Physical Therapists’ Practices and Attitudes Toward Non-Steroidal Anti-Inflammatory Drugs: A National Cross-Sectional Study
Samia A. Alamrani, Wadia S. Alruqayb, Hamad S. Al Amer, Sultan A. Alanazi

TL;DR
This study explores how Saudi physical therapists use and discuss NSAIDs, finding inconsistent practices and a need for better guidelines and education.
Contribution
The study provides new insights into Saudi PTs' NSAID-related practices and attitudes, identifying gaps in knowledge and policy.
Findings
Over half of PTs frequently discuss NSAID use with patients, especially over-the-counter formulations.
Only 14.6% of PTs reported having institutional policies on NSAID discussions.
Most PTs (62%) believe they lack adequate knowledge to provide safe medication advice.
Abstract
Background: Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) are commonly used to manage acute or moderate-to-severe musculoskeletal pain. Physical Therapists (PTs) are involved in patient management from early on, providing education and advice related to medication use. This study aimed to examine Saudi PTs’ practice patterns and attitudes toward NSAID use and to identify factors associated with key practice outcomes by discussing NSAID use, assessing contraindications, monitoring side effects, and documenting discussions. Methods: A cross-sectional study was conducted between February and June 2025. A total of 371 PTs (52.3% male) from all regions of the country participated. Data were collected using an expert-reviewed and pilot-tested self-administered questionnaire. Descriptive statistics, chi-square tests, and logistic regression were used to analyze the data. Qualitative responses…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
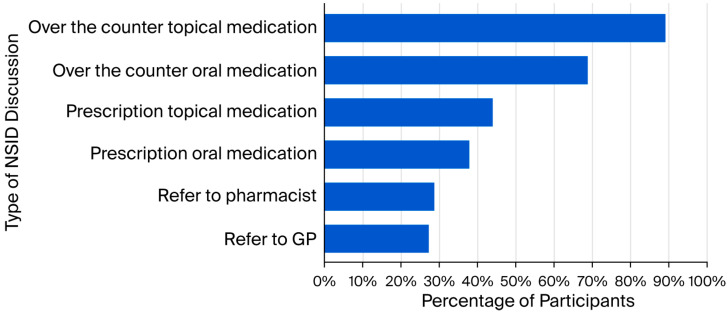 Figure 1
Figure 1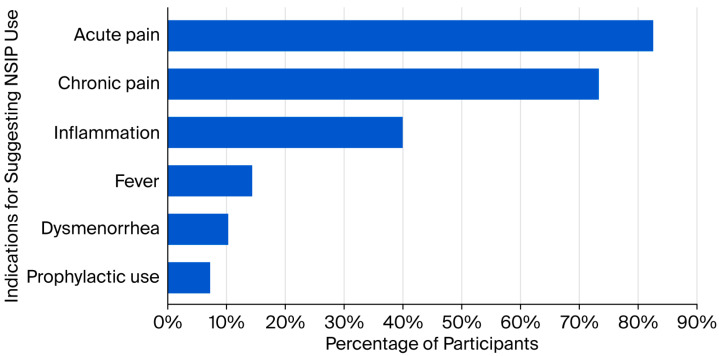 Figure 2
Figure 2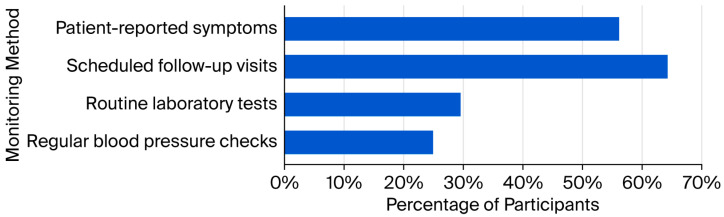 Figure 3
Figure 3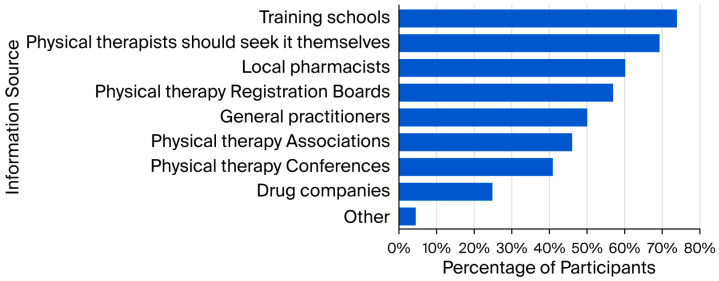 Figure 4
Figure 4- —Deanship of Graduate Studies and Scientific Research, Taif University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory mediators and NSAID effects · Osteoarthritis Treatment and Mechanisms · Contact Dermatitis and Allergies
1. Introduction
Musculoskeletal conditions represent a major health problem, often leading to persistent pain, functional limitations, and long-term disability [1]. Physical Therapists (PTs), as primary practitioners in musculoskeletal rehabilitation, typically utilize non-pharmacological interventions such as therapeutic exercise, manual therapy and patient education as first-line management strategies [2]. However, acute flare-ups or moderate-to-severe musculoskeletal pain may necessitate the incorporation of pharmacological agents, including Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) [3].
NSAIDs are widely used for their analgesic and anti-inflammatory properties [4]. They are also among the most commonly used medications alongside physical therapy interventions, whether prescribed or purchased over the counter [4]. Despite their therapeutic usefulness, NSAIDs are associated with dose- and duration-dependent risks, including gastrointestinal bleeding and ulceration, heightened cardiovascular complications, and renal impairments [5,6]. These potential risks highlight the importance of careful patient screening, accurate dosing, and awareness of drug interactions. Consequently, healthcare professionals involved in pain management must have detailed knowledge of NSAID contraindications and pharmacology, regardless of their prescribing authority.
In Saudi Arabia, the physiotherapy profession has grown considerably in recent decades, with increasing emphasis on evidence-based practice and multidisciplinary models of care [7]. Although PTs in Saudi Arabia cannot prescribe NSAIDs, their role as primary contact practitioners and patient educators places them in a strategic position to influence patients’ understanding, adherence, and safe use of these medications [8]. PTs are often responsible for integrating medication-related considerations into a patient’s active rehabilitation plan, identifying contraindications, and communicating medication-related concerns with prescribing physicians or pharmacists [9]. Research from international settings indicates that a significant number of patients undergoing physical therapy are concurrently taking NSAIDs [10,11], yet studies consistently highlight considerable variability and occasional gaps in PTs’ knowledge and confidence regarding pharmacological pain management [12,13,14]. Such variations underscore the need for context-specific evaluations.
Despite the critical role of PTs in the multidisciplinary pain management, there is a lack of data concerning their clinical practices and professional attitudes towards NSAIDs in the Kingdom of Saudi Arabia. Understanding such aspects is essential to improving patient safety, informing professional development and curriculum planning, and strengthening interprofessional care strategies [15]. Therefore, the primary objective of this study was to examine the clinical practices and professional attitudes of PTs practicing in Saudi Arabia regarding NSAID use in the management of musculoskeletal conditions. The secondary objective was to identify factors associated with their involvement in NSAID-related clinical practices. Specifically, this study sought to answer the following research questions: What are the current practice patterns and attitudes of Saudi PTs toward NSAID use, and which demographic or professional factors are associated with their involvement in NSAID-related clinical practices?
2. Materials and Methods
This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations [16] (Supplementary File S1). A cross-sectional study design was employed, using an online, self-administered questionnaire to assess PTs’ practices and attitudes toward NSAIDs. The survey was distributed to certified PTs across Saudi Arabia between February and June 2025.
2.1. Participants
Certified PTs currently living and working in Saudi Arabia across all settings were invited to participate. Consent was obtained electronically through the survey platform (Google Forms). Sample size was calculated using OpenEpi software (Version 3.01) [17], assuming a 95% confidence interval, 50% expected proportion, and 5% margin of error, yielding a target of 365 participants.
Inclusion criteria: Licensed male and female PTs practicing in Saudi Arabia who provided informed consent.
Exclusion criteria: Interns, physiotherapy assistants/technicians, retired professionals, and individuals who did not complete the questionnaire.
2.2. Measures
Questionnaire
The questionnaire was developed following a review of the relevant literature [12,18,19]. Initial items were generated based on previously published instruments and concepts relevant to NSAID-related practices and attitudes among healthcare professionals. To establish face and content validity, the draft questionnaire was reviewed by an expert panel consisting of three senior physical therapy academics with 10–18 years of clinical and research experience and one clinical pharmacist with 14 years of clinical and research experience. The panel qualitatively evaluated the questionnaire for clarity, relevance, and comprehensiveness and alignment with study objectives. Feedback was obtained through iterative discussion, and items were revised based on consensus recommendations. No formal quantitative content validity index was calculated. Prior to data collection, a pilot study was conducted with 10 practicing PTs to assess clarity, readability, and applicability. Minor modifications were made accordingly (Supplementary File S2). Data from the pilot study were not included in the final analysis.
The final questionnaire comprised four sections: consent and study information, demographics (11 items including age, sex, region, years of experience, and specialization), practice patterns (11 items assessing discussion of NSAID use, adherence to policy, patient assessment, and monitoring) and attitudes (4 items, including 3 closed and 1 open-ended question). For the purposes of this study, the term “discuss” referred to medication-related conversations conducted within existing scope-of-practice boundaries, whereas “prescribing” referred solely to participants’ attitudes toward hypothetical prescribing authority.
Formal psychometric reliability testing (e.g., internal consistency using Cronbach’s alpha or test–retest reliability) was not conducted, as the questionnaire primarily consisted of descriptive and standalone items rather than multi-item scales measuring latent constructs.
2.3. Data Collection
Ethical approval was obtained from the Ethics Committee at Taif University, Saudi Arabia (46-155). All participants provided informed consent prior to their inclusion in the study. Participation was voluntary, and respondents were informed of their right to withdraw at any time without any consequences. To ensure confidentiality, all data were collected anonymously, and no identifiable personal information was recorded. The questionnaire was hosted on Google Forms and distributed via social media (X, Telegram, and WhatsApp), emails, PT forums and professional associations using a snowball sampling approach. Data were collected anonymously and cleaned prior to analysis.
2.4. Statistical Analysis
Data were analyzed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics summarized participant characteristics, practice patterns, and attitudes. Differences across categorical variables were assessed using chi-square tests (p < 0.05 considered significant).
Binary logistic regression was conducted to identify factors associated with key practice outcomes (discussing NSAID use, assessing contraindications, monitoring side effects, and recording discussions in clinical records). Both univariate models (crude odds ratios [COR] with 95% confidence intervals [CI]) and multivariate models (adjusted odds ratios [AOR] with 95% CI) were used. Variables with p < 0.05 were considered statistically significant factors.
Multicollinearity was assessed using variance inflation factor (VIF), with a threshold of ≤5 indicating acceptable levels [20]. The VIF values ranged from 1.01 to 1.70 and were well below the cutoff of 5, suggesting the absence of multicollinearity.
Open-ended responses were analyzed thematically and categorized as supportive, opposing, or neutral/uncertain, with illustrative quotations included in the results.
3. Results
3.1. Participant Characteristics
A total of 371 PTs participated in the study; their mean age was 33.3 years (SD = 6.67). Slightly more than half were males (52.3%), while females represented 47.7%. Participants represented all regions of Saudi Arabia and varied in terms of gender, employment sector, level of experience, academic qualifications, and clinical specializations. The Western region contributed the largest proportion of respondents. Most participants held a bachelor’s degree and worked in public or private clinical settings, with orthopedics and neurology being the most common specialties. Detailed characteristics are presented in Table 1.
3.2. Practice Characteristics Regarding NSAID Use
A significant proportion (n = 178; 48.0%) reported that their institution had no formal policy on NSAID-related discussions, compared with only 14.6% (n = 54) who reported the presence of a policy (χ^2^ = 65.02; p < 0.001). Among those with a policy, almost all (n = 51; 94.4%) stated that they follow it (χ^2^ = 42.67; p < 0.001). Of those without a policy or who were unsure, more than two thirds (n = 217; 68.5%) believed that such a policy would be beneficial (χ^2^ = 178.39; p < 0.001).
More than half of participants (n = 219; 59.0%) frequently discussed NSAID use with their patients, compared with 41.0% (n = 152) who did not (χ^2^ = 12.10; p < 0.001). As depicted in Figure 1, this discussion most often involved over-the-counter topical (n = 193; 88.1%) and oral medications (n = 149; 68.0%), followed by prescription topical (n = 95; 43.4%) and oral medications (n = 82; 37.4%), pharmacist referral (n = 62; 28.3%), and general practitioner referral (n = 59; 26.9%).
Nearly half (n = 176; 47.4%) of PTs indicated that they never suggest NSAID use, while 26.1% (n = 97) reported doing so daily (χ^2^ = 228.8; p < 0.001). Smaller proportions reported suggesting NSAID use rarely (13.7%, n = 51), weekly (10.2%, n = 38), and monthly (2.4%, n = 9). The distribution was statistically significant (χ^2^ = 228.88, p < 0.001). As shown in Figure 2, suggestions for use were most commonly acute pain (n = 161; 82.6%) and chronic pain (n = 143; 73.3%), with fewer citing inflammation (n = 78; 40.0%), fever (n = 28; 14.4%), dysmenorrhea (n = 20; 10.3%), or prophylactic use (n = 14; 7.2%).
No significant difference was found between the proportion of participants who assessed contraindications before suggesting NSAID use (n = 172; 46.4%) and those who did not (n = 199; 53.6%) (χ^2^ = 1.97; p = 0.161). Only 29.4% (n = 109) monitored patients on long-term NSAIDs for side effects, compared with 70.6% (n = 262) who did not (χ^2^ = 63.10; p < 0.001). As shown in Figure 3, monitoring strategies included follow-up visits (n = 70; 64.2%), patient-reported symptoms (n = 61; 56.0%), laboratory tests (n = 32; 29.4%), and blood pressure checks (n = 27; 24.8%).
Finally, less than one third (n = 111; 29.9%) recorded discussions on medications in their clinical records, compared with 70.1% (n = 260) who did not (χ^2^ = 59.84; p < 0.001).
Scope of Discussing NSAID Use
Most PTs reported including indications when discussing NSAID use with their patients (n = 273; 73.6% vs. n = 98; 26.4%) (χ^2^ = 82.55; p < 0.001). In contrast, a substantial proportion did not address drug interactions (n = 240; 64.7%) compared with those who did (n = 131; 35.3%) (χ^2^ = 82.55; p < 0.001).
There was no significant difference between those who provided and did not provide warnings/advice (n = 203; 54.7% vs. n = 168; 45.3%) (χ^2^ = 3.30; p = 0.069), precautions (n = 179; 48.2% vs. n = 192; 51.8%) (χ^2^ = 0.46; p = 0.500), contraindications (n = 170; 45.8% vs. n = 201; 54.2%) (χ^2^ = 2.59; p = 0.108), side effects (n = 172; 46.4% vs. n = 199; 53.6%) (χ^2^ = 1.97; p = 0.161), or dosage information (n = 185; 49.9% vs. n = 186; 50.1%) (χ^2^ = 0.003; p = 0.959).
3.3. Associations Between Participant Characteristics and NSAID-Related Practices
3.3.1. Discussing NSAID Use with Patients
In the univariate analysis (Table 2), male PTs were more likely than females to discuss NSAID use with patients (COR = 2.01, 95% CI: 1.32–3.06). Longer experience (1–5 years: COR = 2.64, 95% CI: 1.24–5.62; 6–10 years: COR = 2.82, 95% CI: 1.28–6.20; ≥11 years: COR = 3.69, 95% CI: 1.67–8.14), postgraduate degrees (COR = 5.45, 95% CI: 1.05–28.32), and orthopedic (COR = 2.04, 95% CI: 1.09–3.81), neurological (COR = 2.44, 95% CI: 1.21–4.89), and sports (COR = 2.40, 95% CI: 1.08–5.35) specializations were also significant predictors. In the multivariate model, male therapists (AOR = 1.72, 95% CI: 1.09–2.73) and those with 1–5 years (AOR = 2.44, 95% CI: 1.04–5.60) and ≥11 years of experience (AOR = 3.77, 95% CI: 1.31–10.86) remained significantly more likely to discuss NSAIDs, with bachelor’s degree (AOR = 6.92, 95% CI: 1.18–40.76) emerging as a significant factor.
3.3.2. Assessing Contraindications Before Suggesting NSAID Use
In univariate analysis (Table 3), assessing contraindications was associated with Central region (COR = 2.36, 95% CI: 1.10–5.07), university facility (COR = 2.71, 95% CI: 1.52–4.84), Doctor of PT degree (COR = 18.20, 95% CI: 1.76–188.07), postgraduate degree (COR = 12.71, 95% CI: 1.51–107.21), and neurological (COR = 2.27, 95% CI: 1.12–4.60) and sports (COR = 2.40, 95% CI: 1.08–5.35) specializations. Only Doctor of PT degree (AOR = 11.46, 95% CI: 11.01–130.08) remained significant in the multivariate model.
3.3.3. Monitoring Side Effects of Long-Term NSAID Use
In terms of monitoring long-term side effects, univariate analysis (Table 4) showed significant associations with Central region (COR = 4.01, 95% CI: 1.52–10.58) and orthopedic (COR = 3.57, 95% CI: 1.42–8.97), neurological (COR = 3.39, 95% CI: 1.28–8.95) pediatric (COR = 6.55, 95% CI: 2.06–20.84), geriatric (COR = 5.95, 95% CI: 1.43–24.78), and sports specialists (COR = 5.65, 95% CI: 2.02–15.81) specializations. In the multivariate model, therapists with 6–10 years of experience were less likely to monitor (AOR = 0.27, 95% CI: 0.09–0.80), while orthopedic (AOR = 3.49, 95% CI: 1.24–9.84), pediatric (AOR = 7.39, 95% CI: 1.99–27.42), geriatric (AOR = 4.83, 95% CI: 1.03–22.73), and sports specialists (AOR = 5.65, 95% CI: 1.77–17.99) were significantly more likely to monitor side effects compared with general practitioners.
3.3.4. Recording Discussions on Medications
Univariate analysis indicated that Central (COR = 3.17, 95% CI: 1.26–8.01) and Northern regions (COR = 3.17, 95% CI: 1.17–8.60), university facilities (COR = 3.34, 95% CI: 1.86–6.01), and pediatric specialization (COR = 2.88, 95% CI: 1.04–7.95) were associated with higher odds of recording medication discussions. In the multivariate model, Central region (AOR = 2.87, 95% CI: 1.06–7.77) and university facility (AOR = 2.41, 95% CI: 1.18–4.94) remained significant predictors (Table 5).
3.4. Attitudes Toward NSAID Usage
A significant proportion of participants believed that PTs should hypothetically be able to prescribe NSAIDs (n = 141; 38.0%), compared with those who disagreed (n = 100; 27.0%), while more than one third (n = 130; 35.0%) were uncertain (χ^2^ = 7.28; p = 0.026). At the same time, most participants reported that their current knowledge was insufficient to advise patients on the safe use of NSAIDs (n = 230; 62.0%), and a further 26.1% (n = 97) were unsure (χ^2^ = 148.50; p < 0.001).
Regarding responsibility for providing NSAID-related information to PTs, the majority identified training schools (n = 274; 73.9%), followed by self-directed learning (n = 257; 69.3%), local pharmacists (n = 223; 60.1%), registration boards (n = 211; 56.9%), general practitioners (n = 186; 50.1%), professional associations (n = 171; 46.1%), and conferences (n = 152; 41.0%). Fewer participants considered drug companies (n = 92; 24.8%) or other sources (n = 17; 4.6%) as responsible (Figure 4).
Of the 371 participants, 75 (20.2%) responded to the open-ended question on attitudes toward NSAIDs. Among these, 46.7% expressed supportive views, emphasizing their effectiveness in reducing pain and inflammation as adjuncts to physical therapy. Representative comments included:
“I worked on myself to build up knowledge about it, thus I feel confident to advise patients”.
In contrast, 17.3% were opposed, citing safety issues, scope-of-practice concerns, and need for further training. Examples included the following:
“PTs should be able to prescribe NSAIDs, but only after sufficient training and passing a licensing exam”.
The remaining 36.0% provided neutral or uncertain responses, reflecting a lack of knowledge and a tendency to rely on referral. Typical statements included:
“I believe I am lacking information about these medications, which impacts my confidence. I often refer patients to doctors or pharmacists”.
Overall, while nearly half of the responding PTs expressed positive views toward NSAID use as part of physical therapy care, a substantial number emphasized regulatory limitations, safety concerns, or the need for additional education before wider adoption in practice.
4. Discussion
To the best of the authors’ knowledge, this is the first nationwide study to comprehensively examine the practices and professional attitudes of PTs in Saudi Arabia regarding NSAID use in musculoskeletal care. The findings demonstrate that, although PTs in Saudi Arabia do not have prescribing authority, they are frequently involved in discussing, educating, and advising patients about NSAIDs as part of routine clinical practice. This highlights PTs’ expanding role as primary contact practitioners and their growing influence on patients’ medication-related decisions. However, the results also reveal important gaps in safety practices, documentation, and pharmacological knowledge that warrant critical attention. These insights also have broader relevance for countries where PTs function as first-contact practitioners.
More than half of the participating PTs reported routinely discussing NSAID use with patients, predominantly over-the-counter topical and oral formulations. This pattern is consistent with international evidence showing that PTs commonly discuss NSAIDs in additions to manual therapy and exercise, particularly in the management of acute and chronic musculoskeletal pain [9,21,22]. Despite this involvement, substantial safety concerns were identified. Less than half of PTs reported screening patients for contraindications, and fewer than one third monitored patients using NSAIDs in the long term. Furthermore, documentation of medication-related discussions was uncommon. These findings are concerning given the well-established gastrointestinal, renal, and cardiovascular risks associated with NSAIDs, particularly with prolonged use or in vulnerable populations [23]. In addition to systemic safety concerns, experimental evidence suggests that NSAIDs may influence biological processes related to tissue healing. For example, animal studies have demonstrated that selective COX-2 inhibitors can impede bone and tendon-to-bone healing and reduce prostaglandin-mediated signaling essential for tissue repair [24]. Furthermore, basic science research indicates that NSAIDs may negatively affect cellular proliferation and collagen synthesis in soft tissues, which are critical for musculoskeletal recovery [25]. While the current study did not explicitly measure PTs’ knowledge of these biological healing mechanisms, the observed gaps in monitoring suggest a potential lack of awareness regarding how NSAIDs influence the physiological stages of rehabilitation beyond simple pain modulation. The limited monitoring and documentation observed suggest that NSAID-related discussions may often be informal, inconsistently structured, and insufficiently integrated into clinical records.
While most PTs reported providing information about indications, fewer addressed drug interactions, precautions, side effects, or dosage. This selective counseling may reflect partial pharmacological knowledge or uncertainty about professional boundaries. Similar gaps have been reported internationally, where PTs reported low confidence in advising on drug interactions and contraindications [26,27]. The absence of formal pharmacology training in many physical therapy programs may contribute to this gap, limiting PTs’ ability to provide comprehensive patient education [15,28].
The likelihood of discussing NSAID use was higher among male PTs and those with greater clinical experience, which aligns with literature linking experience to increased confidence and autonomy in clinical decision-making [29]. PTs with orthopedic, neurological, and sports specializations were more likely to discuss NSAID use, likely reflecting greater exposure to pain-intensive conditions where adjunctive symptom management is common [18].
Notably, PTs working in university-affiliated facilities demonstrated better practices in assessing contraindications and recording medication discussions. This finding emphasize the role of academic settings in promoting evidence-based clinical practice [19].
Monitoring of long-term NSAID use was more common among pediatric, geriatric, and sports specialists, which may indicate heightened awareness of medication risks in vulnerable populations [30]. However, the overall low monitoring rates suggest that structured follow-up mechanisms and interprofessional collaboration remain insufficient across practice settings.
Attitudinal findings reveal considerable uncertainty within the physical therapy profession. Although over one third of participants supported the inclusion of clinical guidance on NSAIDs as part of physical therapy care, the majority reported insufficient knowledge to provide safe advice. This mismatch between clinical involvement and perceived competence raises important concerns about patient safety and professional accountability [31].
Qualitative responses (20%) further illustrated this tension. Supportive PTs described confidence gained through self-directed learning and collaboration with physicians or pharmacists, while others expressed reluctance due to safety concerns and scope-of-practice limitations. Neutral responses reflected uncertainty and reliance on referral, highlighting variability in confidence and preparedness across practitioners. These findings are similar to those reported from the United Kingdom, where early implementation of prescribing rights for PTs was met with similar uncertainty until structured competency frameworks were introduced [29]. Saudi PTs appear to have similar goals, but they do not have the systematic framework needed to carry them out safely.
Participants predominantly attributed responsibility for NSAID-related education to training institutions and self-learning, emphasizing gaps in structured continuing professional development. International experience suggests that embedding pharmacological modules into undergraduate and Continuing Professional Development. (CPD) curricula enhances PTs’ readiness to manage pain collaboratively [18,32,33].
4.1. Clinical Implications
Undergraduate and postgraduate curricula could benefit from greater emphasis on pharmacovigilance, particularly regarding the identification of adverse effects and contraindications screening. Developing structured workshops or certification programs may further support PTs in providing evidence-based medication guidance.Healthcare facilities might consider establishing formal framework to guide NSAID-related discussions within physical therapy departments. Standardizing documentation and education protocols could help ensure that patient guidance is provided safely and consistently across all practice settings.There is an opportunity to enhance communication between PTs, pharmacists, and physicians to better coordinate pain management. By identifying risks in patients who self-medicate with over-the-counter (OTC) NSAIDs, PTs can potentially serve as a vital link in the interprofessional team, facilitating safer patient outcomes through formal referral pathways.
4.2. Strength and Limitations
This study represents the first nationwide assessment of Saudi PTs’ practices and attitudes toward NSAID use, adding important knowledge to the regional literature. The inclusion of a large, geographically diverse sample from various regions enhances the representativeness of the results, while comprehensive assessment of multiple NSAID-related behaviors—including discussing indications, screening for contraindication, monitoring side effects, and documenting conversation—provides a comprehensive understanding of clinical practices.
Nonetheless, several limitations should be acknowledged. The cross-sectional design precludes causal relationships between predictors and behaviors. Although the study achieved nationwide reach, the use of snowball sampling via social media may have introduced selection bias toward digitally active therapists, potentially limiting the findings’ generalizability to the broader Saudi PT workforce. Although the questionnaire was expert-reviewed and pilot-tested, the absence of formal psychometric evaluation may affect its measurement robustness. In addition, the instrument primarily focused on clinical practices and safety-related behaviors and did not comprehensively assess physiotherapists’ knowledge of NSAIDs’ biological effects on tissue healing, which may limit the interpretation of rehabilitation implications. Furthermore, the low response rate to the open-ended question suggests that the qualitative findings should be interpreted with caution, as they may not fully capture the diverse perspectives of the entire sample. Finally, reliance on self-reported data may have introduced recall or social desirability bias. Therefore, future studies may use objective clinical assessment or intervention-based designs to validate self-reported practices and assess the impact of targeted pharmacology education on PTs’ competence and confidence.
5. Conclusions
PTs in Saudi Arabia take an active role in NSAID-related guidance without any institutional support or training. While many PTs express positive attitudes towards integrating medication knowledge into practice, there are significant safety and ethical concerns due to gaps in knowledge, regulations, and documentation. To address these gaps and provide evidence-based, patient-centered care for musculoskeletal pain management, coordinated efforts in education, policy making, and interprofessional collaboration are needed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jiang F. Lu C. Zeng Z. Sun Z. Qiu Y. Global Burden of Disease for Musculoskeletal Disorders in All Age Groups, from 2024 to 2050, and a Bibliometric-Based Survey of the Status of Research in Geriatrics, Geriatric Orthopedics, and Geriatric Orthopedic Diseases J. Orthop. Surg. Res.20252017910.1186/s 13018-025-05580-y 39972346 PMC 11841256 · doi ↗ · pubmed ↗
- 2Ezzatvar Y. Dueñas L. Balasch-Bernat M. Lluch-Girbés E. Rossettini G. Which Portion of Physiotherapy Treatments’ Effect Is Not Attributable to the Specific Effects in People with Musculoskeletal Pain? A Meta-Analysis of Randomized Placebo-Controlled Trials J. Orthop. Sports Phys. Ther.20245439139910.2519/jospt.2024.1212638602164 · doi ↗ · pubmed ↗
- 3Turkistani A. A Systematic Review of Pharmacological Interventions for Chronic Pain Management S. East. Eur. J. Public Health 2024 XXIII 61963410.70135/seejph.vi.1454 · doi ↗
- 4Biederman R.E. Pharmacology in Rehabilitation: Nonsteroidal Anti-Inflammatory Agents J. Orthop. Sports Phys. Ther.20053535636710.2519/jospt.2005.35.6.35616001907 · doi ↗ · pubmed ↗
- 5Sohail R. Mathew M. Patel K. Reddy S. Haider Z. Naria M. Habib A. Abdin Z. Chaudhry W. Akbar A. Effects of Non-Steroidal Anti-Inflammatory Drugs (NSAI Ds) and Gastroprotective NSAI Ds on the Gastrointestinal Tract: A Narrative Review Cureus 202315 e 3708010.7759/cureus.3708037153279 PMC 10156439 · doi ↗ · pubmed ↗
- 6Pham H. Spaniol F. The Efficacy of Non-Steroidal Anti-Inflammatory Drugs in Athletes for Injury Management, Training Response, and Athletic Performance: A Systematic Review Sports 20241230210.3390/sports 1211030239590904 PMC 11598303 · doi ↗ · pubmed ↗
- 7Al-Abbad H.M. Al-Haidary H.M. The Perception of Physical Therapy Leaders in Saudi Arabia Regarding Physical Therapy Scope of Practice in Primary Health Care J. Phys. Ther. Sci.20162811211710.1589/jpts.28.11226957740 PMC 4755986 · doi ↗ · pubmed ↗
- 8Alodaibi F.A. Alotaibi M.A. Almohiza M.A. Alhowimel A.S. Physical Therapists’ Role in Health and Wellness Promotion for People with Musculoskeletal Disorders: A Cross-Sectional Description Study Conducted in Saudi Arabia J. Multidiscip. Healthc.20221556757610.2147/JMDH.S 35693235378741 PMC 8976574 · doi ↗ · pubmed ↗