Deep Brain Stimulation for Movement Disorders in Spain: Temporal Trends, Complications, and Sex-Related Disparities (2002–2019)
Víctor Gómez-Mayordomo, Jose J. Zamorano-León, David Carabantes-Alarcon, Valentín Hernández-Barrera, Ana Lopez-de-Andrés, Natividad Cuadrado-Corrales, Fernando Alonso-Frech, Ana Jiménez-Sierra, Rodrigo Jiménez-García

TL;DR
This study analyzed DBS trends in Spain from 2002 to 2019, finding increased use, shorter hospital stays, and sex-related disparities in treatment.
Contribution
The study provides a comprehensive nationwide analysis of DBS trends, complications, and sex disparities in Spain over 17 years.
Findings
DBS use for movement disorders increased significantly, with shorter hospital stays over time.
Men accounted for 60% of DBS procedures for Parkinson’s and essential tremor, with women undergoing surgery at older ages.
Hardware-related issues and infections were the most common complications, especially during explantations.
Abstract
Background/Objectives: This study aimed to describe temporal trends in deep brain stimulation (DBS) use for Parkinson’s disease (PD), essential tremor (ET), and dystonia; characterize patient age and sex distribution and comorbidity; assess postoperative complications and in-hospital mortality (IHM) after implantation and explantation; and explore sex-specific differences in utilization and outcomes. Methods: We conducted a retrospective nationwide population-based study using the Spanish National Hospital Discharge Database (RAE-CMBD) from 2002 to 2019. All hospital admissions with DBS implantation or explantation/revision and a diagnosis of PD, ET, or dystonia were identified. Sociodemographic variables, the Charlson Comorbidity Index (CCI), length of hospital stay (LOHS), postoperative complications, and IHM were analyzed across three calendar periods and stratified by diagnosis and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
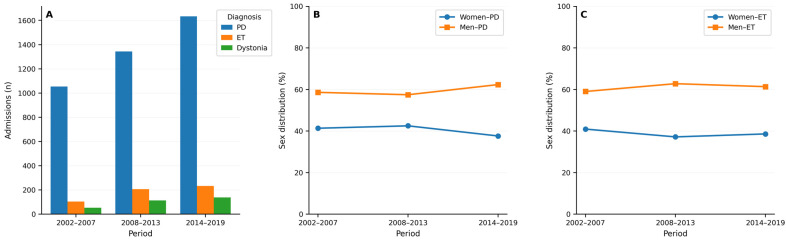 Figure 1
Figure 1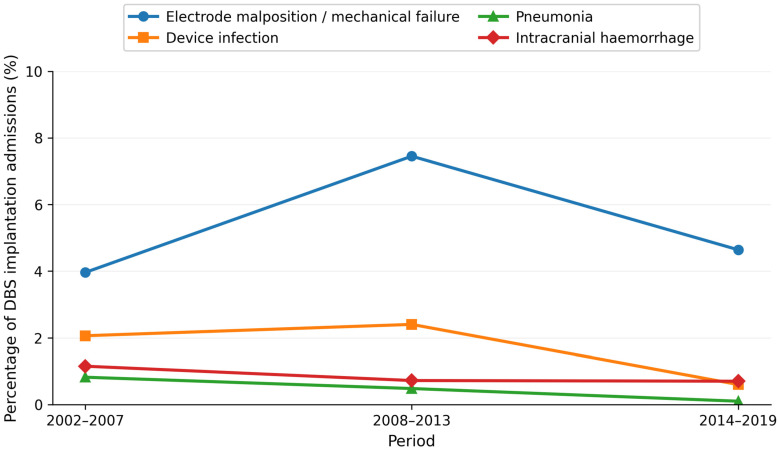 Figure 2
Figure 2- —Universidad Complutense de Madrid, Grupo de Investigación en Epidemiología de las Enfermedades Crónicas de Alta Prevalencia en España
- —Grupo de Investigación en Biomedicina Predictiva e Investigación Traslacional en las Enfermedades Respiratorias, Cardiovasculares y Metabólicas of the Health Research Institute of the Hospital Clínico
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological disorders and treatments · Parkinson's Disease Mechanisms and Treatments · Parkinson's Disease and Spinal Disorders
1. Introduction
Movement disorders such as Parkinson’s disease (PD), essential tremor (ET), and dystonia are common chronic neurological conditions and a major cause of disability worldwide [1,2,3,4]. PD is the second most common neurodegenerative disease, and its global prevalence is projected to rise substantially in the coming decades as the age of the population increases [1,2]. ET is considered the most prevalent isolated tremor disorder, often leading to marked functional impairment [3]. Focal and generalized dystonias, although less common, can cause severe, long-lasting motor disability, pain, and social stigma [4]. Together, these disorders impose a considerable burden on patients, caregivers, and health systems in terms of loss of independence, reduced quality of life, and increased healthcare utilization and costs [5].
Deep brain stimulation (DBS) has become an established surgical treatment for selected patients with movement disorders whose symptoms are insufficiently controlled with pharmacological therapy. Since its introduction in the 1990s, DBS of the subthalamic nucleus or internal globus pallidus has been shown in randomized controlled trials and long-term observational studies to improve motor symptoms, reduce motor complications, and enhance quality of life in advanced PD compared with best medical therapy alone [6,7]. Thalamic (ventral intermediate nucleus) DBS is an effective option for medication-refractory ET, and pallidal DBS is an accepted treatment for certain forms of dystonia, including primary generalized and segmental dystonia and some monogenic dystonias [8,9,10]. International guidelines now recommend DBS as a key component of the therapeutic armamentarium for appropriately selected patients with PD, ET, and dystonia [11,12,13].
Despite its benefits, DBS is a complex and resource-intensive intervention that carries specific risks. Most common complications are largely related to the implanted hardware, such as lead malposition, migration or fracture, pulse-generator malfunction, and device or wound infection, whereas perioperative complications include intracranial hemorrhage, seizures, and systemic medical events [14,15]. These complications may necessitate surgical revision or explantation of the system and are associated with prolonged hospital stays, additional costs, and in rare cases, serious morbidity or mortality [16]. Reported complication rates vary widely across centres and studies, partly due to differences in patient selection, surgical technique, follow-up duration, and definitions of adverse events [15,17]. Most available data come from single-centre series or clinical trials, which typically involve relatively small, highly selected cohorts and may not fully reflect routine clinical practice.
Over the past three decades, the indications and use of DBS have progressively expanded, and patient selection criteria have evolved. Improvements in imaging, surgical targeting, and perioperative management, together with growing surgical experience, have likely facilitated safer procedures and may have encouraged the treatment of older patients and those with greater comorbidity in routine clinical practice [18,19]. At the same time, concerns have been raised about potential inequities in access to advanced therapies [20,21]. However, evidence on sex-related patterns in DBS use remains limited and heterogeneous, and robust population-based data stratified by underlying movement disorders are scarce.
Despite nearly three decades of DBS activity in Spain, there is a lack of nationwide data specifically addressing the hospital burden of DBS implantation and explantation for movement disorders and the associated postoperative complications. A comprehensive, diagnosis- and sex-specific description of patients undergoing DBS, their comorbidity burden, and the spectrum and temporal evolution of perioperative complications is essential to inform patient counselling, refine selection criteria, and anticipate resource needs. This is also relevant from a public health perspective, as the number of potential candidates for DBS is expected to increase in parallel with the projected rise in the prevalence of PD and other movement disorders [22,23,24].
According to this, administrative health databases and national hospital discharge registries provide an opportunity to overcome some of these limitations by enabling the analysis of large, unselected cohorts over long time periods. In Spain, the Spanish National Hospital Discharge Database (RAE-CMBD) compiles standardized information on virtually all discharges from public hospitals, including demographic variables (sex and age), diagnoses, procedures, length of hospital stay, and in-hospital mortality [25,26].
In this context, we conducted a retrospective, nationwide, population-based study using the RAE-CMBD to characterize hospital admissions for DBS implantations and explantations or surgical revision due to movement disorders in Spain from 2002 to 2019. Our objectives were to: (1) describe long-term temporal trends in the use of DBS for PD, ET, and dystonia; (2) define the demographic and clinical profile of hospitalizations undergoing DBS, including age and comorbidity patterns; (3) quantify the frequency and evolution over time of postoperative complications and in-hospital mortality after DBS implantation and explantation; and (4) explore sex-specific differences in DBS utilization and outcomes, particularly among hospitalizations with PD and ET.
2. Materials and Methods
2.1. Study Design and Data Source
We conducted a retrospective, nationwide, population-based observational study using data from the Spanish National Hospital Discharge Database (Registro de Altas del Conjunto Minimo Basico de Datos; RAE-CMBD). This database is managed by the Spanish Ministry of Health and compiles information on virtually all discharges from public hospitals in Spain, covering more than 95% of all hospital admissions in the national health system. The RAE-CMBD includes demographic variables such as sex and date of birth, admission and discharge dates, discharge destination (e.g., home, death, transfer), and multiple diagnosis (up to 20) and procedure (up to 20) fields coded according to the Spanish adaptations of the International Classification of Diseases (ICD). A detailed description of the design, coverage, and data collection procedures of this registry has been published by the Ministry of Health [25].
During the study period, diagnoses and procedures were coded using ICD-9-CM until 2015 and ICD-10-ES from 2016 to 2019, following the transition previously described [25,26].
2.2. Study Population
We identified all hospitalizations recorded in the RAE-CMBD between 1 January 2002 and 31 December 2019 in which a DBS procedure for a movement disorder was coded. Two cohorts of admissions were defined: hospitalizations with codes indicating DBS electrode implantation and hospitalizations with codes indicating explantation, removal, or revision of existing DBS hardware.
To restrict the analysis to DBS procedures performed for movement disorders, we included only those admissions in which at least one diagnostic field contained a code compatible with Parkinson’s disease, essential tremor, or dystonia, using ICD-9-CM and ICD-10-ES codes that have been previously applied in administrative data analyses of Parkinsonian disorders [26]. No age restriction was applied.
Because the RAE-CMBD is an anonymized discharge-level database and does not include unique patient identifiers, multiple hospitalizations from the same individual cannot be linked. Consequently, each eligible admission was analyzed as a separate event and reported per hospitalization episode, reflecting the hospital burden associated with DBS implantation and explantation/revision procedures, as done in previous national studies based on this registry. We restricted the study period to 2002–2019 to avoid COVID-19-related disruptions in hospital activity from 2020 onwards, which could artefactually affect temporal trends.
2.3. Variables
For each hospitalization, we obtained sociodemographic information (age at admission and sex), clinical data (type of movement disorder and comorbidity burden), and outcomes related to the hospital stay.
Age was treated both as a continuous variable and categorized into five groups (<40, 40–49, 50–59, 60–69, and ≥70 years), following the stratification used in our tables to describe the age distribution of patients undergoing DBS implantation and explantation/revision. Sex was classified as male or female according to the RAE-CMBD record.
The diagnosis of the type of movement disorder was classified into three mutually exclusive categories: Parkinson’s disease, essential tremor, or dystonia. This classification was based on the presence of the corresponding ICD codes in any diagnostic position. In those few admissions in which more than one of these diagnoses co-occurred, a hierarchical rule was applied to assign a single underlying condition for descriptive purposes, prioritizing Parkinson’s disease, then essential tremor, and finally dystonia.
Overall comorbidity was summarized using the Charlson Comorbidity Index (CCI), calculated from all diagnosis fields recorded at discharge with validated algorithms for ICD-9-CM and ICD-10 administrative data [27]. We categorized the CCI into three groups (0, 1, and ≥2) to describe the distribution of comorbidity burden among hospitalizations and its evolution over time. None of the movement disorder diagnoses are included in the CCI, and therefore, they were not considered in the calculation of the index.
For each admission, we calculated the length of hospital stay (LOHS) as the difference in days between admission and discharge dates. In-hospital mortality (IHM) was defined as any death occurring during the index hospitalization as recorded in the discharge status field of the RAE-CMBD.
2.4. Postoperative Complications
Postoperative complications were identified using specific diagnosis and procedure codes recorded during the same hospitalization in which the DBS procedure took place. For DBS implantation admissions, we examined hardware-related complications (such as electrode malposition or lead migration, mechanical failure or malfunction of the device, and a need for surgical revision of the system), infectious complications (including device or pocket infection, postoperative wound infection, central nervous system infection, and sepsis), neurological complications (intracranial hemorrhage, epileptic seizures, and delirium), and systemic complications (pneumonia, deep vein thrombosis, pulmonary embolism, and acute renal failure). We also assessed the need for blood transfusion and for mechanical ventilation as indicators of procedure-related complexity and resource use. These procedures and diagnoses were identified in any position of the database.
The same set of complications was evaluated for admissions involving DBS explantation or surgical revision. In this cohort, particular attention was paid to the presence of device infection and hardware malfunction, as these are common indications for DBS system removal reported in the literature.
The ICD-9-CM and ICD-10-ES codes used to define all diagnoses, procedures, and complications are listed in Supplementary Table S1.
2.5. Time Periods and Stratified Analyses
To examine long-term temporal trends while minimizing the impact of year-to-year variability, the 18-year study period was a priori divided into three consecutive 6-year intervals (2002–2007, 2008–2013, and 2014–2019). This grouping guaranteed sufficient numbers of procedures in each stratum, especially for less prevalent diagnoses and interventions, and allowed robust comparisons over time, including subgroup analyses by diagnosis and sex. All analyses were conducted separately for DBS implantation and DBS explantation/revision admissions. Within these two cohorts, results were stratified by underlying movement disorder and, for Parkinson’s disease and essential tremor, by sex, following the approach used in previous RAE-CMBD-based studies on Parkinson’s disease hospitalizations in Spain [26].
2.6. Statistical Analysis
We first performed a descriptive analysis of all hospitalizations for DBS implantation and explantation. Continuous variables are shown as mean with standard deviation (SD) or as median with interquartile range (IQR) according to their normal distribution (Kolmogorov–Smirnov test). Categorical variables are reported as absolute frequencies and percentages.
To compare the distribution of study variables, we used the Chi-square test, or the Fisher exact test when required, for categorical variables. For continuous variables with normal distribution, we applied the Student t-test or analysis of variance (ANOVA), whereas for non-normally distributed variables, we used the U of Mann–Whitney or Kruskal–Wallis tests. The methods used to assess potential changes in the distribution of the variables over time included the Cochran–Mantel–Haenszel statistic or Cochran–Armitage test for categorical variables and the linear regression t-test or Jonckheere–Terpstra test for continuous variables.
The RAE-CMBD is an anonymized administrative database that is curated and quality-controlled by the Spanish Ministry of Health prior to release. For this study, the Ministry provided an anonymized, cleaned record-level extract for the study period. The final analytic outputs (tables/figures and key counts) were reviewed by the investigator group to ensure internal consistency and accuracy.
All statistical tests were two-sided, and a p-value < 0.05 was considered statistically significant. Statistical analyses were conducted using SPSS version 29.0.2.0 (IBM Corp., Armonk, NY, USA).
2.7. Ethical Considerations
The RAE-CMBD is an anonymized administrative database that does not contain direct personal identifiers. According to Spanish legislation on biomedical research and data protection, the use of fully anonymized secondary data provided by public institutions does not require informed consent from patients and exemption of evaluation and approval by a research ethics committee is granted [28]. Access to the RAE-CMBD can be obtained from the Spanish Ministry of Health upon submission of a formal data request [29].
3. Results
3.1. Characteristics and Temporal Trends of DBS Implantations
From 2002 to 2019, a total of 4883 hospital admissions for DBS electrode implantation due to movement disorders were recorded in Spain. The number of implantations increased steadily across the three time periods, from 1213 admissions in 2002–2007 to 1664 in 2008–2013 and 2006 in 2014–2019 (p < 0.001, Table 1).
PD was the main indication for DBS throughout the study, accounting for 4031 admissions (82.6%), followed by ET (545; 11.2%) and dystonia (307; 6.3%). The proportion of PD showed a modest decline over time (86.9% in 2002–2007 vs. 81.5% in 2014–2019; p < 0.001), whereas ET and dystonia increased slightly (ET 8.7% to 11.6%; dystonia 4.5% to 6.9%).
The mean age of hospitalizations undergoing DBS implantation for any movement disorder was 59.45 years (SD 11.67) and decreased slightly but significantly over the study period (60.27 years in 2002–2007 vs. 59.05 in 2014–2019; p = 0.009). Most procedures were performed in hospitalizations aged 60–69 years (43.2%), followed by those aged 50–59 years (24.9%). The proportion of hospitalizations aged ≥70 years declined from 18.2% in the first period to 13.6% in the last (p < 0.001).
Comorbidity burden, as measured by the grouped CCI, was generally low. Overall, 87.8% of admissions had a CCI of “0”, 9.7% had a CCI of “1”, and only 2.5% had a CCI “≥2”. However, there was a statistically significant increase in the proportion of hospitalizations with at least one comorbidity (CCI ≥ 1) over time (from 9.6% in 2002–2007 to 13.9% in 2014–2019; p = 0.012).
LOHS decreased markedly during the study period. The median LOHS for DBS implantation fell from 12 days (IQR 9) in 2002–2007 to 8 days (IQR 6) in 2008–2013 and 6 days (IQR 5) in 2014–2019 (p < 0.001). In parallel, IHM after DBS implantation declined significantly, from 0.82% in the first period to 0.12% in 2008–2013 and 0.05% in 2014–2019 (overall IHM 0.27%, p < 0.001 for trend).
3.2. DBS Implantation in Parkinson’s Disease According to Sex
Among the 4031 DBS implantation admissions for PD, 2409 (59.8%) occurred in men and 1622 (40.2%) in women (Table 2 and Figure 1).
In men with PD, the number of implantations increased from 618 in 2002–2007 to 772 in 2008–2013 and 1019 in 2014–2019 (p < 0.001). Mean age remained stable around 60 years (60.8, 60.28, and 59.26 years in the three periods; p = 0.087), with most procedures performed in the 60–69-year group (44.1% overall). The proportion of men aged ≥70 years showed a modest decrease over time (16.2% to 10.5%; p = 0.020 for age categories). Comorbidity burden was low: 87.1% of male admissions had CCI = 0, 10.3% CCI = 1, and 2.6% CCI ≥ 2, with no statistically significant change in this distribution over time (p = 0.067). Median LOHS decreased from 12 days (IQR 10) to 8 days (IQR 6) and 6 days (IQR 5) (p < 0.001). IHM in men with PD was 0.25% overall (six deaths), with a clear decrease over time, although not significant (p = 0.070).
In women with PD, the number of implantations also increased steadily (from 436 to 571 and 615 admissions across the three periods; p < 0.001). Women were slightly older than men (overall mean age 61.9 vs. 60.0 years, p = 0.038), and half of the procedures were performed in those aged 60–69 years (51.3%). The proportion aged ≥70 years declined from 18.6% to 13.7% (p = 0.179 for age categories). Comorbidity was very low: 91.7% of female admissions had CCI = 0, and only 1.5% had CCI ≥ 2, without significant variation over time (p = 0.254). As in men, LOHS decreased significantly in women (median 12, 8, and 7 days; p < 0.001). IHM was 0.25% overall (four deaths), and a significant decline was observed across periods (p = 0.004).
3.3. DBS Implantation in Essential Tremor According to Sex
A total of 545 DBS implantation admissions were identified for ET, of which 335 (61.5%) occurred in men and 210 (38.5%) in women (Table 3 and Figure 1).
In men with ET, the number of implantations rose from 62 in 2002–2007 to 130 in 2008–2013 and 143 in 2014–2019 (p < 0.001). Mean age was around 62 years and remained stable (61.39, 62.37, and 62.54 years; p = 0.337). Across the whole period, 38.4% of male implantations were in the 60–69-year group and 27.6% in those ≥70 years. Comorbidity burden was modest, with 75.5% of admissions having CCI = 0 and 6.0% CCI ≥ 2; no significant changes in comorbidity distribution over time were observed (p = 0.522). Median LOHS decreased from 9.5 days (IQR 5) to 7 (IQR 7) and 5 (IQR 4) (p = 0.035). IHM in men with ET was very low (0.3%, 1 death) and did not change significantly over time (p = 0.110).
In women with ET, the total number of implantations increased from 43 to 77 and 90 across the three periods (p < 0.001). More than one-third of female implantations were performed in patients aged ≥70 years (36.7%) and 29.5% in those aged 60–69 years. Comorbidity remained low and stable over time (CCI = 0 in 78.1%, CCI ≥ 2 in 3.8%; p = 0.680). However, LOHS decreased markedly, from a median of 14 days (IQR 8) in 2002–2007 to 8 days (IQR 6) in 2008–2013 and 5 days (IQR 4) in 2014–2019 (p < 0.001). IHM was 0.95% (two deaths), with no significant temporal variation (p = 0.402).
Overall, these results indicate that DBS for ET was performed in slightly older hospitalizations than for PD, with a sizeable proportion of procedures in individuals aged ≥70 years, but with similarly low comorbidity and in-hospital mortality.
3.4. Postoperative Complications After DBS Implantation
During the study period, 713 of the 4883 DBS implantation admissions (14.6%) had at least one coded postoperative complication (Table 4). The distribution of underlying diagnoses among these complicated admissions was similar to that of the full cohort: 81.9% PD, 11.4% ET, and 6.7% dystonia, with no significant change over time.
Among all DBS implantations, the most frequent specific complications were electrode malposition or mechanical failure in 265 admissions (5.43%), device infection in 77 (1.58%), intracranial hemorrhage in 40 (0.82%), pneumonia in 20 (0.41%), and epileptic seizures in 52 (1.06%). The need for mechanical ventilation was recorded in 46 admissions (0.94%) and blood transfusion in 30 (0.61%).
Temporal patterns varied by complication. Rates of electrode malposition or mechanical failure peaked in 2008–2013 (7.45%) and were lower in the first and last periods (3.96% and 4.64%; p < 0.001). Device infection was more frequent in the first two periods (2.06% and 2.40%) and decreased to 0.60% in 2014–2019 (p < 0.001). Pneumonia also declined significantly over time (0.82%, 0.48%, and 0.10%; p = 0.007). The frequency of epileptic seizures showed a modest but statistically significant decrease (1.57%, 0.60%, and 1.15%; p = 0.040). For most other complications, absolute numbers were very low, and temporal differences did not reach statistical significance (Figure 2).
When complication rates were examined by underlying diagnosis (Supplementary Table S2), hardware-related problems and device infection were similarly frequent across PD, ET, and dystonia. For example, electrode malposition or mechanical failure affected 5.6% of PD admissions, 5.1% of ET, and 3.6% of dystonia admissions, with no significant differences between groups. However, pneumonia was significantly more common in ET than in PD (0.92% vs. 0.30%; p = 0.026), and epileptic seizures, blood transfusion, and mechanical ventilation occurred slightly more often in patients with dystonia, although absolute numbers were small. Also, several complications, such as ischemic stroke and blood transfusion, were rare (<1% of implantation admissions) and should be interpreted cautiously as admission-level coded events rather than definitive procedure-attributable complications.
3.5. Characteristics of DBS Explantations and Associated Complications
Over the same period, 497 hospital admissions for DBS surgical revisions or explantation/revision were identified (Table 5). The number of procedures increased from 82 in 2002–2007 to 131 in 2008–2013 and 284 in 2014–2019. Most explant admissions occurred in patients hospitalized with PD (425; 85.5%), followed by ET (38; 7.7%) and dystonia (34; 6.8%). Men represented 64.0% of explant admissions.
The mean age of hospitalizations undergoing DBS surgical revision was 62.3 years (SD 11.5) and did not change significantly over time (61.39, 62.37, and 62.54 years in the three periods; p = 0.790). Overall, 38.4% of admissions concerned patients aged 60–69 years and 27.6% of those aged ≥70 years. Comorbidity burden remained low but showed a significant temporal shift: the proportion of admissions with CCI = 0 decreased from 93.9% to 82.0%, whereas those with CCI = 1 increased from 2.4% to 14.1% (p = 0.007). Admissions with CCI ≥ 2 remained infrequent (3.0% overall).
As observed for implantations, LOHS for surgical revisions shortened over time. Median LOHS decreased from 13 days (IQR 10) in 2002–2007 to 7 days (IQR 11) in 2008–2013 and 5 days (IQR 8) in 2014–2019 (p < 0.001). IHM after DBS explantation/revision was 0.6% (three deaths, one in each period), with no significant differences across periods (p = 0.646).
Regarding complications specifically associated with explantation/revision (Supplementary Table S3), device infection was recorded in 165 admissions (33%) and electrode malposition or mechanical failure in 125 (27%), confirming these as the leading conditions associated with DBS system change or removal. Postoperative wound infection was present in 7.8% of explant admissions, while systemic complications such as pneumonia, deep vein thrombosis, pulmonary embolism, and acute renal failure were uncommon (each < 3%). Overall complication patterns were similar across PD, ET, and dystonia; although some comparisons (e.g., deep vein thrombosis and pulmonary embolism) reached statistical significance, the absolute number of events was very small, and no consistent diagnosis-specific gradient was observed.
4. Discussion
In this nationwide, population-based study using the Spanish RAE-CMBD, we describe temporal trends, clinical characteristics, and in-hospital outcomes of hospital admissions undergoing DBS for movement disorders in Spain from 2002 to 2019. We observed a steady increase in DBS implantations and explantations over time, with Parkinson’s disease as the predominant indication, followed by essential tremor and dystonia. Overall comorbidity and age increased modestly across the study period, whereas LOHS shortened and IHM decreased and remained very low. Hardware-related complications and infections were the main causes of explantation. Additionally, we found consistent sex differences, with men being more frequently hospitalized for DBS and women with PD undergoing surgery approximately two years later in life than men, despite similar comorbidity profiles and in-hospital outcomes.
These results are primarily representative of DBS-related hospital admissions within Spain and the Spanish healthcare system; extrapolation to other countries or healthcare contexts should be made with caution due to differences in referral pathways, reimbursement structures, surgical organization, and coding practices. However, our findings are consistent with the international literature reporting a sustained increase in DBS utilization for movement disorders over the last two decades. Large administrative database analyses from the United States, using the Nationwide Inpatient Sample and other national datasets, have shown a marked rise in the number of DBS procedures since the mid-1990s, accompanied by an expansion of indications and a gradual shift towards older and more comorbid patients. In these studies, PD was also the leading indication for DBS, followed by ET and dystonia, with PD typically representing 60–80% of procedures [30,31]. Data from Europe and Asia similarly report that PD is the most frequent indication, with ET and dystonia accounting for smaller but clinically relevant subsets [16,32,33,34,35]. Notably, studies from Latin America show that dystonia is the second most common indication after Parkinson’s disease, ahead of essential tremor [36]. Taken together, the diagnostic distribution and broad temporal trends we describe in Spain mirror those observed in other high-income countries.
Within this overall pattern, we observed a modest change in the relative contribution of diagnoses across periods. Interestingly, the relative share of PD among DBS implantations decreased modestly in the last study period, from 86.9% in 2002–2007 to 81.5% in 2014–2019, despite a continued increase in the absolute number of PD procedures. In parallel, the proportions of ET and dystonia rose slightly. A plausible interpretation is that, over the same period, access to other device-aided second-line therapies for advanced PD, such as continuous levodopa–carbidopa intestinal gel or subcutaneous apomorphine infusion, has progressively expanded in Spain [37]. These infusion therapies are often considered in older or more comorbid patients who might previously have been referred for DBS, and their wider availability could have shifted part of this population away from surgery, thereby reducing the proportion of PD DBS in the oldest and most comorbid groups. In the future, it will be important to examine how DBS utilization patterns evolve in the post-COVID era and in the context of the growing use of magnetic resonance-guided focused ultrasound (MRgFUS) for tremor and, more recently, for selected Parkinsonian symptoms, as these developments may further reshape the balance between DBS and other advanced therapies.
The clinical profile of hospital admissions undergoing DBS also resembles that reported elsewhere. The mean age at implantation in our cohort falls within the sixth to seventh decade of life, consistent with previous studies [16,30,38]. Over time, we observed a progressive increase in the CCI, indicating that a growing proportion of hospitalizations had at least one relevant comorbidity. The absolute number of hospitalizations of patients older than 70 years also increased, although the overall proportion lowered due to a greater rise in younger patients. Importantly, despite this higher comorbidity burden, we found that LOHS decreased over time and IHM remained very low for both implantation and explantation/revision procedures. This pattern is consistent with international data showing that, as surgical and perioperative techniques have evolved, DBS is increasingly being offered to older and more comorbid patients, with low perioperative mortality and acceptable morbidity even in carefully selected older individuals [38,39,40]. In Spain, previous nationwide analyses of overall PD hospitalizations have shown a parallel trend of increasing comorbidity, with stable or only slightly increased adjusted in-hospital mortality and a progressive reduction in LOHS [26]. Taken together, these data support patient decision-making, as current mortality related to DBS in Spain remains below 0.1%.
The sex differences observed in our cohort deserve special consideration. Men accounted for most DBS procedures and hospitalizations across all diagnostic groups, and this “gender gap” widened steadily over the study period. Women with PD underwent surgery two years later in life than men but did not show worse in-hospital outcomes or longer stays, suggesting that this delay is not explained by a higher perioperative risk as captured in our data. This pattern replicates the “gender gap” described in other countries. Jost et al. described sex differences in PD surgery, showing that women are less likely to receive DBS and often present with more advanced disability at the time of implantation, despite similar postoperative benefits [20]. The recent literature on disparities in DBS and other advanced therapies for PD has also highlighted intersectional barriers related to sex, socioeconomic status, and race, which may influence referral patterns, patient preferences, and decision-making [21]. Other factors may include gender differences in health-seeking behaviour, caregiver roles, risk perception, and potential bias in referral and selection processes [41,42]. Moreover, women with PD may experience a greater burden of non-motor symptoms and quality-of-life impairment, which can further modulate expectations and priorities regarding surgery [43,44,45].
Our findings may suggest disparities in access; however, several alternative explanations should be considered. First, male predominance in DBS may partly reflect the higher prevalence of PD in men (roughly two-fold in many epidemiological studies) and a less marked, but still present, male predominance in ET [2,3]. Second, differences in referral patterns and care pathways may play a role: for example, neurologists might be more likely to refer younger, working-age men when motor disability interferes with employment, while women might be referred later or less often [21,41,42]. Finally, unmeasured comorbidities not captured by the CCI—such as cognitive impairment, psychiatric symptoms, frailty, or limited social support—might differentially affect eligibility or timing of DBS in women and men. Future studies should integrate clinical, psychosocial, and qualitative data to better understand sex- and gender-related determinants of DBS access and timing in Spain, and to design interventions that promote equitable care.
Complications, particularly those related to hardware, are a critical dimension when evaluating DBS programs. In our study, around 14% of implantation admissions were complicated by at least one coded adverse event, and approximately 8% of surgeries were associated with device-related mechanical problems or infections. These proportions are broadly in line with large single-centre series and systematic reviews, which have reported overall complication rates ranging from roughly 5% to 30% over variable follow-up periods, depending on how adverse events are defined and ascertained [14,15,46,47,48,49]. Large US database analyses have shown that between 15% and 34% of DBS procedures in routine practice are revisions or removals, with infection and hardware malfunction among the main drivers [50].
Electrode-related complications are consistent with other international studies that report rates of 5–10% [15,16,48]. In our series, hardware malposition or malfunction accounted for 5–6% of procedures and infections for 1–2%. We observed a transient increase in ‘electrode malposition/mechanical failure’ during 2008–2013, followed by a decline in 2014–2019. This pattern may reflect the rapid expansion of DBS activity during the mid-period, with greater heterogeneity in case mix and a potential learning-curve/centre-volume effect. In addition, because our dataset is episode-based, early lead revisions or staged procedures may be captured as separate admissions, inflating per-admission frequencies. Finally, temporal changes in postoperative imaging practices or coding sensitivity could have increased the detection and documentation of hardware-related events. Notably, this peak was not accompanied by increases in severe systemic complications or in-hospital mortality, suggesting a technical/reporting phenomenon rather than a generalized worsening of perioperative safety.
The infection proportion observed appears to lie at the lower end of the published range, although underestimation is likely, as some infections are probably managed in outpatient settings or during readmissions not coded with DBS procedure codes [17,49,51,52,53,54,55]. Device infections in our cohort accounted for only a minority of index implantations but were disproportionately represented among explantations and surgical revisions, suggesting that many infections are delayed rather than acute and ultimately culminate in hardware removal. Consistent with this, hardware-related complications and infections were frequently associated with explantation/revision in our cohort.
From a health-system perspective, the prominence of hardware-related complications and infections has important implications. Observational studies and expert-based recommendations have emphasized that DBS infections, although relatively infrequent, are associated with substantial morbidity, prolonged courses of intravenous and oral antibiotics, longer hospital stays, repeated procedures, and high costs, particularly when complete system explantation is required [17,49,51,52,53,54,55]. Our findings, showing that infections and mechanical complications are associated with explantation, support the prioritization of infection-prevention protocols, concentration of DBS surgery in experienced centres, and structured follow-up pathways as key quality and safety indicators for DBS programs in Spain.
Our study has several strengths. First, it is based on a nationwide administrative database that captures more than 95% of public hospital discharges in Spain, providing a comprehensive, real-world overview of DBS practice over nearly two decades. Second, the RAE-CMBD enables the analysis of a large sample of cases that would be impossible to obtain in other study settings. Third, we distinguished between DBS implantations and explantations/revisions, and stratified analyses by primary diagnosis and sex, allowing a nuanced characterization of trends and outcomes in PD, ET, and dystonia. Fourth, our long observation period spans major changes in DBS technology and perioperative care, enabling the description of temporal improvements in LOHS and stability of IHM despite increasing age and comorbidity.
Nevertheless, several limitations must be acknowledged. As with all studies based on administrative data, the RAE-CMBD lacks detailed clinical information such as disease duration, motor subtype, levodopa responsiveness, DBS target and programming parameters, cognitive status, or specific surgical techniques (awake vs. asleep, frame-based vs. frameless). In addition, the RAE-CMBD does not record ethnicity/race, country of birth, or other migration-background variables; therefore, we could not assess potential disparities in DBS access or outcomes across ethnic minority or migrant populations. The database also lacks information on referral pathways and waiting-list times (e.g., time from clinical indication to surgery), precluding analyses of waiting time trends by disorder. All these factors can influence both the indication for DBS and the risk of complications but could not be evaluated. Misclassification and under-coding are possible, particularly for specific complications and for secondary diagnoses that may not be systematically recorded [56]. The database is episode-based, so we could not track individual patients over time or capture long-term outcomes beyond index admission, including delayed complications (such as later infections), stimulation efficacy, or quality-of-life changes, which may underestimate the overall complication burden. Moreover, in-hospital mortality reflects deaths occurring during the index admission only and therefore underestimates post-discharge mortality. However, perioperative estimates from published DBS cohorts suggest that subsequent mortality is very low (approximately 0–0.3% at 30 days and ~0.2% at 90 days) [57,58]. For the same reason, we were unable to determine how many unique individuals underwent DBS during the study period or to calculate true complication, reintervention, or explantation rates at the patient level. Additionally, private hospitals and outpatient procedures are incompletely represented, which might lead to an underestimation of the true burden of complications and revisions. Finally, changes in coding systems (transition from ICD-9-CM to ICD-10-ES) over the study period might have introduced artefacts in temporal trends, although we applied consistent coding algorithms to identify diagnoses and procedures [26].
Finally, changes in coding systems (transition from ICD-9-CM to ICD-10-ES) over the study period might have introduced artefacts in temporal trends, even though we applied consistent coding algorithms to identify diagnoses and procedures [26]. Importantly, the coding era is almost completely aligned with calendar time; therefore, modelling the coding era as a covariate would be highly collinear with period effects and may yield unstable or difficult-to-interpret estimates. In addition, for some administrative endpoints (particularly complications and explantation/revision causes), the ICD-9 to ICD-10 transition does not always allow a straightforward one-to-one mapping, which may lead to differential misclassification across eras. For these reasons, we did not apply model-based “corrections” for the coding era, and temporal trends across the transition should be interpreted with caution. Similarly, because the dataset lacks key clinical variables required for meaningful perioperative risk adjustment and does not allow patient-level linkage across admissions, we did not perform risk-adjusted analyses, and our findings should be considered hypothesis-generating.
5. Conclusions
In conclusion, this nationwide study shows that DBS for movement disorders in Spain has expanded over the last two decades, with increasing age and comorbidity of treated patients, stable very low in-hospital mortality, and shorter hospital stays. Hardware complications and infections remain the most frequent diagnoses associated with explantation, and women with PD tend to undergo DBS less frequently and at an older age than men, despite similar in-hospital outcomes. These findings underscore the importance of optimizing patient selection, perioperative care, and infection-prevention strategies, while addressing potential sex- and gender-related inequities in access to DBS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD 2016 Neurology Collaborators Global, regional, and national burden of neurological disorders, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016 Lancet Neurol.20191845948010.1016/S 1474-4422(18)30499-X 30879893 PMC 6459001 · doi ↗ · pubmed ↗
- 2Ben-Shlomo Y. Darweesh S. Llibre-Guerra J. Marras C. San Luciano M. Tanner C. The epidemiology of Parkinson’s disease Lancet 202440328329210.1016/S 0140-6736(23)01419-838245248 PMC 11123577 · doi ↗ · pubmed ↗
- 3Louis E.D. Ferreira J.J. How common is the most common adult movement disorder? Update on the worldwide prevalence of essential tremor Mov. Disord.20102553454110.1002/mds.2283820175185 · doi ↗ · pubmed ↗
- 4Albanese A. Bhatia K. Bressman S.B. Delong M.R. Fahn S. Fung V.S. Hallett M. Jankovic J. Jinnah H.A. Klein C. Phenomenology and classification of dystonia: A consensus update Mov. Disord.20132886387310.1002/mds.2547523649720 PMC 3729880 · doi ↗ · pubmed ↗
- 5Yang W. Hamilton J.L. Kopil C. Beck J.C. Tanner C.M. Albin R.L. Ray Dorsey E. Dahodwala N. Cintina I. Hogan P. Current and projected future economic burden of Parkinson’s disease in the U.Snpj Park. Dis.202061510.1038/s 41531-020-0117-1PMC 734758232665974 · doi ↗ · pubmed ↗
- 6Deuschl G. Schade-Brittinger C. Krack P. Volkmann J. Schäfer H. Bötzel K. Daniels C. Deutschländer A. Dillmann U. Eisner W. A randomized trial of deep-brain stimulation for Parkinson’s disease N. Engl. J. Med.200635589690810.1056/NEJ Moa 06028116943402 · doi ↗ · pubmed ↗
- 7Follett K.A. Weaver F.M. Stern M. Hur K. Harris C.L. Luo P. Marks W.J.Jr. Rothlind J. Sagher O. Moy C. Pallidal versus subthalamic deep-brain stimulation for Parkinson’s disease N. Engl. J. Med.20103622077209110.1056/NEJ Moa 090708320519680 · doi ↗ · pubmed ↗
- 8Kumar R. Lozano A.M. Sime E. Lang A.E. Long-term follow-up of thalamic deep brain stimulation for essential and parkinsonian tremor Neurology 2003611601160410.1212/01.WNL.0000096012.07360.1C 14663050 · doi ↗ · pubmed ↗