Mindfulness-Based Interventions for Bereavement: A Systematized Narrative Review
Fabio D’Antoni, Fabio Mattiussi, Cristiano Crescentini

TL;DR
This review explores how mindfulness-based interventions may help people cope with grief, though more research is needed to confirm their effectiveness.
Contribution
The paper provides a systematized narrative review of mindfulness-based interventions for bereavement, highlighting their potential and limitations.
Findings
MBSR and MBCT showed improvements in grief-related distress and psychological well-being.
MBIs were linked to reduced rumination and increased self-compassion.
Most studies had small samples and lacked long-term follow-up.
Abstract
Background/Objectives: Mindfulness-based interventions (MBIs) have shown promising effects across diverse areas of psychiatry, yet their specific role in bereavement remains insufficiently synthesized. Bereavement is a universal but heterogeneous process, with a minority of individuals at risk of developing prolonged grief disorder (PGD). Understanding the potential benefits of MBIs in this context is crucial for informing clinical practice. Methods: Following the methodological framework of systematized narrative reviews, a comprehensive literature search was conducted across major databases. Eligible studies included empirical investigations of MBIs applied to bereavement, without restrictions on type of loss, population, or intervention format. Data were narratively synthesized and summarized in tables; no meta-analysis was performed. Results: Seventeen studies met inclusion…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
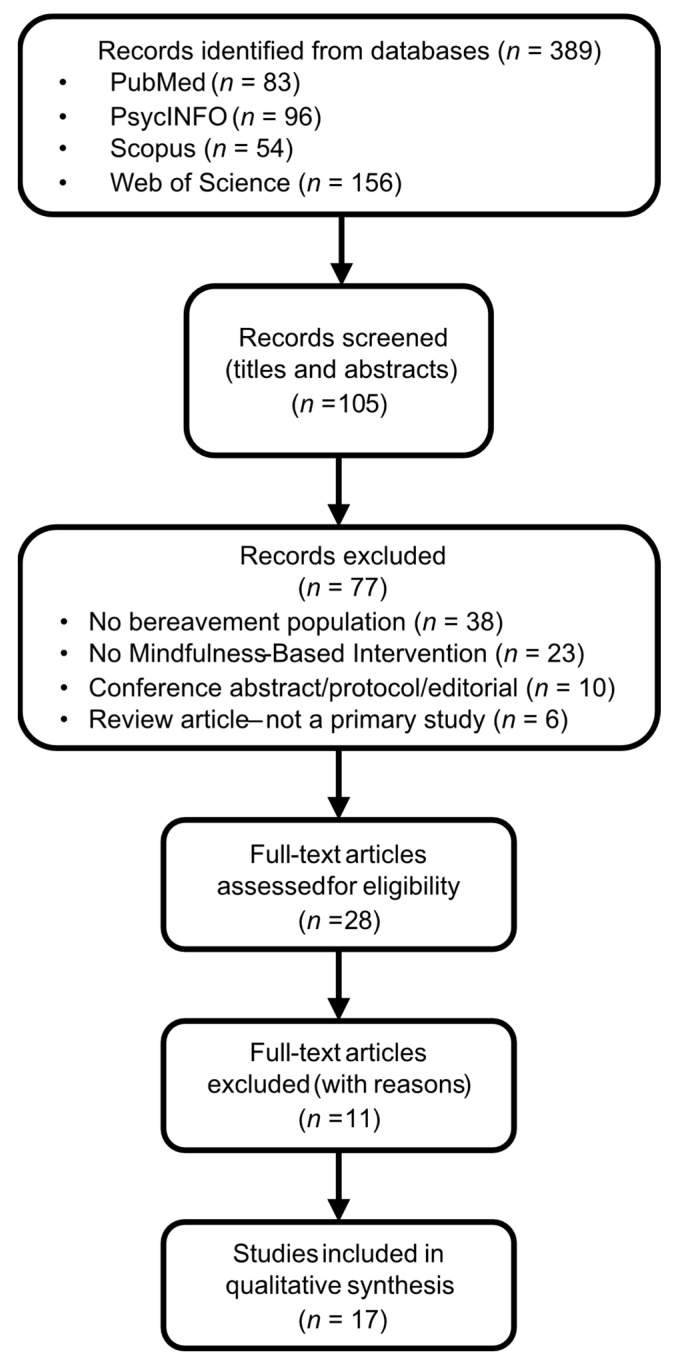 Figure 1
Figure 1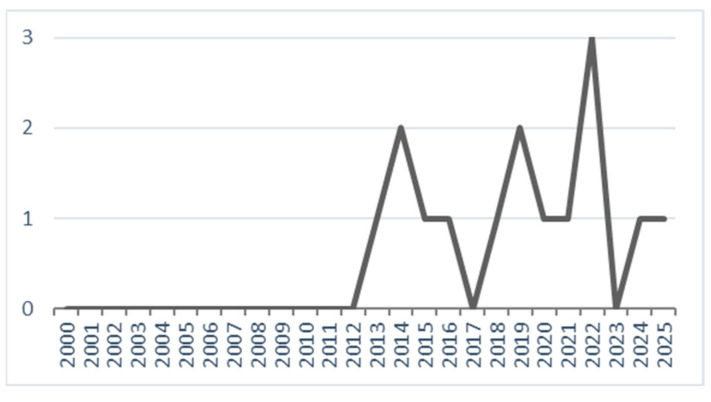 Figure 2
Figure 2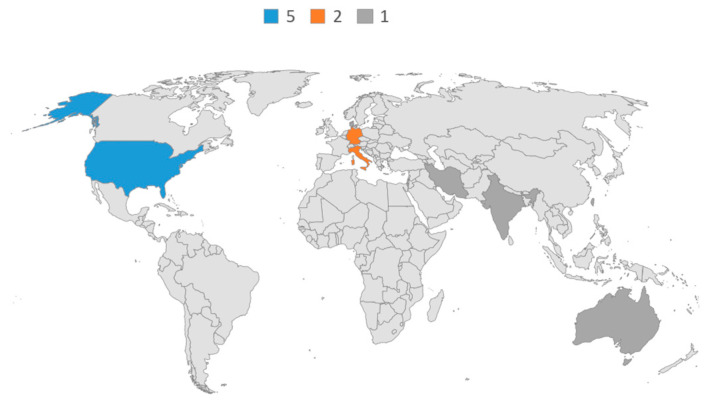 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGrief, Bereavement, and Mental Health · Mindfulness and Compassion Interventions · Resilience and Mental Health
1. Introduction
1.1. Mindfulness-Based Interventions
Mindfulness-Based Interventions (MBIs) refer to a broad spectrum of structured psychological programs and meditation practices unified by the cultivation of mindful-ness—commonly defined as “the awareness that emerges through paying attention, on purpose, in the present moment, and nonjudgmentally” [1]. This operationalization has been further refined into two interrelated components: the self-regulation of attention toward present-moment experience and an orientation of openness and acceptance [2].
Among the most established protocols are Mindfulness-Based Stress Reduction (MBSR) [3] and Mindfulness-Based Cognitive Therapy (MBCT) [4,5], typically delivered as secular, manualized group programs of eight weekly sessions plus a retreat [6]. These interventions integrate formal practices (e.g., sitting meditation, body scan, mindful movement) with informal practices designed to bring awareness into daily life [7]. The term MBI has also been extended to include “third wave” approaches such as Dialectical Behavior Therapy (DBT) [8] and Acceptance and Commitment Therapy (ACT) [9], which incorporate mindfulness skills even when not centered on formal meditation [10].
MBIs are extensively utilized in the psychiatric domain for treating a broad spectrum of psychological and psychiatric problems [10]. Across various patient populations, MBIs generally produce small-to-large reductions (standardized mean difference = 0.21–0.89) in common psychological symptoms, including depression, anxiety, and stress, relative to no treatment controls [11]. MBCT was developed specifically for psychiatric application and has demonstrated consistent efficacy for preventing relapse in major depressive disorder. MBSR and other MBIs show broader utility in reducing current anxiety and mood symptoms in patients with affective disorders [7].
MBIs are unified by the cultivation of mindfulness as a core mechanism of change across diverse clinical applications [6,10]. Their clinical utility can be understood in terms of both specific psychological mechanisms and common therapeutic factors. At the psychological level, MBIs foster (1) acceptance and non-reactivity, encouraging an open and nonjudgmental stance toward inner experience [7]; (2) meta-awareness and decentering, the capacity to observe thoughts and emotions as transient mental events rather than facts, thereby reducing identification with maladaptive patterns; (3) enhanced emotion regulation and cognitive flexibility, which diminish rumination and worry; and (4) positive psychological resources, such as self-compassion and positive affect, linked to greater well-being [6,7]. Beyond these mechanisms, MBIs also benefit from common therapeutic factors: the therapeutic alliance, strengthened when instructors embody mindfulness qualities; the group context, which provides social support and shared ritual; and the treatment rationale and expectancy, which frame mindfulness practice as an active pathway to relief and resilience [11]. Together, these ingredients explain the transdiagnostic effectiveness of MBIs in fostering adaptation and alleviating distress.
1.2. Bereavement
Bereavement refers to the universal yet highly individualized experience that follows the death of a significant other. Psychologically, it represents a multidimensional response activated by the disruption of a meaningful bond, encompassing affective, cognitive, behavioral, relational, and existential components. Although bereavement is a normative human experience, its expression and trajectory are shaped by personal, relational, cultural, and situational factors. The earliest psychological conceptualization of bereavement emerged within psychoanalysis. Freud (1917), in Mourning and Melancholia, described mourning as a process of gradual withdrawal of libidinal investment from the lost object [12]. A major paradigm shift occurred with attachment theory. Bowlby (1980) conceptualized grief as a biologically grounded response to separation from an attachment figure [13]. Parkes (1972) and Bowlby (1980) described sequential phases including shock, yearning and searching, disorganization, and reorganization [13,14]. While stage-based models such as Kübler-Ross’s five stages (1969) gained widespread influence, they have been criticized for oversimplifying and rigidifying a fundamentally non-linear process [15,16].
Later models reframed mourning as an active adaptive process. Worden (2002) proposed four tasks of mourning, emphasizing acceptance of the loss, emotional processing, adaptation to an altered world, and redefinition of the ongoing relationship [17]. Rubin’s Two-Track Model distinguished between biopsychosocial functioning and the continuing inner relationship with the deceased [18,19]. The Dual Process Model, grounded in stress and coping theory, conceptualized mourning as oscillation between loss-oriented and restoration-oriented coping [20]. Constructivist approaches further emphasized meaning-making processes. Neimeyer (2001) described bereavement as a reconstruction of disrupted meaning systems, involving sense-making, benefit-finding, and identity reorganization [21]. Similarly, the Continuing Bonds framework demonstrated that maintaining an adaptive internalized relationship with the deceased is not pathological but can facilitate integration [22].
Although bereavement is a universal human experience, its trajectory varies considerably; most individuals adapt over time, yet a significant minority experience persistent and debilitating symptoms consistent with Prolonged Grief Disorder (PGD) [23]. PGD, previously referred to as “complicated grief” or “persistent complex bereavement disorder,” is now formally recognized in both the ICD-11 and the DSM-5-TR [24]. It is characterized by intense yearning and longing for the deceased, persistent preoccupation with thoughts or memories of the lost person, and clinically significant functional impairment. Additional associated features include identity disruption (e.g., feeling that part of oneself has died), emotional numbness, intense emotional pain such as bitterness or anger, and difficulty reintegrating into social, occupational, or relational roles [25]. These symptoms exceed expected cultural or religious norms and result in marked impairment in daily functioning.
PGD is typically assessed using validated self-report and clinician-administered instruments. Commonly used measures include the Prolonged Grief Disorder-13 (PG-13), a 13-item scale aligned with ICD-11 criteria; the Inventory of Complicated Grief (ICG), a 19-item measure of symptom severity (with scores ≥ 25–30 indicating clinically significant impairment); the Brief Grief Questionnaire (BGQ), a 5-item screening tool; and the Structured Clinical Interview for Complicated Grief (SCI-CG), a clinician-administered diagnostic interview [25].
Prevalence estimates suggest that PGD affects approximately 9.8% to 34.3% of be-reaved individuals, depending on population and context [24]. Certain forms of loss, such as perinatal bereavement, are associated with substantially elevated risk, with rates nearly three times higher than other bereavement types [26]. PGD is also associated with significant adverse outcomes, including increased risk of suicidal ideation and behavior, as well as physical health conditions such as cardiovascular disease, cancer, hypertension, and immune dysregulation [25].
Given its prevalence, functional burden, and health implications, PGD represents a major clinical concern and underscores the need for interventions targeting core maintaining mechanisms such as rumination, experiential avoidance, emotional dysregulation, and self-criticism—processes that mindfulness-based approaches may specifically address.
1.3. Mindfulness and Bereavement
MBIs may support both normative and pathological grief by targeting mechanisms central to adaptation [26]: enhancing present-moment awareness, reducing rumination and avoidance [27,28], and fostering acceptance [29] and continuing bonds with the de-ceased [30]. These processes can mitigate maladaptive cognitive-emotional cycles and promote flexibility in the confrontation–avoidance oscillation typical of grief [19].
At the psychological level, mindfulness may counteract experiential avoidance by cultivating non-judgmental present-moment awareness, enabling bereaved individuals to remain in contact with painful emotions without compulsive suppression or withdrawal [31]. This stance may be particularly relevant in PGD, where persistent avoidance of grief-related affect paradoxically maintains distress. Mindfulness also helps to interrupt rumination by strengthening attentional flexibility and fostering decentering—the capacity to observe thoughts as transient mental events rather than as definitive truths about the self or the loss [32]. By weakening repetitive self-referential loops, MBIs may reduce the cognitive entrenchment characteristic of prolonged grief. In addition, mindfulness-based approaches cultivate self-compassion, which may mitigate guilt and shame frequently observed in traumatic forms of bereavement. Through self-kindness and recognition of common humanity, individuals may soften harsh self-criticism and reduce over-identification with narratives of failure or responsibility [31].
1.4. Aims of the Study
Despite encouraging findings in various psychiatric contexts, the evidence base for MBIs in bereavement remains fragmented, heterogeneous, and methodologically limited. Indeed, while several studies report improvements in grief-related distress and associated psychological outcomes following MBIs, the evidence remains methodologically diverse, with variability in study design, populations, intervention formats, and outcome measures. Notably, some comparative trials suggest that grief-focused cognitive-behavioral therapies may yield stronger effects on primary grief outcomes, whereas mindfulness-based approaches appear to exert more consistent benefits on transdiagnostic processes such as rumination, emotional regulation, and self-compassion. These mixed findings underscore the need for a structured synthesis of the available literature.
Therefore, the purpose of this article is to provide a systematized narrative review of MBIs in bereavement, in light of the growing clinical interest in mindfulness as an adjunct or alternative to established grief therapies. Specifically, this review seeks to examine (1) the current evidence regarding the feasibility, safety, and potential efficacy of MBIs in be-reaved populations; (2) the extent to which grief-specific versus transdiagnostic outcomes are affected; and (3) the methodological strengths and limitations that characterize the existing body of research. Given the heterogeneity of the literature, the review adopts an exploratory rather than hypothesis-testing approach.
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
This review followed the methodological framework of systematized narrative reviews [33,34], which combine elements of systematic reviews (explicit search strategy, eligibility criteria, PRISMA flow diagram) with the flexibility of narrative synthesis. Electronic searches were performed in PubMed/MEDLINE, PsycINFO, Scopus, and Web of Science Core Collection from 1 January 2000, to 9 August 2025. Search strings combined mindfulness terms (“mindfulness,” “mindfulness-based,” “mindfulness meditation,” “mindfulness-based stress reduction/MBSR,” “mindfulness-based cognitive therapy/MBCT,” “mindful self-compassion/MSC,” “acceptance and commitment therapy/ACT”) with bereavement terms (“grief,” “bereavement,” “mourning,” “complicated grief,” “prolonged grief,” “prolonged grief disorder”), using database-specific field codes and controlled vocabulary where available. Searches were limited to peer-reviewed articles in English involving human participants.
2.2. Eligibility Criteria
Inclusion and exclusion criteria were defined a priori:
- Population: Adults bereaved by the death of a loved one. Eligible populations included perinatal loss (miscarriage, stillbirth), suicide, homicide, spousal/partner, child, parent, or heterogeneous bereavement samples.
- ○Included: bereavement due to death, across different causes.
- ○Excluded: losses unrelated to death (e.g., chronic pain, job loss, identity loss); “professional grief” in healthcare providers when not related to personal bereavement.
- ○Ambiguous loss (e.g., disappearance of a relative) was excluded for conceptual consistency with the definition of bereavement as loss through death.
- Intervention: Structured MBIs, including manualized protocols such as MBSR, MBCT, and retreats with explicit mindfulness training. ACT-based programs were included only when mindfulness constituted a central therapeutic component, rather than a superficial mention.
- ○Excluded: interventions mentioning mindfulness superficially without structured practice or protocol.
- Study design: Empirical studies, including randomized controlled trials (RCTs), non-randomized controlled trials, pre–post cohort studies, and qualitative investigations exploring participant experiences.
- ○Excluded: study protocols, editorials, conference abstracts, scoping or narrative reviews (these were retained for background only).
- Outcomes: Studies were eligible if they assessed either grief-specific outcomes (e.g., Prolonged Grief Disorder, Inventory of Complicated Grief, Texas Revised Inventory of Grief) or clinically relevant secondary outcomes (e.g., depression, anxiety, PTSD symptoms, emotion regulation, mindfulness, self-compassion, quality of life). Studies lacking a grief-specific outcome were included but explicitly annotated and downgraded in quality appraisal.
- Language: Only articles published in English were included.
When multiple publications referred to the same participant cohort, these were all retained if they reported complementary findings (e.g., quantitative outcomes and qualitative experiences from the same intervention). In such cases, we noted the overlap in the evidence tables and synthesized the studies narratively, without double counting participants in the interpretation of results.
2.3. Data Extraction and Synthesis
For each eligible study, data were extracted using a standardized form: author, year, country, study design, population, type of loss, relationship to deceased, time since loss, sample size, intervention name, delivery mode, duration and dose, comparator, primary and secondary measures, main findings, other findings, and adverse events. Given the heterogeneity of study designs, interventions, and outcomes, findings were synthesized narratively and summarized in evidence tables. No meta-analysis was planned.
2.4. Quality Appraisal
The methodological quality of the included studies was appraised using a pragmatic approach adapted to the aims of this systematized narrative review. Given the marked heterogeneity of study designs included in this review (RCTs, quasi-experimental, pre–post, and qualitative studies), a simplified appraisal strategy was adopted to ensure consistency across the analysis. Therefore, each study was evaluated along two dimensions: (a) effect direction (i.e., whether the intervention showed improvements [↑], no effect [↔], or deterioration [↓] on grief-related or secondary outcomes), and (b) an overall quality rating based on study design, sample size, follow-up, and appropriateness of outcome measures. The quality rating was summarized using a traffic-light system:
- Green = higher-quality evidence (well-designed RCTs or large controlled studies with grief-specific outcomes and adequate follow-up),
- Yellow = moderate-quality evidence (pilot trials, quasi-experimental, qualitative, or controlled studies without grief-specific outcomes),
- Red = low-quality evidence (small uncontrolled studies, descriptive reports, or studies with major methodological flaws).
Each study was independently evaluated by two reviewers using the three-level traffic-light system based on predefined methodological criteria. To ensure the reliability of the traffic-light classification, inter-rater agreement between the two independent reviewers was assessed using Cohen’s unweighted kappa. The unweighted version was selected because the traffic-light categories represent nominal classifications without an inherent quantitative distance. Inter-rater agreement was used exclusively to assess the reliability of the appraisal procedure and does not imply validation of the traffic-light system as a formal quality assessment tool. Any disagreement was subsequently resolved through discussion.
In accordance with guidance on synthesis without meta-analysis, a pragmatic appraisal strategy was adopted to summarize heterogeneous evidence using direction-of-effect coding and transparent study descriptors, rather than applying formal risk-of-bias tools across highly diverse designs. The traffic-light system was used as a visual aid to support clarity and interpretability across studies and should be understood as an integrative summary of methodological considerations rather than a substitute for structured risk-of-bias assessment [35]. The operational criteria used to assign the traffic-light ratings are reported in Appendix A (Table A1). The use of a traffic-light system reflects established evidence-grading principles, whereby complex and continuous judgments about methodological quality are summarized into discrete categories, while acknowledging the inherent arbitrariness of such classifications [36].
2.5. Study Selection Process
The database search (2000–2025) yielded a total of 389 records (PubMed n = 83; PsycINFO n = 96; Scopus n = 54; Web of Science n = 156). After duplicate removal, 105 unique records remained for title and abstract screening.
Given the variability in intervention protocols, grief populations, and measured outcomes, a narrative synthesis was considered more appropriate than a quantitative meta-analysis. This approach enables a structured evaluation of methodological quality while allowing for theoretical integration across diverse study contexts. The study selection process is depicted in a PRISMA-style flow diagram adapted for narrative reviews (Figure 1). Eleven full-text articles were excluded after eligibility assessment, and the complete list of these excluded studies together with the specific reasons for exclusion is provided in Appendix B—Table A2.
3. Results
3.1. Characteristics of the Included Studies
A total of 17 studies met the eligibility criteria, published between 2013 and 2025 (see Table 1). When considering only unique studies (excluding secondary analyses or publications based on the same participant cohort), the chronological distribution shows an emerging but still limited evidence base. The first eligible study was published in 2013, followed by a gradual increase with peaks in 2014 (2 studies), 2019 (2 studies), and 2022 (3 studies). In recent years, research has continued steadily, with single studies published in 2024 and 2025 (see Figure 2). Overall, the evidence remains sparse, with no more than three new studies published in a single year. The majority of studies were conducted in the United States (n = 5), followed by Germany (n = 2) and Italy (n = 2). Single studies were carried out in Australia, Denmark, India, Iran, Israel, and Taiwan (see Figure 3). This distribution indicates that the current evidence base is concentrated in Western countries, particularly the United States, while research from Asia and the Middle East remains limited to isolated contributions.
Moreover, studies conducted in Western countries often report samples that are predominantly White and with higher levels of education [38,42,51,54]. However, studies from Iran and India highlight different socioeconomic and cultural contexts, focusing on women from public hospitals or rural, low-income backgrounds, sometimes with low literacy rates [46,48].
3.2. Research Design
The analysis of research designs across the included sources indicates that 15 studies involved primary data collection, employing either quantitative or qualitative methodologies. Two additional publications [44,53] were based on secondary analyses or subsamples drawn from previously published primary studies. Specifically, Ref. [43] reanalyzed data from the randomized controlled trial reported in [42], while the qualitative study by [52] was conducted on a subsample of participants from the quasi-experimental study reported in [51]. Accordingly, these two sources were retained in the total count of 17 included publications, but they do not represent distinct primary studies in terms of original data acquisition.
As summarized in Table 1, the 17 included studies employed a wide range of research designs. Only one study adopted a fully powered and methodologically rigorous randomized controlled trial (RCT) design, directly comparing Cognitive–Behavioral Therapy (CBT) with Mindfulness-Based Cognitive Therapy (MBCT) for PGD [38]. Two additional RCTs, conducted in specific bereavement-related populations, evaluated MBIs: one focused on women following early pregnancy loss [46], and the other tested Existential Behavioral Therapy (EBT) among informal caregivers of patients receiving palliative care [45]. Several studies employed quasi-experimental or non-randomized controlled designs, typically incorporating comparison groups without full random allocation. These included a controlled trial comparing Mindfulness Training (MT) with Progressive Muscle Relaxation (PMR) and a waitlist control group in widowed individuals [42], with secondary outcome analyses reported separately [43]. Other non-randomized studies evaluated MBCT in older bereaved adults [47], examined a brief and intensive MBI for suicide-loss survivors [50], and applied a non-equivalent comparison group design to assess a mindfulness-based retreat for bereaved parents [51].
A substantial proportion of the evidence base consisted of single-group pre–post de-signs, primarily pilot or feasibility studies assessing changes before and after mindful-ness-based programs without the inclusion of a control group. These included a retrospective cohort analysis of a mind–body group intervention for mothers following stillbirth [37], investigations of MBCT in bereaved individuals incorporating functional neuroimaging methods [39], an uncontrolled pilot study of MBSR for victims of gun violence [41], a retrospective chart review evaluating the ATTEND model in traumatic grief counseling [53], a pilot study of a culturally adapted MBI for perinatal bereavement in India [48], and a feasibility pilot study of residential retreats for suicide-loss survivors [49].
One study relied on cross-sectional baseline data only [54], while two studies employed qualitative methodologies to explore participants’ lived experiences. These included an analysis of perceived helpful factors within Existential Behavioral Therapy (EBT) [44] and a thematic analysis of bereaved parents’ perceptions of a mindfulness-based retreat [52].
Overall, this distribution indicates a predominant focus on intervention research, with most studies designed to evaluate the feasibility, acceptability, or preliminary efficacy of mindfulness-based approaches for bereavement. While RCTs provide higher-level evidence, the majority of available studies remain exploratory or quasi-experimental, underscoring the need for more controlled trials with larger and more diverse samples.
3.3. Type of Loss
The included studies varied in the type of bereavement targeted, although several re-ports did not specify this information in detail. Among those that did, the most common categories were suicide-related deaths (e.g., [49,51]), perinatal or stillbirth loss (e.g., [41,42,47]), and illness-related deaths, often in palliative care or cancer contexts (e.g., [44,45]). Traumatic deaths, such as gun violence, were specifically addressed in [41], while medical fatalities and unintentional injuries were included in the randomized trial by [38]. In some studies, detailed percentages were provided: for instance, Ref. [38] reported that 64% of losses were due to medical causes, 28% to suicide, and 8% to unintentional injuries. Other investigations, particularly those employing pre–post or qualitative methodologies (e.g., [39,40]), described participants as bereaved adults but did not report the specific type of death. Overall, the distribution suggests that suicide and perinatal loss are the most frequently represented causes of bereavement, with smaller but important contributions from illness, traumatic, and medical/unintentional deaths. The lack of systematic reporting of the cause of death in several studies limits the possibility to compare intervention effects across different types of bereavement.
3.4. Relationship with the Deceased
Information on participants’ relationship to the deceased was inconsistently reported across the included studies. When specified, the most frequently represented categories were spousal/partner loss and child loss, followed by parental loss and sibling loss. For example, Ref. [38] reported that participants were primarily bereaved of a parent (52%), child (22%), or partner (14%), with smaller proportions losing siblings (10%) or grandparents (2%). Similarly, Refs. [49,50] described samples that included partners, children, siblings, and parents bereaved by suicide, whereas [42] focused exclusively on widowed adults. Other studies targeted narrower categories: Refs. [37,48] included only bereaved mothers after stillbirth, while [46] investigated women following early pregnancy loss. Thieleman, Cacciatore, and colleagues (2014; 2020; 2022) focused specifically on bereaved parents, often in the context of traumatic loss. By contrast, several studies (e.g., [39,44,45,47]) reported that participants were “bereaved adults” but did not consistently specify their relationship to the deceased. Taken together, the evidence base is dominated by studies involving parents and partners, with relatively fewer studies addressing sibling, grandparent, or more extended kinship losses. The lack of systematic reporting of relationship categories across studies limits the possibility of assessing whether intervention effects differ according to the type of bond with the deceased.
3.5. Time Since Loss
The interval between bereavement and participation in the intervention was highly variable across the included studies. Some trials focused on recent loss, such as [37], where women bereaved by stillbirth were enrolled on average less than two months after the event (M = 1.79 months), or [39,40], which included participants bereaved within 6 months to 4 years. Similarly, Ref. [46] targeted women shortly after early pregnancy loss, although exact timing was not reported. Other studies involved longer-term bereavement. For instance, Refs. [42,43] included widowed adults approximately 14 months post-loss (M = 14.46 months), Ref. [47] recruited bereaved partners around four years after loss, and [44,45] reported mean times since loss of over one year. Refs. [49,50] described heterogeneous samples bereaved by suicide with median or mean durations of more than two years (median ~840 days, range 68–11.285 days), while [51,52,53] included parents bereaved on average between 1.7 and 5 years earlier. Several studies did not clearly report time since loss, limiting comparability (e.g., [41,48]). Overall, the evidence base includes both early interventions (within weeks or months of the death) and long-term interventions targeting bereavement persisting for several years. This variability reflects the diverse contexts in which mindfulness-based approaches have been tested, but it also complicates the possibility to evaluate timing as a moderator of intervention effects.
3.6. Sample Size
The sample sizes for MBI groups range from as few as 12 completers [47] and 19–20 in within-subject designs ([39,40], respectively) to larger groups of 72–74 ([37,54], respectively) and 97 [46]. Randomized controlled trials, such as [38], aimed for 50 participants in the MBCT arm, while [42,43] had 37 assigned to Mindfulness Training (MT), with about 30 completing the intervention. Many studies explicitly state their pilot nature (e.g., [41,47,48,49]), and thus inherently feature smaller sample sizes. These studies serve to explore feasibility and preliminary efficacy, paving the way for larger trials. Small sample sizes often lead to in-sufficient statistical power to detect significant effects, particularly for subtle changes or when dealing with high variability in grief experiences [47,54]. Some studies mention aiming for specific sample sizes based on power calculations (e.g., [38,40]) but do not always achieve them. A recurring limitation is that the samples are often small, self-selected, and homogeneous (e.g., predominantly White, female, or highly educated), limiting the generalizability of findings to broader, more di-verse bereaved populations [41,42,43,48,51]. This limitation is particularly critical in trauma contexts such as gun violence victimization, where the demographic characteristics of the affected population may differ substantially from those of the study participants [41]. Small samples can make it difficult to differentiate between intervention effects and other factors (e.g., natural recovery, social support, or regression to the mean) [38,41]. The need for replication in larger, more diverse, and rigorously controlled trials is a consistent recommendation across the sources [47,48,50]. In summary, while the existing body of literature provides encouraging preliminary evidence for the benefits of MBIs in various bereaved populations, it also underscores the need for larger, well-powered randomized controlled trials with more diverse samples to confirm these findings and enhance their generalizability and clinical applicability.
3.7. Intervention
3.7.1. Foundational Mindfulness-Based Programs (MBSR/MBCT and Their Adaptations)
These are typically structured, often 8-week, group-based programs that emphasize both formal (e.g., meditation) and informal (e.g., daily life awareness) mindfulness practices. MBSR is an 8-week evidence-based program designed to train individuals in non-judgmental reactivity to sensory events by focusing attention on somatic sensations like breath and body [41]. It provides intensive training that often includes practices such as body scan, mindful awareness of breath, sitting meditation, Hatha Yoga, emotional regulation, and compassion for others [41]. Participants are given daily assignments and encouraged to integrate mindfulness into daily life [41,46]. The goal is to be present in the moment without excessive worry about the future or past [46]. Sessions may also cover stress and body reactions, thought-emotion-body senses-behavior relationships, short concentration exercises (e.g., Three-Minute Breathing Space), mindful walking, conscious mind interactions, and “mountain meditation” [46]. This intervention was used in a pilot study for victims of gun violence [41] and for women with early pregnancy loss [46]. A shortened, culturally adapted five-week MBI was developed from the MBSR curriculum for women after stillbirth in rural India. It included mindfulness skills for daily life and psychoeducation on stillbirth risk factors, delivered by trained local nurses [48].
MBCT is an 8-week group-based clinical intervention that integrates elements of Cognitive-Behavioral Therapy (CBT) with systematic mindfulness meditation training [47]. Its aim is to teach participants to become more aware of and relate differently to their thoughts, feelings, and bodily sensations [47]. Key practices involve learning to accept in-tense emotional distress non-judgmentally, detaching attention from the content of automatic thoughts, and regulating attention back to present-moment experiences like the breath or bodily sensations [47]. MBCT also addresses unhelpful appraisals, which are considered crucial in maintaining PGD [38]. It typically includes guided meditations (such as body scans, sitting meditation, compassion meditation, and yoga), experiential exercises, discussions, and daily home practice. For bereaved individuals, specific adaptations like an additional introductory session on “acknowledgment of grief and theory of psycho-physical reactions to loss” might be included [39]. For elderly participants, session duration might be slightly reduced, and the focus of psycho-educational parts adapted [47]. MBCT has been applied in studies for PGD [38], for bereaved individuals (with fMRI analysis) [39,40], and for elderly bereaved people with loss-related distress [47].
3.7.2. Broader Mindfulness Training and Mind-Body Interventions
These interventions incorporate mindfulness as a key component but might not strictly adhere to the MBSR/MBCT manuals, often blending mindfulness with other therapeutic elements or using a more general “Mindfulness Training” (MT) label.
This latter type of intervention typically involves a systematic practice of focusing attention on present-moment experiences, emotions, and thoughts from an open, nonreactive, and nonjudgmental perspective [42,43]. Often based on programs like the UCLA Mindful Awareness Practices Level 1 course, it includes sessions on introduction to mindfulness, listening, working with pain/difficult emotions/thoughts, mindful interactions, and cultivating positive emotions (e.g., loving kindness) [42,43]. In-session practices can range from 10–25 min, with daily home practice of guided meditation (e.g., 5–19 min) [42,43]. The goal is to hone focused and receptive attention to reduce the automaticity of habits of mind like yearning and rumination, leading to “decentering” (observing thoughts/feelings as temporary mental phenomena) [42]. MTs were employed for bereavement-related grief in widow(er)s [42,43].
Mind-Body Group Therapy (MBGT). MBGT is a holistic therapeutic approach that combines techniques to enhance the connection between mental and physical health [37]. It includes practices such as relaxation techniques, mindfulness, cognitive behavioral strategies, and psychoeducation to reduce stress, improve emotional resilience, and alleviate psychological or physical symptoms [37]. The protocol, adapted from an existing model for infertility, involves eight group sessions and targets populations like women who experienced stillbirth [37].
Existential Behavioural Therapy (EBT). EBT is a group intervention, typically comprising six weekly meetings (22 h in total), designed to support informal caregivers of palliative patients during caregiving and bereavement [44]. Mindfulness training is a core element, integrated into the “third wave” of behavioral therapy alongside existential psychology [44]. Mindfulness, defined as focusing attention on the present experience with a nonjudgmental, accepting attitude, is practiced formally (e.g., following one’s breath, noticing and letting go of thoughts/feelings/sensations) in every session (at least 15 min) and encouraged at home (formally twice a day for 10 min, and informally through daily activities) [44,45]. This practice aims to help individuals (e.g., caregivers of palliative patients) distance themselves from ruminative thoughts and painful feelings [44].
3.7.3. Retreat-Based Mindfulness Interventions
These interventions are typically more intensive and shorter in duration, often offered in a retreat format, and frequently incorporate elements of self-compassion.
Mindfulness-based weekend retreats (Panta Rhei). These are short, intensive experiential retreats (16 h of practice over two days), based on principles from MBSR, MBCT, and Mindful Self-Compassion (MSC) [49,50]. They are specifically tailored for people bereaved by suicide, focusing on addressing grief pain and facilitating “letting go” [49,50]. Practices include Raisin Meditation, Body Scan, Breath Meditation, exercises like “How would I treat a friend?” and “Why am I here? What do I need?”, meditation on a compassionate friend, loving-kindness (Metta) meditation, kindness practice, mindful walking, mindful yoga, and mindfulness of sounds, colors, and smells [49,50]. The intervention emphasizes non-judgmental awareness, self-compassion, and acceptance, often within a supportive group setting with moments for silence and interaction [49,50].
Grief-focused mindfulness-based retreat (Selah). A 4-day retreat for bereaved parents that combines mindfulness practices with psychoeducation about child death [51,52]. It aims to help parents understand their experiences within a broader, often invalidating social context, fostering interpersonal and communal aspects of healing [51,52]. The retreat focuses on reducing psychological distress (trauma, anxiety, depression) and increasing well-being (mindfulness and self-compassion) [51]. Participants learn to bring an open and accepting attitude to their experiences, with reported benefits including a deepened sense of awareness through guided meditations, grief-related exercises, mindful movement, and art [52].
ATTEND model. This model is a MBI where clinicians are specifically trained in and encouraged to practice mindfulness (e.g., meditation, various styles of yoga, mindful movement, speech, and actions) and self-care [51,53]. The model’s six elements are Attunement, Trust, Therapeutic touch, Egalitarianism, Nuance, and Death education [53]. Clinician mindfulness is central to “Attunement,” fostering empathy, compassion, and connection. The goals are to increase emotional tolerance and awareness in clients by modelling non-judgmental acceptance. Clients may be taught specific mindfulness practices like 15-min breath exercises, awareness journaling, and nature walks. The model promotes individualized care rather than a rigid protocol [53].
In summary, the evidence base reflects a broad spectrum of MBIs adapted for bereavement populations. Foundational and manualized programs such as MBSR and MBCT remain the most widely applied, often delivered in standardized 8-week formats, while other studies tested shortened or culturally adapted versions tailored to specific contexts (e.g., stillbirth in India, pregnancy loss in Iran). Beyond these, several trials evaluated broader mindfulness training programs and integrative approaches such as Mind-Body Group Therapy (MBGT) and Existential Behavioral Therapy (EBT), embedding mindfulness practice within wider therapeutic frameworks. A distinct line of research has focused on retreat-based interventions, including the Panta Rhei model for suicide bereavement and the Selah retreats for bereaved parents, which combine intensive mindfulness and self-compassion practices in supportive group settings. Finally, innovative models such as the ATTEND framework emphasize clinician mindfulness as a relational vehicle for attunement and compassion in bereavement care. Taken together, these interventions illustrate the flexibility and adaptability of mindfulness-based approaches, spanning from standardized protocols to culturally specific adaptations and retreat formats. However, the diversity of programs and variability in their implementation complicate direct comparisons and underscores the need for future research to clarify which formats, components, and delivery modes are most effective for different bereavement populations.
3.8. Delivery Mode
Across the 17 included studies, the delivery of MBIs for bereavement was heterogeneous.
Group-based, in-person interventions were most common, including MBCT, MBSR, MBGT, MT, and EBT [37,39,40,42,43,44,45,46,47]. Retreat-based formats, such as Panta Rhei and the Selah retreats, offered intensive short-term group experiences for suicide-bereaved adults and bereaved parents [49,50,51,52]. Online delivery was less frequent but feasible, as shown by [41] with MBSR delivered via videoconference. Individual interventions were relatively rare: MBCT adapted for prolonged grief dis-order was administered individually [38], while the ATTEND model provided individualized therapy guided by trained clinicians [53].
In summary, while in-person group interventions predominate, emerging evidence highlights the feasibility of online programs and the potential of individualized approaches, with retreat-based models adding further diversity to available formats.
3.9. Duration and Dose
The duration and intensity of interventions varied considerably. Most manualized programs followed standardized structures of 6–8 weekly sessions, each lasting 2–2.5 h [39,40,42,43,46,47]. MBGT also comprised eight weekly sessions [37]. EBT was delivered in six group sessions of approximately 3.5 h [44,45]. Shorter and adapted interventions included the five-week culturally tailored MBSR for stillbirth in India [48]. More intensive formats were represented by the Panta Rhei weekend retreat (16 h across two days) [49,50] and the Selah retreats (four consecutive days) [51,52]. Individualized formats varied: MBCT for PGD involved 11 weekly 90-min sessions [38], while the ATTEND model extended over an average of 19 weeks with flexible session structures [53].
Several studies encouraged daily home practice ranging from 15–40 min, often supported by guided audio or written materials (e.g., [39,40,48,49,50]). Retreat formats, by contrast, concentrated practice into immersive schedules with multiple daily sessions.
In sum, dose ranged from brief 5-week courses to multi-month individual therapy and multi-day retreats, with most studies converging on the 6–8 week, 2-h weekly group session as the dominant structure, usually reinforced by regular home practice.
3.10. Comparator
The comparators employed across the included studies were heterogeneous, reflecting both the exploratory nature of much of the research and the diversity of bereavement populations.
Only a minority of studies incorporated active comparators. Ref. [38] directly compared MBCT adapted for grief with grief-focused CBT, demonstrating superior outcomes for the CBT arm at 6-month follow-up. Refs. [42,43] contrasted Mindfulness Training (MT) with Progressive Muscle Relaxation (PMR) and a wait-list control, showing that both MT and PMR reduced grief-related distress, though PMR out-performed MT for some outcomes. Several studies used passive control groups. Ref. [47] employed a wait-list design for bereaved partners, while [52] compared participants attending the Panta Rhei retreat with a non-intervention control group recruited from an online suicide-bereavement forum. Ref. [51] also used a passive comparison group of bereaved parents who did not attend the Selah retreat.
In contrast, many investigations were conducted as single-arm pre–post studies without a control condition, such as [42,47,48,49,51,54]. These designs provide useful feasibility and acceptability data but limit causal inference.
Finally, some studies employed qualitative or uncontrolled frameworks [44,52], where no comparator was applicable.
In summary, while a few well-designed trials included active or passive comparators, the majority of studies relied on uncontrolled pre–post designs. This imbalance highlights the need for future research employing rigorous randomized comparisons with active control conditions to better isolate the specific effects of mindfulness-based interventions in bereavement.
3.11. Primary Grief Outcome Measure
The use of grief-specific outcome measures was inconsistent across the included studies.
Among the randomized controlled trials, Ref. [38] employed the Prolonged Grief Disorder scale (PG-13) [29,55] and the Grief Cognitions Questionnaire (GCQ) [56] as primary measures. Ref. [42] used the Inventory of Complicated Grief—Revised (ICG-R) [57,58], complemented by yearning (YSL) [59] and grief rumination (UGRS), whereas [47] also relied on the ICG-R. Refs. [39,40] administered the Texas Revised Inventory of Grief (TRIG) [60] to evaluate pre–post changes in bereaved adults. Ref. [48] employed the Perinatal Grief Scale (PGS) [61,62] in their culturally adapted intervention for women after stillbirth. Ref. [41] used the Inventory of Complicated Grief (ICG) in a sample of adults bereaved by gun violence, though high dropout limited analyses.
By contrast, several studies did not include a direct grief-specific measure. These included [37], which conceptualized stillbirth grief indirectly and focused on depressive and trauma-related outcomes [46], which assessed psychological distress using the DASS-21; and [44,45], which relied on psychological well-being, quality of life, and mindfulness outcomes. Retreat-based interventions such as Panta Rhei [49,50] and the Selah retreats [51,52] also did not include standardized grief measures, instead evaluating psychological distress, mindfulness, and self-compassion. The ATTEND model was assessed primarily through trauma- and depression-related indicators rather than grief-specific scales [53].
The grief-related outcome measures employed across the included studies are sup-ported by established psychometric validity and reliability, although their heterogeneous use limits direct comparability of findings. The PG-13 demonstrates strong internal consistency (α = 0.89) and alignment with ICD-11 diagnostic criteria [38], while the ICG/ICG-R shows excellent internal consistency (α ≈ 0.94), good test–retest reliability (r ≈ 0.80), and solid criterion validity [42]. The PGS also demonstrates good reliability (α = 0.89) in perinatal populations [48]. Measures targeting grief-related processes, such as the YSL and the UGRS, exhibit excellent internal consistency (α = 0.85–0.97) and strong discriminant validity from depression and anxiety [42], while the TRIG remains a widely used and reliable measure of grief severity (α = 0.89–0.94) [39,40].
In summary, less than half of the included studies employed validated grief-specific measures (e.g., PG-13, ICG, ICG-R, TRIG, PGS), while the remainder relied on indirect indicators such as depression, anxiety, trauma, or quality of life. This methodological gap reduces the comparability of findings and limits the possibility to draw firm conclusions about the efficacy of mindfulness-based interventions in alleviating grief itself.
3.12. Secondary Outcome Measures
Beyond grief-specific assessments, most of the included studies incorporated a wide range of secondary measures addressing broader domains of psychological distress and well-being [37].
Depression was frequently evaluated, using instruments such as the Beck Depression Inventory-II [38,41,47,63], the Edinburgh Postnatal Depression Scale [37,64], the Tai-wan Depression Scale [39,40,65], or the depression subscale of the DASS-21 [46,66]. Anxiety was similarly assessed across several trials, most often with the Beck Anxiety Inventory [38,67], the Generalized Anxiety Disorder Scale [39,40,68], or the anxiety subscale of the DASS-21 [46,66]. The Hopkins Symptom Checklist (HSCL) [69], in its 10- and 25-item versions (HSCL-10 and HSCL-25), was also employed as a measure of anxiety and depressive symptomatology [48,51,53].
Post-traumatic stress symptoms were also a central focus, measured with tools such as the PTSD Checklist for DSM-5 [41,70,71], the Trauma Symptom Checklist-40 [41,72], the Harvard Trauma Questionnaire [43,47,73], and the Impact of Event Scale–Revised [51,53,74], while coping responses to trauma were captured by the Perceived Ability to Cope with Trauma Scale, specifically its flexibility subscale (PACT-flexibility) [43,75]. Other studies focused on stress and emotion regulation, using the Perceived Stress Scale [43,76] and the Difficulties in Emotion Regulation Scale [39,40,77]).
Consistent with the mindfulness focus of these interventions, nearly all programs included validated instruments to capture dispositional mindfulness, most prominently the Five Facet Mindfulness Questionnaire [78] (e.g., [39,40,41,48,49,50,51]), but also the Cognitive and Affective Mindfulness Scale–Revised [45,79] and the Mindful Attention Awareness Scale [43,54,80]. Self-compassion was another recurrent domain, measured through the Self-Compassion Scale in either its full or short form [49,50,51,81].
Finally, several studies investigated broader indicators of well-being and functioning, including the Satisfaction With Life Scale [41,43,45,48,82], the WHO Quality of Life-BREF [38,45,83,84], and the Schedule for the Evaluation of Individual Quality of Life [45,85]. A smaller number of investigations extended to additional domains such as sleep quality (Pittsburgh Sleep Quality Index—PSQI) [43,54,86], loneliness (UCLA Loneliness Scale) [43,87], religious coping (Brief RCOPE) [48,88], social support [48], and even cognitive performance tasks [39,59].
With respect to the validity and reliability of the principal scales not specifically de-signed for grief assessment, the PCL-5, used to assess post-traumatic stress symptoms in bereaved populations, demonstrates excellent internal consistency (α ranging from 0.91 to 0.93) [37,41]. Similarly, the EPDS and the STAI-S, applied in perinatal bereavement contexts, show strong internal reliability (α = 0.93 and α = 0.89, respectively) [37]. The FFMQ, widely used to assess dispositional mindfulness, is also well validated, with high overall reliability in both meditator (α ≈ 0.95) and non-meditator samples (α ≈ 0.86) [39,49].
This heterogeneity of secondary outcome measures illustrates the multidimensional scope of mindfulness-based interventions in bereavement, but also highlights the challenge of synthesizing findings across such diverse constructs.
3.13. Descriptive Synthesis
Across the 17 included studies, mindfulness-based interventions for bereavement were applied in highly heterogeneous ways, reflecting differences in populations, study designs, intervention formats, and outcome measures. This heterogeneity precludes quantitative pooling but allows for an integrative narrative overview. Most programs were delivered as structured group interventions based on established protocols such as MBCT or MBSR, while others employed retreat-based or individualized formats. Study designs ranged from randomized controlled trials to non-randomized controlled studies, single-arm pre–post designs, and qualitative investigations. Sample sizes varied considerably, from fewer than 20 participants in small pilot trials to nearly 150 in larger non-randomized studies.
The assessment of outcomes was equally diverse. While some studies employed validated grief-specific measures (e.g., PG-13, ICG, ICG-R, TRIG, PGS), many relied instead on indirect indicators such as depression, anxiety, post-traumatic stress, mindfulness, self-compassion, and quality of life. The uneven use of grief-specific instruments complicates comparability across studies and constrains the possibility to draw firm conclusions about the direct impact of mindfulness on grief per se.
Overall, the evidence suggests that mindfulness-based interventions are generally feasible, well tolerated, and potentially beneficial across multiple domains of psychological adjustment in bereavement. However, the heterogeneity of designs, the predominance of small and uncontrolled studies, and the inconsistent use of grief-specific outcomes underscore the need for cautious interpretation. The following sections present the main intervention outcomes and adverse events reported in the included studies.
3.14. Main Outcomes
3.14.1. Bereavement Related Outcomes
Among the 17 included studies, fewer than half employed direct grief-specific measures, while two relied on qualitative assessments of grief-related experiences (see Table 2).
The strongest evidence derives from the randomized controlled trial by [38], where MBCT adapted for grief significantly reduced prolonged grief disorder symptoms (PG-13). Both MBCT and grief-focused CBT showed large within-group improvements, though CBT proved superior at six-month follow-up, particularly in reducing maladaptive grief-related cognitions (GCQ).
Other controlled studies provided supportive findings. Ref. [42] reported significant reductions in complicated grief (ICG-R), yearning (YSL), and grief-related rumination (UGRS) following both Mindfulness Training (MT) and Progressive Muscle Relaxation (PMR), with PMR showing stronger effects than MT and wait-list. In contrast, the secondary analysis [43] did not include grief-specific outcomes, limiting its relevance to bereavement per se.
Uncontrolled pre–post studies further suggested potential benefits. Refs. [39,40] observed robust reductions in grief (TRIG) among bereaved adults after MBCT, complemented by neuroimaging findings linking grief improvement to changes in neural connectivity supporting emotion regulation. Similarly, Ref. [48] found significant decreases in perinatal grief (PGS) in Indian women following a culturally adapted five-week MBSR program.
Evidence in contexts of traumatic loss was weaker. Ref. [41] documented a 23% reduction in complicated grief (ICG) after MBSR for survivors of gun violence, though the effect did not remain significant after correction for multiple testing due to small sample size and attrition. Ref. [47] also reported no significant effects of MBCT on grief (ICG-R) compared with waitlist, in a small pilot with high dropout.
Qualitative studies provided convergent insights. Ref. [44] highlighted acceptance, reduced rumination, and reorientation as perceived benefits of mindfulness, while [52] emphasized enhanced self-compassion, continuing bonds, and validation of grief in a supportive retreat setting, albeit with some participants experiencing temporary distress when exposed to others’ traumatic narratives.
In summary, the available evidence suggests that mindfulness-based interventions can alleviate grief symptoms, with consistent improvements observed in validated scales such as the PG-13, ICG-R, TRIG, and PGS. Qualitative data reinforce these findings by illustrating processes of acceptance, reduced rumination, and strengthened continuing bonds. Nonetheless, the overall strength of evidence remains limited by the small number of RCTs, modest sample sizes, and inconsistent use of grief-specific outcomes.
3.14.2. Other Findings
Several studies reported additional results that, although not designated as primary outcomes, provide valuable insights into grief processes and their modulation through mindfulness. In the trial by [42], reductions in yearning and grief-related rumination paralleled the decline in grief severity, suggesting that mindfulness training may operate by reducing maladaptive cognitive processes that sustain bereavement distress. Similarly, Refs. [39,40] found that increases in dispositional mindfulness were negatively correlated with grief severity (TRIG), indicating that enhanced mindful awareness may buffer against intrusive grief-related thoughts and emotions.
Studies also identified neurocognitive correlates of change. Ref. [39] demonstrated that improvements in grief scores were associated with reduced activation in the posterior cingulate cortex and thalamus, while [40] highlighted changes in cortico-subcortical connectivity linked to emotional regulation. These findings suggest that the beneficial effects of MBCT on grief may be mediated by neural mechanisms supporting attentional control and affective regulation.
In contexts of traumatic loss, Ref. [41] observed that gains in mindfulness predicted greater reductions in complicated grief, even though overall grief score changes did not remain significant after correction. This underscores the potential role of mindfulness as a mediator of grief adaptation, even in highly challenging bereavements such as gun violence.
Qualitative evidence further deepens this picture. Ref. [44] reported that participants described mindfulness and acceptance as tools to counter ruminative thinking and to foster reorientation after loss, while [52] emphasized how retreat participation supported continuing bonds, communal validation of grief, and improved emotional regulation. At the same time, some participants described transient distress when exposed to others’ traumatic narratives, highlighting the ambivalence of group processes in bereavement.
Taken together, these findings suggest that mindfulness-based interventions may influence grief not only by reducing symptom severity but also by addressing underlying processes such as yearning, rumination, emotional regulation, and continuing bonds. The convergence of quantitative and qualitative evidence points toward a multifaceted role of mindfulness in reshaping the way bereaved individuals relate to their loss.
3.15. Acceptability and Safety
Across the included studies, mindfulness-based interventions for bereavement were generally considered safe and acceptable, with very few adverse events reported. No study described serious harms attributable to the intervention. However, some participants noted transient emotional discomfort. For instance, in the Selah retreats, exposure to others’ traumatic narratives occasionally intensified grief-related emotions, a phenomenon described as cathartic rather than harmful when contained within a safe and supportive group environment [51,52]. Similarly, participants in the Panta Rhei retreats sometimes reported emotional intensity during practices, though this was interpreted as part of the grief process rather than an adverse effect [49,50].
Retention varied widely across studies and constituted a recurrent methodological challenge. The large RCT by [38] retained only 60% of participants at 6-month follow-up, limiting the strength of conclusions regarding long-term efficacy. Ref. [47] reported that only 36% of eligible participants ultimately completed the MBCT intervention, reflecting difficulties in engaging bereaved individuals in longer protocols. In contrast, retreat-based programs such as Panta Rhei showed relatively high adherence, with most participants completing the intensive weekend format and reporting strong acceptability [49,50]. Similarly, Ref. [48] observed adherence rates close to 90% in the culturally adapted MBSR program for stillbirth in India, facilitated by shorter duration and local delivery.
Overall, dropout rates tended to be higher in multi-week clinical trials than in brief, retreat-based, or culturally adapted programs. This pattern suggests that while mindful-ness interventions are generally acceptable, their feasibility may depend on program length, intensity, and contextual tailoring to bereaved populations.
In summary, MBIs for bereavement appear to be safe, with no evidence of intervention-related harm, and generally acceptable to participants. Nonetheless, in the context of suicide bereavement, facilitators should remain attentive to the risk of temporary emotional intensification, particularly during group sharing, which may require additional containment strategies. Feasibility also depends on program format: attrition tends to be higher in longer clinical trials, whereas brief, retreat-based, or culturally adapted programs show consistently higher adherence and participant satisfaction.
3.16. Quality of Included Studies
Inter-rater agreement for the traffic-light classification was substantial (Cohen’s unweighted κ = 0.64). Disagreement occurred in only one of the 17 studies evaluated (94% raw agreement). The kappa coefficient should be interpreted in light of the small number of ratings and the skewed marginal distributions across categories, conditions that attenuate κ values despite high observed agreement. In the present case, the obtained κ approached the maximum possible value given the observed marginal frequencies. The methodological appraisal showed that only one study, the randomized controlled trial by [38], met criteria for high-quality evidence (Green rating), as it combined a rigorous randomized design, an adequate sample size, and the use of grief-specific outcome measures. All of the remaining 16 studies were classified as moderate quality (Yellow rating). This was due either to limitations in study design (e.g., non-randomized controlled trials, pre–post pilots, qualitative investigations, or secondary analyses) or to the absence of grief-specific outcome measures, which led to systematic downgrading irrespective of methodological rigor. No study was classified as low quality (Red rating). Table 3 provides a synthesis of effect directions across grief-related and secondary outcomes, together with the overall quality rating for each study based on the traffic-light appraisal system.
Across the evidence base, several recurring limitations emerged. First, sample sizes were generally small, often fewer than 40 participants per group, limiting statistical power and raising concerns about representativeness. Attrition further reduced effective sample sizes, particularly in multi-week protocols, undermining the robustness of findings. Second, most studies relied on homogeneous samples, predominantly female, White, and highly educated, thereby restricting the generalizability of results to more diverse bereaved populations. Third, grief-specific outcome measures were inconsistently employed: fewer than half of the studies used validated grief scales such as the PG-13, ICG, ICG-R, TRIG, or PGS, while others relied exclusively on indirect indicators (e.g., depression, PTSD, mindfulness, or self-compassion). This limits comparability across trials and weakens the possibility to isolate intervention effects on grief per se. Fourth, follow-up assessments were rare and typically short-term, with most studies evaluating outcomes only immediately post-intervention; sustained effects beyond three to six months remain largely undocumented. Finally, comparators were often weak or absent, as only a handful of studies included active control conditions (e.g., grief-focused CBT, PMR), while many adopted uncontrolled pre–post designs.
Taken together, the current evidence base suggests that MBIS for bereavement are promising, but the methodological quality remains limited. Stronger conclusions will require well-powered randomized controlled trials, the systematic use of grief-specific outcome measures, longer follow-up periods, and greater diversity in participant samples. Addressing these limitations is essential to establish the efficacy and clinical applicability of mindfulness-based approaches in bereavement care.
In summary, the 17 publications analyzed in this review provide preliminary but encouraging evidence regarding the feasibility, safety, and potential efficacy of MBIs in bereavement care. MBSR and MBCT emerged as the most established protocols, showing improvements in grief-related distress, depressive symptoms, and overall psychological well-being across heterogeneous loss contexts. Reported therapeutic benefits were generally associated with reductions in maladaptive cognitive processes, such as rumination and experiential avoidance, alongside gains in self-compassion and emotion regulation. Neuroimaging findings, although limited, suggest that symptomatic improvements may be linked to enhanced attentional flexibility and reduced activity in neural regions implicated in affective and self-referential processing, including the posterior cingulate cortex and the thalamus.
Despite these promising findings, the evidence base remains largely composed of pilot and quasi-experimental studies, with only one study meeting high methodological quality criteria. Additionally, several investigations lacked grief-specific outcome measures or long-term follow-up assessments. Therefore, while MBIs show potential as adjunctive interventions, further high-quality randomized controlled trials with diverse samples and standardized grief assessments are needed to clarify their long-term efficacy and clinical positioning alongside established grief therapies.
4. Discussion
This systematized narrative review synthesized the emerging evidence on Mindful-ness-Based Interventions (MBIs) in bereavement. The most consistent findings were re-ported for Mindfulness-Based Stress Reduction (MBSR) and Mindfulness-Based Cognitive Therapy (MBCT), which demonstrated preliminary but encouraging effects on grief-related distress, depressive symptoms, and psychological well-being across diverse bereaved populations [40,47]. Despite these promising signals, the evidence base is constrained by several methodological limitations. Many studies relied on small sample sizes (e.g., [26,40]), limiting generalizability and statistical power. In addition, long-term follow-up assessments were often absent, making it difficult to evaluate the durability of treatment effects [51,89]. Another recurring issue is the lack of standardized grief-specific outcome measures, with many studies focusing on general indicators of psychological distress rather than validated grief instruments [26,32], thus reducing comparability across trials.
4.1. Theoretical Implications
From a theoretical perspective, MBIs integrate therapeutic elements that appear relevant for both normative grief and PGD [32]. Their efficacy in grief contexts largely derives from enhancing emotion regulation and transforming individuals’ relationship with painful thoughts and feelings [40,53]. Three core mechanisms can be highlighted.
First, acceptance and non-judgmental awareness—defined as intentional present-moment attention with openness and curiosity [51]—counteracts experiential avoidance, a maladaptive coping strategy strongly implicated in complicated grief [32]. For example, In Selah retreats for bereaved parents, the “being with grief” phase explicitly encourages turning toward painful emotions non-judgmentally. Participants reported that this approach helped them “befriend” their grief; for instance, one parent noted that while the grief remained, they “don’t fear it anymore” and stopped trying to “stuff” their tears [51]. The ATTEND model emphasizes attunement and validation of the client’s affective states. By creating a safe environment where “everybody has cried at least once” without judgment, mourners can move away from social and internal “oppression” that forces them to “move on” before they are ready [52]. This orientation increases emotional tolerance and reduces symptom severity, as shown in suicide-bereavement retreats where the non-judging facet of mindfulness improved significantly [49,50]. For example, Panta Rhei retreats resulted in a significant decrease across all measured areas of psychological distress, including tension-anxiety, depression, and anger-hostility [49,50].
Neurobiological evidence increasingly supports the hypothesis that MBIs may alleviate grief-related distress through mechanisms of acceptance and non-judgment. Functional Magnetic Resonance Imaging (fMRI) studies indicate that MBCT enhances executive control and reduces emotional interference in regions implicated in affective and self-referential processing, including the Posterior Cingulate Cortex (PCC) and thalamus [39]. Longitudinal findings further show that MBCT reorganizes resting-state functional connectivity, particularly by reducing internetwork connectivity within the Default Mode Network (DMN) and salience networks [40].
A central mechanism underlying mindful acceptance concerns the distinction between primary affective signals and secondary cognitive reactivity. In line with the classical metaphor of the “two arrows,” the first arrow represents the raw emotional pain (e.g., sudden waves of sadness or longing), whereas the second arrow consists of evaluative judgments and resistance (e.g., “this is unbearable,” “it will never end”) that amplify distress [90]. Emerging neuroscientific evidence suggests that mindfulness reduces this secondary amplification process. Specifically, mindful acceptance appears to down-regulate affective distress via bottom-up mechanisms, modulating primary affective representations without relying predominantly on top-down prefrontal cognitive control [90]. Ap-plied to bereavement, this mechanism suggests that grief-related emotional pain may be recontextualized not as an overwhelming or identity-defining catastrophe, but as a transient and natural affective state. Rather than suppressing grief experiences, mindful acceptance modifies the initial appraisal of affective significance, allowing the experience to unfold without secondary resistance [40,90]. For example, interviewees reported learning that sadness did not need to be fought or suppressed, recognizing instead that “I do not need to battle the sadness, because this is how it must be … if I try to fight it, I do not necessarily feel better” [44].
This process can be conceptually aligned with the Dual Process Model of Coping with Bereavement [20,91], which posits an adaptive oscillation between loss-oriented and restoration-oriented processes. By reducing cognitive elaboration and experiential avoidance, mindfulness may facilitate a more flexible engagement with loss-oriented distress while preventing rigid over-immersion or chronic avoidance. In this sense, mindful acceptance may support the oscillatory regulation described in the Dual Process Model, attenuating prolonged psychophysiological activation and fostering adaptive integration of the loss experience. This oscillatory dynamic is conceptually aligned with the Selah model, which explicitly describes an oscillation between self-focused and other-focused modes of grieving (e.g., being with, surrendering to, and doing with grief). Such oscillatory flexibility prevents rigid entrenchment in distress while also discouraging defensive disengagement from the loss. Notably, participants described that, after “making space” for their pain, they experienced a renewed interest in work and other daily activities, reflecting a fluid transition toward restoration-oriented engagement [51,52].
Second, decentering and attentional regulation allow mourners to observe thoughts and emotions as transient mental events, thereby interrupting grief rumination, another key maintaining factor of PGD [32,42]. Decentering refers to the capacity to experience thoughts and affective states as objective and passing phenomena rather than as accurate reflections of reality or of the self [31,92,93]. This shift reduces cognitive fusion and promotes what has been described as cognitive defusion—viewing catastrophic or absolute thoughts (e.g., “I cannot continue my life without him/her”, “Life has permanently lost its meaning”, etc.) as mental events rather than truths [92,94].
Grief-related rumination is characterized by repetitive, prolonged, and recurrent thinking focused on the loss and its consequences, and represents a key maintaining fac-tor in prolonged grief symptomatology [55]. Mindfulness may interrupt this cycle through attentional training mechanisms [93]. Specifically, mindfulness practice cultivates the capacity to notice when the mind drifts toward ruminative content and to intentionally redirect attention toward a neutral present-moment anchor, such as the breath or bodily sensations [31,95]. This repeated shifting of attentional focus strengthens cognitive flexibility and may reduce automatic immersion in grief-related thought patterns. For example, qualitative evidence from the Existential Behavioral Therapy (EBT) model (which heavily utilizes MBCT exercises) shows that participants use present-moment anchors—such as the breath or nature (the smell of woods, the reflection of trees on water)—to exit the “vicious cycle” of ruminative thinking [44]. Through the development of “letting go,” individuals learn not to suppress intrusive thoughts but to disengage from rigid cognitive loops, thereby weakening maladaptive perseverative processing [93]. This form of psychological distancing may facilitate gradual acceptance of the reality of the loss without reinforcing avoidance [95,96]. Importantly, the notion of “letting go” in mindfulness should not be conflated with the classical psychoanalytic idea of withdrawing libidinal investment from the deceased, as described by Freud [97]. Contemporary bereavement theory has challenged the assumption that adaptive mourning requires detachment. For instance, the Continuing Bonds perspective posits that maintaining an on-going inner relationship with the deceased can represent a protective and integrative process, involving a transformation from love in physical presence to love in symbolic or internalized absence [22]. Within this framework, mindful letting go refers not to relinquishing the bond with the deceased, but to releasing maladaptive cognitive entanglement, thereby allowing the relationship to be integrated in a more flexible and less distressing form.
Neuroimaging findings provide biological support for the proposed role of mindfulness in reducing grief-related rumination and cognitive fusion. For instance, MBCT has been shown to enhance executive control and emotion regulation, with changes in resting-state connectivity linked to improved attentional flexibility [39,40,94]. At the attentional level, mindfulness practice strengthens the anterior cingulate cortex (ACC), a region central to conflict monitoring and attentional regulation [31]. A more efficient ACC may facilitate early detection of attentional drift toward ruminative content, enabling flexible redirection toward present-moment awareness. In this way, neuroplastic changes associated with mindfulness training support decentering and cognitive defusion, weakening the “thought trap” characteristic of grief rumination. The cultivation of meta-awareness creates a psychological “gap” between stimulus and response, allowing painful memories or affective surges to be recognized without immediate immersion [92,94]. In parallel, mindfulness may shift processing from a narrative, self-referential mode toward a more experiential mode of awareness, reducing the subjective and identity-based centrality of grief experiences [31,92,96].
From a constructivist and meaning-centered perspective, the mechanisms described above can be coherently interpreted within Neimeyer’s theory of meaning reconstruction, which conceptualizes bereavement as an active process of rebuilding disrupted assumptive worlds rather than merely attenuating symptoms [21,98]. Grief-related rumination often reflects an attempt to restore coherence in a disrupted assumptive world; however, when rigid and self-referential, it may instead perpetuate distress. Through decentering and attentional flexibility, mindfulness weakens cognitive fusion with catastrophic or identity-defining narratives, thereby creating psychological space for alternative meaning-making processes to emerge. Neurocognitive adaptations may support this shift from perseverative narrative processing toward a more flexible, experiential engagement with loss. In this sense, mindfulness does not eliminate the search for meaning; rather, it trans-forms the mourner’s relationship to meaning-making itself, allowing reconstruction to unfold without the rigid amplification characteristic of prolonged grief. For example, in the study by [52], bereaved parents described a profound shift in self-appraisal: they moved from perceiving themselves as “crazy” for the intensity of their grief to recognizing that “I suffer because I loved” [52]. This reframing represents an instance of meaning reconstruction, whereby emotional pain is no longer interpreted as a pathological symptom requiring elimination, but as a coherent and intelligible response to attachment and love. In this sense, grief becomes recontextualized not as evidence of dysfunction, but as testimony to the enduring relational bond.
Third, self-compassion emerges as a resilience factor, associated with adaptive psychological functioning and reduced self-criticism [94,99]. Interventions embedding compassion practices foster common humanity, mitigating isolation and stigma, and supporting bereaved families in contexts of traumatic loss [99].
Guilt and shame frequently play a central and often debilitating role in bereavement, acting as significant maintaining factors in prolonged grief symptomatology [100]. While guilt typically involves negative evaluation of a specific behavior (e.g., “I should have done more”), shame reflects a global negative evaluation of the self, often accompanied by feelings of worthlessness, powerlessness, and withdrawal. These affective states may obstruct adaptive mourning by predicting more intense grief reactions and elevated symptoms of anxiety, depression, and post-traumatic stress [101]. In cases of suicide bereavement, guilt and shame may be further exacerbated by social stigma and perceived abandonment, leading survivors to conceal the cause of death and to withdraw socially [49,50]. Cultural expectations regarding what constitutes “normal” grieving can additionally intensify shame when individuals feel unable to meet perceived standards of recovery [101]. Within this framework, MBIs cultivate self-compassion through three interrelated components: non-judgmental awareness, self-kindness, and common humanity [81]. Mindful awareness enables individuals to observe guilt- and shame-related thoughts as transient mental events rather than as objective truths or reflections of a fixed identity, thereby reducing over-identification with a “defective self” [96]. Self-kindness directly counteracts harsh self-criticism by fostering an attitude of care toward one’s own suffering. Instead of engaging in punitive internal dialogue, bereaved individuals are encouraged to relate to themselves with the same compassion they would extend to a close friend in distress [99]. The recognition of common humanity reduces the isolating and stigmatizing effects of shame. Acknowledging that suffering, imperfection, and loss are universal aspects of the human condition can normalize grief reactions and restore a sense of belonging, thereby buffering against social withdrawal [99]. For example, The Panta Rhei retreats explicitly utilize the exercise “How would I treat a friend?” to help participants realize the disparity between the compassion they offer others and the harshness they direct toward themselves [49,50].
Beyond its psychological effects, emerging neuroscientific evidence suggests that self-compassion is associated with measurable neural and psychophysiological adaptations. At the structural level, higher self-compassion has been linked to reduced fractional anisotropy in the right superior longitudinal fasciculus (SLF), a white-matter tract connecting the inferior parietal lobule (IPL) and prefrontal regions [102]. Given that the IPL is a key node of both the mirroring network and the Default Mode Network (DMN), these findings suggest that self-compassion may attenuate maladaptive self-referential processing and mind-wandering, thereby reducing grief-related rumination. The mirroring network—comprising the inferior frontal gyrus (IFG), IPL, insula, and anterior cingulate cortex (ACC)—is classically implicated in empathy toward others [102]; generating compassion toward oneself may recruit similar circuits, enabling bereaved individuals to re-late to their own suffering with care and understanding rather than self-criticism.
At the functional level, prolonged grief has been associated with hyperactivation of DMN regions, particularly the posterior cingulate cortex (PCC) and thalamus, which sustain intrusive self-referential thoughts and affective distress [39,40]. As a core component of mindfulness-based approaches, self-compassion may facilitate a shift from a narrative-evaluative self toward an experiential mode of awareness [31]. Compassion-focused practices have been associated with reduced PCC and thalamic activity, suggesting diminished emotional interference and attenuation of catastrophic self-narratives related to the loss [39].
Self-compassion also appears to modulate the autonomic threat system. It has been proposed as a stronger predictor of vagally mediated heart rate variability (vmHRV) than mindfulness alone, indicating enhanced psychophysiological flexibility and stress regulation [103]. Neuroimaging studies further suggest that adopting a compassionate stance toward one’s own suffering down-regulates neural markers of negative affect, whereas self-criticism and self-blame activate threat-related regions such as the amygdala and dorsal ACC [102,103]. In bereavement contexts characterized by intense guilt or shame, this regulatory shift may buffer against sustained threat activation.
Finally, MBIs often integrate holistic mind–body practices, such as yoga or other MBSR exercises, which reduce stress and depressive symptoms in perinatal bereavement and other traumatic losses [26,41,43,48]. Improvements in sleep quality, frequently disrupted in grief, may further mediate these benefits [26,39,54].
In sum, MBIs provide tools to address maladaptive grief processes—particularly avoidance and rumination [32,104]—while enhancing acceptance, decentering, and self-compassion. By doing so, they may not only alleviate suffering but also foster post-traumatic growth and meaning reconstruction in bereavement [105].
4.2. Clinical Implications
Mindfulness-based approaches may be especially appropriate in cases of traumatic or high-risk bereavement. Emerging evidence suggests potential benefits for mothers experiencing stillbirth or early pregnancy loss [37,46,48], as well as for individuals be-reaved by suicide, where shame, stigma, and self-blame are particularly prominent [49,50]. In such contexts, mindfulness and self-compassion practices may help regulate intense affective arousal, reduce maladaptive cognitive loops, and support gradual emotional integration.
These interventions may also serve as a secondary preventive function for individuals presenting with elevated grief-related distress who do not yet meet full diagnostic criteria for PGD. Early incorporation of mindfulness-based strategies may reduce rumination, experiential avoidance, and emotional dysregulation, potentially mitigating progression toward more persistent symptomatology [42].
Mindfulness-based approaches may further be considered when grief-focused cognitive-behavioral therapy (CBT) becomes clinically stalled due to the overwhelming intensity of trauma-related affect. In such cases, mindfulness does not require immediate explicit confrontation with loss-related material but instead cultivates distress tolerance and pre-sent-moment awareness, which may enhance emotional regulation and prepare patients for subsequent trauma-focused work [38].
Nevertheless, clinical timing remains crucial. In the very acute phase of bereavement (generally within the first three months), intensive open-monitoring or deep experiential practices may be less appropriate than interventions emphasizing emotional containment, stabilization, and relational support [50]. Gradual, titrated introduction of brief and structured mindfulness exercises may therefore be preferable, ensuring that engagement with painful affect remains within tolerable limits.
The clinical implementation of mindfulness-based approaches in bereavement care requires both therapist preparation and the use of structured intervention models. A foundational element is the therapist’s own contemplative practice. Regular personal engagement in mindfulness meditation may enhance attunement, empathic presence, and affect regulation within the therapeutic relationship, thereby modeling embodied awareness and emotional containment for the bereaved individual [38]. Such therapist presence is particularly relevant in grief work, where relational safety and emotional resonance are central.
Structured frameworks may guide clinical applications. The ATTEND model provides a relationally grounded, mindfulness-informed approach to traumatic bereavement [53,106]. This model emphasizes compassionate presence, validation, and psychoeducation about grief processes, integrating mindfulness principles into a coherent therapeutic stance.
Specific practices can be flexibly incorporated depending on clinical presentation:
- The 3-Minute Breathing Space may be used to help patients regulate acute waves of emotional activation, fostering brief but structured moments of grounding and attentional stabilization [89,105].
- Loving-Kindness (Metta) meditation may support the transformation of anger, resentment, or self-directed hostility, particularly in contexts of traumatic or stigmatized loss [49,50].
- Self-compassion–focused exercises (e.g., structured cognitive reframing practices aimed at identifying self-critical “thought traps”) may be especially helpful for be-reaved clients struggling with guilt and self-blame [99].
In addition, integrating mind–body techniques may enhance accessibility for patients who initially find seated meditation difficult or destabilizing. Progressive Muscle Relaxation (PMR), for example, has demonstrated benefits in bereaved populations and may serve as a somatic entry point to emotion regulation by reducing physiological tension associated with grief [42]. Such integration underscores the importance of tailoring interventions to the individual’s regulatory capacity and readiness.
Overall, mindfulness-based grief interventions appear most effective when delivered within a relationally attuned, structured, and gradually introduced clinical framework rather than as decontextualized meditation practices.
4.3. Future Directions
These limitations highlight important directions for future research. Larger, methodologically rigorous randomized controlled trials (RCTs) are needed to establish the efficacy of MBIs for bereavement, particularly in populations at risk for PGD [106]. Future research should include direct comparisons with established “gold standard” treatments, such as grief-focused cognitive behavioral therapy (GF-CBT), to clarify differential efficacy and identify which subgroups may benefit most from each modality. Longitudinal designs with follow-up assessments extending to 6–12 months or beyond are essential to evaluate the durability of treatment gains [24,89].
Second, greater diversification of study populations is warranted. Existing research has relied predominantly on White, female, and highly educated samples, limiting generalizability. Future trials should prioritize the inclusion of males and individuals from di-verse ethnic, racial, and socioeconomic backgrounds. Tailored investigations for high-risk contexts—such as suicide bereavement, gun violence, and perinatal loss—remain particularly important.
Third, refinement of outcome measurement is needed. Researchers should consistently employ validated grief-specific instruments (e.g., PG-13, ICG, TRIG) [32], while integrating multi-method assessments, including physiological markers (e.g., heart rate variability), neuroimaging, and behavioral indices, to complement self-report measures. Beyond symptom reduction, future studies should also assess positive adaptation outcomes, such as life satisfaction, personal growth, and meaning reconstruction.
Fourth, mechanistic and process-oriented research is critical to identify the active ingredients of MBIs. Studies should examine whether specific mindfulness facets (e.g., non-judging, decentering) mediate therapeutic change [26,94], explore dose–response relationships, and clarify the optimal timing of intervention across acute versus chronic phases of bereavement.
Finally, future research should expand to examine systemic and intergenerational impacts. For example, investigating the psychological well-being of partners and children when a family member engages in an MBI may clarify broader family-level effects. In peri-natal loss, longitudinal studies examining outcomes in subsequent pregnancies may pro-vide valuable insight into the enduring protective effects of mind–body interventions.
5. Conclusions
Although the current evidence remains limited and heterogeneous, MBIs show promise as adjunctive interventions in bereavement care. By targeting transdiagnostic mechanisms of adaptation, they hold potential to complement established grief therapies and to address unmet needs in populations vulnerable to prolonged or complicated grief. Future high-quality studies are essential to establish their efficacy, clarify their mechanisms of action, and determine their place within evidence-based bereavement interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kabat-Zinn J. Wherever You Go, There You Are: Mindfulness Meditation in Everyday Life Hyperion New York, NY, USA 1994
- 2Bishop S.R. Lau M. Shapiro S. Carlson L. Anderson N.D. Carmody J. Segal Z.V. Abbey S. Speca M. Velting D. Mindfulness: A proposed operational definition Clin. Psychol. Sci. Pract.20041123024110.1093/clipsy.bph 077 · doi ↗
- 3Kabat-Zinn J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain and Illness Dell Publishing New York, NY, USA 1990
- 4Currie C.L. Larouche R. Voss M.L. Trottier M. Spiwak R. Higa E. Scott D.R. Tallow T. Effectiveness of Live Health Professional-Led Group e Health Interventions for Adult Mental Health: Systematic Review of Randomized Controlled Trials J. Med. Internet Res.202224 e 2793910.2196/2793934878409 PMC 8790691 · doi ↗ · pubmed ↗
- 5Segal Z.V. Williams J.M.G. Teasdale J.D. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse Guilford Press New York, NY, USA 2002 xiv, 351
- 6Zhang D. Lee E.K.P. Mak E.C.W. Ho C.Y. Mindfulness-based interventions: An overall review Br. Med. Bull.2021138415710.1093/bmb/ldab 00533884400 PMC 8083197 · doi ↗ · pubmed ↗
- 7Shapero B.G. Greenberg J. Pedrelli P. de Jong M. Desbordes G. Mindfulness-Based Interventions in Psychiatry Focus 201816323910.1176/appi.focus.2017003929599651 PMC 5870875 · doi ↗ · pubmed ↗
- 8Linehan M.M. Cognitive-Behavioral Treatment of Borderline Personality Disorder; Diagnosis and Treatment of Mental Disorders Guilford Press New York, NY, USA 1993 xvii, 558