies (n = 14, 78%) employed significance tests to evaluate preference outcomes [26,27,28,29,31,32,34,35,36,39,40,41,42,43].
4. Discussion
This systematic review identified 18 DCE studies that explored preferences for lung cancer treatment among various stakeholders, including patients, physicians, and caregivers. Lung cancer is one of the most common malignancies globally, and the number of DCE studies on this topic has increased in recent years, further emphasizing the necessity of conducting systematic reviews of DCE studies on preferences for lung cancer treatment. This systematic review summarized the key characteristics of the included studies, including the attributes and levels incorporated, the design of choice tasks, and the relative importance of attributes. The findings of this study will provide valuable insights for future research design, particularly in comparing preferences among different stakeholders, and offer crucial information to support clinical decision-making in lung cancer treatment.
We summarized and categorized the attributes reported in 18 DCE studies, finding that outcome attributes were the most frequently reported, followed by process and cost attributes. Most studies included two types of attributes, while only five incorporated all three. Notably, cost attributes were the least frequently reported, and all studies that included them focused solely on out-of-pocket treatment costs, without addressing other cost-related factors. Compared to outcome and process attributes, cost attributes are often more clearly defined, and their impact is usually perceived more intuitively [47]. However, existing studies primarily focused on out-of-pocket medical costs, neglecting other potential cost factors in lung cancer treatment, such as indirect costs associated with lost productivity due to treatment. Although cost attributes were less frequently studied, their importance in treatment decisions is undeniable. Therefore, it is suggested that future DCE studies incorporate a broader range of cost attributes.
In DCE studies, different groups may choose various preferences in the same scenarios, reflecting their distinct needs and concerns [48,49,50]. Specifically, lung cancer patients tend to focus more on health-related factors. PFS was identified as the most valued attribute by most patients, reflecting lung cancer patients’ desire for disease stability and preservation of quality of life during treatment. Adverse effects were consistently ranked as the least important attribute across many studies, indicating patients’ explicit trade-offs between risks and benefits: to obtain meaningful survival gains, they are willing to accept a certain level of treatment-related risk. However, this is not absolute. Brundage et al. showed that when OS benefits are uncertain, most patients do not prefer treatments that compromise quality of life solely for gains in PFS [51]. In addition, compared with physicians and caregivers, patients placed greater importance on out-of-pocket costs, possibly because they face more immediate concerns about the real-world risk of financial hardship due to illness.
As the primary decision-makers for treatment plans, physicians’ preferences for lung cancer treatment were similar to those of patients, with a greater emphasis on treatment effectiveness. However, physicians exhibit a lower preference for out-of-pocket costs. This may stem from their disease-centered approach to medical decision-making, where survival benefit remains the primary objective, while other attributes are viewed as secondary factors subject to trade-offs. For caregivers, their main concern is the patient’s OS. Extending a patient’s lifespan is not only a medical objective but also reflects the emotional bond with the patient and the value of their caregiving work. However, compared to physicians and patients, caregivers do not prioritize PFS or adverse effects. This may be because PFS benefits and adverse effects do not directly impact their caregiving burden and are difficult to translate into tangible, daily value.
In summary, although outcome attributes were generally regarded as the most important by different stakeholders, the degree of importance attached to specific outcome attributes varied. It should be noted that the relative importance of outcome, process, and cost attributes may also be context-dependent. Differences in the healthcare system and risk tolerance may partly shape how stakeholders trade off survival benefits, adverse effects, and costs. Furthermore, among DCE studies involving multiple groups, only one study varied the attributes used between two respondent groups. Although most DCE studies on lung cancer treatment preferences involved similar attributes, the concerns of different groups were not identical. To better reflect the true preferences of different stakeholders, future research should focus on tailoring attributes and level selection to the features of target populations, thereby enhancing the practical applicability of the findings.
In DCE designs, respondents are typically required to make decisions from a set of predefined choice tasks. However, we observed that most of the included studies did not include “opt-out” or “status quo” options in their choice task designs, instead requiring respondents to choose between two alternatives. While this approach may reduce the cognitive burden on respondents, it does not fully reflect real-world situations where respondents may decline all treatment options or prefer to maintain current treatment due to uncertainties or other factors. Including “opt-out” or “status quo” options would more accurately reflect respondents’ decision-making behaviors in such a context [52]. Additionally, forced choices may introduce bias by failing to capture respondents’ true preferences [53,54]. This may overstate respondents’ willingness to trade off treatment benefits against harms or costs. While “opt-out” or “status quo” options are common and important in real-world decisions, they have received limited attention in DCE studies. Therefore, we believe it is feasible that future DCE studies incorporate “opt-out” or “status quo” options into their design to simulate a more realistic choice environment. At the same time, allowing an “opt-out” or “status quo” option may increase task complexity or lead to higher opt-out rates, and these trade-offs should be considered when designing future studies.
The quality of the included studies was assessed using the PREFS checklist. Overall, the studies demonstrated high quality, with 72% scoring 4 out of 5 on the checklist. The main reason for score deductions was related to the “respondent” dimension, which assesses the risk of selection bias [19]. Selection bias may arise if responders differ from non-responders. Only one study reported similarities between responders and non-responders, while the others did not report such information, which could lead to non-response bias. Therefore, although the overall quality of these DCE studies is relatively high, certain areas still need improvement to enhance the representativeness of the results.
Although this review closely adhered to established best practice guidelines for systematic reviews, several potential limitations remain. First, the number of DCE studies included was limited, especially those involving physicians and caregivers. A total of 18 studies were included in this review, of which only 5 involved physicians and 3 involved caregivers. This may affect the generalizability of the results, particularly when exploring the preference differences among various stakeholders. Second, some studies did not report estimates of attribute preference weights, which prevented their inclusion in the analysis of relative attribute importance. Third, this review did not include a comparison of WTP among patients, physicians, and caregivers. While WTP is an important economic indicator, it was reported for caregivers in only one study, which resulted in an insufficient sample size for a representative comparison. Fourth, this review did not include grey literature, which may increase the risk of publication bias. Fifth, this review utilized the PREFS checklist to evaluate the quality of DCE studies, which focuses on five key areas and cannot cover all critical aspects of DCE research, such as the attribute identification and selection process or the use of econometric models. Finally, this review covered publications up to 12 July 2024, and more recent studies may not have been captured.
5. Conclusions
This systematic review synthesized evidence on the treatment preferences of patients, physicians, and caregivers for lung cancer. Existing studies have differences in the coverage of study populations, the scope of attributes, and the research design of experiments. Most DCEs have focused on patients’ preferences for treatment efficacy and adverse effects, with less attention to other attributes that may influence treatment choices. Moreover, there is heterogeneity in the preferences for lung cancer treatment among physicians, patients, and caregivers. Therefore, to better understand and reach consensus on lung cancer treatment among stakeholders, more DCE or other explicit preference studies are needed to provide evidence-based support for personalized lung cancer treatment plans.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F. Laversanne M. Sung H. Ferlay J. Siegel R.L. Soerjomataram I. Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA A Cancer J. Clin.20247422926310.3322/caac.2183438572751 · doi ↗ · pubmed ↗
- 2Ferlay J. Ervik M. Lam F. Laversanne M. Colombet M. Mery L. Piñeros M. Znaor A. Soerjomataram I. Bray F. Global Cancer Observatory: Cancer Today (Version 1.1)International Agency for Research on Cancer Lyon, France 2024 Available online: https://gco.iarc.who.int/today(accessed on 1 August 2024)
- 3Ramalingam S.S. Owonikoko T.K. Khuri F.R. Lung cancer: New biological insights and recent therapeutic advances CA A Cancer J. Clin.2011619111210.3322/caac.2010221303969 · doi ↗ · pubmed ↗
- 4Arbour K.C. Riely G.J. Systemic Therapy for Locally Advanced and Metastatic Non-Small Cell Lung Cancer: A Review JAMA 201932276477410.1001/jama.2019.1105831454018 · doi ↗ · pubmed ↗
- 5Li Y. Yan B. He S. Advances and challenges in the treatment of lung cancer Biomed. Pharmacother.202316911589110.1016/j.biopha.2023.11589137979378 · doi ↗ · pubmed ↗
- 6Miao D. Zhao J. Han Y. Zhou J. Li X. Zhang T. Li W. Xia Y. Management of locally advanced non-small cell lung cancer: State of the art and future directions Cancer Commun.202444234610.1002/cac 2.12505 PMC 1079401637985191 · doi ↗ · pubmed ↗
- 7Meyer M.L. Fitzgerald B.G. Paz-Ares L. Cappuzzo F. Jänne P.A. Peters S. Hirsch F.R. New promises and challenges in the treatment of advanced non-small-cell lung cancer Lancet 202440480382210.1016/S 0140-6736(24)01029-839121882 · doi ↗ · pubmed ↗
- 8Mark T.L. Swait J. Using stated preference and revealed preference modeling to evaluate prescribing decisions Health Econ.20041356357310.1002/hec.84515185386 · doi ↗ · pubmed ↗