Toxic Megacolon With a Positive Clostridioides difficile Antigen but Negative Toxin Assay
Milikyas A Feyisa

TL;DR
An elderly man with a positive C. difficile antigen test but negative toxin assay developed severe toxic megacolon, highlighting limitations in diagnostic testing for severe CDI.
Contribution
This case emphasizes the need to prioritize clinical judgment over conflicting lab results in severe C. difficile infections.
Findings
A patient with a positive C. difficile antigen but negative toxin assay developed toxic megacolon.
Toxin enzyme immunoassays may lack sensitivity in severe CDI cases.
Clinical and radiological findings should guide treatment when lab results are discordant.
Abstract
The diagnosis of Clostridioides difficile infection (CDI) relies on a combination of clinical presentation and laboratory testing. However, a critical diagnostic discordance occurs when laboratory results contradict a rapidly evolving clinical picture. This is a case of a 78-year-old man with four comorbidities who presented with watery diarrhea and a C. difficile screen-positive but toxin-negative stool sample. His main risk factors included advanced age and the prolonged use of a proton pump inhibitor. Despite his initial negative toxin assay, his condition progressively worsened over three days following his admission, with the development of toxic megacolon, diagnosed clinically and radiologically. This report synthesizes evidence on the limitations of toxin enzyme immunoassays in severe CDI, contextualizing a well-documented, but dangerously overlooked, phenomenon where test…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
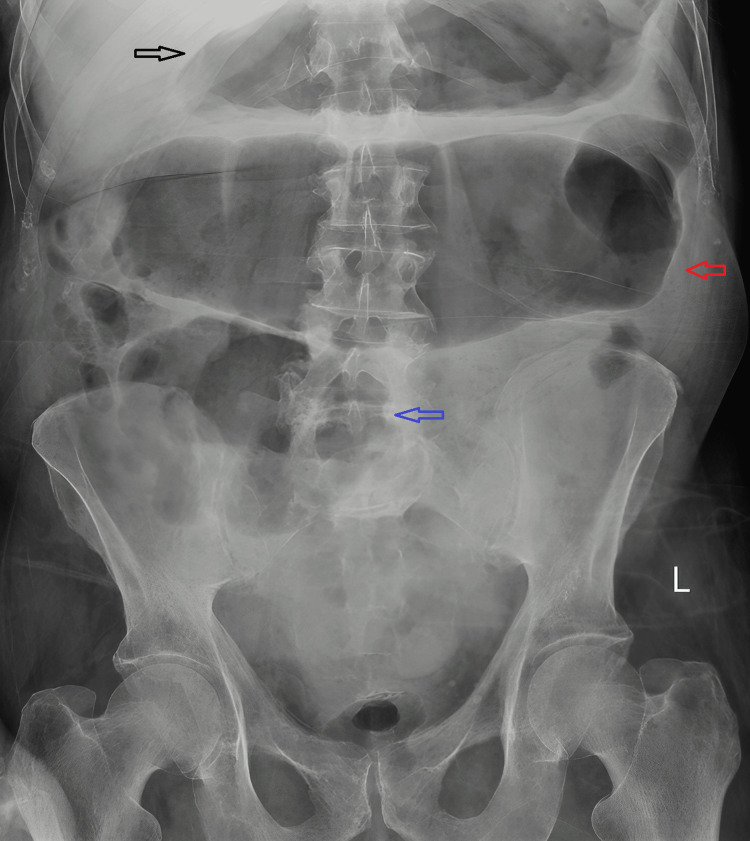 Figure 1
Figure 1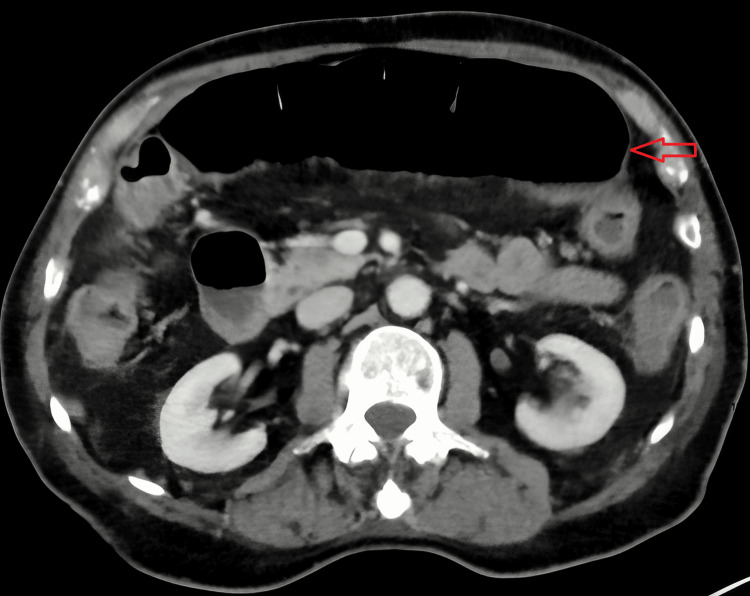 Figure 2
Figure 2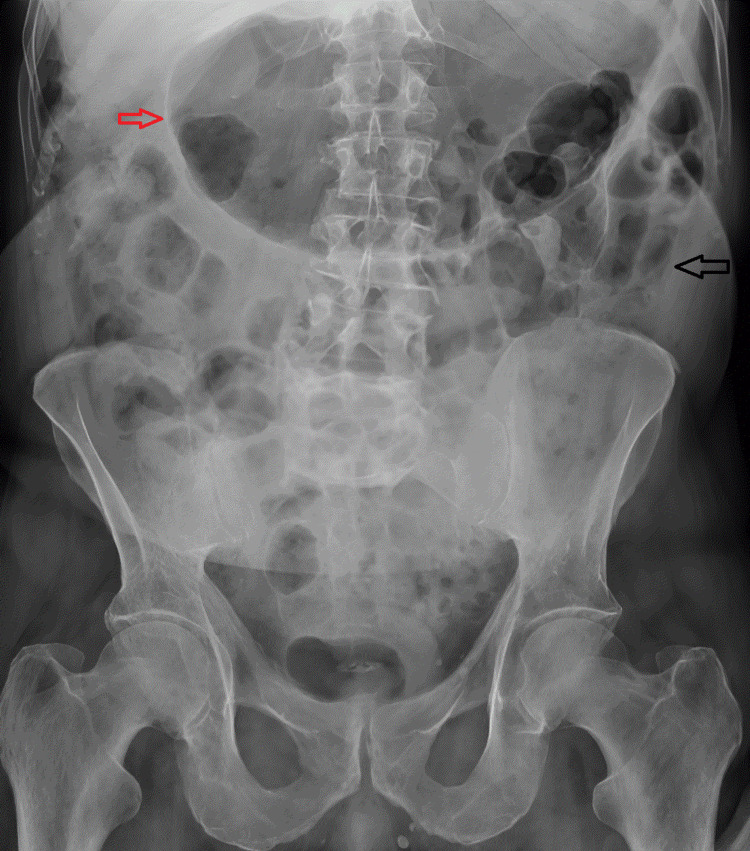 Figure 3
Figure 3| Pathogen | Result |
| Yersinia enterocolitica | Not detected |
|
| Not detected |
|
| Not detected |
|
| Positive |
|
| Not detected |
| Verotoxin gene | Not detected |
| Salmonella | Not detected |
| Campylobacter | Not detected |
| Ova/Parasite | Not detected |
| Norovirus | Not detected |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClostridium difficile and Clostridium perfringens research · Gastrointestinal motility and disorders · Nosocomial Infections in ICU
Introduction
Clostridioides difficile infection (CDI) is a leading cause of healthcare-associated diarrhea, with a spectrum ranging from asymptomatic colonization to mild colitis to life-threatening toxic megacolon and septic shock [1]. Broad-spectrum antibiotics are the main predisposing factors, while the use of gastric acid suppressants (proton pump inhibitors (PPIs) and H2 antagonists), prolonged hospitalization, and immunocompromised states (advanced age or acquired immunodeficiency) are also important risk factors [2].
Modern laboratory diagnostic algorithms often employ a two-step process using a sensitive screening test for glutamate dehydrogenase (GDH), followed by a confirmatory test for toxins A and B via enzyme immunoassay (EIA) [3]. While cost-effective, the toxin EIA has known sensitivity limitations, particularly in severe disease due to reasons discussed in this article. This limitation can cause a diagnostic challenge if sound clinical judgement is not used along with supplementary imaging. This case report illustrates the perilous clinical scenario where reliance on a negative toxin EIA can delay critical, life-saving treatment in a patient progressing to toxic megacolon.
Case presentation
A 78-year-old man was admitted with a two-day history of fatigue, lethargy, and five episodes of watery diarrhea. He had no abdominal pain or fever spikes. His past medical history was significant for schizophrenia, a remote brain hemorrhage with craniotomy, seizure, and high cholesterol. He lived alone with home care support twice daily and used a walking stick for mobility. Regular medications included pantoprazole, aripiprazole, phenytoin, rosuvastatin, folic acid, and nutritional supplements. There was no recent history of antibiotic use or hospitalization in the preceding two years.
On admission, he was pleasantly confused (4AT score, 4/12; Glasgow Coma Scale score, 14/15) with dry mucous membranes. Abdominal examination was initially unremarkable, revealing a soft, non-tender, and non-distended abdomen. Initial blood tests revealed leukocytosis (white cell count, WCC 22.1 x 10⁹/L; neutrophils, 20.5 x 10⁹/L) and an elevated C-reactive protein (CRP) (54 mg/L). Hemoglobin level was 17 g/dL. An abdominal X-ray showed gassy bowel loops but no evidence of obstruction or free air. A stool sample was reported on the next of admission as C. difficile screen (GDH) was positive, but the toxin A/B EIA was negative. The stool pathogen panel is shown in Table 1.
By day three of admission, the patient subjectively felt better, was eating and drinking, and had no further vomiting. However, he continued to have high-volume diarrhea (up to six times per day of type 7 diarrhea). Abdominal examination revealed new distension with hypertympany. His CRP rose sharply to 164 mg/L. A repeat abdominal X-ray demonstrated a dilated transverse colon measuring 9.7 cm, consistent with megacolon (Figure 1). Serum lactate remained normal (0.6-0.7 mmol/L). CT of the abdomen/pelvis confirmed the diagnosis (Figure 2), showing diffuse circumferential thickening and mucosal hyperenhancement of the entire colon and rectum (proctocolitis) and a dilated transverse colon (5.7-7.7 cm) with reduced wall enhancement, consistent with megacolon complicating severe colitis. The discrepancy between the radiographic (9.7 cm) and CT (5.7 cm anteroposterior and 7.7 craniocaudal) measurements is attributable to both imaging technique and pathophysiological change. Projection radiography can overestimate the diameter of a tortuous, gas-filled loop, while CT provides a precise axial measurement. Furthermore, during interval hours between the two imagings allowed for possible colonic decompression and redistribution of intraluminal content, altering the gas-to-fluid ratio seen on CT.
Abdominal X-ray on day three.Dilated transverse colon measuring up to 9.7 cm in keeping with megacolon (red arrow), with gassy distension of the stomach (black arrow) and the caecum (blue arrow).
CT scan of abdomen and pelvis on day three.The transverse colon (red arrow) is dilated measuring 5.7 cm in the anteroposterior diameter and 7.7 cm in the craniocaudal diameter consistent with megacolon.
Given the ongoing profuse watery diarrhea and radiological findings, antibiotic therapy was started with high-dose oral vancomycin (500 mg four times daily) and intravenous metronidazole (400 mg three times daily), alongside aggressive electrolyte replacement. Surgical review deemed the patient medically unfit for operative intervention. Progressively, the diarrhea started to settle, decreasing to one to two episodes per day of type 5 stool. On the eighth day of admission, his diarrhea settled, and he was engaging well with physiotherapy to attain his baseline mobility. A follow-up abdominal X-ray showed interval improvement (Figure 3).
Follow-up abdominal X-ray.The black arrow shows interval improvement in the transverse colon and the red arrow shows the gassy stomach.
Discussion
CDI is a leading cause of healthcare-associated diarrhea, with a spectrum ranging from mild colitis to life-threatening toxic megacolon and septic shock. This case exemplifies a well-documented but clinically treacherous pitfall in CDI diagnosis: the development of fulminant colitis and toxic megacolon despite an initial negative stool toxin EIA. The two-step diagnostic algorithm (GDH + toxin EIA) is widely used for its high negative predictive value and cost-effectiveness [3]. However, its weakness lies in the suboptimal sensitivity of the toxin EIA. Meta-analyses report a sensitivity of approximately 75% compared to the gold-standard cell culture cytotoxicity neutralization assay, meaning one in four true cases may yield a false-negative toxin result [4,5].
Several pathophysiological mechanisms explain this phenomenon in severe disease, which can explain our patient’s presentation. One mechanism is that the dilutional effect of a profuse, watery diarrhea leads to significant stool dilution, potentially reducing toxin concentration below the detection threshold of the EIA [6,7]. The other is toxin sequestration that occurs in fulminant colitis, where *C. difficile *toxin B (TcdB) binds extensively to high-affinity receptors (e.g., Frizzled proteins, CSPG4) on colonic epithelial cells [8-10]. This binding and subsequent internalization “sequesters” the toxin within the colonic tissue, leaving less free toxin in the stool lumen to be detected by commercial assays [8,10,11]. Lastly, patients who are immunosenescent (due to advanced age, as in this patient) might not mount an adequate response, resulting in an inflammatory cascade outpacing toxin production or release, creating a diagnostic window where stool toxin levels are low despite severe tissue damage [11].
This patient’s clinical trajectory underscores the vital recommendations from the Infectious Diseases Society of America/Society for Healthcare Epidemiology of America guidelines, which advise initiating empirical treatment for CDI when clinical suspicion is high, without waiting for test results [5]. Furthermore, in suspected severe cases, imaging is a critical diagnostic tool. The findings of colonic wall thickening (>4 mm) and megacolon (>6 cm diameter) on CT scan are hallmark indicators of severity [6,7]. In this case, radiology provided the definitive evidence of disease severity that compelled aggressive medical management, overriding the negative toxin assay.
While the lack of reflex molecular confirmation is a limitation in this case, the diagnosis of fulminant CDI was made clinically based on a positive GDH antigen in the setting of toxic megacolon and significant leukocytosis. Given that toxin EIA has a high false-negative rate, and the patient’s critical status precluded waiting for further confirmatory testing, empirical treatment was initiated. The subsequent resolution of toxic megacolon upon targeted CDI therapy further supports the diagnosis.
Conclusions
This case serves as a critical reminder that a negative C. difficile toxin EIA does not exclude severe, life-threatening infection. Clinicians must maintain a high index of suspicion for fulminant CDI in patients with compatible symptoms, especially new or worsening abdominal distension, high-volume diarrhea, and systemic inflammation, irrespective of initial toxin test results. Clinical judgment, supported by timely radiological imaging, must guide the decision to initiate aggressive empirical therapy to prevent progression to toxic megacolon, colectomy, and death. The literature unequivocally supports treating the patient’s clinical syndrome, not the laboratory report. Most importantly, however, unnecessary PPI treatment should be deprescribed by a pharmacist or general practitioner as it is a known risk factor.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pseudomembranous colitis Dis Mon Farooq PD Urrunaga NH Tang DM von Rosenvinge EC 1812066120152576924310.1016/j.disamonth.2015.01.006PMC 4402243 · doi ↗ · pubmed ↗
- 2Laboratory markers predictive of fulminant Clostridioides difficile infection refractory to fluid resuscitation Infect Prev Pract Ahmad O Crawford TN Arora V Maskey MK 100127320213436874410.1016/j.infpip.2021.100127 PMC 8336175 · doi ↗ · pubmed ↗
- 3Diagnostic guidance for C. difficile infections Adv Exp Med Biol Crobach MJ Baktash A Duszenko N Kuijper EJ 2744105020182938366210.1007/978-3-319-72799-8_3 · doi ↗ · pubmed ↗
- 4Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA)Clin Infect Dis Mc Donald LC Gerding DN Johnson S 066201810.1093/cid/cix 1085 PMC 601898329462280 · doi ↗ · pubmed ↗
- 5Accuracy of diagnostic assays for the detection of Clostridioides difficile: a systematic review and meta-analysis J Microbiol Methods Zangiabadian M Ghorbani A Nojookambari NY 10665720420233652818310.1016/j.mimet.2022.106657 · doi ↗ · pubmed ↗
- 6Toxic megacolon: background, pathophysiology, management challenges and solutions Clin Exp Gastroenterol Desai J Elnaggar M Hanfy AA Doshi R 2032101320203254715110.2147/CEG.S 200760 PMC 7245441 · doi ↗ · pubmed ↗
- 7Toxic megacolon secondary to Clostridium difficile colitis. Case report Rev Gastroenterol Mex Sánchez-Pérez MA Muñoz-Juárez M Luque-de León E Moreno-Paquentin E Cordera-González de Cosio F Jean-Silver E 103106752010 http://www.researchgate.net/publication/43347955_Toxic_megacolon_secondary_to_Clostridium_difficile_colitis_Case_report 20423791 · pubmed ↗
- 8Frizzled proteins are colonic epithelial receptors for C. difficile toxin B Nature Tao L Zhang J Meraner P 35035553820162768070610.1038/nature 19799 PMC 5519134 · doi ↗ · pubmed ↗