Clinical features and treatment outcomes of acute-onset endophthalmitis caused by Staphylococcus lugdunensis: a case series
Justin A. Chen, Michael Y. Zhao, Lauren C. Kiryakoza, Salomon Merikansky, Landon J. Rohowetz, Darlene Miller, Harry W. Flynn Jr.

TL;DR
This study examines eye infections caused by Staphylococcus lugdunensis and finds that treatment with vancomycin leads to good outcomes.
Contribution
The study provides updated data on the effectiveness of vancomycin against S. lugdunensis in eye infections.
Findings
All S. lugdunensis isolates were sensitive to vancomycin and moxifloxacin.
Most patients achieved a visual acuity of 20/150 or better after treatment.
Vancomycin remains a reliable empiric treatment for this type of eye infection.
Abstract
To report a series of patients with acute-onset endophthalmitis caused by culture-proven Staphylococcus lugdunensis and to provide an update on the microbiologic susceptibility and clinical outcomes resulting from this organism. This study included 6 eyes of 6 patients. The etiologies included cataract surgery (4), intravitreal injection (1), and posterior segment surgery (1). All isolates (100%) of S. lugdunensis demonstrated sensitivity to vancomycin with minimal inhibitory concentration (MIC) values ranging from ≤ 0.5 to 1 mcg/mL and to moxifloxacin with MIC values ranging from ≤ 0.25 to 1 mcg/mL. One of 6 isolates demonstrated intermediate resistance to gentamicin with a MIC value of 8 mcg/mL. Four of 6 patients underwent pars plana vitrectomy following initial treatment with intravitreal antibiotics, and 1 eye underwent vitrectomy as initial management. Best-corrected visual…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
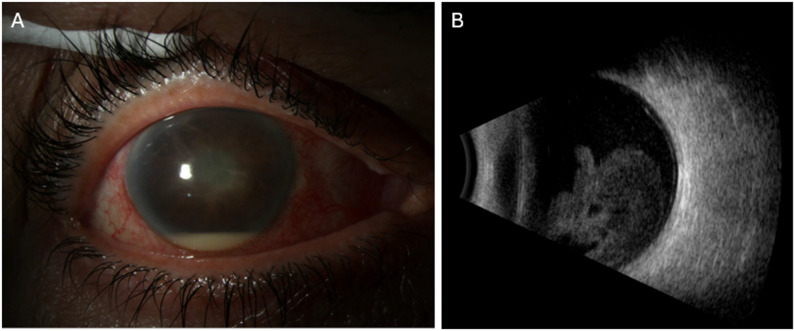 Figure 1
Figure 1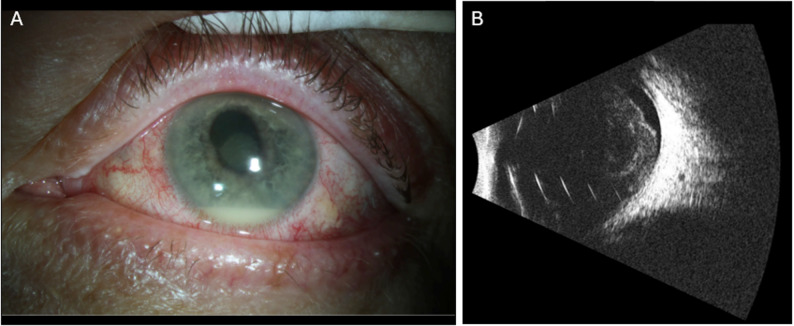 Figure 2
Figure 2- —https://doi.org/10.13039/100001818Research to Prevent Blindness
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Infections and Treatments · Antimicrobial Resistance in Staphylococcus · Ocular Diseases and Behçet’s Syndrome
Introduction
Acute-onset exogenous endophthalmitis is a rare but vision-threatening infection that can occur following intraocular procedures. Coagulase-negative Staphylococci are the most common causative organisms, accounting for approximately 70% of cases of postprocedural endophthalmitis [1]. Of the group, the 2 most common isolates cultured are Staphylococcus epidermis (81.9%) and Staphylococcus lugdunensis (5.9%) [2]. Staphylococcus lugdunensis may have been previously under-reported, as advances in microbiological laboratory techniques have allowed for improved identification of less prevalent coagulase-negative Staphylococci species [3]. Investigations into acute-onset endophthalmitis caused by S. lugdunensis have shown a wide variability of visual outcomes following appropriate intervention. This case series aims to provide an update on the clinical presentation, antibiotic susceptibility patterns, and treatment outcomes of patients diagnosed with acute-onset endophthalmitis due to S. lugdunensis.
Findings
A review of all patients with a diagnosis of acute-onset endophthalmitis at the University of Miami, Bascom Palmer Eye Institute Microbiology Department from January 2015 through April 2025 was performed. Patients were included in this study if vitreous and/or aqueous samples taken at the time of diagnosis identified isolates of S. lugdunensis. In total, 7 patients (6 men, 1 woman; mean age 64.9 years) were identified to have met study criteria. One immunocompromised patient with a history of primary intraocular lymphoma treated with systemic chemotherapy and radiation, complicated by radiation retinopathy and disseminated chorioretinal inflammation, presented with a 5-year history of gradual decline in visual acuity that later progressed from 20/400 to light perception over the course of 1 month. This patient subsequently underwent PPV due to concern for lymphoma recurrence, with vitreous cassette cultures identifying S. lugdunensis. Anterior chamber cultures obtained 4 days post-vitrectomy again confirmed growth of S. lugdunensis. This patient was removed from data analysis as he was unique compared to the other patients in how endophthalmitis was acquired.
The remaining 6 patients (5 men, 1 woman; mean age 62.4 years) all presented with acute-onset exogenous endophthalmitis with culture-proven S. lugdunensis. Four patients had undergone cataract extraction with intraocular lens implantation and presented on average 7.0 days after intraocular surgery. On examination, patients typically exhibited significant vision loss, conjunctival injection, hypopyon, fibrin in the anterior chamber, and marked vitreous opacities (Fig. 1). Patient 2 presented 8 days after cataract surgery, complaining of a tender eye but a visual acuity of 20/25. Examination was significant for diffuse conjunctival injection and significant cells in the anterior chamber. The patient later represented two days later with hand motion vision and new 1.5 mm hypopyon and dense vitreous debris on exam. Patient 6 presented 5 days after receiving an intravitreal injection of bevacizumab for proliferative diabetic retinopathy and diabetic macular edema (Fig. 2). Visual acuity was hand motions and exam was significant for diffuse conjunctival injection and hypopyon. B-scan ultrasound revealed dense, mobile vitreous opacities. Patient 3 presented with a visual acuity of light perception 3 days after pars plana vitrectomy (PPV) for visually significant vitreous opacities. Due to the abrupt and significant loss of vision following surgery, the patient underwent emergent PPV. The remaining patients were initially treated with vitreous aspiration and intravitreal antibiotics, most commonly vancomycin 1.0 mg and ceftazidime 2.25 mg. Patient presentation, clinical data and initial management are summarized in Table 1.
Fig. 1. Patient 5: A 71-year-old female presented 4 days after cataract surgery in the right eye. Visual acuity was light perception. (A) Examination demonstrated diffuse conjunctival injection, corneal edema, and a hypopyon. (B) B-scan ultrasound revealed dense mobile vitreous opacities. The patient underwent vitreous tap and injection with vancomycin, ceftazidime and dexamethasone. Best-corrected visual acuity at last follow-up was 20/40.
Fig. 2. Patient 6: A 64-year-old male presented 5 days after receiving intravitreal bevacizumab in the left eye. Visual acuity was hand motions. (A) Examination demonstrated diffuse conjunctival injection, corneal infiltrate, and a 2 mm hypopyon. (B) B-scan ultrasound demonstrated dense vitreous debris and an incomplete posterior vitreous detachment. The patient underwent vitreous tap and injection with vancomycin, ceftazidime and dexamethasone and eventual pars plana vitrectomy with repeat injection of intravitreal vancomycin, ceftazidime and dexamethasone. Best-corrected visual acuity at last follow-up 6 days after initial presentation was hand motions.
Table 1. Clinical presentations, interventions, and treatment outcomes of patients with acute-onset endophthalmitis caused by S. lugdunensisPatientAge/Sex/EyeHistoryCo-MorbiditiesBCVA @ PresentationInitialTreatmentsAdditionalTreatmentsBCVA @ LastFollow-upComments150/M/ODCE-IOLNoneHM @POD#11Day 0: IV van, cef(POD#11)YAG of fibrin and membrane@ POD#14 (Day 3)20/150LTFU POD#17 (Day 6)253/M/OSCE-IOLVitreous cassette from PPV grew MDR Serratia marcescens20/25 @POD#8Day 0: IV van, cef, vori(POD#8)Day 3: PPV/FAX/1000cs SO, IV vanc, cef(POD#11)PPV/SOR/FAX@ POM#320/70BCVA HM @POD#10 (Day 2)NVS ERM noted POM#4370/M/ODPPV for visually significant PVDAllergic to amoxicillinLP @POD#3Day 0: PPV/1000cs SO, IV van, ami, dex(POD#3)PPV/SOR/AC washout@ POW#620/30Recurrent CME noted POM#6464/M/OSCE-IOLNoneLP @POD#5Day 0: IV van, cef, dex(POD#5)Day 1: PPV with IV van, cef, dex(POD#6)None20/20None571/F/ODCE-IOLPOAGLP @POD#4Day 0: IV van, cef, dex(POD#4)PPV for debulking vitreous opacities@ POM#120/40NVS ERM noted POM#2NVS temporal operculated hole noted POY#2664/M/OSIV bevacizumab for DMEPDR with DME receiving IV bevacizumabHM @POD#5Day 0: IV van, cef, dex(POD#5)Day 1: PPV with IV van, cef, dex(POD#6)NoneHMLTFU POD#11 (Day 6)Abbreviations: AC, anterior chamber; Ami, amikacin; BCVA, best corrected visual acuity; Cef, ceftazidime; CE, cataract extraction; CME, cystoid macular edema, Cs, centistoke; Dex, dexamethasone; DME, diabetic macular edema; ERM, epiretinal membrane; FAX, fluid-air exchange; HM, hand motion; IOL, intraocular lens; IV, intravitreal; LP, light perception; LTFU, lost to follow-up; MDR, multi-drug resistant; NVS, not visually significant; OD, right eye; OS, left eye; PDR, proliferative diabetic retinopathy; POAG, primary open angle glaucoma; POD, post-operative day; POM, post-operative month; POW, postoperative week; POY, postoperative year; PPV, pars plana vitrectomy; PVD, posterior vitreous detachment; SO, silicone oil tamponade; SOR, silicone oil removal; Van, vancomycin; Vori, voriconazole; YAG, yttrium aluminum garnet laser capsulotomy.
Of the 6 patients who presented, patient 1 and patient 6 were both lost to follow-up 6 days after initial evaluations; last documented best corrected visual acuity (BCVA) was 20/150 and hand motions, respectively. Of the remaining 4 patients, BCVA was favorable; 100% (4/4) had BCVA ≥ 20/70 and 75% (3/4) had BCVA ≥ 20/40 at last follow-up. Five of the 6 patients were initially treated with intravitreal antibiotics, while 1 patient underwent vitrectomy as initial management. Of the 5 patients who received intravitreal antibiotics, 4 patients subsequently underwent PPV. Subsequent treatments and clinical outcomes are described in Table 1.
S. lugdunensis was isolated in microbiologic cultures in all 6 cases, with antibiotic susceptibilities and minimum inhibitor concentrations (MIC) in mcg/mL documented in Table 2. All isolates were sensitive to vancomycin with MIC values ranging from ≤ 0.5 to 1 mcg/mL and to moxifloxacin with MIC values ranging from ≤ 0.25 to 1 mcg/mL. Five isolates were sensitive to gentamicin with MIC values of ≤ 0.5 mcg mL, with 1 demonstrating intermediate resistance with an MIC of 8 mcg/mL Of the 6 total isolates, 5 were tested for oxacillin susceptibilities, with 2 demonstrating resistance with MIC values ≥ 4 mcg/mL.
Table 2. Antibiotic susceptibilities and minimum inhibitory concentrations (mcg/ml) of patients with acute-onset endophthalmitis caused by S. lugdunensisPatient #VancomycinGentamicinOxacillinMoxifloxacinClindamycin1S (≤ 0.5)S (≤ 0.5)S (2)S (≤ 0.25)S (0.25)2S (≤ 0.5)S (≤ 0.5)N/AS (≤ 0.25)S (≤ 0.12)3S (1)I (8)R (≥ 4)S (≤ 0.25)S (0.25)4S (≤ 0.5)S (≤ 0.5)S (2)S (≤ 0.25)S (0.25)5S (0.5)S (0.5)S (2)S (1)S (0.25)6S (1)S (≤ 0.5)R (≥ 4)S (≤ 0.25)S (0.25)Abbreviations: I, Intermediate; R, Resistant; S, Sensitive. Minimum inhibitory concentration, if available, is in parentheses in mcg/ml.
Discussion
Staphylococcus lugdunensis is known to cause an array of clinical infections including skin and soft tissue infections but can also demonstrate marked pathogenicity in cases of osteomyelitis, prosthetic joint infections, and infective endocarditis [3]. The virulence and aggressive clinical course of non-ocular cases of S. lugdunensis is well documented and has been compared to that of Staphylococcus aureus [4]. Studies evaluating non-ocular infections of S. lugdunensis have demonstrated greater pathogenicity than other coagulase-negative Staphylococci species, often requiring more intensive treatment [4].
There has been a wide range in reported visual outcomes in patients with acute-onset exogenous endophthalmitis caused by S. lugdunensis. In a retrospective study, Murad-Kejbou et al. documented 3 patients with limited visual recovery, although these poor outcomes may have had limited visual potential due significant co-morbidities (e.g., end-stage glaucoma and advanced age-related macular degeneration) [5]. Another case series by Chiquet et al. described 5 cases, noting poor visual outcomes after PPV potentially due to post-operative retinal detachment [6]. However, a retrospective case series by Chen et al. reported 2 cases of acute-onset exogenous endophthalmitis caused by culture-proven S. lugdunensis from Taiwan; both patients achieved a BCVA ≥ 20/50 following intravitreal antibiotics and subsequent PPV [7].
In this review, visual outcomes were encouraging in patients with acute-onset endophthalmitis caused by S. lugdunensis, especially in those who were able to attend longitudinal follow-up. The poor visual acuity observed in 2 patients may reflect the brief duration of follow-up, which did not extend beyond 1 week. These favorable outcomes are similar to the previous retrospective case series of 6 patients by Garoon et al. At last follow-up, Garoon et al. reported 5 of 6 patients (83.3%) with BCVA ≥ 20/100 and 3 (50%) with BCVA ≥ 20/40 [8]. It was noted that of the 3 patients who had more limited visual recovery, 1 patient experienced corneal decompensation requiring keratoplasty and intraocular lens repositioning, and 2 other patients had open globe injury in addition to endophthalmitis, followed by macula off retinal detachment, aphakia, and irregular astigmatism [8]. However, interpretation is ultimately limited by the small cohort size and incomplete follow-up.
There are multiple factors that may affect the visual outcomes of patients with endophthalmitis. Visual outcomes tend to be poorer if the identified organism is more virulent and/or has a higher rate of antibiotic resistance (e.g., Enterococci) [9]. However, prompt diagnosis of suspected endophthalmitis and appropriate treatment can be vision saving. Initial treatment tends to be either vitreous tap and injection of antibiotics or PPV with intravitreal antibiotics [10]. An investigation on antibiotic-resistant endophthalmitis by Choi et al. demonstrated that patients who underwent early vitrectomy (< 24 h of symptom onset) following initial intravitreal antibiotics achieved better final visual acuity at the last follow-up visit than those who received delayed vitrectomy [11]. Close monitoring is important to monitor clinical progression and determine the need for repeat intravitreal antibiotics or vitrectomy.
Data on the microbiologic susceptibility of S. lugdunensis isolated from intraocular sources remain relatively limited. All isolates in this review demonstrated sensitivity to vancomycin and moxifloxacin, which is consistent with the sensitivities reported by Garoon et al.^4^ Differing from Garoon et al., 1 isolate in this review demonstrated intermediate resistance to gentamicin. A large epidemiologic study from United States tertiary care centers by Palumbo et al. investigating S. lugdunensis isolated from various non-ocular sources demonstrated comparable susceptibility patterns. However, the authors reported that all isolates demonstrated sensitivity to gentamicin [5]. To our knowledge, this represents the first documented instance of gentamicin resistance across all isolates of S. lugdunensis reported in the USA.
Surveillance for aminoglycoside resistance in endophthalmitis caused by S. lugdunensis may be warranted, and use of intravitreal amikacin in endophthalmitis should be guided by susceptibility testing. As reflected in this review, S. lugdunensis remains susceptible to vancomycin and fluoroquinolones with no documented resistance; these isolates demonstrated less overall antibiotic resistance relative to general susceptibility patterns [3, 5]. Despite concerns for rising antibiotic resistance with other Staphylococcus species, vancomycin continues to be effective against S. lugdunensis and should remain as a first-line antibiotic for treatment of acute-onset endophthalmitis caused by coagulase-negative Staphylococci.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen KJ, Sun MH, Tsai ASH, Sun CC, Wu WC, Lai CC (2022) Staphylococcus lugdunensis endophthalmitis: case series and literature review. Antibiot (Basel) 11(11):1485. 10.3390/antibiotics 1111148510.3390/antibiotics 11111485 PMC 968658836358140 · doi ↗ · pubmed ↗
- 2Garoon RB, Miller D, Flynn HW Jr (2017) Acute-onset endophthalmitis caused by Staphylococcus lugdunensis. Am J Ophthalmol Case Rep 9:28–30. 10.1016/j.ajoc.2017.12.00610.1016/j.ajoc.2017.12.006PMC 578686129468213 · doi ↗ · pubmed ↗
- 3Murad-Kejbou S, Kashani AH, Capone A Jr, Ruby A (2014) Staphylococcus lugdunensis endophthalmitis after intravitreal injection: a case series. Retin Cases Brief Rep 8(1):41–44. 10.1097/ICB.0b 013e 3182 a 85a 4f 10.1097/ICB.0b 013e 3182 a 85a 4f 25372206 · doi ↗ · pubmed ↗
- 4Chiquet C, Pechinot A, Creuzot-Garcher C et al (2007) Acute postoperative endophthalmitis caused by Staphylococcus lugdunensis. J Clin Microbiol 45(6):1673–1678. 10.1128/JCM.02499-0610.1128/JCM.02499-06PMC 193310117392442 · doi ↗ · pubmed ↗