Pulmonary Hemorrhage and Pneumothorax Risk During CT-Guided Lung Biopsy for Suspected Lung Cancer
Rosa Alba Pugliesi, Nour Maalouf, Giuseppe Gullo, Andreas H. Mahnken, Jonas Apitzsch

TL;DR
This study found that limited bleeding during lung biopsies may reduce the risk of lung collapse, especially for deeper lung lesions.
Contribution
The study reveals a novel inverse relationship between pulmonary hemorrhage and pneumothorax risk during CT-guided lung biopsies.
Findings
Pneumothorax occurred less frequently in patients with pulmonary hemorrhage.
Lesion depth showed a borderline association with pneumothorax risk, which was potentially attenuated by hemorrhage.
Abstract
CT-guided lung biopsy is widely used to diagnose suspected lung cancer and to guide treatment decisions such as surgery, radiotherapy, and immunotherapy. Pneumothorax, a collapse of the lung caused by air leakage, is the most common complication of this procedure. Pulmonary hemorrhage, which appears as localized bleeding around the biopsy site, is usually considered an adverse event. In this retrospective study of 118 patients undergoing CT-guided lung biopsy for suspected or confirmed lung cancer, we found that pneumothorax occurred less frequently in patients who developed pulmonary hemorrhage. Our results suggest that limited hemorrhage may partially seal the biopsy tract and reduce air leakage, especially in deeper lung lesions. Understanding this interaction may help improve biopsy safety, reduce procedure-related delays, and support timely initiation of cancer treatments.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
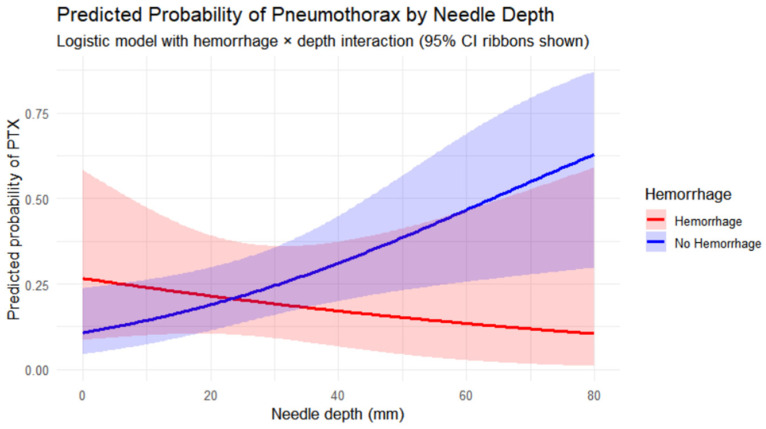 Figure 1
Figure 1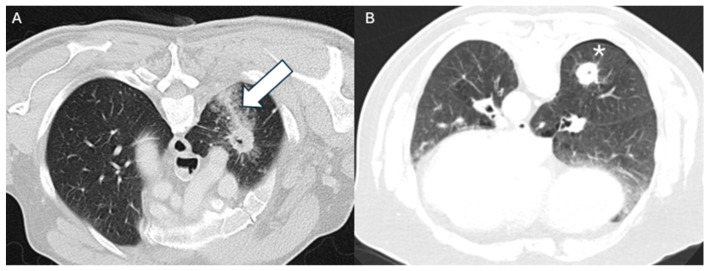 Figure 2
Figure 2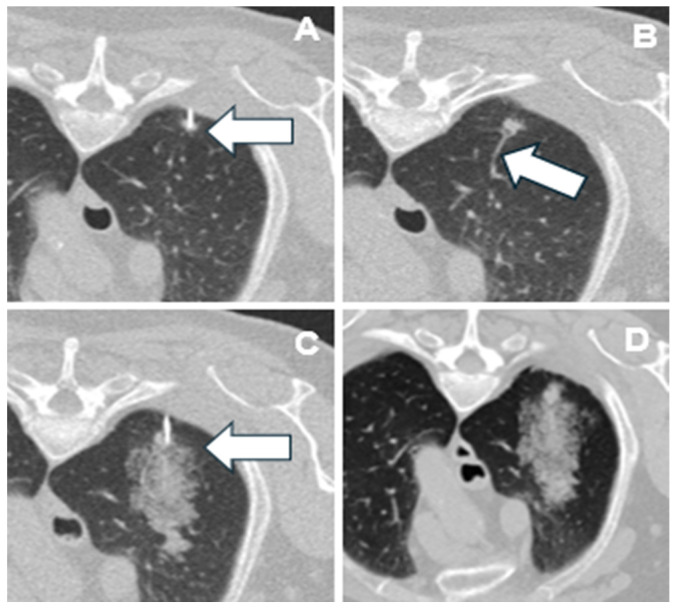 Figure 3
Figure 3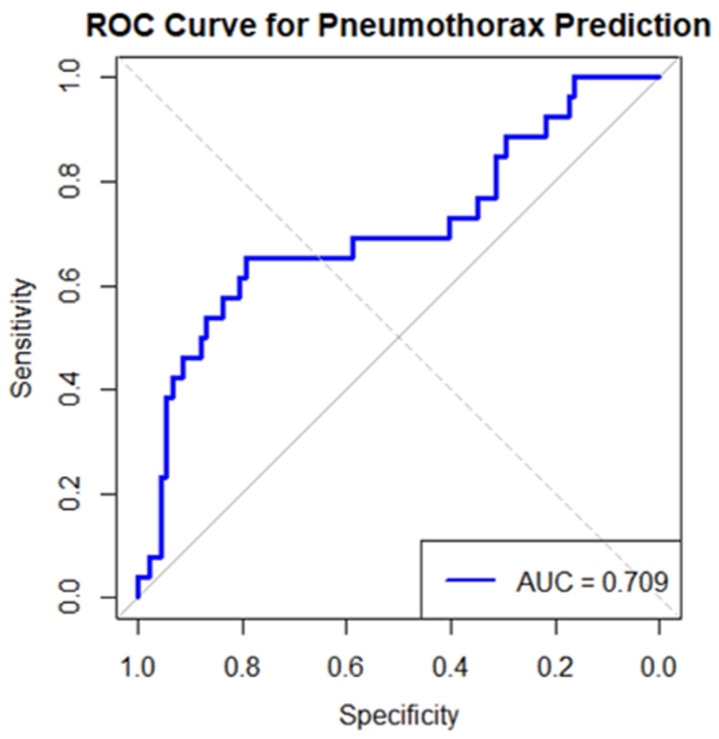 Figure 4
Figure 4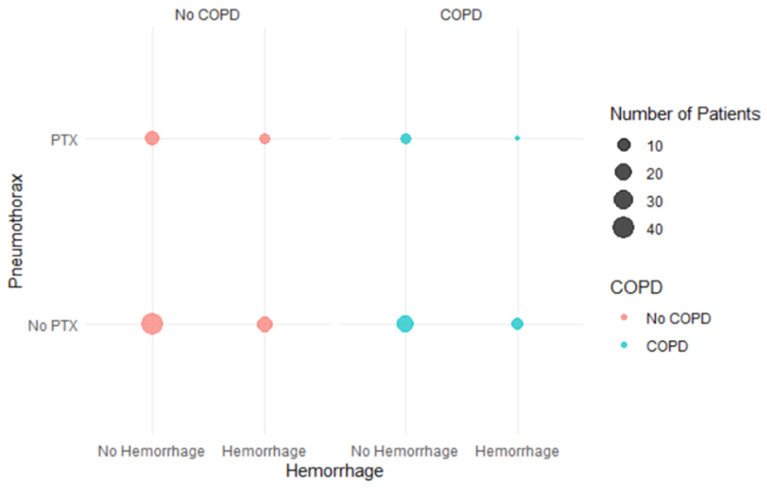 Figure 5
Figure 5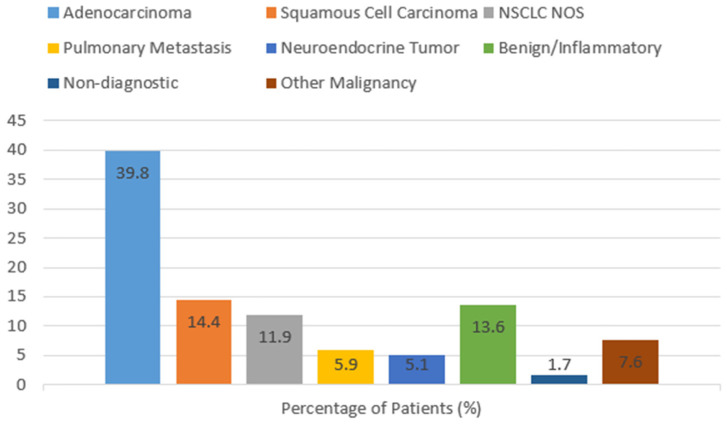 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Diagnosis and Treatment · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Radiomics and Machine Learning in Medical Imaging
1. Introduction
Lung cancer is the predominant cause of cancer-related mortality worldwide, leading to a rising demand for minimally invasive diagnostic techniques, with more than two million new cases diagnosed annually [1]. The widespread implementation of molecular profiling and precision oncology has markedly increased the incidence of CT-guided lung biopsies performed for initial diagnosis and treatment stratification [2]. Consequently, improving the safety profile of CT-guided transthoracic needle biopsy (TTNB) has become a clinically important objective [3].
TTNB is a crucial minimally invasive technique for detecting pulmonary nodules, masses, and ground-glass opacities in individuals with suspected lung cancer [4]. The precise histological and molecular characterization obtained by TTNB is essential for personalized cancer treatment, guiding the selection and sequence of radiation, immunotherapy, targeted therapy, and surgical interventions [5]. In precision oncology, procedural challenges may obstruct therapy or limit appropriate treatment options, making the safety and reliability of diagnostic techniques crucial [6]. Although pulmonary hemorrhage typically manifests as perilesional or intrapulmonary bleeding and often resolves spontaneously, pneumothorax (PTX) may necessitate chest tube placement and prolonged hospitalization, potentially complicating cancer staging, radiation planning, or surgical interventions [7,8].
Given that numerous patients qualify for multimodal treatment strategies encompassing surgery, radiation, and immunotherapy, mitigating biopsy-related complications is particularly crucial within the framework of multidisciplinary lung cancer management [9]. Delays or cancellations caused by PTX may negatively impact treatment schedules and overall cancer results. Traditionally, PTX and pulmonary hemorrhage have been regarded as independent complications; however, emerging evidence suggests a possible inverse relationship between them [10,11,12,13]. Immediate post-biopsy pulmonary bleeding has been linked to decreased PTX rates [14], suggesting that it may seal the biopsy tract and reduce alveolar air leakage [4,11,12].
Deeper, peripheral lesions, commonly targeted for stereotactic radiation or minimally invasive surgical excision, have a higher intrinsic risk of PTX, making this protective relationship of relevance in oncologic imaging. Determining if pulmonary bleeding alters this risk could guide biopsy planning procedures that facilitate subsequent cancer therapy.
Unlike our prior studies [15,16,17], which concentrated on technical standardization, needle angulation within an 80–100° safe zone and organized post-biopsy monitoring protocols to mitigate PTX incidence, the current study examines whether pulmonary hemorrhage may biologically influence PTX risk.
While demographic factors, COPD status, lesion size, patient positioning, and procedural standardization have already been systematically evaluated in our prior publications [15,16,17], the current analysis specifically explores the interaction between pulmonary hemorrhage and lesion depth in an oncologic cohort. Rather than re-examining established predictors, this study was designed to investigate whether tract-related hemorrhage exerts a potential tamponade-like effect that attenuates depth-associated PTX risk.
A methodologically oriented study that emphasized predictive modeling and risk stratification of biopsy complications has previously analyzed a partially overlapping cohort from our institution [18]. In contrast, the current study examines the relationship between pulmonary hemorrhage and PTX, with a focus on a possible depth-dependent protective interaction, in order to answer a clinical and mechanistic question. Rather than enhancing predictive algorithms, the objective of the present study is to offer clinically interpretable insights into complication mechanisms that are pertinent to cancer treatment workflows and procedural decision-making.
Bronchoscopic procedures, although associated with lower PTX risk, demonstrate lower diagnostic accuracy than TTNB for peripheral pulmonary lesions, including early-stage lung cancers or oligometastatic disease [19]. TTNB is crucial in lung cancer management, emphasizing the necessity for improved risk classification and complication mitigation [20,21].
This study explores the correlation between pulmonary hemorrhage and PTX in individuals undergoing oncologic CT-guided lung biopsy. We hypothesized that pulmonary hemorrhage reduces the depth-related risk of PTX, thereby enabling safer diagnostic access to lesions pertinent for radiotherapy targeting, immunotherapy decision-making, and surgical planning. Using multivariable logistic regression, we sought to characterize this relationship and contribute clinically meaningful data, including borderline and negative findings, to the optimization of diagnostic pathways in lung cancer therapy. Although COPD and other established predictors were not the primary focus of this investigation, they were incorporated into the regression model as adjustment variables. Additionally, exploratory subgroup analyses were performed to assess whether the hemorrhage–PTX relationship differed within clinically relevant subpopulations such as patients with COPD.
2. Materials and Methods
A retrospective single-center cohort study was performed in 118 consecutive patients (66 men, 52 women; median age: 69 years, range: 49–90 years) who had undergone CT-guided transthoracic lung biopsy between 9 January 2020 and 4 April 2025. All biopsies were performed by a single board-certified interventional radiologist with 18 years’ experience, minimizing inter-operator variation. The study was approved by the Institutional Ethics Committee of the Landesärztekammer Baden-Württemberg, Germany (approval number F-2021-038), and all procedures were conducted in accordance with the Declaration of Helsinki. All participants were informed about the intervention more than 24 h in advance and provided written informed consent.
Patients were sampled from an institutional radiology database by procedural code for CT-guided biopsies. All patients with adequate follow-up imaging and in the absence of a pre-existing chest tube were considered for inclusion. COPD was defined based on clinical diagnosis corroborated by imaging evidence of emphysema. Spirometric data were available for 62% of patients; where absent, imaging features (centrilobular or paraseptal emphysema) were used as surrogate criteria.
Data collected included demographics (age, sex), lesion features (size in mm, distance from pleural surface in mm), and presence of existing COPD. Histopathological diagnoses were derived from pathology reports. Only pathology records relating to CT-guided biopsy were used.
Only intrapulmonary lesions were included; mediastinal or pleural-based targets were excluded. All cases were evaluated pre-procedurally by a thoracic radiologist and classified as unsuitable for bronchoscopy due to peripheral location, absence of bronchial access, or lesion size. Biopsies were performed for suspected malignancy, metastatic lesions, or atypical infectious/inflammatory disease.
Standardized definitions were applied: PTX was defined as any pleural air collection visible on immediate or delayed post-biopsy CT; pulmonary hemorrhage as high-attenuation perilesional or intrapulmonary opacities on immediate post-biopsy CT; chest drainage as chest tube placement performed immediately after the procedure or during hospitalization; and needle path length as the manually measured distance from the pleural puncture site to the lesion center on CT. The primary outcome was PTX (yes/no), the key independent variable was pulmonary hemorrhage (yes/no), and secondary outcomes included the need for chest drainage as well as the interaction between hemorrhage and lesion depth.
Given that COPD status, patient positioning, demographic variables, and technical standardization effects have been comprehensively analyzed in our previous institutional studies, the present investigation did not aim to re-establish these predictors. Instead, these variables were included in the multivariable model as adjustment covariates to isolate the independent association between pulmonary hemorrhage and PTX.
No formal sample size calculation was performed prior to data collection due to the retrospective design. With 26 PTX events among 118 patients, the number of outcome events relative to included covariates may limit statistical power, particularly for interaction testing. This is acknowledged as a methodological limitation. In addition to multivariable modeling, subgroup analyses were performed in patients with COPD to evaluate whether the association between pulmonary hemorrhage and PTX differed within this high-risk population. These analyses were considered exploratory due to limited sample size.
2.1. Biopsy Needle and Trocar
An 18G semi-automatic Tru-Cut biopsy needle with a notched inner stylet and sliding outer sheath was used through a 17G coaxial trocar (Möller Medical GmbH, Fulda, Germany). The coaxial system permitted multiple tissue samples through a single pleural puncture, minimizing trauma and improving diagnostic yield.
2.2. Biopsy Protocol
All procedures followed a standardized protocol including sterile preparation, local anesthesia with 1% mepivacaine, and a single pleural puncture. Needle trajectory was planned using pre-biopsy imaging and executed with the patient in prone or supine position depending on lesion location. Sequential CT guidance (64-slice Siemens Somatom Edge, 2 mm slice thickness, end-expiratory breath-hold, no contrast) was used to confirm needle placement. A single pleural pass was targeted in all cases, with the needle placed as perpendicular to the pleura as feasible. Biopsy duration was kept under six minutes. No prophylactic blood patches were used. Tissue samples were fixed in formaldehyde and sent for histopathology.
All patients underwent immediate post-biopsy low-dose CT, acquiring just a short z-axis volume of the area biopsied, to detect complications. Follow-up imaging within 7 days was performed if patients developed new symptoms or signs suggestive of delayed complications.
2.3. Statistical Analysis
Continuous variables were presented as mean ± standard deviation (SD) or median (range), while categorical variables were presented as counts and percentages. Association between hemorrhage and PTX was tested by Chi-square or Fisher’s exact tests for categorical variables and t-tests or Mann–Whitney U tests for continuous variables, based on distribution.
A multivariable logistic regression model was constructed with PTX as the outcome variable. Independent predictors included pulmonary hemorrhage, lesion size, lesion depth (needle path), COPD status, age, gender, and biopsy position. An interaction term between hemorrhage and lesion depth, representing whether the effect of depth on PTX risk differs depending on the presence or absence of hemorrhage, was included to test for effect modification. All predictors were entered simultaneously in the multivariable model.
Model performance was evaluated using the area under the ROC curve (AUC), and multicollinearity was assessed via variance inflation factors (VIF). Sensitivity analysis was conducted by excluding statistical outliers (i.e., very deep or very large lesions).
No formal sample size calculation was performed prior to data collection; however, with 26 PTX events in a sample of 118, the study had sufficient power for approximately five covariates; however, seven variables were explored based on clinical relevance, acknowledging possible model overfitting as a limitation.
A two-sided p-value < 0.05 was considered statistically significant. Analyses were performed using R software (version 4.5.0).
3. Results
A total of 118 patients were included in this study. CT-guided biopsies were performed in the supine position in 65 patients (55%) and in the prone position in 53 patients (45%). Thirty-nine patients (33%) had a prior diagnosis of COPD. The mean lesion size was 38.6 ± 26.6 mm (range: 2.6–115 mm), and the mean lesion depth (needle path length) was 24.1 ± 16.9 mm.
A PTX occurred in 26 patients (22%), of whom 7 (27%) required immediate chest tube placement. An additional 8 patients (7%) required chest drainage during the clinical course. Pulmonary hemorrhage occurred in 35 patients (30%).
Among patients with PTX, 73% did not experience hemorrhage, while 27% experienced both complications (Table 1). This descriptive distribution suggests, but does not statistically demonstrate, an inverse trend between hemorrhage and PTX.
Excluding statistical outliers (lesion depth > 70 mm or size > 90 mm) yielded similar results: hemorrhage OR 0.48 (p = 0.27); COPD remained statistically significant (OR 3.12, p = 0.041); AUC = 0.71.
3.1. Lesion Size Analysis
Lesion sizes in the population under study ranged from 2.6 mm to 115 mm. The mean lesion size among patients with PTX was 33.3 mm, while among patients without PTX had a mean lesion size of 40.1 mm. This difference was not statistically significant (p = 0.221, Mann–Whitney U test).
3.2. Lesion Depth and Hemorrhage Interaction
Needle path length ranged from 0 to 80 mm. Logistic regression showed that greater needle depth was significantly associated with increased PTX risk (β = 0.033, p = 0.012). Hemorrhage demonstrated a non-significant association with PTX (β = 1.103, p = 0.191). The interaction term between hemorrhage and needle depth approached significance (β = −0.047, p = 0.065), suggesting that hemorrhage may moderate the effect of needle depth on PTX risk.
Model-predicted risks of PTX increased rapidly with deeper needle depth in the absence of hemorrhage. In contrast, the presence of hemorrhage appeared to blunt this depth-associated risk increase, supporting a potential protective interaction. These are shown graphically in Figure 1, where diverging risk curves with depth can be observed over the range of depths. The overall model fit was acceptable (residual deviance = 117.10 on 114 degrees of freedom; AIC = 125.1).
Predicted PTX risks were estimated for lesions at 10-, 20-, and 40 mm depths: without hemorrhage = 8%, 17%, 32%; with hemorrhage = 7%, 10%, 15%, respectively, indicating attenuation of depth-related risk.
3.3. Complication Interaction
Hemorrhage was significantly less frequent in patients who developed PTX in unadjusted analysis (p = 0.021), whereas in the multivariable model this association did not reach statistical significance (OR 0.33, p = 0.135). Chest tube placement occurred in 3/35 (9%) patients with hemorrhage versus 12/83 (14%) without hemorrhage; this difference was not statistically significant (p = 0.48, Fisher’s exact test). Fewer patients with hemorrhage required chest tubes, although the difference was not statistically significant. These findings suggest a potential protective effect of hemorrhage (Figure 2), possibly via local tamponade or sealing mechanisms [22], as illustrated in Figure 3, which provides a case example showing the development of hemorrhage following vessel injury during needle placement, supporting a biologically plausible pathway for this protective effect.
The image sequence demonstrates that hemorrhage originated from a disrupted feeding vessel, not from parenchymal trauma, while the needle remained in place. Hemorrhage from a small vessel may exert a local tamponade effect, promoting clot formation along the needle tract, thereby reducing air leakage and the likelihood of PTX formation. Similar mechanisms have been postulated in prior interventional studies, where intrapulmonary bleeding or tract embolization was shown to decrease post-biopsy PTX by sealing the puncture channel [23,24,25]. Conversely, diffuse parenchymal trauma produces air leakage without effective sealing, a phenomenon also described in experimental models of alveolar injury and barotrauma [26,27].
3.4. Logistic Regression Predictors and Model Performance in PTX Risk Prediction
A multivariable logistic regression model was constructed to evaluate predictors of PTX, including pulmonary hemorrhage, lesion size, lesion depth, COPD, age, and gender. VIF values were all below 2, indicating no evidence of multicollinearity among the included variables.
Two variables emerged as statistically significant predictors of PTX risk:
- -Lesion size: OR 0.97 per mm increase (95% CI: 0.95–0.99, p = 0.020).
- -COPD: OR 3.17 (95% CI: 1.08–9.48, p = 0.035).
Lesion depth showed borderline association (p = 0.060). Hemorrhage and the interaction term did not reach statistical significance.
Model performance is illustrated in Figure 4, which displays the ROC curve for PTX prediction. The model achieved an AUC of 0.709 (95% CI: 0.61–0.81), indicating moderate discriminatory ability.
Lesion size and COPD remained the strongest predictors within the multivariable model, whereas hemorrhage, age, and gender were not statistically significant in this cohort. Full regression results, including odds ratios and confidence intervals, are presented in Table 2.
3.5. COPD and Risk Profile
As shown in the multivariable model (Table 2), COPD independently predicted PTX risk (OR 3.17, p = 0.035). Within the COPD subgroup (n = 39), PTX occurred in 7/39 (18%). PTX occurred in 6/29 (21%) without hemorrhage versus 1/10 (10%) with hemorrhage (Fisher’s exact p = 0.653). However, by Fisher’s exact test, there was no statistically significant association between hemorrhage and PTX in COPD patients (p = 0.653), with an estimated odds ratio of 0.43 (95% CI: 0.01–4.45). This suggests a trend towards lower risk of PTX in hemorrhage cases, although with limited interpretation with small sample size and wide confidence intervals. Pearson’s chi-square tests, with and without continuity correction, also confirmed the lack of statistical significance (p = 0.45 and p = 0.78, respectively). Figure 5 visualizes the subgroup counts for COPD patients, highlighting these distributions without displaying regression coefficients.
3.6. Histological Outcomes
Histopathological evaluation was completed successfully in 116 (98.3%) of 118 patients but 2 (1.7%) were described as non-diagnostic with no satisfactory material or no tumor cells available. Of the cases diagnosed, 77.6% were malignancies. The most prevalent malignant type was adenocarcinoma, which was found in 39.8% of patients. This was followed by squamous cell carcinoma (14.4%), NSCLC NOS at 11.9%, and pulmonary metastases at 5.9%. Neuroendocrine tumors, including carcinoids and atypical ones, accounted for 5.1%. Other malignancies, such as sarcoma and fibrous tumors, comprised 7.6%. Benign and inflammatory lesions were 13.6% of the cases, i.e., organized pneumonia, chronic inflammation, fibrosis, granulomatous diseases, and hamartomas. Figure 6 illustrates the frequencies of histological findings.
Because several histological subgroups contained limited numbers of cases, diagnosis-specific risk analyses for PTX or pulmonary haemorrhage were not performed. Therefore, histological outcomes are presented descriptively and were not included as predictors in multivariable modeling.
4. Discussion
In an oncological population, this retrospective single-center cohort study examined the correlation between PTX and pulmonary hemorrhage subsequent to CT-guided transthoracic lung biopsy. Our data suggest that pulmonary hemorrhage may be associated with a reduced incidence of PTX, particularly in cases of increased lesion depth. This implies a tamponade-like mechanism in which PTX is inhibited by localized hemorrhage from the biopsy tract, which reduces the influx of alveolar air into the pleural cavity [17,28,29]. This method is advantageous in the management of lung cancer, as it frequently requires tissue confirmation for radiation therapy, immunotherapy, and surgical intervention, particularly for the treatment of larger and peripheral lesions.
The 22.0% PTX rate in our sample corresponds with the rates reported in extensive meta-analyses utilizing CT-guided transthoracic needle biopsy, which range from 15% to 30%, depending on patient selection, lesion characteristics, and technical methodologies [30]. Chest tube implantation rates in documented research typically range from 5% to 15% [31], consistent with our cohort’s findings, where 5.9% required immediate drainage, and an additional 6.8% requiring further chest tube insertion. This consistency reinforces the external validity of our findings and indicates that the identified interaction patterns between bleeding and lesion depth are improbable to represent unusual complication rates.
From a clinical management standpoint, these complication rates highlight the necessity of doing a comprehensive procedural risk assessment, since hospitalization or intervention due to PTX may postpone cancer staging, radiation planning, or the commencement of systemic therapy.
Numerous constraints merit attention. The retrospective design limits causal inference and creates potential selection and information biases. Despite all procedures being conducted by a solitary, proficient interventional radiologist, thereby minimizing technical variability, the single-center context may restrict generalizability. The small sample size, especially the restricted number of PTX occurrences, hampered statistical power for subgroup analyses, including those involving patients with COPD. Consequently, these subgroup findings should be regarded as exploratory and necessitate validation in larger prospective multicenter datasets.
Unmeasured confounders, such as comprehensive smoking history, quantitative emphysema burden, and specific procedural factors, may have affected the probability of complications [32]. Future research utilizing standardized clinical datasets, quantitative imaging biomarkers, or radiomic factors may enhance personalized risk modeling for patients undergoing lung biopsy. Moreover, despite the documentation of histological diagnoses, the subgroup numbers were inadequate to provide a reliable comparison of PTX or bleeding risk across distinct tumor types. Consequently, diagnosis-specific odds ratio studies were not conducted and should be examined in larger multicenter cohorts.
The study’s strengths comprise a consistent procedural technique executed by a solitary experienced interventional radiologist, standardized biopsy protocols involving a single pleural pass, and a systematic immediate post-biopsy CT assessment, which collectively minimized procedural variability and facilitated a concentrated evaluation of hemorrhage-pneumothorax interactions.
Notwithstanding these constraints, the multivariable model exhibited considerable discriminative efficacy (AUC = 0.709), aligning with previous studies that recognize lesion depth, lesion size, and COPD as significant predictors of PTX risk [33,34]. The interaction between pulmonary hemorrhage and lesion depth did not achieve statistical significance but indicated a potential depth-dependent protective effect that warrants further exploration. This approach is especially pertinent in cancer, where deeper lesions are frequently targeted to facilitate definitive treatment techniques such as stereotactic radiation therapy, minimally invasive resection, or systemic therapy [35].
Reconceptualizing pulmonary bleeding as a potential modulator instead of merely an undesirable event could influence post-biopsy care. Identifying restricted tract bleeding on initial imaging may guide customized monitoring techniques and discharge planning, thereby decreasing unnecessary hospitalizations and eliminating delays in oncologic therapy [36]. Moreover, these findings offer conceptual validation for novel preventive strategies, such as tract embolization procedures, which similarly seek to occlude the biopsy channel and diminish the incidence of PTX [18,37,38]. Our findings collectively advance procedural risk models aimed at improving the safety of diagnostic techniques critical to modern lung cancer treatment.
5. Conclusions
In patients undergoing CT-guided lung biopsy for lung cancer evaluation, pulmonary hemorrhage may decrease the likelihood of pneumothorax, particularly in cases involving lesions located deeper within the lung tissue. By potentially reducing PTX-related morbidity and the need for invasive interventions, this interaction may help preserve procedural safety and minimize delays in diagnosis-dependent treatment processes. Ensuring the safety of biopsies is essential for the timely initiation of radiotherapy, immunotherapy, and surgical interventions, all of which depend on accurate and efficient tissue diagnosis. Although constrained by its retrospective single-center design and moderate sample size, this study offers clinically significant insights into the interplay of biopsy-related complications within an oncologic setting. Prospective multicenter studies are necessary to confirm these findings and to further enhance risk stratification models that facilitate efficient, therapy-focused diagnostic workflows in lung cancer management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen H.H. Wu Y.J. Wu F.Z. Precision Medicine in Lung Cancer Screening: A Paradigm Shift in Early Detection-Precision Screening for Lung Cancer Diagnostics 202515156210.3390/diagnostics 1512156240564882 PMC 12192117 · doi ↗ · pubmed ↗
- 2Tang F.H. Wong H.Y.T. Tsang P.S.W. Yau M. Tam S.Y. Law L. Yau K. Wong J. Farah F.H.M. Wong J. Recent advancements in lung cancer research: A narrative review Transl. Lung Cancer Res.20251497599010.21037/tlcr-24-97940248731 PMC 12000946 · doi ↗ · pubmed ↗
- 3Poulou L.S. Tsagouli P. Ziakas P.D. Politi D. Trigidou R. Thanos L. Computed tomography-guided needle aspiration and biopsy of pulmonary lesions: A single-center experience in 1000 patients Acta Radiol.20135464064510.1177/028418511348159523528565 · doi ↗ · pubmed ↗
- 4Sridhar S. Ahn H.G. Ebrahimzadeh S. Tang F. Elicker B. Evidence-based approach to transthoracic needle biopsy: Procedural techniques, risks, and controversies Radio Graphics 202545 e 24009410.1148/rg.24009440875452 · doi ↗ · pubmed ↗
- 5Riedl J.M. Moik F. Esterl T. Kostmann S.M. Gerger A. Jost P.J. Molecular diagnostics tailoring personalized cancer therapy—An oncologist’s view Virchows Arch.202448416917910.1007/s 00428-023-03702-737982847 PMC 10948510 · doi ↗ · pubmed ↗
- 6Constantinescu A. Stoicescu E.R. Iacob R. Chira C.A. Cocolea D.M. Nicola A.C. Mladin R. Oancea C. Manolescu D. CT-Guided Transthoracic Core-Needle Biopsy of Pulmonary Nodules: Current Practices, Efficacy, and Safety Considerations J. Clin. Med.202413733010.3390/jcm 1323733039685787 PMC 11642045 · doi ↗ · pubmed ↗
- 7Wattanasatesiri T. Puntu W. Vithitsuvanakul N. Influencing factors of pneumothorax and parenchymal hemorrhage after CT-guided transthoracic needle biopsy: Single-institution experience Pol. J. Radiol.20188337938810.5114/pjr.2018.79202 PMC 633409030655914 · doi ↗ · pubmed ↗
- 8Huang Z.G. Sun H.L. Wang C.L. Gao B.X. Chen H. Yang M.X. Chen X.L. CT-guided transthoracic needle biopsy of pulmonary lesions: Comparison between the cutting needle and aspiration needle Br. J. Radiol.2021942019093010.1259/bjr.2019093033245675 PMC 7934311 · doi ↗ · pubmed ↗