Frequency of Acute Stress Disorder (ASD) and Postnatal Depression in Mothers Of Preterm Neonates Hospitalized in a Neonatal Intensive Care Unit (NICU) in Pakistan
Saima Fayyaz, AS Hussain, Maheen Choudhry, Vardah Noor Ahmed Bharuchi

TL;DR
This study found that nearly half of mothers of preterm infants in a Pakistani NICU experienced acute stress disorder and postnatal depression.
Contribution
The study provides new data on the mental health of mothers of preterm infants in a Pakistani NICU setting.
Findings
43.1% of mothers met criteria for Acute Stress Disorder (ASD).
Mothers with ASD had infants with lower birth weight and longer NICU stays.
ASD was associated with higher Edinburgh Postnatal Depression Scale scores.
Abstract
To determine the frequency of Acute Stress Disorder (ASD) and postnatal depression in mothers of preterm neonates hospitalized in the neonatal intensive care unit (NICU) of the Aga Khan University Hospital. It is a cross-sectional study. It was conducted in a 24-bed level-3 NICU at a tertiary care hospital in Karachi. Mothers of preterm newborns under 34 weeks’ gestational age admitted to the NICU were included in the study. Among 123 postpartum women, 43.1% (n=53) met criteria for Acute Stress Disorder (ASD), with significantly lower gestational age in this group: median 29.9 weeks (IQR: 27.6-31.0) vs. 33.0 weeks (IQR: 32.0-33.0) in non-ASD cases (difference in medians: 3.1 weeks, 95% CI: 2.1-4.0). Infants of mothers with ASD had a less mean birth weight (1.3 ± 0.4 kg) compared to those without ASD (1.8 ± 0.5 kg), with a mean difference of 0.5 kg (95% CI: 0.34-0.66). Median NICU stay…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
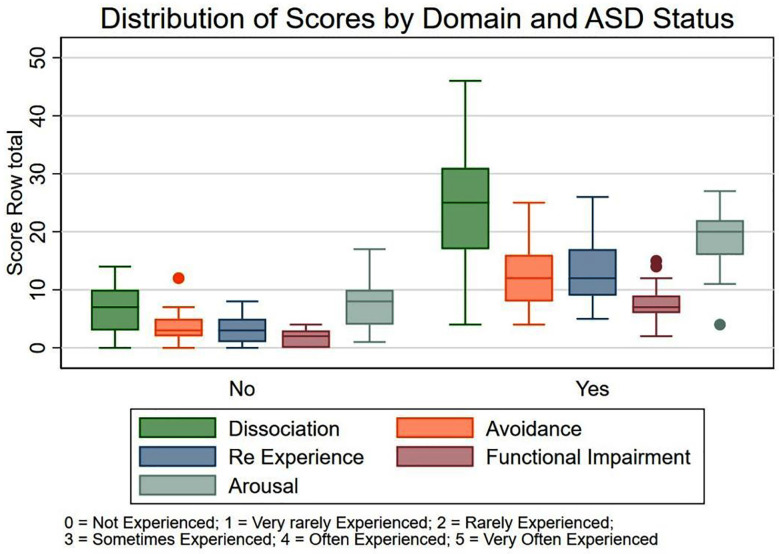 Fig.1
Fig.1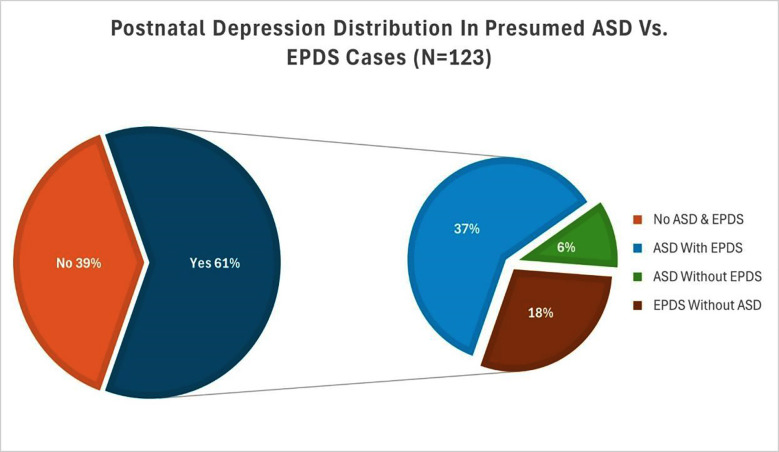 Fig.2
Fig.2| Variables | Range |
|---|---|
| Baseline Characteristics of Infants N=123 | n % |
| Gestational Age in Weeks, Median (IQR) | 32.0 (29.6-33.0) |
| Extremely preterm (<28 weeks) | 18 (14.6%) |
| Very preterm (28 - <32 weeks) | 34 (27.6%) |
| Moderate preterm (32 - <37 weeks) | 71 (57.7%) |
| Apgar Score at (1 min), Median (IQR) | 7.0 (6.0-8.0) |
| Apgar Score at (10 min), Median (IQR) | 9.0 (8.0-9.0) |
| Baby’s Weight at birth in KG, Mean ± SD | 1.6 ± 0.5 |
| Days in NICU, Median (IQR) | 14.0 (7.0-20.0) |
| < 13 days | 60 (48.8%) |
| ≥ 13 days | 63 (51.2%) |
| Mother’s Age (yrs), Mean ± SD | 30.6 ± 5.3 |
|---|---|
| 18-29 years old | 60 (48.8%) |
| 30-59 years old | 63 (51.2%) |
| Married Since, Median (IQR) | 4.0 (2.0-6.0) |
| < 3 years | 38 (30.9%) |
| ≥ 3 years | 85 (69.1%) |
| No. of Children, Mean ± SD (n=122) | 1.0 ± 1.2 |
| No. of Children, Median (IQR) (n=122) | 1.0 (0.0-2.0) |
| Alive, Mean ± SD | 0.8 ± 1.1 |
| Alive, Median (IQR) | 0.0 (0.0-1.0) |
| Deceased, Mean ± SD | 0.1 ± 0.5 |
| Deceased, Median (IQR) | 0.0 (0.0-0.0) |
|
| |
| No | 113 (91.9%) |
| Yes | 10 (8.1%) |
|
| |
| No | 83 (67.5%) |
| Yes | 40 (32.5%) |
|
| |
| No | 116 (94.3%) |
| Yes | 7 (5.7%) |
|
| |
| No | 118 (95.9%) |
| Yes | 5 (4.1%) |
|
| |
| No | 104 (84.6%) |
| Yes | 19 (15.4%) |
|
| |
| Matric | 3 (2.4%) |
| Intermediate | 12 (9.8%) |
| Undergraduate | 21 (17.1%) |
| Graduate | 58 (47.2%) |
| Masters | 29 (23.6%) |
|
| |
| No | 91 (74.0%) |
| Yes | 32 (26.0%) |
|
| |
| < 50,000 | 2 (1.6%) |
| 50,000-100,000 | 5 (4.1%) |
| 100,000-200,000 | 23 (18.7%) |
| > 200,000 | 93 (75.6%) |
| Edinburgh Postnatal depression Scale (EPDS) Total Score, Median (IQR) | 15.0 (10.0-19.0) |
| No | 56 (45.5%) |
| Yes | 67 (54.5%) |
|
| |
| Not at all disturbing | 6 (4.9%) |
| Somewhat disturbing | 31 (25.2%) |
| Moderately disturbing | 15 (12.2%) |
| Very disturbing | 39 (31.7%) |
| Extremely disturbing | 32 (26.0%) |
| Stanford Acute Stress Reaction Questionnaire (SASRQ) Total Score, Median (IQR) | 36.0 (19.0-70.0) |
|
| |
| No | 70 (56.9%) |
| Yes | 53 (43.1%) |
|
| |
| ASD With EPDS | 45 (36.6%) |
| ASD Without EPDS | 8 (6.5%) |
| EPDS Without ASD | 22 (17.9%) |
| No ASD & EPDS | 48 (39.0%) |
| No. of days pt experienced symptoms of distress, Median (IQR) | 5.0 (3.0-5.0) |
|
| |
| Boy | 82 (66.7%) |
| Girl | 41 (33.3%) |
| Factors associated with Acute Stress Disorder (ASD), N=123 | Yes | No | p-value |
|---|---|---|---|
| 53 (43.1%) | 70 (56.9%) | ||
| Mother’s Age (yrs), Mean ± SD | 30.8 ± 5.8 | 30.5 ± 4.9 | 0.79 |
| 18-29 years old | 29 (54.7%) | 31 (44.3%) | 0.25 |
| 30-59 years old | 24 (45.3%) | 39 (55.7%) | |
| Married Since, Median (IQR) | 5.0 (3.0-7.0) | 3.0 (2.0-5.0) | 0.19 |
| < 3 years | 13 (24.5%) | 25 (35.7%) | 0.18 |
| ≥ 3 years | 40 (75.5%) | 45 (64.3%) | |
| No. of Children, Mean ± SD, n= 122 | 1.0 ± 1.2 | 0.9 ± 1.1 | 0.72 |
| No. of Children, Median (IQR), n= 122 | 1.0 (0.0-2.0) | 1.0 (0.0-2.0) | 0.82 |
| Alive, Mean ± SD | 0.9 ± 1.1 | 0.8 ± 1.1 | 0.49 |
| Alive, Median (IQR) | 1.0 (0.0-2.0) | 0.0 (0.0-1.0) | 0.42 |
| Deceased, Mean ± SD | 0.2 ± 0.5 | 0.1 ± 0.4 | 0.37 |
| Deceased, Median (IQR) | 0.0 (0.0-0.0) | 0.0 (0.0-0.0) | 0.4 |
| Child Death History | 0.33 | ||
| No | 47 (88.7%) | 66 (94.3%) | |
| Yes | 6 (11.3%) | 4 (5.7%) | |
| Miscarriage History | 0.025 | ||
| No | 30 (56.6%) | 53 (75.7%) | |
| Yes | 23 (43.4%) | 17 (24.3%) | |
| Premature Birth History | 0.14 | ||
| No | 48 (90.6%) | 68 (97.1%) | |
| Yes | 5 (9.4%) | 2 (2.9%) | |
| NICU Admission History | 0.65 | ||
| No | 50 (94.3%) | 68 (97.1%) | |
| Yes | 3 (5.7%) | 2 (2.9%) | |
| Trauma History | 0.015 | ||
| No | 40 (75.5%) | 64 (91.4%) | |
| Yes | 13 (24.5%) | 6 (8.6%) | |
| Education Level | 0.93 | ||
| Matric | 1 (1.9%) | 2 (2.9%) | |
| Intermediate | 5 (9.4%) | 7 (10.0%) | |
| Undergraduate | 10 (18.9%) | 11 (15.7%) | |
| Graduate | 23 (43.4%) | 35 (50.0%) | |
| Masters | 14 (26.4%) | 15 (21.4%) | |
| Employed | <0.001 | ||
| No | 30 (56.6%) | 61 (87.1%) | |
| Yes | 23 (43.4%) | 9 (12.9%) | |
| Family Income | 0.41 | ||
| < 50,000 | 2 (3.8%) | 0 (0.0%) | |
| 50,000-100,000 | 3 (5.7%) | 2 (2.9%) | |
| 100,000-200,000 | 9 (17.0%) | 14 (20.0%) | |
| > 200,000 | 39 (73.6%) | 54 (77.1%) | |
| Gestational Age in Weeks, Median (IQR) | 29.9 (27.6-31.0) | 33.0 (32.0-33.0) | <0.001 |
| Preterm | <0.001 | ||
| Extremely preterm (<28 weeks) | 14 (26.4%) | 4 (5.7%) | |
| Very preterm (28 - <32 wks) | 27 (50.9%) | 7 (10.0%) | |
| Moderate preterm (32 - <37 wks) | 12 (22.6%) | 59 (84.3%) | |
| Baby’s Weight in KG, Mean ± SD | 1.3 ± 0.4 | 1.8 ± 0.5 | <0.001 |
| Days in NICU, Median (IQR) | 20.0 (12.0-28.0) | 10.0 (7.0-15.0) | <0.001 |
| < 13 days | 14 (26.4%) | 46 (65.7%) | <0.001 |
| ≥ 13 days | 39 (73.6%) | 24 (34.3%) | |
| Apgar Score at (1 min), Median (IQR) | 6.0 (5.0-8.0) | 7.0 (7.0-8.0) | 0.021 |
| Apgar Score at (10 min), Median (IQR) | 8.0 (7.0-9.0) | 9.0 (9.0-9.0) | <0.001 |
| Edinburgh Postnatal depression Scale (EPDS) Total Score, Median (IQR) | 19.0 (17.0-21.0) | 11.0 (9.0-15.0) | <0.001 |
| No | 8 (15.1%) | 48 (68.6%) | <0.001 |
| Yes | 45 (84.9%) | 22 (31.4%) | |
| Most Disturbing Event Level (1-5) | <0.001 | ||
| Not at all disturbing | 0 (0.0%) | 6 (8.6%) | |
| Somewhat disturbing | 5 (9.4%) | 26 (37.1%) | |
| Moderately disturbing | 4 (7.5%) | 11 (15.7%) | |
| Very disturbing | 18 (34.0%) | 21 (30.0%) | |
| Extremely disturbing | 26 (49.1%) | 6 (8.6%) | |
| Postnatal depression | <0.001 | ||
| ASD With EPDS | 45 (84.9%) | 0 (0.0%) | |
| ASD Without EPDS | 8 (15.1%) | 0 (0.0%) | |
| EPDS Without ASD | 0 (0.0%) | 22 (31.4%) | |
| No ASD & EPDS | 0 (0.0%) | 48 (68.6%) | |
| No. of days pt experienced symptoms of distress, Median (IQR) | 6.0 (5.0-6.0) | 3.0 (2.0-4.0) | <0.001 |
| Gender | 0.52 | ||
| Boy | 37 (69.8%) | 45 (64.3%) | |
| Girl | 16 (30.2%) | 25 (35.7%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal Mental Health During Pregnancy and Postpartum · Infant Development and Preterm Care · Preterm Birth and Chorioamnionitis
INTRODUCTION
A preterm birth occurs before 37 weeks of gestation.1 Advances in neonatal intensive care have resulted in dramatically higher survival rates for preterm neonates. Preterm birth is still associated with considerable childhood mortality and morbidity.2 Having a newborn child admitted to the Neonatal Intensive Care Units (NICU) is an unexpected and frightening experience for parents.3 Parents may be concerned about their child’s health and survival, in addition to experiencing separation from their newborn, expected issues of accessing information and talking with the medical staff.4 According to research, bonding with newborns begins before delivery and evolves afterward however, if the birth arrives sooner than planned, the usual bonding process may be disrupted.5 The experience of a preterm delivery affects parents’ emotional health both immediately and over time, which may influence the child’s long-term development.6
Although the NICU has experienced considerable adjustments in the recent decade to facilitate the presence of parents throughout their baby’s hospitalisation, the NICU continues to be a stressful place for parents, as proved in several studies.7 Previous studies have consistently demonstrated that feelings of parental stress, estrangement and heightened anxiety are widespread.3-8 According to studies, parents who experience stressful events such as NICU/pediatric intensive care unit (PICU) admission and pediatric traumas may exhibit symptoms of Acute stress disorder (ASD). The DSM-5 describes ASD as the development of specific fear behaviors that last from three days to one month after a traumatic event. Diagnostic criteria for ASD involve symptoms of dissociation, reexperiencing, avoidance, and hyperarousal that cause significant impairment to everyday functioning. ASD has been used as a marker to reasonably predict post-traumatic stress disorder (PTSD).9 Postpartum ASD was diagnosed in 14.9% of mothers and 4.8% in fathers with very low birth weight infants, but in no mother or father with term infants.10 In another study on the prevalence of posttraumatic stress in parents of infants in the NICU, it was found that 35% of mothers and 24% of fathers met the ASD diagnostic criteria.11
Our research aimed to investigate the frequency of ASD and postnatal depression in mothers with preterm infants admitted to the NICU. The significant proportion, with approximately 30-40 % of monthly preterm admissions in our NICU, underscores the relevance and urgency of understanding the psychological consequences for mothers in this specific population.
METHODOLOGY
The is a cross-sectional study done in a 24-bed level-3 NICU at Aga Khan University Hospital in Karachi. The study was conducted between July 2024 to February 2025.
Ethics Statement:
Informed written consent was obtained from each participant prior to data collection. All data were collected anonymously and kept confidential in accordance with the Declaration of Helsinki guidelines.
Ethical Approval:
This study was reviewed and approved by the Ethics Review Committee of Aga Khan University, Karachi, Pakistan (ERC Reference No.: 2024-9927-29911).
Inclusion Criteria:
Mothers of preterm newborns below 34 weeks’ gestational age admitted to the NICU, including multiple births, who offer written informed consent.
Exclusion Criteria:
Mothers whose infants had known fetal abnormalities or a serious disease that required compassionate care, as evaluated by the Physician NICU. Mothers who were not visiting their infants due to any medical condition or had been diagnosed with a mental health illness and at that time taking antidepressant, as these characteristics might alter maternal-infant contact and affect study outcomes.
Sample Size:
The sample size was calculated using OpenEpi, version 3. A comparable survey found that 34.9% of preterm mothers were diagnosed with ASD.11 The sample size was determined to be 119. However, research on postnatal depression found that the prevalence of postnatal depression ranges between 3.5% and 40%. 12 Hence, the ultimate sample size is 123.
Sampling Method:
Study participants were conveniently sampled through a Structured Interview.
Data Collection:
Interviews were caried out 2-4 weeks after admission to NICU. The research team used validated Stanford Acute Stress Reaction Questionnaire (SASRQ) for (ASD) and the Edinburgh Postnatal Depression Scale (EPDS) for Depression. Participants filled up a demographic questionnaire. Data on newborn characteristics such as gestational age, birth weight, Apgar scores, and length of stay in the NICU were retrieved from medical records.
Statistical Analysis:
The data were analysed using PSPP software. Descriptive statistics were utilised to sum up maternal and neonatal parameters. Continuous variables were measured using means and standard deviations, whilst categorical data were reported using frequencies and percentages. Associations between potential predictors and outcomes (ASD and postpartum depression) were evaluated using chi-square tests.
RESULTS
For this study, 123 premature babies were enrolled.
Participants:
Descriptive Data:
For this study, 123 premature babies were enlisted. The mean and SD were used to summarize continuous variables for descriptive analysis, whereas frequencies and percentages were used to report the categorical variables.
Outcome data:
Baseline characteristics of Preterm Neonates:
The baseline attributes of preterm neonates as shown in Table-I. With an IQR of 29.6 to 33.0 weeks and a median gestational age of 32.0 weeks. The majority of them (57.7%) were moderately preterm (32 - <37 weeks). Apgar scores are a rapid indicator of a newborn’s physical health just after birth. Median values and IQRs are reported for 1 and 10 minutes post-delivery. At one minute after delivery, the median Apgar score was 7.0 (IQR: 6.0-8.0), and ten minutes later, it improved to 9.0 (IQR: 8.0-9.0). The average birth weight was 1.6 ± 0.5 kg, which is in line with (Table-I) overall preterm status. Additionally, it revealed that the period of supportive care needed varied, with a median of 14.0 days and an IQR of 7.0 to 20.0 days for NICU hospitalization. While 51.2% of infants needed extended hospital admissions, almost 60 (48.8%) had NICU stays that were comparatively shorter, suggesting a quicker clinical recovery or less need for intensive assistance.
Gynaecological and Sociodemographic Characteristics of the mothers of Preterm babies:
The mean age of the mothers was 30.6 ± 5.3 years. The median duration of marriage was 4.0 years (IQR: 2.0-6.0), with 69.1% being married for three or more years. Among 123 respondents, the mean number of children was 1.0 ± 1.2, with a median of 1.0 (IQR: 0.0-2.0). The mean number of living children was 0.8 ± 1.1, and of deceased children was 0.1 ± 0.5. A history of child death was reported by 8.1% of participants, while 32.5% reported a history of miscarriage. Premature birth had occurred in 5.7%, and NICU admission was reported by 4.1%. A history of trauma was present in 15.4% of the mothers. The majority of mothers were graduates (47.2%). Regarding household income, 75.6% reported a monthly income of more than PKR 200,000.
Psychological Health Status of Mothers:
The median EPDS score was 15.0 (IQR: 10.0-19.0). Based on EPDS scores, 54.5% of mothers screened positive for postnatal depression, while 45.5% did not. The median SASRQ score was 36.0 (IQR: 19.0-70.0). ASD was present in 43.1% of mothers. Around 36.6% of mothers had both ASD and postnatal depression, as displayed in (Table-II).
A significant association (<0.025) between miscarriage history and ASD. Mothers who had experienced miscarriage were more likely to develop ASD, possibly due to the cumulative psychological burden. ASD was substantially more common in mothers of preterm infants, particularly those born extremely or very preterm. Mothers with ASD were also more likely to suffer from postnatal depression (<0.001). Most mothers with ASD (84.9%) also obtained high scores on the EPDS. This highlights the overlap between ASD and depressive symptoms postpartum. Longer NICU stays, especially stays ≥13 days, significantly increase ASD risk (<0.001), possibly due to prolonged maternal stress, uncertainty, and separation from the infant. At one and ten minutes, the ASD group’s median Apgar scores were lower, indicating worse neonatal outcomes.
A statistically significant (<0.001) relationship was found that prior exposure to trauma may predispose mothers to acute stress reactions following childbirth-related stressors. Nearly half of the mothers with ASD rated the most upsetting incident as “extremely disturbing,” indicating higher levels of distress. ASD was substantially correlated with employment, which may be a reflection of added stress from juggling job and caring obligations. Participants with ASD report much greater and more varied symptom severity across all categories, particularly dissociation and re-experience (Fig.1).
Frequency of ASD symptoms among mothers.
The majority of postpartum mothers (61%) reported having clinically severe depressive symptoms, as seen in (Fig.2). A significant psychological load was indicated by the fact that more than one-third (37%) had both postnatal depression and ASD. These results emphasize the necessity of early intervention and frequent screening in the postnatal period.
Postnatal Depression Distribution in Presumed ASD vs. EPDS Cases.
DISCUSSION
This study fills a major gap in the local literature to evaluate the prevalence of postnatal depression and ASD in mothers of preterm newborns admitted to the NICU in the Pakistani population. There is a significant paucity of Pakistani research on the NICU experience as a parental stressor. The average maternal age was 30.6 years, with about equal distribution between the younger (18-29 years; 48.8%) and older (30-59 years; 51.2%) age groups. The median marital duration of four years, with 69.1% of women married for ≥3 years, suggests a solid marital context, which is frequently considered protective against prenatal mental health issues. Despite this, a large proportion of mothers (54.5%) tested positive for postnatal depression using the EPDS and 43.1% fulfilled criteria for ASD using the SASRQ.
The dissociation and arousal domains had significantly higher median and interquartile range values, indicating frequent and varied stress-related symptoms in these regions. Prior obstetric hardship was not rare, despite the comparatively low average number of children per mother (Mean = 1.0 ± 1.2) and the infrequent reporting of child loss (8.1%). Approximately one-third (32.5%) had experienced a miscarriage, while 5.7% and 4.1% reported premature births and NICU admissions, respectively. Previous study proved that the incidence of ASD/PTSD has been associated with psychosocial stressors, trauma exposure, and demographic characteristics.12 Although delivering a baby is typically a happy event, many postpartum women develop depressive symptoms and disorders.13 According to the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM-5), onset of postpartum major depression can occur prior to or after parturition.14
The DSM-5 specifier “with peripartum onset” is used when the onset of major depression occurs either during pregnancy or in the four weeks following delivery. According to randomized control trials reasonable time to screen is four to eight weeks after delivery.15-16 Holditch and associates found significant depressive symptoms in 40% of mothers of very premature infants compared with 10% to 15% of the population.17 According to another study, the prevalence of postnatal depression varies significantly. Due to time restrictions and concerns about the social acceptability of screening, these illnesses, despite their frequency, are typically neither recognized nor treated.18 In this cross-sectional study we used the SASRQ and EPDS which are well validated instruments to ensure accurate measurement of acute stress and postpartum depression.
The SASRQ identifies acute stress symptoms across dissociation, re-experiencing, avoidance, arousal, and functional impairment. The requirement of multiple dissociative symptoms (≥3) increases diagnostic specificity and authenticity.19-20 EPDS has been considered extensively validated for postpartum populations of Asia.21 According to Stefanie Zaers et al.’s study, 22% of women experienced depression symptoms six weeks after giving birth.22 According to a study conducted in Iran by Naeem, Azam Naeem et al., 32.5% of mothers experienced ASD shortly after birth, with 40% developing PTSD a month later.23 Allison Baylor Williams et al. discovered that about 55 percent of NICU mothers had ASD symptoms.24
Our study suggests that socio-demographic indicators further contextualise the findings, which goes against the usual trends that emphasise the universality of postpartum emotional distress and challenge the conventional wisdom that perinatal mental health burdens are more common in socioeconomically disadvantaged populations. The majority of mothers (70.8%) were educated at the graduate level or above, and over three-quarters (75.6%) came from households with higher incomes (>PKR 200,000), indicating that psychological morbidity was not limited to low-resource groups’ distress. According to our study’s results, 61% of participants had positive results for postnatal depression on the EPDS. According to research by Anna Alkozei et al., 38% of mothers exhibited major depression symptoms (EPDS score ≥10) and 52% of mothers reported higher levels of stress (PSS: NICU score ≥3). The biggest cause of stress among NICU mothers was stress associated with changes in their parental roles.25
In a Ghanaian cohort, John Pellegrino et al. employed the Perceived Stress Scale-4 (PSS-4) and the Patient Health Questionnaire-9 (PHQ-9) to determine that 43.5% of the population had postpartum stress, whereas 3.9% of the population had moderate to moderately severe postpartum depression.26 According to a study by Kameelah Gateau et al., which involved a majority of Hispanic, non-English speaking individuals, 33% of mothers tested positive for acute PTS.27 According to a study by Jubinville et al., 43% of mothers of premature infants in the NICU experienced severe depressive symptoms 7-10 days after the baby was born, and the symptoms persisted for a month.28
Strengths:
This study ensures data dependability by using standardised screening instruments in a tertiary care context. Additionally, focusing on an under-researched population highlights important cultural and contextual factors relevant to maternal mental health in low- and middle-income countries.
Limitations:
A cross-sectional study design was employed. However, longitudinal or prospective cohort studies may yield better results. The study has limited generalisability.
CONCLUSION
Recognizing ASD in the early stages is crucial, as it can potentially impact the long-term mental health outcomes for both mothers and their infants. The premature birth experience is traumatic for mothers and may lead to various emotional responses, including stress-related symptoms such as postnatal depression and/or ASD. Mothers with significant symptoms of depression and those with symptoms of stress are more at risk for developing symptoms of ASD followed by PTSD. These findings encourage the inclusion of mental health services in programs for the care of mothers and highlight the importance of routine psychological screening throughout the postnatal period, irrespective of socioeconomic position. Importantly, the presence of ASD alone, or in combination with depression, may impair maternal-infant bonding and breastfeeding, and affect long-term neurodevelopmental outcomes for the infant. Therefore, early recognition and intervention are essential.
Authors’ Contribution:
SF: Conceived, designed and did statistical analysis & editing of manuscript, is responsible for integrity of research.
SF, MC and VNAB: Did data collection and manuscript writing.
AS: Did critical review and final approval of manuscript..
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Quinn JA Munoz FM Gonik B Frau L Cutland C Mallett-Moore T Preterm birth: Case definition &guidelines for data collection, analysis, and presentation of immunization safety data Vaccine 2016344960476056 doi: 10.1016/j.vaccine.2016.03.0452774364810.1016/j.vaccine.2016.03.045PMC 5139808 · doi ↗ · pubmed ↗
- 2Garg D Chaudhury S Saldanha D Kumar S Stress, postpartum depression, and anxiety in mothers of neonates admitted in the NICU: A cross-sectional hospital-based study Ind Psychiatry J 20233214854 doi: 10.4103/ipj.ipj_93_223727456610.4103/ipj.ipj_93_22PMC 10236660 · doi ↗ · pubmed ↗
- 3Shaw RJ Deblois T Ikuta L Ginzburg K Fleisher B Koopman C Acute stress disorder among parents of infants in the neonatal intensive care nursery Psychosomatics 2006473206212 doi: 10.1176/appi.psy.47.3.2061668493710.1176/appi.psy.47.3.206 · doi ↗ · pubmed ↗
- 4Malouf R Harrison S Burton HA Gale C Stein A Franck LS Prevalence of anxiety and post-traumatic stress among parents of babies admitted to neonatal units: A systematic review and meta-analysis E Clinical Medicine 202243101233 doi: 10.1016/j.eclinm.2021.1012333499342510.1016/j.eclinm.2021.101233 PMC 8713115 · doi ↗ · pubmed ↗
- 5Goldberg S Di Vitto B Parenting children born preterm(Suspicious) recheck this reference
- 6Howard K Martin A Berlin LJ Brooks-Gunn J Early mother-child separation, parenting, and child well-being in Early Head Start families Attach Hum Dev 2011131526 doi: 10.1080/14616734.2010.4881192124069210.1080/14616734.2010.488119 PMC 3115616 · doi ↗ · pubmed ↗
- 7Franck LS Cox S Allen A Winter I Measuring NICU-related parental stress J Adv Nurs 2005496608615 doi: 10.1111/j.1365-2648.2004.03336.x 1573722110.1111/j.1365-2648.2004.03336.x · doi ↗ · pubmed ↗
- 8Vanderbilt D Bushley T Young R Frank DA Acute posttraumatic stress symptoms among urban mothers with newborns in the NICU: A preliminary study J Dev Behav Pediatr 20093015056 doi: 10.1097/DBP.0b 013e 318196 b 0de 1919432210.1097/DBP.0b 013e 318196 b 0de · doi ↗ · pubmed ↗