Return to work after myocardial infarction: A systematic review
Tais Santana Barbosa, Natasha Cordeiro dos Santos, Millena Pereira Costa, Roque Aras Junior

TL;DR
This paper reviews how people return to work after a heart attack, finding that most return within a year but face challenges like reduced income and mental health issues.
Contribution
The study provides consolidated evidence on return-to-work rates and factors influencing them after myocardial infarction.
Findings
Return to work rates range from 21.5% to 41.7% after one month and 76.9% to 92.7% after one year.
Work modifications, salary reductions, job dismissals, and mental health issues are reported post-myocardial infarction.
Return to work is influenced by physical, psychological, and social factors.
Abstract
The majority of people experiencing Myocardial Infarction are of working age, which may result in prolonged work disability. This study seeks to consolidate the available evidence regarding the return to work for individuals following a Myocardial Infarction, while also examining its correlation with disease severity, job engagement, and duration of hospitalization. This research is a systematic review. The databases utilized include MEDLINE, Lilacs, Scielo, and Web of Science, with keywords and synonyms sourced from the Health Sciences Descriptors (DeCS), Medical Subject Headings (MeSH), and Embase Subject Headings (Emtree). Data collection took place between November 2023 and June 2024. The studies’ quality was evaluated using the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. The search yielded 4,695 articles, from which 12 cohort studies were selected…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
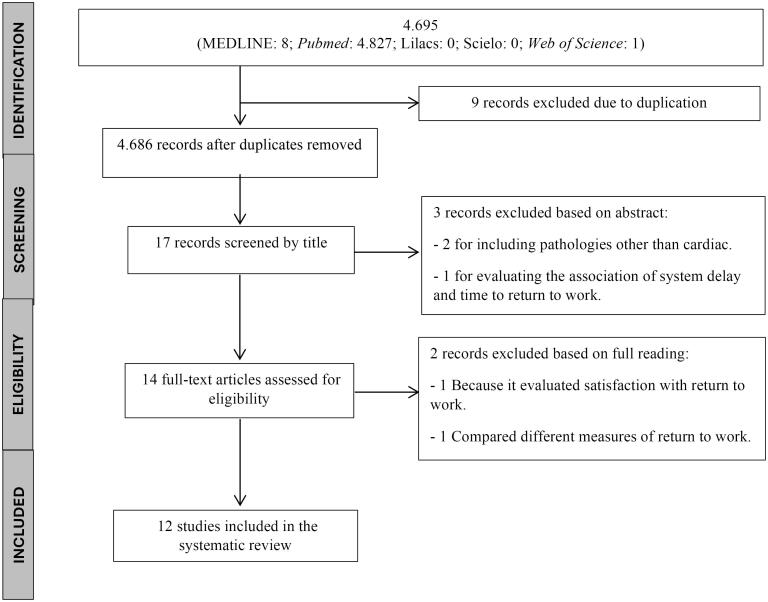 Figure 1
Figure 1|
|
| |
| DECS | Myocardial Infarction | Myocardial Infarct, Myocardial Infarctions, Myocardial Infarcts |
| Return to Work | Back to Work, Back-to-Work, Return-to-Work | |
| Cohort Study | Cohort Analysis | |
| MESH | Myocardial Infarction | Myocardial Infarctions, Myocardial Infarctions, Myocardial Infarcts |
| Return to Work | Back to Work | |
| Cohort Study | Cohort Studies | |
| EMTREE | Myocardial Infarction | Myocardial Infarctions, Myocardial Infarctions |
| Return to Work | Back to Work | |
| Cohort Study | Cohort Studies |
|
|
|
|
|
|
|
|---|---|---|---|---|---|
| Sun et al, 2022 | Longitudinal prospective cohort study. | South Korea | STEMI | - Total of 136 participants; | - Received a diagnosis of myocardial infarction (MI) from a cardiologist; |
| Stendardo et al, 2018 | Prospective cohort study. | Italy | NSTEMI 64 (62,75%). | - A total of 102 patients were included in the study. | - Diagnosis of myocardial infarction based on the criteria established by the European Cardiac Society; |
| Jiang et al, 2018 | Prospective cohort study. | China | - STEMI 103 (6,6%) patients; | - A total of 1,566 patients participated from 53 hospitals. | - Individuals who indicated they were working (either part-time or full-time) during their hospitalization for a myocardial infarction (MI), consented to participate in follow-up interviews, were discharged in stable condition, did not transfer to another intensive care facility, and successfully completed the 12-month interview. |
| Butt et al, 2018 | Prospective cohort study. | Denmark | Not specified | - 6,031 Individuals | - Identified all Danish individuals who underwent their initial isolated coronary artery bypass grafting (CABG). |
| Warraich et al, 2018 | Longitudinal observational study. | United States | STEMI | - Total Participants: 9,319 | - Patients were eligible for inclusion in the registry if they were 18 years of age or older, diagnosed with either STEMI or NSTEMI, received treatment via PCI along with a P2Y12 inhibitor, were not participating in any other research studies, and could provide written consent for ongoing telephone follow-up and data gathering. |
| Babić et al, 2015 | Prospective, single-center, open study. | Croatia | STEMI | - The average age of the 145 patients examined was 53.17 years, with a standard deviation of ± 7.29. | - Participants were required to be under the age of 60 and currently employed. |
| Osler et al, 2014 | Cohort study. | Denmark | Most people who RTW had unstable angina (55.1%), 5,773 had STEMI, 4,136 NSTEMI, and 6,542 unspecified MI. | - 21,926 Participants | - The National Patient Registry classified all initial hospitalizations for Acute Coronary Syndrome (ACS) as unstable angina, ST-Elevation Myocardial Infarction (STEMI), Non-ST-Elevation Myocardial Infarction (NSTEMI), and myocardial infarction (MI). |
| de Jonge et al, 2014 | Prospective cohort study | Netherlands | Unspecified | - Total Participants: 186 | - To qualify, patients needed to satisfy a minimum of two criteria: (1) experiencing chest pain for at least 20 minutes, (2) having elevated levels of enzymes such as creatine phosphokinase and creatine phosphokinase-MB, and (3) demonstrating new pathological Q waves on the electrocardiogram across at least two leads. |
| Worcester et al, 2014 | Prospective, longitudinal, observational cohort study | Australia | Unspecified | - 401 Patients | - The criteria for inclusion consisted of being employed within two months following hospital admission and being 75 years old or younger. |
| Lauridsen et al, 2022 | Danish national cohort study. | Denmark | STEMI with CS | - Total participants: 19,799, comprising 19,146 individuals without CS and 653 with CS (3%); | - Individuals were identified through the Danish National Patient Register, specifically those with their initial hospitalization due to STEMI. The diagnosis of CS was established either through a corresponding diagnosis code for CS or by any administration of vasoactive medications during the myocardial infarction hospitalization. |
| Smedegaard et al, 2017 | Nationwide retrospective cohort study. | Denmark | Not specified | - Among the patients, 22,394 individuals (56.9%) were employed prior to their first myocardial infarction (MI). | - Individuals between the ages of 30 and 65 who received a diagnosis of myocardial infarction (MI) upon their initial primary discharge were considered for inclusion. |
| Mohd Mustafah et al, 2017 | Retrospective cohort study. | Malaysia | 46 (63.9%) had STEMI and 18 (25.0%) NSTEMI among RTW. | - 112 Individuals | - All participants were patients in rehabilitation following a cardiac incident (myocardial infarction, percutaneous coronary intervention, or coronary artery bypass grafting) and were currently on medical leave. |
|
|
|
|
|
|---|---|---|---|
| Sun et al,2022 | - The percentage of myocardial infarction patients in South Korea who resumed work three months post-discharge. | - Of the 136 participants, 56 individuals (41.2%) were employed at the time of their myocardial infarction (MI), while 80 individuals (58.8%) were not in employment. At the three-month follow-up, 87.5% (n = 49) of those who had jobs at the beginning of the study successfully returned to work. | The primary findings of this research indicate that most employed patients who undergo a myocardial infarction (MI) are capable of resuming their professional duties within three months following their discharge. |
| Stendardo et al, 2018 | - Examine the influence of physical, psychological, sociodemographic, and occupational variables on the likelihood of returning to work within one year following a myocardial infarction (MI) in a uniform group of patients who have undergone coronary angioplasty and did not experience a postoperative MI. | - At the one-month follow-up appointment, 60 individuals (59.80%) indicated they had not experienced any cardiac symptoms since being discharged. The estimated median MET values reflecting patient exercise capacity were calculated at 6.03 (IQR 5.50–6.53). Scores from both HADS questionnaires measuring anxiety and depression, along with spirometric parameters (FEV1, FVC, and FEV1/FVC), fell within normal reference ranges. | The most significant factors influencing a return to work within one year following discharge from a myocardial infarction treated with percutaneous coronary intervention include being self-employed, possessing a higher level of education, and maintaining a positive emotional state. |
| Jiang et al, 2018 | - Return to work refers to resuming either full-time or part-time employment within a 12-month period following discharge from the initial hospitalization due to myocardial infarction (MI). | - A total of 875 patients (55.9%) resumed work within 12 months following hospitalization for a myocardial infarction (MI). Among the 691 patients who did not return to work, 287 (41.5%) were either unable or opted not to work due to their MI, 131 (19.0%) retired early as a result of the condition, 44 (6.4%) became full-time homemakers or were unemployed, while 229 (33.1%) did not provide a reason for their absence from the workforce. | Among employed individuals hospitalized due to myocardial infarction (MI) in China, almost 50% did not resume their jobs within a year. Factors such as being female, having a history of smoking, and experiencing negative incidents during hospitalization were associated with a decreased likelihood of returning to work post-MI. |
| Butt et al, 2018 | - The main objective was to assess the return to employment, which was anticipated to occur within a timeframe ranging from 5 weeks to one year following coronary artery bypass grafting (CABG). | - One year post-discharge, 4,827 patients (80.0%) re-entered the workforce, while 614 patients (10.2%) were on paid medical leave. Additionally, 63 patients (1.0%) required support due to diminished work capacity, 204 patients (3.4%) received disability pensions, 250 patients (4.1%) opted for early retirement, 57 patients (0.9%) had passed away, and 16 patients (0.3%) had emigrated. | Working-age individuals who were employed in the month preceding their coronary artery bypass graft (CABG) surgery demonstrated a notable trend in workforce reintegration. A year following their discharge, approximately 80% of these patients successfully resumed their professional roles, accompanied by a low mortality rate. |
| Warraich et al, 2018 | - Examination of the occurrence of negative employment shifts from baseline to one year following myocardial infarction in a national cohort study conducted in the United States. | - Among patients who were employed at the start of the study, 10% (n = 492) experienced a negative shift in their employment status one year later. Of these, 7% (n = 349) reported being unemployed, while 3% (n = 143) indicated they were working fewer hours. Only 27 individuals who faced an adverse employment change cited retirement as the reason; notably, 172 patients (representing 49% of those who became unemployed) reported losing their jobs involuntarily due to circumstances such as termination or health-related issues. | Patients facing unfavorable changes in their employment status are more susceptible to depression, experience a diminished quality of life, and encounter increased financial burdens related to medication expenses when compared to those who remain employed. The most significant predictors of adverse employment shifts are unanticipated readmissions and bleeding events following a myocardial infarction, highlighting the critical need to mitigate the occurrence of these negative outcomes. |
| Babić et al, 2015 | - Examine various factors related to returning to work, socioeconomic issues, and overall quality of life among 145 employed patients under the age of 60 who have experienced STEMI and received treatment through primary PCI. | - The average duration of sick leave following a STEMI event was 125.83 days, with a standard deviation of 125.04 days. | Individualized cardiac rehabilitation must be prioritized and organized by the assigned team right after the acute phase of a myocardial infarction (MI). Insufficient health policies and delays in initiating cardiac rehabilitation post-MI can result in extended hospital stays, increased sick leave, and a diminished quality of life following the event, even when optimal treatment is administered during the acute stage of the condition. |
| Osler et al, 2014 | - To investigate how factors such as patient gender, comorbidity, and socioeconomic status influence later labor market participation (including categories like employed, unemployed, on sick leave, and those opting for disability or voluntary early retirement) within a group of working patients in Denmark. | - Among the 21,926 patients studied, 37% were employed 30 days post their initial admission for an Acute Coronary Syndrome (ACS) diagnosis. In contrast, 55% were on medical leave, and 8% were unemployed. | More than 50% of patients experiencing their first acute coronary syndrome (ACS) event either stay at work or return shortly afterward. However, certain groups—including women, those from socially disadvantaged backgrounds, individuals facing more severe cardiac incidents, and those with additional health conditions—exhibit lower rates of returning to work when other clinical variables are taken into consideration. It is essential to factor in these aspects during both physical recovery and social rehabilitation. |
| de Jonge et al, 2014 | - We analyzed the impact of depressive and anxiety disorders, identified through a diagnostic interview, on the rates of returning to work one year following a myocardial infarction (MI). | - After three months post-myocardial infarction (MI), 86 patients, accounting for 46.2%, resumed work, while 100 did not. | The occurrence of a depressive episode was linked to a heightened risk of not resuming work among patients with myocardial infarction (MI). The relationship between anxiety and the likelihood of failing to return to work may, in some respects, be attributed to the co-occurrence of depression. Future research could explore the potential for mitigating the impact of depression through appropriate therapeutic interventions. |
| Worcester et al, 2014 | - To examine the employment re-entry rate within the first year following ACS or CABG procedures. | - RTW data were collected for a total of 378 patients. Among these, 343 individuals (90.7%) successfully returned to work, with 309 of them (91.1%) doing so within a four-month period. Conversely, 35 patients (9.3%) did not return to their jobs. At the one-year mark, 302 patients (79.9%) remained employed, while 32 (8.5%) were unemployed and 20 (5.3%) had retired. | A substantial percentage of individuals who were employed prior to experiencing an acute cardiac incident tend to resume their jobs within a year. The inability to validate predictors of work return identified in previous studies can be attributed, in part, to the exceptionally high rate of employment reinstatement observed in our research, which took place during a period of low unemployment. Nonetheless, there exists a small yet notable group of patients who either did not go back to work, exited the workforce prematurely after initially returning, or were subsequently lost to follow-up. |
| Lauridsen et al, 2022 | - The relationship between myocardial infarction (MI) and chronic stress (CS) in the context of returning to work, job retention, and the various factors influencing this return. | - Among patients without cardiac surgery (CS), 83% were able to return to work within one year. Conversely, only 52% of patients who underwent CS managed to resume work. | Approximately 80% of individuals without cardiac surgery (CS) resumed employment, whereas only 50% of those who underwent CS were back at work after one year. Nonetheless, once employed, both groups demonstrated comparable rates of secondary disengagement from work. For patients with CS, being male and surviving an out-of-hospital cardiac arrest (OHCA) were positively associated with a return to work, while extended hospital stays and anoxic brain injuries negatively impacted this outcome. |
| Smedegaard et al, 2017 | - Resuming employment within one year following the initial hospitalization for a myocardial infarction and the cessation of work after re-entering the workforce. | - Within a month following myocardial infarction (MI), 9,329 patients (41.7% [95% CI, 41.0%–42.3%]) resumed work. This figure rose significantly to 20,415 individuals (91.1% [95% CI, 90.7%–91.5%]) after one year, while there were 92 reported fatalities (0.4% [95% CI, 0.3%–0.5%]). When assessing employment after three months, the number of patients who returned to work totaled 19,369 (86.4% [95% CI, 86.0%–86.9%]). | 91% of individuals resumed employment; however, within the following year, 24% of these patients lost their jobs, reflecting a detachment rate three times greater than that of the general population. Key factors influencing this employment loss included being younger (ages 30-39) and having a lower socioeconomic status. |
| Mohd Mustafah et al, 2017 | - Assess the frequency of individuals returning to work, along with their sociodemographic traits, medical conditions, and overall quality of life. | - There were 74 participants who returned to work and 38 who did not. | Increasing age, involvement of multiple vessels, and the presence of diabetes mellitus (DM) were identified as adverse predictors for returning to work. Conversely, a higher Mental Component Summary (MCS) score was associated with a greater likelihood of returning to work. In this study, psychological well-being emerged as the sole modifiable factor influencing the ability to return to employment. |
|
|
|
|
|
|
|---|---|---|---|---|
| Sun et al, 2022 | - 77.9% of participants had a history of myocardial infarction (MI). | No data | 3 months after hospital discharge | - Number per patient (34.6%, 32.4%, and 30.1%) one, none, and two, respectively |
| Stendardo et al, 2018 | - LVEF 50.22 ± 8.16 | Median length of stay was 4 (IQR 4–6) days | 1 and 2 months and 1 year after hospital discharge | - In 32.35% of study participants, MI was associated with other comorbidities, the most prevalent being: HTN (57%), DM (15%), and Depression (7%) |
| Jiang et al, 2018 | - 84 (5.4%) had LVEF < 40% | Length of stay, median (IQR), 11.0 (8.0-14.0) days | 1, 6, and 12 months after hospital discharge | - The five most common comorbid conditions identified in the population were: Hypertension (727 individuals, representing 46.4%), a history of Coronary Artery Disease (620 individuals, or 39.6%), Dyslipidemia (492 individuals, accounting for 31.4%), Heart Failure (345 individuals, which corresponds to 22.0%), and Type 2 Diabetes Mellitus (292 individuals, equating to 18.6%). |
| Butt et al, 2018 | - All patients underwent CABG | No data | 5 weeks to 1 year after CABG | - Most participants had a |
| Warraich et al, 2018 | - LVEF 51.4 (10.7) | Length of stay 2.9 days | 1 year after hospital discharge | - The predominant comorbid conditions identified were Heart Failure at 8.9%, Arrhythmia at 7.3%, Diabetes Mellitus at 9.3%, and Depression at 4.6%. |
| Babić et al, 2015 | - Anterior myocardial infarction was observed in 65 patients (44.8%), while inferior myocardial infarction occurred in 70 patients (48.3%). | The average length of stay was 11.84 ± 4.62 days | The time to return to work for those who considered their quality of life worse was 60 days, 25th-75th percentile (61.0 – 244), and for those who considered it the same, it was 43 days (61 – 122) | Most prevalent comorbidities: HTN 82 (56.6%), dyslipidemia 79 (54.5%), and DM 24 (16.6%) |
| Osler et al, 2014 | - 8,777 people underwent CAG and 6,257 PCI | No data | 30 days, 1 year, 2 years, and 5 years after ACS | 4,246 had 1-2 comorbidities |
| de Jonge et al, 2014 | - LVEF < 40% was observed in 12 patients (14.0%) at the 3-month mark and in 19 patients (14.3%) at the 12-month mark, both of whom returned to work (RTW). | No data | At 3 and 12 months after MI | The comorbid conditions observed in patients who resumed employment at 3 and 12 months post-treatment included dyslipidemia, hypertension (HTN), and diabetes mellitus (DM). |
| Worcester et al, 2014 | - The incidence of Killip class 2 or 3 among medical patients was recorded at 22 cases, representing 12.1%. | - Medical patients: Average length of stay is 5.05 days, with a standard deviation of 3.21. | Up to 12 months | DM 87 (22.6%) and other comorbidities 45 (11.6%) |
| Lauridsen et al, 2022 | - Majority of patients underwent CAG during hospitalization (CS: 93% vs. without CS: 90%) | 4 [2-16] days; without CS 4 [2-14] and with CS 13 [4-94] days | 1 year after hospital discharge | - Charlson Comorbidity Index: Frequent: 0 (78%), 1-2 (18%), and > 2 (5%) - HTN (20%), DM (8%), Cancer (3%), Cerebrovascular Disease (3%), Peripheral Vascular Disease (2%) |
| Smedegaard et al, 2017 | - 16,278 (72.7%) underwent CAG, followed by 55.3% PCI | No data | Within 1 month, 3 months, and 1 year after hospital discharge | - The most prevalent comorbidities were Heart Failure (8.9%), Arrhythmia (7.3%), DM (9.3%), and Depression (4.6%) |
| Mohd Mustafah et al, 2017 | - Among those who resumed employment, 36 individuals (48.6%) underwent coronary angiography (CAG) and 11 individuals (14.9%) received coronary artery bypass grafting (CABG). | No data | No data | - Of the participants who did not return to work, 33 (86.8%) had Dyslipidemia, 27 (71.1%) HTN, and 23 (60.5%) DM. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Sun et al, 2022 | Y | Y | Y | Y | N | NA | Y | N | Y | Y | Y | NA | Y | Y | Good |
| Stendardo et al, 2018 | Y | N | Y | NR | N | NA | Y | Y | Y | Y | Y | NA | Y | Y | Good |
| Jiang et al, 2018 | Y | Y | Y | Y | N | NA | Y | Y | Y | Y | Y | NA | Y | Y | Good |
| Butt et al, 2018 | Y | Y | Y | Y | N | NA | Y | Y | Y | Y | Y | NA | Y | Y | Good |
| Warraich et al, 2018 | Y | N | Y | NR | N | NA | Y | Y | Y | N | Y | NA | Y | Y | Good |
| Babić et al, 2015 | Y | Y | Y | Y | N | NA | Y | Y | Y | Y | Y | NA | Y | Y | Good |
| Osler et al, 2014 | Y | Y | Y | Y | N | NA | Y | Y | Y | Y | Y | NA | Y | Y | Good |
| de Jonge et al, 2014 | Y | Y | Y | Y | N | NA | Y | Y | Y | Y | Y | NA | Y | Y | Good |
| Worcester et al, 2014 | Y | N | Y | NR | N | NA | Y | Y | Y | Y | Y | NA | Y | Y | Good |
| Lauridsen et al, 2022 | Y | Y | Y | Y | N | NA | Y | Y | Y | N | Y | NA | Y | Y | Good |
| Smedegaard et al, 2017 | Y | Y | Y | Y | N | NA | Y | Y | Y | Y | Y | NA | Y | Y | Good |
| Mohd Mustafah et al, 2017 | Y | Y | Y | Y | N | NA | Y | Y | Y | NR | Y | NA | Y | Y | Good |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Health and Mental Health · Workplace Health and Well-being · Acute Myocardial Infarction Research
Introduction
According to the World Health Organization (WHO), Cardiovascular Disease (CVD) is responsible for approximately 17.9 million deaths each year, positioning it as the foremost cause of mortality globally by 2030.^1^ Among its various manifestations, Myocardial Infarction (MI) stands out as a significant contributor to both illness and death worldwide, including in Brazil.^2^ From January 2012 to December 2021, Brazil recorded a staggering 1,103,858 hospital admissions attributed to Myocardial Infarction.^3^
In this scenario, the demand for both clinical and surgical interventions, along with the complications arising from Myocardial Infarction and necessary lifestyle adjustments for patients, substantially influences their physical health, psychological well-being, financial stability, and social interactions. ^4^ It is recognized that beyond conventional outcomes such as mortality rates and readmission statistics, a crucial determinant of functional recovery and health-related quality of life (HRQoL) is the capacity to return to work. ^5^ Consequently, it becomes imperative to identify the facilitators and/or obstacles that may influence this return-to-work process.
It is important to highlight that a majority of individuals who experience Myocardial Infarction are typically of working age, which can result in prolonged work disabilities.^6^ Although the 2023 guidelines from the European Society of Cardiology (ESC) emphasize that maintaining or regaining employment constitutes a vital aspect of recovery post-Myocardial Infarction, ^7^ medical professionals frequently prescribe sick leave as part of rehabilitation strategies for these patients. ^8^
Within this framework, those patients who do not resume work within six months following a Myocardial Infarction are statistically less likely to achieve reintegration into the workforce in subsequent years. ^9^ Therefore, collating information on the return-to-work experiences of Myocardial Infarction patients—alongside its correlation with disease severity, occupational roles, and duration of hospitalization—can aid in formulating tailored interventions for these individuals while simultaneously mitigating healthcare expenditures. This study aims to consolidate existing research regarding the return-to-work dynamics for individuals recovering from Myocardial Infarction and explore its association with disease severity, job engagement, and length of hospital stay.
Methods
This systematic review was carried out following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines established by Moher et al.^10^ The research utilized several databases, including MEDLINE (Medical Literature Analysis and Retrieval System Online), Lilacs (Latin American and Caribbean Health Sciences Literature), SciELO (Scientific Electronic Library Online), and Web of Science. Data collection occurred between November 2023 and June 2024.
The study was designed using the PICOS framework, which stands for Population (individuals who experienced Myocardial Infarction), Intervention or Exposure (hospitalization due to Myocardial Infarction), Comparison (severity, occupational activity, and duration of hospitalization), Outcomes (return to work), and Study design (cohort study). Keywords and their synonyms were selected based on the respective databases, referencing the Health Sciences Descriptors (DeCS), Medical Subject Headings (MeSH), and Embase Subject Headings (Emtree). Boolean operators “AND” and “OR” were utilized as detailed in Table 1. The search strategy focused on terms appearing in article titles, subject headings, and abstracts.
Cohort studies assessing the return to work for individuals who experienced a Myocardial Infarction were included in this review, without any restrictions based on language. Studies that also addressed other conditions within the same cohort, such as Heart Failure and Rheumatic Heart Disease, were excluded. Relevant articles identified through database searches underwent a systematic selection process consisting of three stages: initial title screening, followed by abstract evaluation, and finally a comprehensive reading of the full text.
Subsequently, an exploratory review of all selected materials was conducted, leading to a focused and analytical reading of the most pertinent sections. The identification of methodological features and data extraction from these articles was performed by two independent reviewers. In instances of disagreement, both reviewers revisited the entire article for reevaluation. If discrepancies remained unresolved, a third independent reviewer was brought in to provide further insight.
The quality assessment of the studies included in this review utilized the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies provided by the National Heart, Lung, and Blood Institute (NHLBI). Information from the articles was systematically organized into tables detailing key research attributes such as first author, publication year, study type, database utilized, classification of Myocardial Infarction, inclusion criteria, sample size, along with outcomes studied and their principal findings and conclusions.
The protocol outlining the various stages involved in constructing this systematic review has been submitted to the International Prospective Register of Systematic Reviews (PROSPERO), under registration number CRD42023464316.
Results
The search of the database yielded a total of 4,695 articles (MEDLINE: 8; PubMed: 4,686; Lilacs: 0; Scielo: 0; Web of Science: 1). After eliminating duplicates, 4,686 records remained. From these, 17 articles were chosen through title screening. Three articles were excluded due to their abstracts failing to satisfy the selection criteria, which left 14 articles for comprehensive review. Of those reviewed, 2 did not fulfill all inclusion requirements, leading to a final count of 12 articles, as illustrated in Figure 1.
**
The twelve articles were meticulously reviewed and categorized, resulting in the creation of three tables that encapsulate pertinent research details. These tables include key attributes such as the first author’s name, publication year, study design, country of origin, classification of Myocardial Infarction, sample size, and criteria for inclusion (refer to Table 2). Table 3 summarizes the outcomes investigated, principal findings, and overall conclusions derived from the studies. Additionally, Table 4 provides information regarding disease characterization, duration of hospital stay, time required for return to work, and associated comorbidities. All studies included in this review were cohort studies, comprising nine prospective studies^11-19^ and three retrospective ones.^20-22^ The geographical origins of the research spanned Europe,^12,14,16-18,20,21^ Asia,^11,13,22^ Oceania,^19^ and North America.^15^ The inclusion criteria prominently featured the diagnosis of Myocardial Infarction,^11,12,14,15,18,20-22^ age ( > 18 ^15,22^, 18-63 ^20^, ≥ 55 for women and ≥ 60 for men,^13^ < 60^16^ > 18-60,^14^ 18-64,^17^ 30-65,^21^ ≤ 75^19^), and employment status at the time of or prior to the event. Collectively, these studies involved a total of 83,702 participants, with sample sizes ranging from as few as 102^12^ to as many as 22,394 ^21^ volunteers. A predominance of male participants was noted, with average ages at both minimum (48.65 years)^22^ and maximum (64.35 years)^11^ extremes.
Regarding educational level, most participants had an education level below high school, with mentions of vocational education, basic education,^14,21^ and secondary education,^22^ high school,^17^ and low to medium high school levels.^18^ Only five cohort studies provided insights into participants’ job classifications; predominant occupations included office/coordination roles and manual laborers, ^12^ agricultural workers,^13^ private sector employees across specialized categories and business professionals,^22^ as well as government agency staff.^16^ de Jonge et al also noted that most participants who returned to work had sedentary jobs, classified as light work.^18^
As for being active in the labor market at the time of the MI, among groups of people working or on leave, no more than three articles reported that 41.2%,^11^ 51%,^15^ and 56.9%^21^ of the participants were employed. The prevalence of return to work (RTW) after the acute event varied during the follow-up period. After one month, the return rate was 21.5%,^12^ 37%,^17^ and 41.7%^21^; after two months, it was 59.2%^12^; after three months, it was 46.2%,^18^ 86.4%,^21^ and 87.5%^11^; after four months, 91.1%^19^; after six months, 83.6%^14^; within one year, 55.9%^13^; one year: 76.9%,^18^ 79.9%,^19^ 80%,^14^ 91.1%,^21^ 92.7%^12^ and MI without SC 83% and with SC 52%^20^; after two years, 91.6%.^14^ Only one study presented the return rate without a time limit, with a general rate of 66.1%.^22^
Among those who returned to work, researchers from Malaysia (2017) identified that 93.2% returned to the same job, while 6.8% switched to a less demanding job.^22^ Osler et al noted that 17.9% of patients reported a significant salary reduction compared to the period before the coronary event.^17^ Another point concerns job termination within one or two years, particularly among those who had received medical leave.^14,17,21^ The average time of work leave was 44 days,^12^ 125.83 ± 125.04 days,^16^ and 8.62 weeks.^19^ The main circumstances leading to not returning to work were the inability to work and/or choosing not to work due to the MI,^13,17^ early retirement/disability retirement,^13,14^ regular retirement,^15,17,19^ unemployment,^13,15,17,19^ dismissal,^15,17^ paid medical leave,^14,17^ disability pension, death, emigration,^14^ and unspecified reasons.^13^
Another factor that interfered with RTW was the presence of depression^12,15,18,21^ and anxiety,^12,18^ as noted in four articles. Regarding comorbidities, Table 3 presents results on this variable from all articles. The most prevalent comorbidities were systemic arterial hypertension (SAH),^11,12,14-16,18,20,22^ diabetes mellitus (DM),^11,12,14-16,18-22^ dyslipidemia,^13,16,18,22^ and depression.^12,21^ Regarding the severity of the disease, seven articles provided data on the Left Ventricular Ejection Fraction (LVEF), with reduced EF (< 40),^13,18^ borderline EF (41-49), ^11,19^ and preserved EF ( ≥ 50). ^12,15^ Three articles used the Killip Classification: Killip 3-4,^16^ ≥ 2, ^18^ and 2-3. ^19^ Regarding the length of hospital stay, six articles provided data, in days, ranging from 2.9,^15^ 4, ^12,20^ 5.05-9.92, ^19^ to 11.^13,16^ The time to return to work was assessed at five weeks, ^14^ one month, ^12,13,17,21^ two months,^12,16^ three months, ^11,18,21^ six months, ^13^ one year, ^12,14,15,17-21^ two years, and five years ^17^ after hospital discharge or after MI.
Regarding the assessment of the methodological quality of the articles, all the cohort studies were classified as good quality, with Stendardo et al, ^12^ Warraich et al, ^15^ and Worcester et al ^19^ not clearly describing the study population. Additionally, none of the included articles justified the sample size (Table 5).
Discussion
The findings from this systematic review indicate that the rates of return-to-work (RTW) for individuals following a myocardial infarction (AMI) fluctuate based on the duration of follow-up, showing an upward trend over time. After one year post-event, the RTW rate is notably high, ranging from approximately 76.9% to 92.7%. ^12,14,18,19,21^ It is crucial to highlight that several factors influence the likelihood of an earlier return to work, including age, educational attainment, income level, type of employment—particularly those involving sedentary tasks or roles focused on office coordination—and self-employment status. ^12,14,18,21^ Consequently, the intricate relationship between myocardial infarction and return-to-work encompasses various physiological, socioeconomic, and sociopsychological dimensions that shape individuals’ perceptions and experiences regarding their capacity to resume regular activities.
Severity of the disease
Regarding the disease’s severity, most participants demonstrated either preserved or borderline left ventricular ejection fraction (LVEF). A lower incidence of LVEF values below 40%, along with a higher Killip class and myocardial infarction (MI) history, correlated with returning to work (RTW) compared to those who did not. ^18^ Mohd Mustafah et al indicated that individuals with single-vessel and two-vessel disease were 8.9 times and 3.8 times more likely, respectively, to return to work than their counterparts with three-vessel disease. ^22^ In contrast, researchers from Croatia found no significant association between traditional risk factors for arterial disease—such as affected myocardial wall segments and culprit coronary arteries—and permanent work cessation or the duration until returning to work. ^16^ Consequently, utilizing clinical factors as variables for assessing RTW following MI remains a contentious issue due to its connection to various influencing elements.
Length of hospital stay
Regarding the duration of hospitalization, one study indicated that there were no notable differences in return-to-work (RTW) rates between patients who resumed employment and those who did not. ^13^ Conversely, another investigation found that hospital stays exceeding 30 days and instances of anoxic brain injury during admission were linked to a diminished probability of returning to work, ^20^ alongside an increase in the number of hospitalization days. ^19^ These results are corroborated by Jiang et al, which emphasizes that complications occurring during a myocardial infarction can prolong the RTW process. ^13^ Consequently, the length of hospitalization reported in this study may be considered brief, likely reflecting improvements in treatment modalities and care protocols for the participants involved.
Comorbidity
All studies incorporated in this review examined various forms of comorbidity. The findings clearly indicated that individuals with a greater number of comorbid conditions had reduced chances of re-entering the workforce. ^14,15,20,21^ Among the most commonly observed comorbidities were diabetes mellitus (DM), systemic arterial hypertension (SAH), and acute myocardial infarction (AMI). Specifically, research conducted in Malaysia revealed that participants without DM were 3.7 times more likely to resume work compared to those diagnosed with the condition. ^22^ The advancements in myocardial infarction treatment, along with the rising number of survivors post-event, underscore the necessity for effective management of disease burden, as inadequate management may result in additional negative consequences.
Anxiety and depression
A significant theme that emerged from the reviewed studies was the connection between the inability to return to work or a diminished likelihood of doing so among individuals exhibiting symptoms of anxiety and depression. de Jonge et al found that the presence of any anxiety disorders within the first three months following a myocardial infarction (MI) correlated with a heightened risk of not resuming work. ^18^ This observation is supported by Warraich et al, who noted that over the course of a year, patients experiencing negative changes in employment were more likely to have a Patient Health Questionnaire-2 (PHQ-2) score exceeding 3, indicating potential depression, as well as reduced EQ-5D VAS scores, reflecting lower quality of life. ^15^ These results underscore a diminished self-assessment of health status when individuals do not return to work, highlighting the role of positive mood as a predictive factor for successful reintegration into the workforce. ^12^
Time away from work
In a prospective cohort study conducted in Italy, the average duration of time off work was found to be 44 days. ^12^ Similarly, another investigation revealed that the typical span from 30 days post-diagnosis to either retirement, death, or cessation of work was approximately 4.1 years. ^17^ Among employees who were unable to return following an acute myocardial infarction (AMI), the reasons for not resuming work varied significantly; these included inability to perform job duties, early retirement, receiving a disability pension, termination of employment, or death. ^13^ Researchers have indicated that the probability of experiencing disability or opting for voluntary early retirement was notably higher among specific groups—namely women, individuals aged over 50 years, those with limited educational backgrounds, people in low-skill occupations, those living with a partner, and individuals who were on sick leave or unemployed 30 days after their hospital admission. Additionally, factors such as having undergone myocardial revascularization and the presence of comorbidities also contributed to this increased likelihood.^17^
This review underscores critical factors associated with the return to work following a myocardial infarction (MI) and identifies elements that contribute to prolonged absence from employment. The findings presented offer insights that can inform intervention strategies and guide future research aimed at minimizing the duration of time away from work, thereby alleviating costs for both individuals and society at large.
While a majority of the studies reviewed exhibit strong methodological rigor and provide data on temporal trends, certain limitations are evident concerning the included research: notably, the small sample sizes and specific characteristics of the countries where these outcomes were assessed. Of the twelve studies analyzed, four were conducted in Denmark, with no representation from Latin America or Africa, potentially affecting the observed return-to-work rates. Furthermore, a significant limitation lies in the considerable variability in how results were reported across studies, which precluded the possibility of conducting a meta-analysis.
Conclusion
The rate of individuals returning to work following a Myocardial Infarction is notably high within the first year. This phenomenon is influenced by various physical, psychological, and social factors, alongside the identification of mechanisms that facilitate an expedited return to employment. Nevertheless, further research is essential, particularly studies conducted across diverse populations and separating professional categories, to gather more thorough insights.
Competing Interests
No conflicts of interest.
Ethical Approval
Not applicable.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization (WHO). Cardiovascular Diseases (CV Ds) [Internet]. WHO; 2019. Available from: https://www.who.int/cardiovascular_diseases/en/.
- 2Bett MS Zardo JM Utiamada JL Reckziegel JL dos Santos VV Acute myocardial infarction: from diagnosis to intervention Res Soc Dev 2022113 e 2381132644710.33448/rsd-v 11i 3.26447 · doi ↗
- 3da Silva Mendes LF Leal AK de Sousa LL de Carvalho Lopes BR de Araujo MS da Silva Moreira J Epidemiological analysis of hospitalizations for acute myocardial infarction in Teresina-PI between 2017 and 2022 Res Soc Dev 2023128 e 481284286210.33448/rsd-v 12i 8.42862 · doi ↗
- 4Kang K Gholizadeh L Han HR Health-related quality of life and its predictors in Korean patients with myocardial infarction in the acute phase Clin Nurs Res 20213021617010.1177/105477381989469231823657 · doi ↗ · pubmed ↗
- 5Uhlmann DB Alexandre NM Rodrigues RC São-João TM Acute coronary syndrome patients’ return to work Rev Bras Saúde Ocup 201944 e 1010.1590/2317-6369000019518 · doi ↗
- 6Zetterström K Vaez M Alexanderson K Ivert T Pehrsson K Hammar N Disability pension after coronary revascularization: a prospective nationwide register-based Swedish cohort study Eur J Prev Cardiol 20152233041110.1177/204748731351847224403297 · doi ↗ · pubmed ↗
- 7Byrne RA Rossello X Coughlan JJ Barbato E Berry C Chieffo A 2023 ESC Guidelines for the management of acute coronary syndromes Eur Heart J 20234438372082610.1093/eurheartj/ehad 19137622654 · doi ↗ · pubmed ↗
- 8Moher D Liberati A Tetzlaff J Altman DG PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement Int J Surg 201083364110.1016/j.ijsu.2010.02.00720171303 · doi ↗ · pubmed ↗