Assessment of Fractional Flow Reserve from Coronary CT Angiography Using a Deep Learning-Based Algorithm: A Multicenter Retrospective Study
Ludovica R. M. Lanzafame, Claudia Gulli, Maria Teresa Cannizzaro, Bruno Francaviglia, Laura M. Chisari, Leon D. Grünewald, Vitali Koch, Christian Booz, Thomas J. Vogl, Luca Saba, Silvio Mazziotti, Tommaso D’Angelo

TL;DR
A deep learning model accurately computes fractional flow reserve from coronary CT scans, offering a non-invasive way to assess heart disease.
Contribution
A deep learning algorithm is introduced for non-invasive FFR computation from CCTA with high diagnostic accuracy.
Findings
FFR-CT achieved an AUC of 0.935 and high sensitivity and specificity for detecting significant coronary stenoses.
Automated CAD-RADS classifications showed good agreement with expert radiologist assessments (k = 0.765).
Per-vessel diagnostic performance was high, with the LAD showing the highest accuracy (AUC = 0.932).
Abstract
Objectives: To assess the diagnostic accuracy of a deep learning (DL)-based algorithm for non-invasive computation of fractional flow reserve (FFR-CT) from coronary computed tomography angiography (CCTA) and to evaluate the model’s ability to automatically assign cardiovascular risk categories according to the Coronary Artery Disease–Reporting and Data System (CAD-RADS). Materials and Methods: Sixty patients with suspected coronary artery disease who underwent both CCTA and invasive coronary angiography (ICA) were retrospectively included in this multicenter study. Curved multiplanar reconstructions derived from CCTA were analyzed by the deep learning-based model to estimate FFR-CT values and to automatically assign CAD-RADS risk categories. The diagnostic performance of the software for the identification of hemodynamically significant coronary stenoses was evaluated using ICA as the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
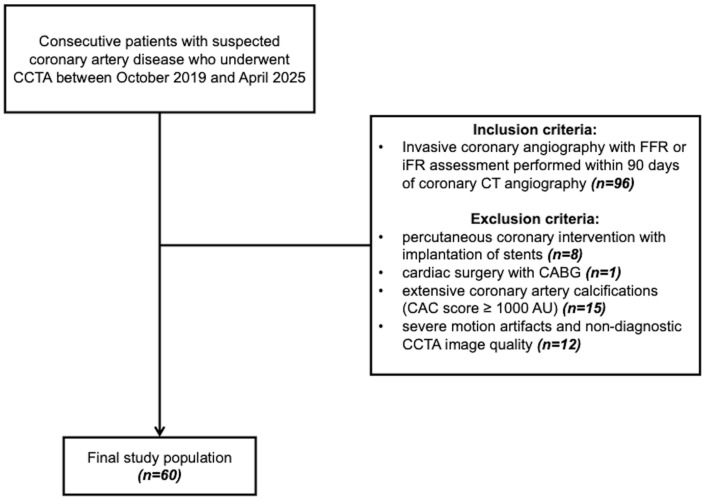 Figure 1
Figure 1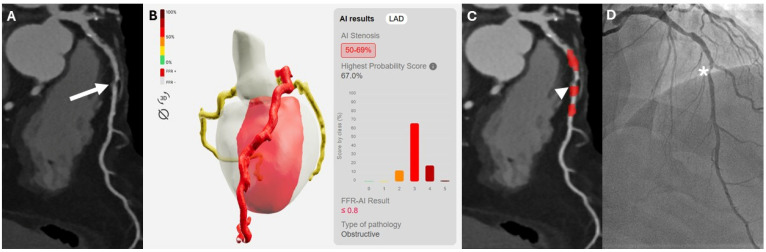 Figure 2
Figure 2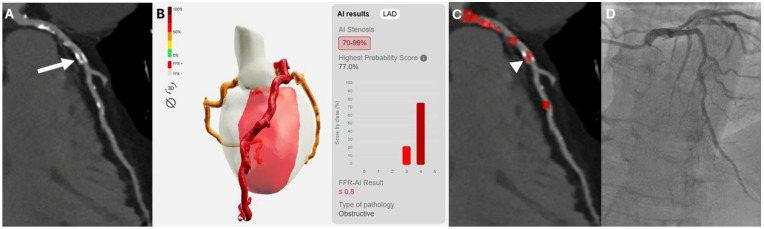 Figure 3
Figure 3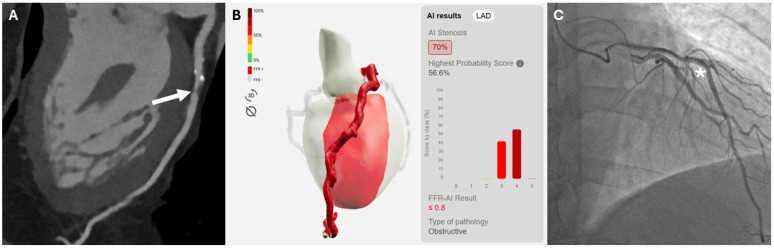 Figure 4
Figure 4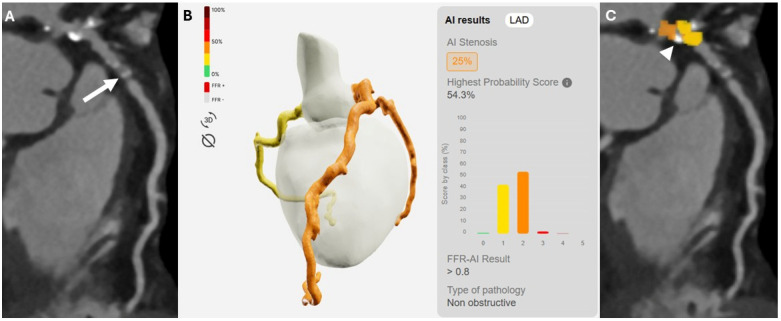 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Imaging and Diagnostics · Coronary Interventions and Diagnostics · Cerebrovascular and Carotid Artery Diseases
1. Introduction
Coronary computed tomography angiography (CCTA) has emerged as a cornerstone in the non-invasive evaluation of patients with moderate clinical pre-test likelihood of coronary artery disease (CAD), due to its high sensitivity and strong negative predictive value in identifying coronary stenoses [1]. However, its ability to predict lesion-specific ischemia remains limited, especially in patients with moderate stenoses (typically defined as 50–69% luminal narrowing) [2]. This often leads to referral for invasive coronary angiography (ICA) and pressure-wire assessments, such as fractional flow reserve (FFR) or instantaneous wave-free ratio (iFR), to further clarify the presence of hemodynamically significant disease [3,4]. Artificial intelligence (AI) has been increasingly applied to automated image analysis tasks, with the potential to streamline image interpretation workflows and facilitate timely and efficient reporting in clinical practice [5,6]. AI-based tools are reshaping radiology by enhancing image analysis, automating detection and segmentation tasks, and improving diagnostic accuracy and workflow efficiency. It enables the extraction of quantitative imaging features and supports more consistent and reproducible interpretations [5]. Importantly, AI-driven reconstruction and optimization techniques also allow reduction in radiation dose while preserving diagnostic image quality [7,8]. Recently, deep learning (DL)-based models have been developed to rapidly predict lesion-specific ischemia directly computing fractional flow reserve from CCTA datasets (FFR-CT) [9,10]. At present, the dissemination of AI-based tools remains largely confined to large, often university-affiliated centers, primarily due to their high costs and infrastructural requirements. However, emerging collaborative and system-level approaches suggest that wider implementation may become increasingly feasible over time, potentially enabling broader access beyond high-resource institutions [11].
The aim of the study was to assess the diagnostic performance of a commercially available DL-based FFR-CT algorithm for the detection of hemodynamically significant coronary stenoses, using ICA as reference standard, and to evaluate the software’s capability to automatically assign Coronary Artery Disease–Reporting and Data System (CAD-RADS) categories.
2. Materials and Methods
Institutional Review Board approval was obtained, with a waiver of informed consent due to the retrospective, observational design.
2.1. Patient Population
This multicenter retrospective study was conducted at two different university hospitals and included consecutive patients with suspected CAD who underwent both CCTA and ICA within a 90-day interval between October 2019 and April 2025. Exclusion criteria included: (i) history of percutaneous coronary intervention with implantation of stents; (ii) history of cardiac surgery with coronary artery bypass grafting (CABG); (iii) extensive coronary artery calcifications (CAC score ≥ 1000 AU); (iv) severe motion artifacts and non-diagnostic CCTA image quality. The flowchart illustrating the patient selection process is shown in Figure 1.
2.2. Acquisition Protocol and Image Reconstruction
CCTA examinations were performed using a 64-row dual-layer CT scanner (IQon CT, Philips Healthcare, Best, The Netherlands) at Center 1 (“G. Martino”, Messina University Hospital) and a 320-row Toshiba Aquilion ONE (Toshiba Medical Systems Corporation, Otawara, Japan) at Center 2 (“G.Rodolico-San Marco”, Catania University Hospital). All examinations were performed with the patient in the supine position, and imaging was obtained in the cranio-caudal direction. Firstly, a prospective ECG-gated non-contrast scan (120 kVp tube voltage, 40 mAs tube current) was acquired for the assessment of coronary artery calcium (CAC) score. Subsequently, a contrast-enhanced scan was performed using a retrospective ECG-gated protocol. Intravenous contrast (Iomeprol 400, Iomeron, Bracco, Milan, Italy) was administered at 0.85 mL/kg injected at 5 mL/s, followed by a 50 mL saline flush. Automated bolus tracking was used, with a region of interest placed in the descending aorta to trigger image acquisition. The tube voltage was set at 120 kVp, with tube current modulation based on patient body weight. Common acquisition parameters included a matrix size of 512 × 512 and a field of view of 220–250 mm. Gantry rotation time and detector configuration varied between the two institutions, being 0.27 s and 64 × 0.625 mm at Center 1 and 0.35 s and 320 × 0.5 mm at Center 2, respectively. Before acquisition, all patients received premedication with sublingual vasodilator (isosorbide dinitrate), when not contraindicated; intravenous β-blocker was administered to patients with a heart rate ≥ 70 bpm (esmolol hydrochloride). CCTA images were reconstructed along the R–R interval, during end-diastolic phases or those providing the best image quality. Image reconstruction was performed using a slice thickness of 0.67 mm with a reconstruction increment of 0.34 mm on the IQon CT system, and a slice thickness of 0.5 mm with a reconstruction increment of 0.25 mm on the Aquilion ONE system. The acquisition parameters at both centers are summarized in Table 1.
2.3. Deep Learning Based Analysis
CorEx version 2.4.1 (Spimed-AI, Paris, France) was used for both FFR-CT computation and CAD-RADS classification. The software is a semi-automated DL-based model, trained on the Inception-v3 convolutional neural network architecture and developed for the automated interpretation of CCTA images [12,13,14,15].
Curved multiplanar reconstructions (cMPRs) from CCTA datasets acquired at both centers were generated at Center 1 by a radiologist with 4-years of expertise (C.G.) in cardiovascular imaging, during this phase, the same reader was responsible for excluding datasets deemed to have insufficient image quality. Reconstructions were performed on a workstation using dedicated software (IntelliSpace Portal, version 8.0, Philips Healthcare, Best, The Netherlands). cMPRs were reconstructed at 40° angular intervals to cover the full circumference of each major coronary artery. For each patient, a total of 27 curved MPR images were generated, including nine for the left anterior descending (LAD), nine for the right coronary artery (RCA), and nine for the circumflex artery (LCx). The left main coronary artery was included in the reformatted images of both LAD and LCx. Coronary artery centerlines were manually reviewed and corrected, when necessary, by the same radiologist. The resulting cMPR datasets were subsequently uploaded to the CorEx platform and automatically processed by the DL-based algorithm to generate binary FFR-CT predictions (≤0.80 vs. >0.80) and automated CAD-RADS classifications.
2.4. Reference Standard
ICA data, including FFR and iFR measurements, were collected from the patients’ clinical records at each participating institution and recorded for analysis. CCTA datasets were independently reviewed by two board-certified radiologists with expertise in cardiovascular imaging (T.D. and M.T.C.), who were blinded to ICA results, using axial images and cMPRs on locally available dedicated workstations with vendor-specific software at each institution. For each patient, CAD severity was categorized according to the Coronary Artery Disease–Reporting and Data System 2.0 as follows: CAD-RADS 0, no plaque or stenosis; CAD-RADS 1, minimal stenosis (1–24%); CAD-RADS 2, mild stenosis (25–49%); CAD-RADS 3, moderate stenosis (50–69%); CAD-RADS 4, including both CAD-RADS 4A, severe stenosis (70–99%) and CAD-RADS 4B, left main stenosis ≥50% or three-vessel disease with ≥70% stenosis; and CAD-RADS 5, a total occlusion (100%) [16].
2.5. Statistical Analysis
Statistical analysis was performed using a commercially available software (MedCalc Software, version 20.1, Ostend, Belgium). Data distribution was assessed with the Shapiro–Wilk test. Categorical variables were indicated as numbers and percentages. Normally distributed data are expressed as mean ± standard deviation (SD), whereas non-normally distributed data are reported as median and interquartile range [IQR]. Comparisons between groups were performed using a two-tailed t-test for normally distributed data, and the Wilcoxon test for non-normally distributed data.
The diagnostic accuracy of the DL-based FFR-CT software was assessed on both a per-patient and per-vessel basis, using invasive FFR and iFR as reference standards, with vessel-specific ischemia defined by thresholds of FFR ≤ 0.80 and iFR ≤ 0.89 [3,17,18,19]. To this end, receiver operating characteristic (ROC) curves were constructed with assessment of the area under the curve (AUC). Accuracy, sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were also assessed. Agreement between FFR-CT and invasive measurement was further evaluated using Cohen’s kappa coefficient (k).
Finally, weighted Cohen’s kappa was calculated to assess the level of agreement between CAD-RADS scores assigned by expert readers at each institution and those automatically generated by the AI-based software.
Results were interpreted as follows: slight or poor agreement (k < 0.20), fair agreement (k = 0.20–0.40), moderate agreement (k = 0.40–0.60), good agreement (k = 0.60–0.80), and excellent agreement (k > 0.80).
3. Results
3.1. Patient Population
From an initial cohort of 96 patients, 36 were excluded according to the following criteria: (i) history of percutaneous coronary intervention with implantation of stents (n = 8); (ii) history of cardiac surgery with CABG (n = 1); (iii) extensive coronary artery calcifications (CAC score ≥ 1000 Agatston units) (n = 15); (iv) severe motion artifacts and non-diagnostic CCTA image quality (n = 12).
The final patient population included 60 patients (45 males and 15 females; mean age 69.5 ± 9.6), 34 from Center 1 and 26 from Center 2. The median interval days between CCTA and ICA was 33.0 [10.0–73.5].
FFR measurements were available in 37 of 60 patients (61.7%), with 54 out of 180 vessels (30%) classified as positive; iFR measurements were available in 23 out of 60 patients (38%), with 14 of 180 vessels (8%) classified as positive. No patient underwent both FFR and iFR assessment. Patient demographic characteristics are reported in Table 2.
3.2. Diagnostic Performance of FFR-CT
On a per-patient basis, the DL-based software demonstrated high diagnostic performance, showing an AUC of 0.935 (95% CI: 0.840–0.982). Sensitivity, specificity PPV, NPV and accuracy were 93.2% (95% CI: 81.3–98.6%), 93.7% (95% CI: 69.8–99.8%), 97.6% (95% CI: 85.9–99.6%), 83.3% (95% CI: 62.5–93.7%) and 93.3% (95% CI: 83.8–98.1%), respectively. Excellent agreement was observed between FFR-CT and the invasive reference standard (k = 0.836).
A total of 180 vessels were analyzed, with 60 vessels for each of the three main coronary arteries. The AUC was 0.902 (95% CI: 0.849–0.941). Sensitivity and specificity were 84.5% (95% CI: 72.6–92.6%) and 95.9% (95% CI: 90.7–98.7%), respectively. PPV, NPV and accuracy were as follows: 90.7% (95% CI: 80.5–95.8%), 92.8% (95% CI: 87.7–95.9%) and 92.2% (95% CI: 87.3–95.7%).
Excellent agreement was also observed on a vessel-based analysis (k = 0.819). In the exploratory subgroup analysis of vessels with moderate stenoses (24/180; 13.3%), invasive coronary angiography demonstrated significant coronary stenoses in 11/24 cases, among these the algorithm correctly detected ischemic lesions in 72.7% of cases (8/11). The remaining moderate stenoses that were not associated with hemodynamically significant disease were correctly classified as such in 12 out of 13 cases (92.3%). The diagnostic accuracy in this subgroup of patients showed an AUC was 0.825 (95% CI: 0.617–0.948), whereas sensitivity, specificity, PPV, NPV and accuracy were as follows: 72.7% (95% CI: 39.1–93.9%), 92.3% (95% CI: 63.9–99.8%), 88.9% (95% CI: 54.0–98.1%), 80.0% (95% CI: 62.6–95.3%), and 83.3% (95% CI: 62.6–95.3%). Two cases of moderate coronary stenosis are illustrated in Figure 2 and Figure 3, representing a true-positive and a false-positive classification, respectively.
A vessel-specific sub-analysis, performed to evaluate the diagnostic performance of the software for each major coronary artery, showed consistently strong diagnostic performance across all major coronary arteries, with LAD exhibiting the highest accuracy. The algorithm achieved an AUC of 0.932 (95% CI: 0.836–0.981%), sensitivity of 94.1% (95% CI: 80.3–99.3%), specificity of 92.3% (95% CI: 74.9–99.0%), and an accuracy of 93.3% (95% CI: 83.8–98.1%). The PPV and NPV were 94.1% (95% CI: 80.8–98.4%) and 92.3% (95% CI: 75.7–97.9%), respectively. Comparable diagnostic performance was also observed across the remaining epicardial coronary vessels, with detailed results summarized in Table 3.
Figure 4 and Figure 5 illustrate a true-positive and a false-negative case of left anterior descending artery (LAD) stenosis, respectively.
3.3. CAD-RADS Agreement
Automated cardiovascular risk stratification yielded the following CAD-RADS distribution: CAD-RADS 0 in 0/60 patients (0%); CAD-RADS 1 in 3/60 patients (5%), CAD-RADS 2 in 11/60 (18.3%), CAD-RADS 3 in 7/60 (11.7%), CAD-RADS 4 in 28/60 (46.7%), and CAD-RADS 5 in 11/60 patients (18.3%).
No statistically significant differences were observed between CAD-RADS scores assigned by expert readers and those automatically generated by the DL-based software (p = 0.567), with good agreement between the two methods (k = 0.765).
4. Discussion
The purpose of this study was to demonstrate the diagnostic performance of a DL-based FFR-CT algorithm in identifying vessel-specific ischemia using FFR and iFR as reference standard, and to evaluate the automated model’s CAD-RADS prediction. Both per-patient and per-vessel analyses showed high sensitivity, specificity, and AUC values for the identification of hemodynamically significant coronary stenoses based on FFR-CT.
The observed results are consistent with prior DL-based FFR-CT studies which have demonstrated per-patient AUCs in the range of 0.86–0.92 [9,20,21]. These findings demonstrated the model’s reliability in both global patient evaluation and vessel-specific ischemia assessment.
Exploratory subgroup analysis by coronary territory consistently revealed consistent performance across LAD, LCx, and RCA vessels. The LAD territory had the highest diagnostic metrics, with an AUC of 0.932 and sensitivity and specificity both exceeding 90%. In contrast, the LCx territory showed lower sensitivity (70%) and agreement (k = 0.687). The LCx typically presents with a smaller vessel caliber and increased tortuosity compared with the LAD, which may complicate accurate image reconstruction and lumen assessment on CCTA [9,22]. The RCA assessment also demonstrated solid performance (AUC = 0.846), despite slight reductions in sensitivity compared to LAD, as reported in similar FFR-CT studies [20,23]. Specifically, the RCA is typically surrounded by a greater amount of pericoronary adipose tissue compared with the LAD, exhibits higher mobility, and is particularly susceptible to motion artifacts due to its more perpendicular movement relative to the CT acquisition plane. This combination of anatomical and technical factors may hinder optimal cMPR quality [24,25]. Collectively, these findings suggest that vessel-specific anatomical characteristics may contribute to the variable accuracy observed in DL-based functional assessment.
A particularly noteworthy result was the model’s diagnostic accuracy in borderline stenoses (50–69%), where conventional CCTA alone often lacks specificity. The relatively small sample size in this category likely contributed to lower sensitivity estimates and wider confidence intervals, thereby limiting the precision of these findings; nevertheless, the algorithm correctly identified ischemic and non-ischemic lesions in a substantial proportion of cases, holding good promise in ambiguous clinical scenarios. This aligns with emerging data highlighting the utility of DL-based FFR-CT tools in refining decision-making for intermediate lesions, where further invasive investigations are frequently required for clarification [20,26]. The analysis of discordant cases also provided additional insight into the model’s limitations. Among the false negatives (9/180 vessels), most were associated with low image quality and suboptimal vessel opacification, reflecting the potential impact of technical factors such as signal-to-noise/contrast-to-noise ratio and motion artifacts on AI-based models, while nonetheless preserving superior diagnostic performance compared with the assessment of coronary stenosis by CT alone [9,27]. Additionally, models based on uploaded cMPRs may not detect ischemia caused by microvascular dysfunction, as downstream resistance cannot be quantified by CCTA-derived algorithms [10]. On the other hand, despite the exclusion of patients with a very high coronary calcium burden (CAC > 1000), false positives (5/180 vessels) were frequently linked to heavy calcifications. In these cases, blooming artifacts likely led to overestimation of stenosis severity and consequent misclassification of functional significance [20,23,28,29]. Other technical factors, such as motion artifacts may also negatively influence diagnostic performance. However, in the present study, datasets with inadequate image quality were excluded a priori to ensure reliable analysis. Future investigations specifically addressing more challenging imaging conditions will be important to further validate the robustness of the software in real-world, heterogeneous scenarios.
Finally, the DL-based FFR-CT model showed good concordance with human-assigned CAD-RADS scores (k = 0.765), reinforcing its utility not only in ischemia detection but also in structured risk stratification, consistent with previous studies on the use of AI in CCTA. However, despite the overall good agreement, a non-negligible rate of misclassification was observed. This aspect should not be underestimated, particularly in cases of risk-class downstaging, which may have significant implications for subsequent patient management. Therefore, at present, human oversight remains essential to ensure appropriate clinical interpretation and decision-making. Furthermore, in our dataset, no patients were classified as CAD-RADS 0, reflecting a cohort characterized by a relatively high cardiovascular risk profile, with the majority of patients falling into category 4. This distribution is consistent with the higher likelihood of referral to invasive procedures in patients belonging to these higher-risk categories.
Medical AI-based approaches are transitioning from the research setting to routine clinical practice and, with the growing number of CCTA examinations, automated CAD-RADS assignment could further streamline reporting, especially in high-volume centers [10,12,30,31,32]. In this setting, a tool capable of delivering automated CAD-RADS classification within a few minutes, while simultaneously providing information on the hemodynamic significance of stenoses, may contribute to a more efficient and integrated clinical workflow.
This study has several limitations. Firstly, its retrospective design and the modest sample size, along with the incomplete availability of detailed baseline comorbidity data, may limit the generalizability of the findings and may have had a more pronounced impact on statistical power in subgroup analyses, particularly those focusing on moderate-grade stenoses and vessel-specific assessments of individual coronary arteries. Larger, prospective, multicenter studies and different healthcare settings are needed to further validate the performance of the DL-based model. Moreover, the relatively long interval between CCTA and ICA may introduce temporal bias related to possible changes in coronary disease status over time, potentially resulting in discrepancies in the assessment of disease severity. However, in routine clinical practice, the timing of invasive angiography often varies due to logistical factors, including specialist availability and patient-related considerations. Although longitudinal studies have shown that FFR may gradually decrease over long-term follow-up in patients with stable coronary artery disease, short-term variations over a period of weeks are generally minimal in the absence of acute events. Therefore, the interval between CCTA and ICA in our cohort is unlikely to have significantly influenced the observed FFR correlation [33]. Secondly, the radiologist’s manual correction of vessel centerlines significantly influenced results thus introducing operator dependency. In the present study, semi-automated centerline correction was performed by a single operator; consequently, operator dependency could not be formally assessed. In addition, CAD-RADS categorization was assigned by a single reader at each center, precluding a formal evaluation of inter-reader agreement and potentially introducing variability in category assignment. Further studies involving multiple readers, ideally with different levels of experience, are warranted to better evaluate inter-operator variability and reproducibility. A third limitation is the use of two different CT scanner models with slight variations in acquisition protocols; however, previous studies have demonstrated stable diagnostic performance of the algorithm across different scanner types and acquisition settings [30]. Finally, the use of two different indices (FFR and iFR) as reference standards may have introduced a degree of heterogeneity in the results, although the literature has consistently demonstrated a strong correlation and high diagnostic agreement between FFR and iFR in the assessment of functionally significant coronary stenoses [17,34].
5. Conclusions
In conclusion, the DL-based FFR-CT algorithm demonstrated promising diagnostic accuracy in identifying hemodynamically significant coronary stenoses, consistently maintaining good diagnostic performance across all major coronary arteries and showing substantial concordance with invasive measurements. The findings of this exploratory study further validate the clinical value of FFR-CT as a reliable noninvasive tool for the assessment of both anatomical and hemodynamic characteristics of coronary lesions. The integration of DL-based FFR-CT into routine clinical practice may allow functional assessment of coronary stenoses directly from CCTA images, potentially reducing the need for invasive procedures, shortening diagnostic timelines, lowering healthcare costs, and benefiting patients by avoiding additional exposure to ionizing radiation associated with ICA. Furthermore, automated CAD-RADS categorization may substantially streamline the reporting process while promoting greater standardization of structured reports, including systematic incorporation of risk categories that are not consistently reported in routine clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Knuuti J. Wijns W. Saraste A. Capodanno D. Barbato E. Funck-Brentano C. Prescott E. Storey R.F. Deaton C. Cuisset T. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes Eur. Heart J.20204140747710.1093/eurheartj/ehz 42531504439 · doi ↗ · pubmed ↗
- 2Meijboom W.B. Meijs M.F. Schuijf J.D. Cramer M.J. Mollet N.R. van Mieghem C.A. Nieman K. van Werkhoven J.M. Pundziute G. Weustink A.C. Diagnostic accuracy of 64-slice computed tomography coronary angiography: A prospective, multicenter, multivendor study J. Am. Coll. Cardiol.2008522135214410.1016/j.jacc.2008.08.05819095130 · doi ↗ · pubmed ↗
- 3Tonino P.A.L. De Bruyne B. Pijls N.H.J. Siebert U. Ikeno F. van’t Veer M. Klauss V. Manoharan G. Engstrøm T. Oldroyd K.G. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention N. Engl. J. Med.200936021322410.1056/NEJ Moa 080761119144937 · doi ↗ · pubmed ↗
- 4Davies J.E. Sen S. Dehbi H.-M. Al-Lamee R. Petraco R. Nijjer S.S. Bhindi R. Lehman S.J. Walters D. Sapontis J. Use of the Instantaneous Wave-free Ratio or Fractional Flow Reserve in PCIN. Engl. J. Med.2017376182418342831745810.1056/NEJ Moa 1700445 · doi ↗ · pubmed ↗
- 5Lanzafame L.R.M. Bucolo G.M. Muscogiuri G. Sironi S. Gaeta M. Ascenti G. Booz C. Vogl T.J. Blandino A. Mazziotti S. Artificial Intelligence in Cardiovascular CT and MR Imaging Life 20231350710.3390/life 1302050736836864 PMC 9968221 · doi ↗ · pubmed ↗
- 6D’Angelo T. Caudo D. Blandino A. Albrecht M.H. Vogl T.J. Gruenewald L.D. Gaeta M. Yel I. Koch V. Martin S.S. Artificial intelligence, machine learning and deep learning in musculoskeletal imaging: Current applications J. Clin. Ultrasound 2022501414143110.1002/jcu.2332136069404 · doi ↗ · pubmed ↗
- 7Mc Collough C. Leng S. Use of artificial intelligence in computed tomography dose optimisation Ann. ICRP 20204911312510.1177/014664532094082732870019 · doi ↗ · pubmed ↗
- 8Zhang S. Zhu Z. Yu Z. Sun H. Sun Y. Huang H. Xu L. Wan J. Effectiveness of AI for Enhancing Computed Tomography Image Quality and Radiation Protection in Radiology: Systematic Review and Meta-Analysis J. Med. Internet Res.202527 e 6662210.2196/6662240053787 PMC 11907168 · doi ↗ · pubmed ↗