GLP-1 Receptor Agonist Use and Survival Among Patients With Type 2 Diabetes and Brain Metastases
Kuan-Yu Chi, Yu Chang, Junmin Song, Chien-Min Chen, Pang-Shuo Perng, Hong-Min Lin

TL;DR
This study examines if using GLP-1 receptor agonists affects survival in type 2 diabetes patients with brain metastases.
Contribution
It explores the novel association between GLP-1 RA use and survival outcomes in this specific patient population.
Findings
The study evaluates survival rates among patients using GLP-1 receptor agonists.
It investigates whether GLP-1 RA use is associated with improved or worsened survival in patients with brain metastases.
Findings may inform treatment strategies for type 2 diabetes patients with brain metastases.
Abstract
This cohort study assesses the association between glucagon-like peptide–1 receptor agonist (GLP-1 RA) use and survival in patients with type 2 diabetes and brain metastases.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Characteristic | Before propensity score matching | After propensity score matching | ||||
|---|---|---|---|---|---|---|
| Patients, No. (%) | Patients, No. (%) | SMD | ||||
| GLP-1 RA (n = 866) | No GLP-1 RA (n = 11 103) | GLP-1 RA (n = 850) | No GLP-1 RA (n = 850) | |||
| Age at index, mean (SD), y | 64.3 (10.3) | 67.7 (10.5) | <.001 | 64.5 (10.2) | 65.0 (10.4) | 0.050 |
| Sex | ||||||
| Male | 393 (45.4) | 5594 (50.4) | .005 | 387 (45.5) | 377 (44.4) | 0.024 |
| Female | 471 (54.4) | 5505 (49.6) | .006 | 461 (54.2) | 470 (55.3) | 0.021 |
| Race | ||||||
| Asian | 47 (5.4) | 731 (6.6) | .18 | 46 (5.4) | 43 (5.1) | 0.016 |
| Black or African American | 120 (13.9) | 1572 (14.2) | .81 | 117 (13.8) | 119 (14.0) | 0.007 |
| White | 622 (71.8) | 7319 (65.9) | <.001 | 610 (71.8) | 625 (73.5) | 0.040 |
| Other | 32 (3.7) | 358 (3.2) | .45 | 32 (3.8) | 32 (3.8) | <0.001 |
| Unknown | 34 (3.9) | 969 (8.7) | <.001 | 34 (4.0) | 25 (2.9) | 0.058 |
| Ethnicity | ||||||
| Hispanic or Latino | 54 (6.2) | 608 (5.5) | .35 | 52 (6.1) | 54 (6.4) | 0.010 |
| Not Hispanic or Latino | 658 (76.0) | 7914 (71.3) | .003 | 645 (75.9) | 648 (76.2) | 0.008 |
| Unknown | 154 (17.8) | 2581 (23.2) | <.001 | 153 (18.0) | 148 (17.4) | 0.015 |
| Malignant entity | ||||||
| Lung cancer | 315 (36.4) | 4440 (40.0) | .04 | 312 (36.7) | 306 (36.0) | 0.015 |
| Breast cancer | 145 (16.7) | 1601 (14.4) | .06 | 140 (16.5) | 151 (17.8) | 0.034 |
| Melanoma | 81 (9.4) | 803 (7.2) | .02 | 80 (9.4) | 71 (8.4) | 0.037 |
| Colon cancer | 27 (3.1) | 389 (3.5) | .55 | 27 (3.2) | 22 (2.6) | 0.035 |
| Rectal cancer | 12 (1.4) | 149 (1.3) | .91 | 12 (1.4) | 13 (1.5) | 0.010 |
| Kidney cancer | 66 (7.6) | 617 (5.6) | .01 | 63 (7.4) | 56 (6.6) | 0.032 |
| Malignant neoplasm of larynx | 10 (1.2) | 51 (0.5) | .006 | 10 (1.2) | 10 (1.2) | <0.001 |
| Bone metastases | 210 (24.2) | 2679 (24.1) | .94 | 205 (24.1) | 203 (23.9) | 0.006 |
| Comorbidities | ||||||
| Essential hypertension | 684 (79.0) | 7776 (70.0) | <.001 | 672 (79.1) | 690 (81.2) | 0.053 |
| Heart failure | 153 (17.7) | 1529 (13.8) | .001 | 150 (17.6) | 156 (18.4) | 0.018 |
| Ischemic heart diseases | 319 (36.8) | 3298 (29.7) | <.001 | 309 (36.4) | 316 (37.2) | 0.017 |
| Atrial fibrillation and flutter | 109 (12.6) | 1415 (12.7) | .89 | 106 (12.5) | 102 (12.0) | 0.014 |
| Cerebrovascular diseases | 257 (29.7) | 2245 (20.2) | <.001 | 245 (28.8) | 205 (24.1) | 0.107 |
| Morbid obesity | 210 (24.2) | 1103 (9.9) | <.001 | 199 (23.4) | 204 (24.0) | 0.014 |
| Nicotine dependence | 195 (22.5) | 2587 (23.3) | .60 | 192 (22.6) | 188 (22.1) | 0.011 |
| Alcohol-related disorders | 30 (3.5) | 458 (4.1) | .34 | 30 (3.5) | 30 (3.5) | <0.001 |
| Chronic kidney disease | 234 (27.0) | 2283 (20.6) | <.001 | 228 (26.8) | 241 (28.4) | 0.034 |
| Other chronic obstructive pulmonary disease | 192 (22.2) | 2368 (21.3) | .56 | 190 (22.4) | 197 (23.2) | 0.020 |
| Procedures | ||||||
| SRS, multisource cobalt 60 based | 24 (2.8) | 158 (1.4) | .002 | 24 (2.8) | 16 (1.9) | 0.062 |
| SRS, linear accelerator based | 29 (3.3) | 180 (1.6) | <.001 | 28 (3.3) | 19 (2.2) | 0.065 |
| Stereotactic body radiation therapy | 56 (6.5) | 488 (4.4) | .005 | 53 (6.2) | 36 (4.2) | 0.090 |
| Craniectomy or craniotomy procedures | 68 (7.9) | 340 (3.1) | <.001 | 62 (7.3) | 51 (6.0) | 0.052 |
| Medications | ||||||
| Antineoplastic therapy | 418 (48.3) | 4747 (42.8) | .002 | 411 (48.4) | 405 (47.6) | 0.014 |
| Systemic corticosteroids | 724 (83.6) | 8033 (72.4) | <.001 | 711 (83.6) | 693 (81.5) | 0.055 |
| Sodium-glucose cotransporter–2 inhibitors | 248 (28.6) | 727 (6.5) | <.001 | 236 (27.8) | 229 (26.9) | 0.018 |
| Metformin | 544 (62.8) | 4352 (39.2) | <.001 | 530 (62.4) | 543 (63.9) | 0.032 |
| Sulfonylureas | 262 (30.3) | 1995 (18.0) | <.001 | 258 (30.4) | 257 (30.2) | 0.003 |
| Thiazolidinediones | 83 (9.6) | 382 (3.4) | <.001 | 79 (9.3) | 87 (10.2) | 0.032 |
| Insulin | 664 (76.7) | 5393 (48.6) | <.001 | 648 (76.2) | 659 (77.5) | 0.031 |
| Dipeptidyl peptidase–4 inhibitors | 180 (20.8) | 1188 (10.7) | <.001 | 177 (20.8) | 182 (21.4) | 0.014 |
| Laboratory values, mean (SD) | ||||||
| Hemoglobin A1c, % | 7.9 (1.8) | 7.0 (1.6) | <.001 | 7.8 (1.8) | 7.5 (1.7) | 0.219 |
| Body mass index | 32.9 (7.4) | 29.1 (6.8) | <.001 | 32.9 (7.4) | 32.7 (6.9) | 0.031 |
| Estimated glomerular filtration rate, mL/min/1.73 m2 | 74.4 (33.1) | 77.8 (33.7) | .007 | 74.4 (32.9) | 75.7 (33.3) | 0.039 |
| Visit type | ||||||
| Emergency department | 456 (52.7) | 5104 (46.0) | <.001 | 446 (52.5) | 442 (52.0) | 0.009 |
| Inpatient encounter | 518 (59.8) | 5311 (47.8) | <.001 | 505 (59.4) | 481 (56.6) | 0.057 |
| Ambulatory | 778 (89.8) | 9713 (87.5) | .04 | 763 (89.8) | 776 (91.3) | 0.052 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Treatment and Management · Metabolism, Diabetes, and Cancer · Cancer, Lipids, and Metabolism
Introduction
Brain metastases (BM) are associated with substantial morbidity and mortality in patients with cancer.^1^ Comorbid type 2 diabetes (T2D) may worsen outcomes through metabolic and inflammatory pathways.^2^ Glucagon-like peptide–1 receptor agonists (GLP-1 RAs) have transformed beyond antiglycemic control, with emerging preclinical evidence suggesting potential neuroprotective and anti-inflammatory effects.^3^ However, clinical evidence evaluating their association with BM remains limited. Thus, we aimed to assess the association between GLP-1 RA use and survival in this population.
Methods
This retrospective cohort study used the TriNetX Global Network, a federated database comprising 151 health care organizations around the world.^4^ (eAppendix 1 in Supplement 1) This research was approved by the National Cheng Kung University Hospital institutional review board. This report was prepared in accordance with the STROBE reporting guidelines for cohort studies, where applicable.
Adult patients (aged ≥18 years) with cancer with BM and T2D between January 1, 2018, and January 1, 2024, were identified. The exposed cohort included patients prescribed GLP-1 RAs within 6 months before the first instance of T2D and BM diagnosis. The control cohort included those with no GLP-1 RA use over the same period. We excluded those with potential contraindications to GLP-1 RA use and those with lower socioeconomic status (eAppendix 2 in Supplement 1). One-to-one propensity score (PS) matching between 2 groups was performed using the greedy nearest-neighbor algorithm with a caliper width of 0.1 pooled SDs (Table). A standardized mean difference less than 0.10 indicated balanced covariates. The primary outcome was all-cause mortality up to 3 years from the study index date—namely, the first recorded date of BM. We also conducted subgroup analyses based on primary cancer sites, GLP-1 RA types, and comparison with other antidiabetic agents. We also set seizure events and pneumonia as falsification end points to examine study findings’ vulnerability to unmeasured confounders. Cox proportional hazards models were used to estimate hazard ratios (HRs) and 95% CIs for the outcome. Statistical significance was defined as 2-tailed P < .05. All analyses were performed within the TriNetX Analytic Platform.
Results
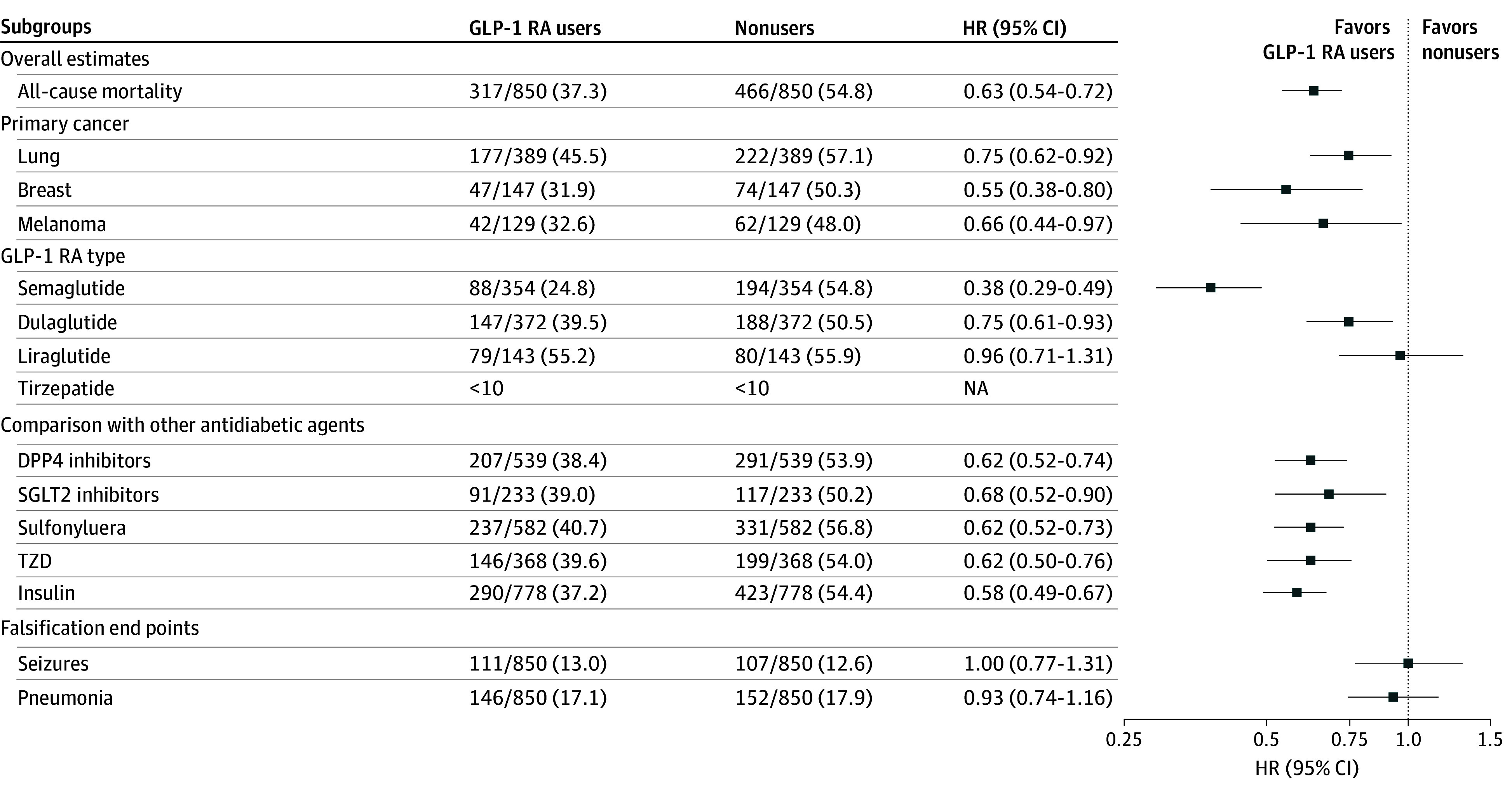
Among a total of 19 234 patients with cancer, BM, and T2D, 866 GLP-1 RA users (semaglutide, 369 patients; dulaglutide, 379 patients; liraglutide, 147 patients; and tirzepatide, 95 patients), and 11 103 nonusers met eligibility criteria. After PS matching, 850 GLP-1 RA users were matched to nonusers, with well-balanced baseline characteristics (Table).
GLP-1 RA use was associated with significantly lower all-cause mortality (HR, 0.63; 95% CI, 0.54-0.72; P < .001) (Figure). The observed mortality benefit remains consistent across major cancer types and GLP-1 RA types, except for liraglutide, and in comparison with other antidiabetic therapy (Figure). Falsification end points were comparable between the 2 groups (Figure).
Forest Plot of Study Findings With Subgroup Analyses and Falsification End PointsDPP4 indicates dipeptidyl peptidase–4; GLP-1 RA, glucagon-like peptide–1 receptor agonist; HR, hazard ratio; NA, not applicable; SGLT2, sodium-glucose cotransporter–2; TZD, thiazolidinedione.
Discussion
The findings of this cohort study suggest that GLP-1 RA use was associated with significant reduction in all-cause mortality among patients with cancer with BM and T2D, with generally consistent association across subgroups. These results build upon existing evidence that GLP-1 receptor activation modulates pathways relevant to neuro-oncologic health, including attenuation of neuroinflammation, preservation of blood–brain barrier integrity, and reduction of oxidative stress and mitochondrial dysfunction.^5,6^
Our study has several limitations. First, the retrospective design limits causal inference despite PS matching and comparable falsification end points. Second, the lack of individual-level data precluded dose-response analyses, detailed assessment of concomitant systemic and radiation therapies, and evaluation of cancer-specific mortality. Third, the restriction of 1:1 PS matching within TriNetX excluded substantial nonusers, limiting the generalizability of our findings to patients with sufficient covariate overlap. Fourth, participating health care organizations within TriNetX are mostly academic hospitals, also limiting the generalizability of our findings to nonacademic setting. GLP-1 RA was associated with significant reduction in all-cause mortality among patients with cancer with BM and T2D, warranting future prospective studies to further elucidate the effects of GLP-1 RA in cancer populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Boire A, Brastianos PK, Garzia L, Valiente M. Brain metastasis. Nat Rev Cancer. 2020;20(1):4-11. doi:10.1038/s 41568-019-0220-y 31780784 · doi ↗ · pubmed ↗
- 2Farmaki P, Damaskos C, Garmpis N, Garmpi A, Savvanis S, Diamantis E. Complications of the type 2 diabetes mellitus. Curr Cardiol Rev. 2020;16(4):249-251. doi:10.2174/1573403 X 160420122911553133407062 PMC 7903505 · doi ↗ · pubmed ↗
- 3Diz-Chaves Y, Mastoor Z, Spuch C, González-Matías LC, Mallo F. Anti-inflammatory effects of GLP-1 receptor activation in the brain in neurodegenerative diseases. Int J Mol Sci. 2022;23(17):9583. doi:10.3390/ijms 2317958336076972 PMC 9455625 · doi ↗ · pubmed ↗
- 4Palchuk MB, London JW, Perez-Rey D, . A global federated real-world data and analytics platform for research. JAMIA Open. 2023;6(2):ooad 035. doi:10.1093/jamiaopen/ooad 03537193038 PMC 10182857 · doi ↗ · pubmed ↗
- 5Salcedo I, Tweedie D, Li Y, Greig NH. Neuroprotective and neurotrophic actions of glucagon-like peptide-1: an emerging opportunity to treat neurodegenerative and cerebrovascular disorders. Br J Pharmacol. 2012;166(5):1586-1599. doi:10.1111/j.1476-5381.2012.01971.x 22519295 PMC 3419902 · doi ↗ · pubmed ↗
- 6Tseng YT, Tsai YH, Fülöp F, Chang FR, Lo YC. 2-Iodo-4′-methoxychalcone attenuates methylglyoxal-induced neurotoxicity by activation of GLP-1 receptor and enhancement of neurotrophic signal, antioxidant defense and glyoxalase pathway. Molecules. 2019;24(12):2249. doi:10.3390/molecules 2412224931208152 PMC 6631972 · doi ↗ · pubmed ↗