Syndromic Diagnostics for Travelers’ Diarrhea: Near-Patient Field-Expedient Testing in Resource-Limited Settings
Romeo Toriro, Christopher T Williams, Dominic L Wooding, Thomas Edwards, Matthew K O’Shea, Thomas E Fletcher, Nicholas J Beeching, Daniel S Burns, Stephen D Woolley

TL;DR
The study compares two diagnostic tests for travelers' diarrhea in resource-limited settings and finds that one is suitable for field use despite some limitations.
Contribution
Demonstrates the suitability of the FilmArray PCR platform for field diagnostics in low-resource areas despite moderate concordance with a reference standard.
Findings
FilmArray and Seegene PCR showed similar overall pathogen detection rates.
FilmArray had low sensitivity for Campylobacter and norovirus.
FilmArray is recommended for field use due to its versatility and ease of use.
Abstract
We assessed the diagnostic agreement of BioFire FilmArray multiplex polymerase chain reaction (PCR) with Seegene Allplex PCR for testing fecal samples collected during a diarrhea outbreak in resource-limited settings. Fecal samples from consented British military personnel training in Kenya were collected without preservative and tested onsite with the FilmArray PCR platform. Anonymized corresponding samples frozen near the point of care were tested 16–18 months later in the United Kingdom using Seegene PCR (reference standard). We compared test sensitivity and specificity and assessed agreement using Cohen κ coefficients. Samples were analyzed from 60 individuals (80% male; median age [interquartile range], 24 [22–28] years). The overall pathogen detection rates did not differ significantly between FilmArray and Seegene PCR (55 of 60 [91.7%] vs 53 of 59 [89.8%], respectively [P >…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
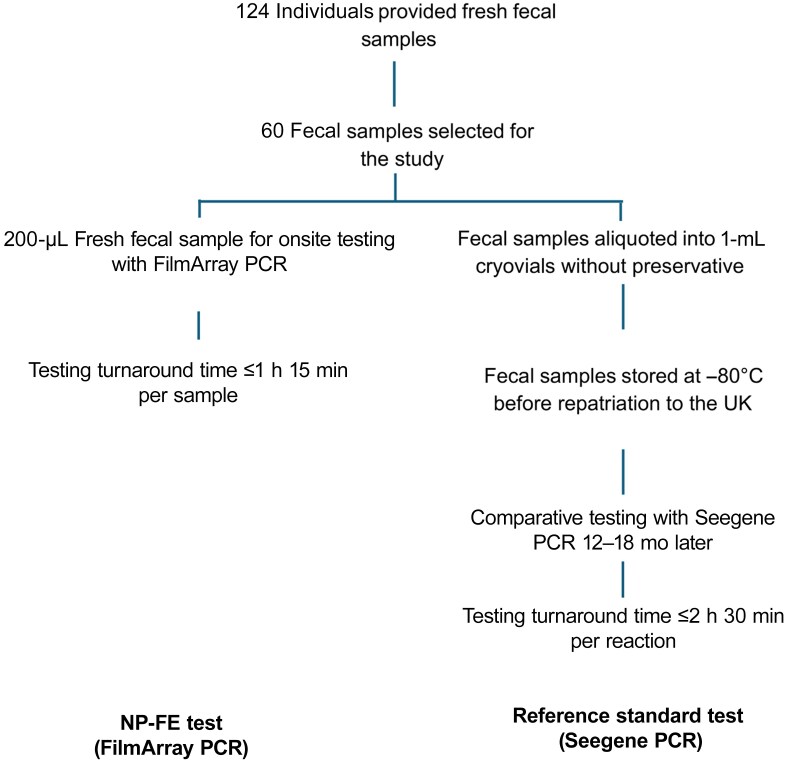 Figure 1
Figure 1| Enteropathogen | Samples by PCR Testing Platform, No. (%) | |
|---|---|---|
| Seegene (Reference Standard; n = 59) | FilmArray (NP-FE Test; n = 60) | |
| EAEC | 32 (54.2) | 22 (36.7) |
|
| 31 (52.5) | 25 (41.7) |
|
| 30 (51) | NA |
| EPEC | 27 (45.8) | 24 (40) |
|
| 17 (28.8) | 6 (10) |
| Norovirus | 14 (23.7) | 1 (1.7) |
|
| 8 (13.6) | NA |
|
| 6 (10.2) | 2 (3.3) |
| STEC | 3 (5.1) | 9 (15) |
| Sapovirus | 2 (3.4) | 2 (3.3) |
|
| 2 (3.4) | NA |
|
| 1 (1.7) | 1 (1.7) |
|
| 1 (1.7) | 1 (1.7) |
| Invalid test result | 1 (1.7) | 0 |
|
| 0 | 1 (1.7) |
|
| 0 | 1 (1.7) |
| Total individual enteropathogens | 134 | 95 |
| Sample Unique Identifier | Seegene PCR Platform | FilmArray PCR Platform |
|---|---|---|
| Negative at POC testing | ||
| S1 | Negative | Negative |
| S2 | Negative | Negative |
| S3 |
| Negative |
| S4 |
| Negative |
| S5 |
| Negative |
| Single enteropathogen at POC testing | ||
| S6 |
|
|
| S7 |
|
|
| S8 | Negative | STEC |
| S9 |
|
|
| S10 | EPEC | EPEC |
| S11 |
|
|
| S12 |
|
|
| S13 |
| STEC |
| S14 |
| EPEC |
| S15 |
| EPEC |
| S16 |
|
|
| S17 | Negative |
|
| S18 |
|
|
| S19 |
|
|
| S20 |
|
|
| S21 |
|
|
| S22 |
|
|
| S23 |
|
|
| S24 |
|
|
| S25 |
|
|
| 2 Enteropathogens at POC testing | ||
| S26 |
|
|
| S27 | Astrovirus, | Astrovirus, |
| S28 | EAEC | EAEC, EPEC |
| S29 |
| ETEC, STEC |
| S30 |
| EAEC, EPEC |
| S31 |
| EAEC, ETEC |
| S32 | Negative | EAEC, EPEC |
| S33 |
|
|
| S34 | EAEC | EAEC, STEC |
| S35 | EPEC | EAEC, EPEC |
| S36 | EPEC, ETEC, STEC, | ETEC, STEC |
| S37 | EPEC, ETEC, | EPEC, ETEC |
| S38 |
|
|
| S39 |
|
|
| S40 |
| EAEC, STEC |
| S41 | Invalid | EPEC, ETEC |
| S42 |
| EAEC, EPEC |
| S43 |
|
|
| S44 |
|
|
| Multiple enteropathogens at POC testing | ||
| S45 |
|
|
| S46 | Negative |
|
| S47 |
|
|
| S48 |
|
|
| S49 |
|
|
| S50 | Rotavirus |
|
| S51 |
| EAEC, EPEC, ETEC, rotavirus |
| S52 |
| EAEC, ETEC, EPEC, sapovirus |
| S53 |
|
|
| S54 |
| EAEC, |
| S55 |
|
|
| S56 | Astrovirus, |
|
| S57 |
| Astrovirus |
| S58 | EAEC, EPEC, ETEC | EAEC, EPEC, ETEC |
| S59 | EAEC, EPEC, ETEC | EAEC, ETEC, STEC |
| S60 |
| EAEC, EPEC, ETEC |
| Enteropathogen | FilmArray vs Seegene PCR Platform | |||
|---|---|---|---|---|
| Sensitivity | Specificity (95% CI), % | POA, | Cohen κ Coefficient | |
| EAEC | 63 (42.37–80.6) | 84.4 (67.21–94.72) | 74.6 | 0.48 |
|
| 65 (45.37–80.77) | 82.1 (63.11–93.94) | 72.9 | 0.46 |
| EPEC | 53.1 (34.74–70.91) | 74 (53.72–88.89) | 62.7 | 0.27 |
|
| 35.3 (14.21–61.67) | 100 (91.59–100) | 81.4 | 0.44 |
| Norovirus | 7.14 (0.18–33.87) | 100 (92.13–100.00) | 77.9 | 0.11 |
|
| 16.67 (0.42–64.12) | 98.11 (89.93 to 99.95) | 89.8 | 0.21 |
| STEC | 66.7 (9.43–99.16) | 87.5 (75.93–94.82) | 86.4 | 0.28 |
| Sapovirus | 50 (1.26–98.74) | 98.25 (90.61–99.96) | 96.6 | 0.48 |
|
| 100 (2.50–100) | 100 93.84–100 | 100 | 1 |
|
| 0 (0–97.50) | 98.28 (90.76–99.96) | 96.6 | −0.02 |
|
| NC | 98.31 (90.91–99.96) | NC | 0 |
|
| NC | 98.31 (90.91–99.96) | NC | 0 |
- —Army Health10.13039/100014054
- —Royal Army Medical Corps Charity10.13039/501100024588
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTravel-related health issues · Viral gastroenteritis research and epidemiology · Parasitic Infections and Diagnostics
Travelers' diarrhea (TD) is a common medical presentation that can have a significant impact on military operational effectiveness in both training and deployment settings [1, 2]. Its etiology depends on a number of factors, including seasonality, travel duration and destination, individual health status, and other determinants of health [3]. During TD outbreaks in resource-limited settings, the need to identify disease etiology is critical in informing clinical case management to curtail disease spread and minimize morbidity and medical evacuation [4] as well as in reinforcing force health protection measures, which include long-term surveillance, as has been highlighted in recent military deployments [1, 3, 5–7]. Rapid near-patient field-expedient (NP-FE) diagnostic capability to identify the causes of TD in forward military deployment locations has historically not been well documented [8]. However, recent studies have reported the utility of culture-independent molecular platforms, such as the field-expedient FilmArray multiplex polymerase chain reaction (PCR) gastrointestinal (GI) panel (bioMérieux) (FilmArray) to provide rapid identification of multiple enteropathogens [9, 10]. Other military studies conducted in austere settings have also highlighted the utility of the FilmArray platform as an ideal alternative or an adjunct to traditional culture methods [4, 6].
The FilmArray PCR platform commissioned for use by the UK Armed Forces in deployed hospital settings targets 22 enteropathogens in a single cartridge-based test on a random-access system with the capability to reduce hands-on time to about 3 minutes [11] and testing turnaround time to <2 hours [12]. The fecal samples are held before testing in Cary-Blair transport medium. The system houses all the chemistry required to extract, amplify, and detect nucleic acid from multiple enteropathogens within a single fecal sample, which can either be held at room temperature at 15°C–25°C or refrigerated at 2°C–8°C, in both cases for up to 4 days. FilmArray software automatically analyzes and interprets the assay results, displaying them qualitatively in a test report [11].
The Seegene Allplex (Seegene) platform is a multiplex 1-step real-time -PCR platform with viral, parasitic, and 2 bacterial assays [13]. These assays allow simultaneous detection of up to 7 enteropathogens within a single reaction tube using a specific detection algorithm, enabling a total of 25 pathogens to be tested across the panel. It is based on multiple genetic quantification by RT-PCR and specific interpretation software, with the panels running in either a combined or a selected manner [13]. The Seegene platform has a run time of <2 hours 30 minutes in a single reaction and has good concordance with other multiplex molecular assays [13–15], including a user-friendly workflow that displays test results as individual cycle threshold (Ct) values of multiple analytes in a single channel on the RT-PCR instrument [16].
Compared with conventional techniques, syndromic testing with platforms such as the Seegene has been described not only as improving and accelerating microbiological diagnosis but also as efficient and cost-effective for patient care [13, 17]. However, in some cases enteropathogens detected may be of uncertain clinical significance, meaning that test results need careful interpretation [10]. Although widespread use of the Seegene platform has led to a paradigm shift in the diagnosis of TD and other infectious diseases in clinical microbiology settings [17], it is less suitable for field diagnostics as it is designed for laboratory use. However, it remains a good comparator to evaluate the performance of the FilmArray platform in TD diagnostics, and it targets more enteropathogens than the FilmArray **(**Supplementary Data Sheets 1 and 2).
Knowledge about the suitability of the FilmArray platform for accurately identifying the causes of TD in forward deployment locations is currently limited. We evaluated the (1) sensitivity and specificity, (2) agreement, and (3) interrater agreement between FilmArray PCR as an NP-FE test and the Seegene platform as the reference standard test for TD diagnostics in resource-limited settings.
METHODS
Study Design and Specimen Collection
Fresh fecal samples from British military personnel who experienced diarrhea during a Cryptosporidium outbreak described elsewhere were analyzed using the FilmArray PCR platform as a clinical NP-FE test [6]. Individuals self-collected loose and semisolid stool samples in 500-mL snap-on lid specimen collection pots, before transferring approximately 10-mL stool volumes into 30-mL sterile bottles. Due to resource and time constraints, we selected 60 of 124 samples comprising a mixture of negative samples and single-, dual-, and multiple-enteropathogen samples as detected by FilmArray PCR for comparison with the Seegene platform as the reference standard test. One corresponding Seegene test was invalid and excluded from the analysis. We used quota sampling to select a varied pool of samples, as described elsewhere [18]: negative samples, 5 of 60 (8.3%); single enteropathogen, 19 of 60 (31.7%); 2 enteropathogens, 20 of 60 (33.4%); and multiple enteropathogens, 16 of 60 (26.7%). Corresponding samples from the selection were anonymized, marked with unique identifiers, and aliquoted into 2-mL cryovials without preservative before storage at −80°C. They were then repatriated to the United Kingdom in dry ice at −50°C to −85°C and kept frozen at −80°C before subsequent Seegene testing 16–18 months later (Figure 1) by investigators blinded to the FilmArray test results. We calculated sensitivity and specificity, the overall detection rate (ODR) as TP/(TP + FP), where TP and FP represent true-positive and false-positive, and the percentage observed agreement as TP + TN/(TP + FN + FP + TN) × 100, where TN and FN represent true-negative and false-negative.
Near-patient field-expedient (NP-FE) and reference standard processing steps. Fecal samples were tested near the point of care for immediate case management, and corresponding samples were repatriated in the cold chain for later comparative testing in the United Kingdom. Abbreviation: PCR, polymerase chain reaction.
Statistical Analysis and Ethics
The Ministry of Defence Research Ethics Committee ethical approval (no. 2076/MODREC/21) was granted in 2021, and all participants provided informed written consent. Cohen κ statistical coefficients (Microsoft Excel, version 2401) were used to measure the interrater agreement and degree of accuracy between tests using the following formula: κ = (po − pe)/(1 − pe), where po represents the relative observed agreement among raters and pe, the expected hypothetical probability of chance agreement.
Rationale for Reference Standard Test Choice
In the absence of a known reference or gold standard multiplex PCR platform for GI molecular diagnostics, we selected the Seegene platform as the reference standard test. It has reliable detection capability, good concordance with other multiplex PCRs (depending on the target enteropathogens), including when compared with the FilmArray platform [19], and superior sensitivity of 89%–100%, particularly for common bacterial targets compared with traditional reference standards, including culture and sensitivity [13]. Its ability to detect multiple pathogens in a single channel with individual Ct values and a rapid turnaround provides a degree of objectivity in the quantitative detail that is missing in other platforms like the FilmArray [20] (Supplementary Data Sheets 1 and 2). The FilmArray platform is preprogrammed to generate results qualitatively, whereas the Seegene platform produces both a qualitative summary and quantitative analysis of results. This can inform clinical decisions on whether enteropathogens are commensal or pathogenic, confirming this platform as a suitable comparator.
FilmArray PCR Testing
Individual FilmArray pouches for each respective sample were placed into the loading block, and the hydration solution was injected into the pouch through the blue inlet port. For each respective sample, approximately 200 µL of stool was added into the sample buffer, and the solution was mixed then injected into the pouch through the red inlet port. Next, the FilmArray pouch was loaded into the instrument, and the pouch identification number scanned using the barcode reader. Finally, the unique respective sample identifiers were entered, and the automated run was started. The test completes with the software assigning test results qualitatively for each of 22 GI enteropathogens, then producing a test report (bioMérieux) (Supplementary Data Sheet 3).
PCR Testing by Seegene Allplex GI Panel
Nucleic acids were extracted from stool samples using the QIAamp 96 PowerFecal QIAcube HT Kit on a QIAcube HT platform, following the manufacturer's instructions. Initial homogenization of the stool samples was conducted on the QIAcube HT platform. Briefly, 200 mg of each stool sample was placed into a well of a PowerBead Pro plate containing preloaded ceramic beads, and 650 µL of prewarmed PW1 buffer was added. The plate was vortexed continuously for 10 minutes and then centrifuged to pellet the debris (Qiagen). (Supplementary Data Sheet 4).
PCR assays were analyzed on a CFX96 (BioRad) platform, and the results were interpreted using Seegene Viewer software, which automatically interprets positivity and produces a test report, including Ct values (Mast Group, UK).
RESULTS
FilmArray Versus Seegene ODRs
Samples from 60 of 124 individuals (48.4%; 80% male; median age [interquartile range], 24 [22–28] years) tested with FilmArray PCR were selected for the study and compared with corresponding samples tested with Seegene PCR, apart from 1 invalid Seegene test that was excluded from the analysis. The ODRs of all enteropathogens were comparable between the FilmArray and Seegene platforms (55 of 60 [91.7%] vs 53 of 59 [89.8%], respectively; P > .93). Both platforms detected more bacterial than protozoal or viral enteropathogens, and the ODRs for bacteria were comparable between FilmArray (42 of 60; [70%]) and Seegene (41 of 59 [69.5%]; P < .05). The FilmArray platform detected fewer viral enteropathogens than the Seegene (in 6 of 60 samples [10%] vs 20 of 59 [33.9%], respectively; P < .02) and fewer protozoal enteropathogens (27 of 60 samples [45%] vs 33 of 59 [55.9%]; P < .05). Three of 5 samples negative with FilmArray PCR were positive with Seegene (2 for multiple enteropathogens and 1 for Dientameba fragilis). D fragilis and Blastocystis hominis are not included in the FilmArray panel but were present in 8 of 59 (13.6%) and 30 of 59 (50.8%) Seegene tests, respectively. The FilmArray platform also detected 1 each of Salmonella spp and Entameba histolytica, while none of either were detected with the Seegene platform.
The Seegene platform detected more Clostridioides difficile and norovirus than the FilmArray (in 6 vs 2 samples and 14 vs 1, respectively). Similarly, the detection rate for Campylobacter spp was significantly higher with Seegene than with FilmArray PCR (6 of 60 [10%] vs 17 of 59 [28.8%]; P = .03). Norovirus and rotavirus were almost always detected in combination in the multiple-enteropathogen samples with Seegene testing. There were only 6 exact matches by the 2 platforms, and 25 of 60 samples (41.7%) were Cryptosporidium spp positive. Of these 25 samples, 20 (80%) were also positive with Seegene PCR, but in combination with multiple other enteropathogens in most samples. The Seegene platform detected multiple pathogens in 32 of 59 samples tested (54%). Overall, diarrheagenic Escherichia coli (DEC) strains were more common than any of the other enteropathogens detected by the individual platforms (55 of 95 [57.9%] for FilmArray vs 62 of 134 [46.3%] for Seegene). DEC detection was comparable between the 2 platforms (P = .33) (Tables 1 and 2).
Comparison of Sensitivity, Specificity, and Interrater Agreement Between Tests
Sensitivity ranged from noncomputable for 2 enteropathogens up to 100%, and specificity ranged from 74% to 100%. The FilmArray platform was highly sensitive (100% [95% confidence interval, 2.50%–100%]) and specific (100% [93.84%–100%]) when compared against the reference standard Seegene test, with an almost perfect agreement (percentage observed agreement, 100%; κ = 1) for Giardia duodenalis. The sensitivity was low for Campylobacter spp (35.3% [95% confidence interval, 14.21%–61.67%]). This trend toward low sensitivity and high specificity was similar for Cryptosporidium spp and other DEC strains. DEC strains were not found to be of major clinical significance, and supportive management and/or isolation were offered as required [6]. Although highly specific for Salmonella and E histolytica, sensitivity and agreement were not computable for these enteropathogens. The agreement between tests was moderate for Cryptosporidium spp, enteroaggregative E coli (EAEC), Campylobacter spp, and sapovirus. Contrastingly, the agreement between the 2 PCR platforms ranged from none to slight (κ = 0.01–0.20) for E coli O157 and norovirus (Table 3).
DISCUSSION
This study demonstrates moderate concordance between the NP-FE FilmArray and reference standard Seegene when testing for 5 GI enteropathogens. Concordance was poor to fair for 7 other enteropathogens. FilmArray PCR proved to be highly adaptable as an NP-FE test in a resource-limited environment, and we were able to confirm this by omitting the fecal preservation by Cary Blair medium step. Corresponding samples repatriated in the cold chain had also been stored without Cary Blair preservative before later testing with Seegene PCR. There was no notable impact on the positivity rate, and we found the FilmArray platform to measure comparably in this regard against the selected reference standard Seegene platform, which is already in wide use in clinical microbiological settings as a tool for diarrhea diagnostics [17]. This confirms the versatility of the FilmArray as a suitable platform for use in resource-limited settings, including military deployments and similar environments with challenging logistic chains.
Some previous work challenges the widespread use of multiplex approaches like the FilmArray platform for TD diagnostics, given that in their case only a few enteropathogens (DEC strains) were related to symptoms of TD [19]. Based on our group’s previous experience in close-knit resource-limited settings, as reported elsewhere [6], we would argue that such platforms with a rapid turnaround are crucial for disease containment, particularly in outbreak scenarios. The comprehensive profile of enteropathogens is necessary for accurate epidemiological surveillance, enforcement of force health protection measures, and wider public health measures to support antimicrobial stewardship efforts. All this is critical for maintenance of military operational effectiveness.
Comparison of Enteropathogen Target Detection
Our data show high specificity for Campylobacter spp, Cryptosporidium spp, and EAEC of between 84.4% and 100% when the FilmArray platform was compared against the reference standard Seegene. The significant mismatch in detection rates of Campylobacter spp for Seegene versus FilmArray PCR (P = .03) may be attributed to the diversity and discrepancies in species coverage within the Campylobacter genus [21, 22]. To confirm this, we would need to analyze data held by manufacturers, but to our understanding such data are internal and not for publication. Only 2 positives each were detected by the FilmArray platform for C difficile and sapovirus and 1 each of E coli O157, E histolytica, Giardia duodenalis, norovirus, and Salmonella spp, which are relatively low ODRs to make any meaningful conclusions on concordance.
Interrater agreement for enteropathogenic E coli and Shiga toxin–producing E coli was fair due to a relatively high number of FPs for both enteropathogens (Supplementary Table 1). Although the agreement between platforms for sapovirus was also moderate, and substantial for Giardia duodenalis (sensitivity and specificity both 100%), the low ODRs and subsequently the number of TPs also make it impractical to conclusively evaluate concordance. There were no TPs for Salmonella spp or E histolytica in the NP-FE. Contrastingly, although there were also no TPs for E coli O157, there was 1 FP and, as a result, a high percentage observed agreement (>96%), even though there was no agreement between the 2 platforms for this particular target.
Analysis of Differences Between Platforms
The high ODR we found for DEC is consistent with previous findings [23], as is the good concordance between platforms in the comparison of bacterial targets in general [19, 24]. One significant discrepancy between the 2 platforms was a 14 times greater detection rate of norovirus for the Seegene platform, for which there are several possible reasons. We postulate that FilmArray platform may have been less sensitive for this particular enteropathogen target. Alternatively, the substantial increase in norovirus detection may represent variations in effects of individual platform chemistry on different molecular targets or differences between the nucleic acid extraction, reverse-transcription/amplification processes or indeed the high prevalence and genetic diversity of norovirus. This viral assay distinguishes between norovirus genotypes 1 and 2, while the FilmArray makes no distinction between those genotypes. The Ct values were generally <32 (data not shown) and therefore fairly strong positives, which would rule out a hypothesis of FPs.
Without further sequencing work, we are unable to confirm the possibility of mutations in the assay sites, or whether there are genetic variations in norovirus lineages circulating in rural Kenya, where the study participants initially presented with TD. It is unlikely that the norovirus detections were clinically relevant; the clinical features of the cases were not typical of norovirus infection at the time of the outbreak [6], suggesting the possibility of overdetection by the Seegene platform. D fragilis and B hominis were detected in 13.3% and 50% of Seegene samples, respectively. Although both protozoal parasites are endemic in some parts of the world and are included in some fecal PCR assays, positive results for D fragilis usually indicate the presence of colonizing flora. There is no consensus regarding clinical significance of D fragilis [25] because of the comparable frequency of occurrence in patients with GI symptoms and healthy cohorts alike [26]. However, some studies have shown correlation between infection and GI symptoms [27]. In contrast, evidence overwhelmingly points to Blastocystis being a commensal [28]. FilmArray PCR does not detect Aeromonas spp, B hominis, or D fragilis, but all 3 are detectable with Seegene assays. We were therefore unable to consider these enteropathogens in our comparison of agreement and interrater agreement between the 2 platforms.
FilmArray Performance Characteristics and Suitability for Resource-Limited Settings
FilmArray operation does not require the operator to have enhanced training in molecular diagnostic techniques. DNA extraction from clinical samples for molecular analysis is difficult to perform in resource-limited settings due to cost, time, limitations in resources, the risk of contamination, and in some cases lack of relevant expertise [29, 30]. Other advantages of the FilmArray platform include minimal hands-on processing time, rapid turnaround time, platform robustness, and versatility. Some studies have reported high sensitivity and specificity for several GI targets but noted some exceptions [17]. Despite the low concordance of FilmArray testing for the majority of enteropathogens, it remains one of a limited number of closed extraction multiplex platforms on the market suitable as an NP-FE diagnostic tool in resource-limited settings; an additional advantage of this syndromic platform is the compatibility that allows other infectious disease assays to be used within the same platform.
Study Limitations
Because we were not able to include case controls in this study due to the cost and time constraints alluded to earlier, the attributable fraction could not be evaluated. Our quota sampling may have introduced selection bias, including the possibility of preselecting FP-testing samples. The possibility of reference standard bias must also be considered as the performance characteristics of the Seegene platform may have skewed the perceived accuracy of the FilmArray platform, and we did not compare these multiplex platforms with classic culture-based microbiological analyses. There was 1 sample each with E coli O157, E histolytica, Giardia duodenalis, norovirus, and Salmonella spp, all detected with the FilmArray platform. These smaller individual enteropathogen numbers, as shown in Table 2, may mean that our study was underpowered by the low number of samples, which could have lowered the probability of producing true effects because of the higher chance of type I or II errors (FPs or FNs) [31, 32]. This could likely have produced the skewed findings reported for some enteropathogens (Table 3).
Samples were also analyzed with Seegene PCR 16–18 months after the initial Film Array analysis, with an additional repatriation step from Kenya to the United Kingdom. Although the samples were transported on dry ice and subsequently stored at −80°C, ideally samples from the same aliquots should have been tested across the 2 platforms at the same time points. Likewise, it is not possible to deduce whether or not fecal DNA recovery was impacted due to differing storage and testing steps for both platforms. Data on optimum storage duration of fecal samples over prolonged periods, including quality assurance details on the stability of nucleic acids, are inconsistent [13, 14, 17].
This limitation may account for discrepancies in sensitivity, including overall concordance, and future studies should attempt to address this. Finally, in multinational deployments, complications resulting from lack of standardization may arise from varied standard operating procedures. In our experience, a diagnostic test can only be marked Conformité Européenne if the entire workflow from extraction to amplification follows the manufacturer's validated instructions. As far as we are aware, clearance of the Seegene assays for in vitro diagnostic use does not cover nucleic acid extraction with the Qiagen columns. We have already highlighted that this approach likely increased sensitivity for some enteropathogens compared with the nucleic acid extraction schemes covered by the in vitro diagnostic clearance of other available commercial products. Such diverse approaches further complicate collaboration between countries that may follow different regulations.
Study Strengths
Although the 5 negative samples tested near the point-of care were not true case controls, they were used in addition to ≥10 more samples collected from asymptomatic individuals as quality controls that were run after a predetermined number of FilmArray testing cycles to rule out the risk of cross contamination. We used corresponding samples from a homogenous group within the same resource-limited setting, thereby ruling out the risk of introducing geographic confounders.
Suggested Future Studies
Expert consensus guidelines should include recommendations for a suitable reference standard multiplex PCR platform for TD diagnostics in resource-limited settings. For qualitative syndromic platforms such as the FilmArray, evidence from case-control studies with larger sample sizes using a combination of clinical and epidemiological data, qualitative as well as quantitative PCR results, including traditional culture-based test outcomes, should be used to help in formulating guidelines for the interpretation of test results to inform treatment decisions and force health protection measures. This is vital for optimizing TD diagnostics and treatment. Such data may also be useful in informing guidelines on distinguishing between commensality or pathogenicity, particularly where multiple enteropathogens are detected. Such a strategy could affect outcomes, including underperformance resulting from morbidity, as well as duty days lost due to bedding down and inappropriate antibiotic use, all which have an overall impact on operational effectiveness.
Conclusions
Our findings show moderate concordance of FilmArray with Seegene PCR testing in the detection of Campylobacter spp, Cryptosporidium spp, EAEC, and sapovirus and poor to fair concordance for 9 other enteropathogens. It was impractical to conclusively evaluate concordance and interrater agreement for some enteropathogens due to low ODRs for the NP-FE test, which led to unreliable results. FilmArray test guidelines require refinement due to the test’s inherent limitations, such as low sensitivity for some key enteropathogens. Future interpretation of results to inform clinical practice should be based on robust evidence from large-scale studies, integrating clinical, qualitative, quantitative, and traditional culture data. Despite these shortcomings and in the absence of a reference standard platform, the performance characteristics of FilmArray PCR demonstrated its continued suitability as an NP-FE platform for diarrhea diagnostics in resource-limited settings.
Supplementary Material
ofag076_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Boatwright MA, Kuo HC, Lindholm DA, et al The impact of infectious disease syndromes on activities during military travel. Open Forum Infect Dis 2023; 10:ofad 461.37771853 10.1093/ofid/ofad 461PMC 10533202 · doi ↗ · pubmed ↗
- 2Toriro R, Tabberer B, Davis SI, et al Epidemiology and impact of travellers’ diarrhoea differs during UK military training exercises in Kenya and Oman. BMJ Mil Health 2025: 1–6. doi:10.1136/military-2024-002913.PMC 1301873639863290 · doi ↗ · pubmed ↗
- 3Riddle MS, Connor BA, Beeching NJ, et al Guidelines for the prevention and treatment of travelers’ diarrhea: a graded expert panel report. J Travel Med 2017; 24:S 63–80.10.1093/jtm/tax 026PMC 573144828521004 · doi ↗ · pubmed ↗
- 4Biswas JS, Lentaigne J, Hill NE, et al Epidemiology and etiology of diarrhea in UK military personnel serving on the United Nations mission in South Sudan in 2017: a prospective cohort study. Travel Med Infect Dis 2019; 28:34–40.30553046 10.1016/j.tmaid.2018.12.004 · doi ↗ · pubmed ↗
- 5Bailey MS, Boos CJ, Vautier G, et al Gastroenteritis outbreak in British troops, Iraq. Emerg Infect Dis 2005; 11:1625–8.16318711 10.3201/eid 1110.050298 PMC 3366745 · doi ↗ · pubmed ↗
- 6Toriro R, Pallett SJC, Woolley SD, et al Outbreak of diarrhoea caused by a novel Cryptosporidium hominis subtype during British military training in Kenya. Open Forum Infect Dis 2024; 11:ofae 001.38250201 10.1093/ofid/ofae 001PMC 10798851 · doi ↗ · pubmed ↗
- 7Libman M . Summary of the committee to advise on tropical medicine and travel (CATMAT) statement on travellers’ diarrhea. Can Commun Dis Rep 2015; 41:272–84.29769922 10.14745/ccdr.v 41i 11a 03PMC 5864280 · doi ↗ · pubmed ↗
- 8Frickmann H, Hagen RM, Geiselbrechtinger F, Hoysal N. Infectious diseases during the European union training mission Mali (EUTM MLI)—a four-year experience. Mil Med Res 2018; 5:19.29848381 10.1186/s 40779-018-0166-5PMC 5977544 · doi ↗ · pubmed ↗