Prevalence and factors associated with chronic low back pain in students of the university of Dschang: a cross-sectional study in a sub-Saharan university
Abdoulaye Abdourahim, Fernando Kemta Lekpa, Sylvain Raoul Simeni Njonnou, Christian Ngongang Ouankou, Sandrine Nadège Chuente Sime, Yannick Fogang Fogoum, Siméon Pierre Choukem, Jerôme Ateudjieu

TL;DR
This study found that about 6% of university students in Dschang suffer from chronic low back pain, with obesity and family history being key risk factors.
Contribution
The study identifies overweight/obesity and parental history as significant risk factors for chronic low back pain in a sub-Saharan university population.
Findings
Chronic low back pain prevalence among students was 6.2%.
Overweight or obese students were 1.82 times more likely to have chronic low back pain.
A parental history of low back pain increased the risk by 2.6 times.
Abstract
Chronic low back pain is a health issue affecting more young people worldwide. This study aimed to determine the prevalence and factors linked to chronic low back pain among students at the University of Dschang. We carried out a two-part study focusing on students at the University of Dschang. For the descriptive cross-sectional part, sampling was stratified by faculty and level of study. Participants were chosen systematically, and data were collected through interviews using a pre-tested questionnaire. We calculated the prevalence of chronic low back pain. In the case-control part, students with chronic low back pain served as cases, while those without low back pain were controls. They were matched for age and sex, with one case for every two controls. An adjusted OR was estimated to assess the association between determinants, considering confounding factors, with a 95% CI and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
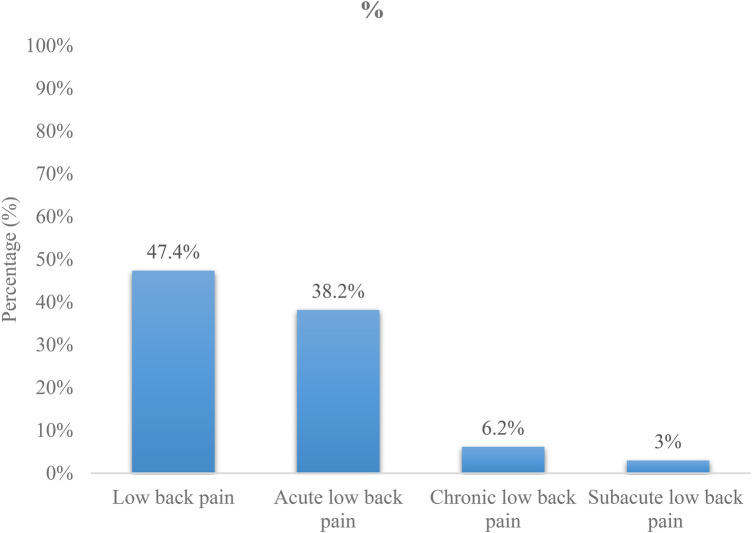 Figure 1
Figure 1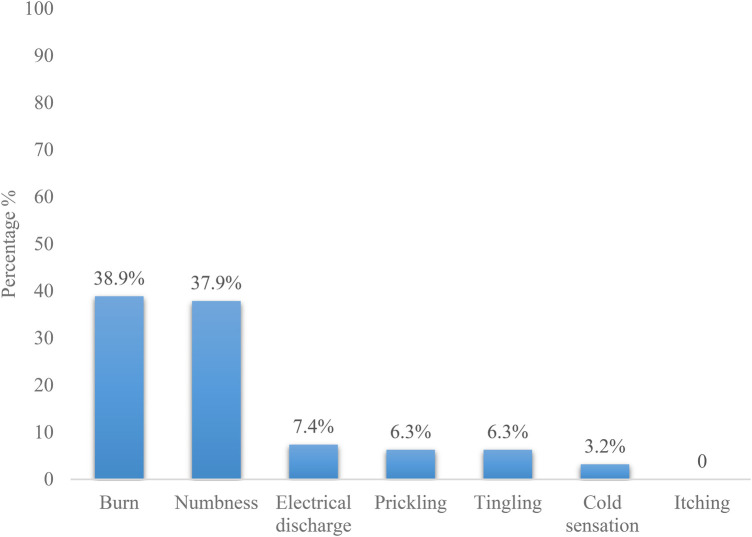 Figure 2
Figure 2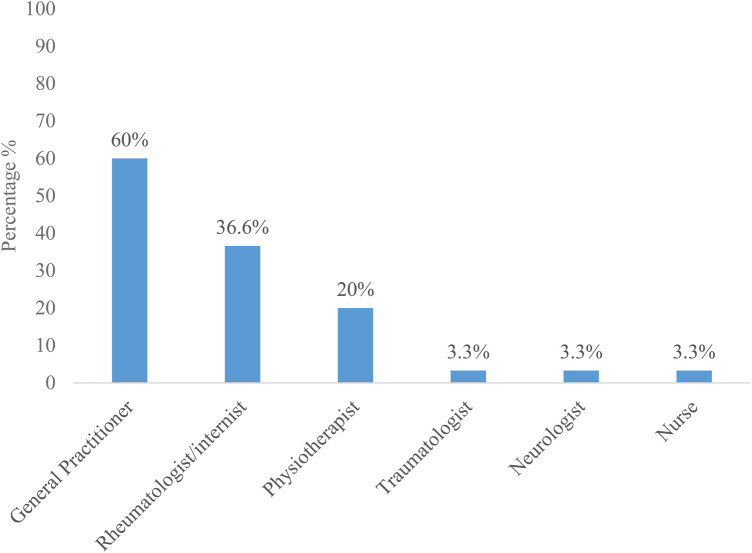 Figure 3
Figure 3| Variables | Number ( | Percentage |
|---|---|---|
| Gender | ||
| Female | 857 | 55.7 |
| Male | 682 | 44.3 |
| Age range | ||
| <20 | 28 | 29.5 |
| 20–24 | 56 | 58.9 |
| 25–29 | 9 | 9.5 |
| >30 | 2 | 2.1 |
| Faculties | ||
| FS | 470 | 30.5 |
| FEMS | 298 | 19.4 |
| FLSS | 257 | 16.7 |
| FLPS | 242 | 15.7 |
| FAAS | 149 | 9.7 |
| FMPS | 123 | 8.0 |
| Study level | ||
| L1 | 421 | 27.4 |
| L2 | 512 | 33.3 |
| L3 | 352 | 22.9 |
| M1 | 135 | 8.8 |
| M2 | 119 | 7.7 |
| Nationality | ||
| Cameroonian | 1,388 | 90.2 |
| Chadian | 142 | 9.2 |
| Gabonese | 5 | 0.3 |
| Ivoirian | 3 | 0.2 |
| Nigerian | 1 | 0.1 |
| Marital status | ||
| Single | 1,511 | 98.1 |
| Married | 26 | 1.7 |
| Widower/widow | 1 | 0.1 |
| Divorced | 1 | 0.1 |
| Type of housing | ||
| In a room | 824 | 53.5 |
| In a family home | 485 | 31.5 |
| In a shared accomodation | 152 | 9.9 |
| In an apartment | 78 | 5.1 |
| University domitory | 3 | 0.2 |
| Presence of electricity at home | 1,519 | 98.7 |
| Presence of flowing water at home | 1,168 | 75.9 |
| Variables | Number in a studying | Number of students with | Frequency (%) |
|---|---|---|---|
| Gender | |||
| Female | 857 | 52 | 6.1 |
| Male | 682 | 43 | 6.3 |
| Age range | |||
| <20 | 537 | 28 | 5.2 |
| 20–24 | 900 | 56 | 6,2 |
| 25–29 | 90 | 9 | 10 |
| >30 | 12 | 2 | 16.6 |
| Faculties | |||
| FEMS | 298 | 22 | 7.3 |
| FS | 470 | 20 | 4.2 |
| FAAS | 149 | 17 | 11.5 |
| FMPS | 123 | 16 | 13 |
| FLPS | 242 | 11 | 4.5 |
| FLSS | 257 | 9 | 3.5 |
| Study level | |||
| L1 | 421 | 11 | 2.6 |
| L2 | 512 | 33 | 6.4 |
| L3 | 352 | 30 | 8.5 |
| M1 | 135 | 15 | 11.1 |
| M2 | 119 | 6 | 5 |
| Marital status | |||
| Single | 1,511 | 93 | 6.1 |
| Married | 26 | 2 | 7.7 |
| Nationality | |||
| Cameroonian | 1,388 | 84 | 6 |
| Chadian | 142 | 11 | 7.7 |
| Type of housing | |||
| In a room | 824 | 51 | 6.1 |
| In a family home | 485 | 30 | 6.2 |
| In an apartment | 78 | 7 | 8.9 |
| In a shared accommodation | 152 | 7 | 4.6 |
| Presence of electricity at home | 1,519 | 95 | 6.2 |
| Flowing water | 1,168 | 66 | 5.6 |
| Variables | Effective in the studying population ( | Effective of students with chronic low back pain (n) | Percentage (%) |
|---|---|---|---|
| Sitting position occupied in class | |||
| Poor posture | 1,224 | 78 | 6.4 |
| Good posture | 315 | 17 | 5.4 |
| Mean lasting lessons per day | |||
| <6h | 1,022 | 56 | 5.5 |
| >6h | 517 | 39 | 7.5 |
| Type of sit | |||
| Bench with backrest | 1,214 | 75 | 6.1 |
| Bench without backrest | 196 | 16 | 8.1 |
| Individual chair | 122 | 5 | 4.1 |
| Type of bag [ | |||
| Hand bag | 538 | 38 | 7.1 |
| Bagpack | 606 | 30 | 4.9 |
| Document holder, folder or binder | 117 | 14 | 11.9 |
| Shoulder bag | 208 | 10 | 4.8 |
| Physical ability | |||
| No | 561 | 36 | 6.4 |
| 3–4/weeks | 847 | 51 | 6 |
| 4–7/weeks | 131 | 8 | 6.1 |
| Competitive sports | 278 | 16 | 5.7 |
| Different competitive sports practiced [ | |||
| Football | 169 | 8 | 4.7 |
| Basket-ball | 28 | 3 | 10.7 |
| Gymnastics | 16 | 2 | 12.5 |
| Athletism | 26 | 1 | 3.8 |
| Volleyball | 21 | 1 | 4.8 |
| Tennis | 13 | 1 | 7.7 |
| Dance | 22 | 1 | 4.5 |
| Judo | 4 | 1 | 25 |
| BMI | |||
| Normal BMI | 1,065 | 59 | 5.5 |
| Overweight | 354 | 25 | 7.1 |
| Obesity | 68 | 6 | 8.8 |
| Insufficient mass index | 52 | 5 | 9.6 |
| Means of transport | |||
| By foot | 1,132 | 70 | 6.1 |
| By bike | 378 | 25 | 6.5 |
| Average walking time | |||
| <15 min | 186 | 5 | 2.7 |
| 15–30 min | 681 | 51 | 7.4 |
| 30–45 min | 360 | 24 | 6.6 |
| 45–60 min | 179 | 13 | 7.3 |
| >1h | 127 | 2 | 1.6 |
| Usage of stairs | 1,168 | 76 | 6.5 |
| Place to borrow the stairs | |||
| Room/House | 232 | 17 | 7.3 |
| Class room | 489 | 29 | 5.9 |
| Both | 447 | 30 | 6.6 |
| Smoking | 230 | 11 | 4.8 |
| Alcohol consumption | |||
| Always | 36 | 4 | 10.8 |
| Often | 235 | 9 | 3.8 |
| Sometimes | 338 | 29 | 8.6 |
| Rarely | 541 | 40 | 7.3 |
| Never | 383 | 13 | 3.4 |
| Past history of low back pains in parents | 708 | 60 | 8.5 |
| Deformation of the lower limbs | 26 | 1 | 3.8 |
| Characteristics | Number ( | Frequency (%) |
|---|---|---|
| Intensity of the pains [ | ||
| None | 1 | 0.1 |
| Mild | 336 | 46.2 |
| Moderate | 327 | 45.0 |
| Severe | 63 | 8.7 |
| [ | ||
| Load lifting efforts | 34 | 39.5 |
| Spontaneously | 34 | 39.5 |
| Flexion and extension | 19 | 22.1 |
| Flexion | 15 | 17.4 |
| Extension | 6 | 7.0 |
| Releaving factors [ | ||
| Lying position | 66 | 76.7 |
| Drugs | 24 | 27.9 |
| Massage at home | 23 | 26.7 |
| Sit position | 14 | 16.3 |
| Physiotherpy | 6 | 7.0 |
| Score | Effective ( | Percentage (%) |
|---|---|---|
| None (0) | 15 | 15,8 |
| Mild (1–6) | 61 | 64,2 |
| Moderate (7–14) | 19 | 20 |
| Severe (>14) | 0 | 0 |
| Variables | Chronic low back pain present | Low back pains absent | Crude OR | Adjusted OR | ||
|---|---|---|---|---|---|---|
| Body mass index | ||||||
| Normal BMI | 59 (65.6) | 146 (78.1) | Ref | |||
| Overweight/obesity | 31 (34.4) | 41 (21.9) | ||||
| Parental past history of low back pains | ||||||
| Yes | 60 (63.2) | 78 (41.1) | ||||
| No | 35 (36.8) | 112 (58.9) | ||||
| Physical activity | ||||||
| Yes | 59 (62.1) | 126 (66.3) | 0.83 (0.49–1.39) | 0.483 | 0.86 (0.49–1.49) | 0.594 |
| No | 36 (37.9) | 64 (33.7) | ||||
| Posture | ||||||
| Poor | 78 (82.1) | 146 (76.8) | 1.38 (0.74–2.58) | 0.307 | 1.24 (0.64–2.41) | 0.521 |
| Good | 79 (17.9) | 44 (23.2) | ||||
| The ergonomics of bench tables | ||||||
| Poor | 16 (16.8) | 28 (14.7) | 0.85 (0.43–1.66) | 0.643 | 1.06 (0.51–2.23) | 0.867 |
| Good | 79 (93.2) | 162 (85.3) | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal pain and rehabilitation · Occupational Health and Performance · Ergonomics and Musculoskeletal Disorders
Background
1
Low back pain (LBP) is widely recognized as one of the most prevalent musculoskeletal conditions and the main cause of years lived with disability worldwide (1, 2). LBP affects individuals of all ages and leads to significant physical, psychological and socioeconomic burdens (1, 3, 4). Although it was traditionally considered to be more prevalent among older adults, recent studies have highlighted its growing prevalence among young individuals, including schoolchildren (5–7). This epidemiological shift has drawn increased attention to the early onset of LBP (1).
In the student population, LBP poses unique challenges. Female gender, obesity, smoking, lifestyle changes, lack of physical activity, parental history of LBP, carrying heavy loads, higher education, academic stress, depressive symptoms, chronic fatigue, prolonged sitting during lectures or study sessions, poor posture, and improper ergonomics characteristics of benches and tables are all suspected to contribute to its development (8–35). If left unaddressed, acute LBP in students can impair academic performance and predispose individuals to lifelong disability and a poor quality of life (8). Despite LBP being increasingly recognized among students, comprehensive data on its prevalence and associated factors remain limited, particularly among those with chronic LBP (CLBP) lasting more than twelve weeks (9–13), and in certain educational contexts and regions, especially in Africa (14–17).
In Cameroon, LBP is believed to affect nearly half of patients seen in Rheumatology clinics (34). A study of 1,075 schoolchildren aged 8–14 years found a prevalence of 12.3% (7). To the best of our knowledge, no research has yet assessed the prevalence of LBP among university students in Cameroon. Furthermore, no published studies on LBP among students in Africa (13–16) have focused specifically on CLBP. Specifically, while some studies conducted among people living with lower back pain have assessed quality of life, to our knowledge, none have been conducted on students with lower back pain (3). One particular issue is the ergonomics of the structures in which students evolve. This study aims to assess the prevalence of CLBP among students and identify socio-demographic, environmental, and clinical factors associated with its onset. By shedding light on these aspects, the study will inform health promotion efforts and policy-making aimed at improving student well-being and academic outcomes.
Patients and methods
2
Study design
2.1
This was a descriptive cross-sectional survey with a nested case-control component involving students at the University of Dschang. The descriptive component aimed to determine the prevalence of CLBP, which is typically defined as pain in the posterior aspect of the body from the lower margin of the 12th ribs to the lower gluteal folds, with or without pain referred into one or both lower limbs, and lasting more than 12 weeks (1). The case-control component was designed to investigate the determinants of chronic LBP in students at the University of Dschang.
Study site
2.2
The study took place on the main campus of the University of Dschang, in the West Region of Cameroon, which has six faculties and two institutes. These are the Faculty of Letters and Social Sciences (FLSS), Faculty of Economics and Management Sciences (FEMS), Faculty of Law and Political Sciences (FLPS), Faculty of Sciences (FS), Faculty of Agronomy and Agricultural Sciences (FAAS), Faculty of Medicine and Pharmaceutical Science (FMPS), and the Fotso Victor's University Institute of Technology (FV-UIT) in Bandjoun and the Institute of Fine Arts in Foumban (IFAF). In 2023, the institution had 19,971 students supervised by several research, teaching, and non-teaching staff.
Duration and period of the study
2.3
The study took place from October 2023 to May 2024, i.e., over a period of 1 year and 7 months. Data collection took place between the 1st November 2023 and the 28th February 2024.
Study population and targeted group
2.4
The source population was any student regularly enrolled at the University of Dschang, whose faculty is based on the main campus in Dschang, for the 2023–2024 academic year, in the bachelor's or master's cycle.
For the descriptive component, all students who consented to participate in the study were included, and all students who withdrew their consent during the study were excluded.
For the analytical part, the cases were students with CLBP. Students without LBP were also included as controls. Any student who participated in the study and had chronic LBP was included as a case, and any student who participated in the study but did not have LBP was included as a control. Matching was done by age and sex.
Study size
2.5
The initial sample size for the descriptive component was 184 participants, calculated using a prevalence of 12.0% among secondary schoolchildren and adolescents, a 95% confidence interval (CI) with a precision of 5%, and a non-respondent rate of 10%. Given that the prevalence of CLBP in our study population is very low, at 12.4% (7, 36). We chose to increase the size of our initial sample. This meant that in order to have 70 cases of chronic LBP for the analytical component calculated using the Schlesselman formula (with Zα/2: 95%; α: 0.05; Zβ of 0.84 for a power of 80% and the ratio = 2:1), we needed a minimum of 688 participants for the descriptive component.
Procedures
2.6
After obtaining approval from the Vice-Chancellor of the University of Dschang and the Regional Human Health Ethics Committee, we conducted a random cluster sampling of our participants. First, in all the faculties on the main campus (FLSS, FLPS, FS, FAAS and FMPS), we randomly selected five departments within each of these faculties. The initial contact was made via a telephone call to the department representatives to explain the study and request their assistance with the field visits. We then consecutively visited the rooms (clusters), each representing a single level of study within a specific program in each department, based on their indicated availability. Visits, generally, took place during students' free time or breaks. Within each room, we surveyed as many students as were willing to participate, within the limits of the allocated period. We repeated this process in each faculty until the desired number of students was reached. Participants were asked to complete the questionnaire truthfully and honestly to minimise information bias. Priority was given to the health of the participants.
Data collection tools and variables
2.7
An online, well-structured self-report questionnaire was developed based on the results of various pilot articles aligned with our research topic and was validated by medical researchers’ expertise to specifically meet the research objectives. It was also pre-tested. Data was collected through face-to-face interviews, each lasting 15 min. During these interviews, weight and height were measured using the same ultra-slim electronic scale and measuring rod.
The dependent variable was chronic LBP (pain located between the lower margins of the 12th rib and the gluteal folds, persisting for more than 12 weeks) and the independent variables were:
- -overweight/obese (BMI greater than 25 kg/m^2^ of body surface),
- -physical inactivity (physical activities less than 60 min per day; according to Anses's definition),
- -parental history of LBP (history of LBP in one or both parents),
- -poor posture in class;
- -and poor ergonomics of desks. The French version of the Roland-Morris Disability Questionnaire – RMDQ (36) was used to assess the functional disability related to CLBP. It comprises 24 questions on the impact of low back pain on physical activities of daily living. Each question corresponds to 1 point, giving a total score of 24 points. The higher the score, the worse the quality of life and the greater the impact.
Statistical analysis
2.8
Data were analyzed using IBM Statistical Package for the Social Sciences®, v.20.0. Categorical variables were presented in terms of numbers and frequencies, while quantitative variables were presented in terms of mean ± standard deviation or median [interquartile range] and extremes. The Chi-square test was used to determine the association between the qualitative variables. Associations between low back pain and relevant categorical variables were assessed using the Pearson chi-square test for independence of observations, the Fisher exact test and the Fisher-Freeman-Halton exact test. Associations between low back pain and ordinal variables were performed using the Cochran-Armitage test for trend. Binomial logistic regression and linear regression analyses were employed to assess the independent factors affecting low back pain. Variables at p ≤ 0.25 in univariate analysis were entered into multiple logistic regression. The threshold for significance was p < 0.05 in multiple logistic analysis.
Results
3
Characteristics of the study population
3.1
A total of 1,780 students were approached, of whom 1,645 agreed to take part in the study, representing a response rate of 92.4%. However, 106 were excluded for incomplete responses. Finally, 1,539 (93.5%) fully participated in the study and were included in the analysis.
Of the 1,539 students included in the study, 857 (55.7%) were female. The median age was 20 years [9–22], with the extremes of 16–34 years. The 20–24 age group was the most represented, at 58.5%. In terms of faculties and levels, our study population consisted mainly of students from the Faculty of Science, 470 (30.5%), followed by the Faculty of Economics and Management, 298 (19.4%). The Faculty of Medicine and Pharmaceutical Sciences was the least represented, with 123 (8%). The L2 level was the most represented, with 512 (33.3%). The M2 level was in the minority: 119 (7.7%). Almost all the students in our study were of Cameroonian nationality: 1,388 (90.2%). Chad was the most represented foreign nationality, with 142 (9.2%). Almost all of our students were single, 1,511 (98.1%), and only 26 (1.7%) were married. The majority, 821 (53.3%) of our participants, lived in studios (Table 1).
Prevalence and distribution of chronic low back pain among students
3.2
At the end of our study, 726 of the 1,539 students included, i.e., 47.2% [95% CI: 44.7–49.6], had had at least one episode of LBP in their lifetime. Of the 1,539 students included, 95 [6.2% (95% CI: 5.0–7.3)] had CLBP. Five hundred and eighty-five students [38% (95% CI: 35.3–40.5)] had acute LBP, and 46 [3% (95% CI: 2.1–3.9)] had subacute LBP (Figure 1).
Low back pain prevalence and distribution in the study population.
Table 2 shows the distribution of students with CLBP by socio-demographic characteristics. The majority of students with CLBP were male (6.3%). Their median age was 21 [19–23] years, with extremes of 17 and 30. According to the faculties, 16 (13%) of the students suffered from LBP in the Faculty of Medicine and Pharmaceutical Sciences.
Table 3 shows the distribution of students with chronic LBP according to clinical characteristics and lifestyle. Over 6.4% of the students with poor posture in class had chronic LBP. Thirty-nine (7.5%) of the students taking classes for more than 6 h a day had chronic LBP.
Clinically, weight ranged from 50 to 104 Kg, with a median of 68.1 Kg [60–75]. Of the students with a high BMI, 31 (15.9%) had chronic LBP. And among those with a parental history of LBP, 60 (8.5%) also had chronic LBP.
Chronic LBP was expressed in 45.3% of cases as mechanical LBP. It radiated to the buttocks and lower limbs in 20% of cases. The pain was intermittent in 64.2% of cases, permanent in 22.1% and a single episode in 13.7% of cases. Pain was described as burning in 38.9% (n = 37) and numbness in 37.9% (n = 36) (Figure 2).
Student's distribution according to the type of Low back pain.
The effort of lifting a load was the triggering factor for LBP in 39.5% of cases (n = 34). Lying down relieved the pain in 76.7% of cases (n = 66). Pain intensity was classified as mild, according to the numerical pain scale (NPS), in 46.2% of cases (Table 4).
The student was forced to interrupt academic activities in 57.9% of cases. The number of days of interruption of academic activities ranged from 1 day to 38 days, with a median of 3 days [1–4]. Of the 95 students suffering from chronic LBP, 30 (31.6%) had sought medical advice. Of these, 60% had consulted a general practitioner and 36% a rheumatologist (Figure 3).
Student's distribution suffering of chronic low back pains according to the health personnel demanded in consultation.
Quality of life of students with chronic low back pain
3.3
Ninety-five students with chronic LBP completed the Roland-Morris questionnaire on quality of life with chronic LBP. The score ranged from 0 to 12, with a median of 4 and an interquartile range of 1–6. Most students with chronic LBP obtained a score of 1–6 (64.2%), followed by 7–14 (20%), then 0 (15.8%). No student obtained a score higher than 14 (Table 5).
Factors associated with chronic low back pain in students
3.4
Bivariate analysis showed that being overweight/obese (p = 0.026) and having a parental history of LBP (p < 0.001) were significantly associated with chronic LBP. Overweight or obese students were 1.87 times more likely to have chronic LBP than those with a normal BMI. Students with a family history of LBP were 2.46 times more likely to have chronic LBP.
After adjustment for confounding factors (type of course, parental history of LBP for the overweight/obesity factor; type of course and overweight/obesity for the parental history of LBP factor), being overweight/obese [ORa = 1.82 (95% CI: 1.02–3.24); p = 0.041], as well as having a parental history of LBP [ORa = 2.6 (95% CI: 1.53–4.43); p < 0.001] remain significantly associated with chronic LBP. Unexpectedly, the following factors were not associated with the development of chronic LBP in our study population: physical inactivity; poor posture in the classroom; and poor ergonomics of bench tables (Table 6).
Discussion
4
The three specifics objectives of this cross-sectional study with a nested case-control component were 1) to determine the prevalence of CLBP, 2) to assess the quality of life of students with CLBP, and 3) to examine whether factors such as overweight/obesity, physical inactivity, parental history of LBP, poor posture, and poor bench ergonomics increase the risk of CLBP among students at the University of Dschang. The current study showed that 47.2% of participants reported LBP, while 6.2% experienced CLBP. Surprisingly, no gender differences were observed among students with CLBP. Of these individuals, two-thirds scored a low score on the Roland-Morris Disability Questionnaire. Only a third of students with CLBP had consulted a healthcare professional about it. Having a parental history of LBP and being overweight or obese were independently associated with CLBP.
To the best of our knowledge, this is the first study to examine the characteristics of CLBP in students in Cameroon. Unlike previous studies, this study specifically evaluated specifically students with CLBP. The prognosis for acute LBP is generally purported to be favourable. However, this is not the case for chronic low back pain, which can lead to disability (1, 2). This survey is also one of the few studies (6, 30–34), not focus solely on health sciences students. Indeed, most published studies on LBP among students have included only medical, nursing and physiotherapy students (8–29). The rigorous random sampling technique employed and the size of the sample obtained are also some strengths of this study. However, this study has some limitations that must be taken into account when interpreting the results. Firstly, due to the cross-sectional design, it is not possible to conclude that there is a causal link between CLBP and BMI or parental history of LBP. Secondly, the single-centre design of the study may limit the generalizability of the results. Nevertheless, this remains possible given that the University of Dschang is a cosmopolitan institution, attracting students from all regions of Cameroon and eleven other African countries. Thirdly, a clinical examination by a physician would have provided a precise medical diagnosis for each student and yielded more qualitative data on their pain experience. This would have enabled us to identify other pain locations, such as neck pain and shoulder pain (4, 28–30). In this study, trained interviewers ensured that the anatomical areas indicated by the students corresponded to the lumbar region. As pain is the main characteristic of LBP, this survey is sufficient for an accurate LBP diagnosis. Fourthly, we did not sufficiently consider the psychological aspects of LBP in students. It was assessed indirectly using the RMDQ (35), designed to measure the impact of CLBP on patients' daily activities. However, we did not find a significant association between these factors and CLBP. Further studies assessing the clinical, radiological and psychological characteristics of CLBP in students in SSA would be interesting. Finally, it would be interesting to conduct a follow-up study with these students to assess how their low back pain evolves during their professional lives.
Many studies assessed LBP in Cameroon before. However, most of them targeted either healthcare workers or schoolchildren. None of them specifically targeted students or investigated the impact on quality of life. Unlike the data found in older people, there is no difference between men and women among students. The main factors identified are overweight/obesity and a family history of LBP. However, we did not explore the impact of stress and anxiety on CLBP (7, 37, 38).
Based on our data, and despite the limitations of the study, policymakers should consider CLBP as a public health issue affecting also young adults, including students. Risk factors significantly associated with CLBP (8–34), particularly the factors identified in our study, should be incorporated into algorithms for the prevention and treatment of LBP. Ergonomic facilities should be included in ergonomics programs developed for students, taking into consideration the type of training. In this study, the level of disability was mild, but this was in contrast to the high number of students who had interrupted their academic activities due to LBP compared to data from other countries (9). Previous research shows that fewer than one in four students with low back pain seek formal medical advice, highlighting possible barriers to accessing healthcare or a low perception of the severity of the condition (16, 19, 21, 33). The high consultation rate observed in our study could be explained by the fact that all University of Dschang students have health insurance, and by the proximity of two university hospitals staffed by experienced medical professionals. The reduced impact on quality of life observed in our study could be explained by rapid and effective treatment.
Further rigorous studies should be conducted to assess the impact of the triggering or aggravating factors of LBP identified, such as carrying heavy loads, flexion and extension movements, long sitting sessions, stress and poor sleeping position (11, 25). Similarly, investigating the effect of weight reduction on the prevention of LBP could help to establish a cause-and-effect relationship between CLBP and BMI.
Conclusion
5
CLBP is common in university settings. It affects one in fifteen students in a Cameroonian university. However, CLBP does not significantly impact the quality of life of these students. Factors associated with CLBP in this study were parental history of LBP and overweight/obesity. However, physical inactivity, poor posture in class, and poor bench ergonomics were not associated with CLBP in this study. We suggest that preventive measures, such as ergonomic facilities and psychosocial supports, must be taken in young adults, as in childhood, to prevent the occurrence of CLBP and its persistence into adulthood. Our findings support the need for further research to improve the understanding of LBP in students.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD 2021 Low Back Pain Collaborators. Global, regional, and national burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Rheumatol. (2023) 5(6):e 316–29. 10.1016/S 2665-9913(23)00098-X 37273833 PMC 10234592 · doi ↗ · pubmed ↗
- 2Hoy D March L Brooks P Blyth F Woolf A Bain C The global burden of low back pain: estimates from the global burden of disease 2010 study. Ann Rheum Dis. (2014) 73(6):968–74. 10.1136/annrheumdis-2013-20442824665116 · doi ↗ · pubmed ↗
- 3Aminde JA Aminde LN Bija MD Lekpa FK Kwedi FM Yenshu EV Health-related quality of life and its determinants in patients with chronic low back pain at a tertiary hospital in Cameroon: a cross-sectional study. BMJ Open. (2020) 10(10):e 035445. 10.1136/bmjopen-2019-03544533028543 PMC 7539580 · doi ↗ · pubmed ↗
- 4Doualla M Aminde J Aminde LN Lekpa FK Kwedi FM Yenshu EV Factors influencing disability in patients with chronic low back pain attending a tertiary hospital in sub-Saharan Africa. BMC Musculoskelet Disord. (2019) 20(1):25. 10.1186/s 12891-019-2403-930646894 PMC 6334448 · doi ↗ · pubmed ↗
- 5BalaguéF Troussier B Salminen JJ. Non-specific low back pain in children and adolescents: risk factors. Eur Spine J. (1999) 8(6):429–38. 10.1007/s 00586005020110664299 PMC 3611213 · doi ↗ · pubmed ↗
- 6Swain MS Henschke N Kamper SJ Gobina I Ottová-Jordan V Maher CG. An international survey of pain in adolescents. BMC Public Health. (2014) 13(14):447. 10.1186/1471-2458-14-447PMC 404651324885027 · doi ↗ · pubmed ↗
- 7Kemta Lekpa F Enyama D Noukeu Njinkui D Ngongang Chiedjio A Simeni Njonnou SR Ngongang Ouankou C Prevalence and factors associated with low back pain in schoolchildren in Cameroon, sub-Saharan Africa. Int J Rheum Dis. (2021) 24(9):1186–91. 10.1111/1756-185X.1417234235853 · doi ↗ · pubmed ↗
- 8Shekhar S Rao R Nirala SK Naik BN Singh C Pandey S. Prevalence of acute low back pain with risk of long-term disability and its correlates among medical students: a cross-sectional study. J Educ Health Promot. (2023) 12:179. 10.4103/jehp.jehp_1460_2237404938 PMC 10317279 · doi ↗ · pubmed ↗