Case Report: High-altitude exposure and severe respiratory infection precipitating diabetic ketoacidosis: new-onset ketosis-prone diabetes unmasked by physiological stress
Killen H. Briones-Claudett, Jaime Benites-Solis, Patricia Delgado-Cedeño, Fabián Alfonso Ortiz-Herbener, Anahí D. Briones-Zamora, Diana C. Briones-Márquez, Michelle Grunauer, Killen H. Briones-Zamora

TL;DR
A woman developed diabetic ketoacidosis after high-altitude travel and a severe lung infection, revealing a previously undiagnosed form of diabetes.
Contribution
This case introduces a new-onset ketosis-prone diabetes unmasked by combined high-altitude and infectious stress.
Findings
High-altitude exposure and respiratory infection can trigger DKA in individuals with undiagnosed chronic dysglycemia.
Multiplex PCR detected multiple pathogens, but interpretation required clinical correlation due to potential colonization.
The patient exhibited A−β+ ketosis-prone diabetes, with full recovery of pulmonary function within 6 months.
Abstract
Diabetic ketoacidosis (DKA) may represent the first presentation of previously unrecognized diabetes, with acute environmental and infectious stressors lowering the threshold for ketoacidosis. High-altitude hypoxia can impair glucose homeostasis and host defenses, potentially predisposing to severe respiratory infections. A previously undiagnosed 28-year-old woman from sea level developed DKA 1 week after returning from a 5-day trip to Cusco, Peru (3,400 m). She presented with altered mental status, Kussmaul breathing, and severe metabolic acidosis (pH 7.09, glucose 548 mg/dL, bicarbonate 6.1 mmol/L, anion gap 26 mEq/L) in the setting of progressive respiratory symptoms and hypoxemia. Chest CT showed multifocal consolidations with cylindrical bronchiectasis and air trapping. Bronchoscopy with bronchoalveolar lavage revealed thick purulent secretions, and multiplex PCR identified…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
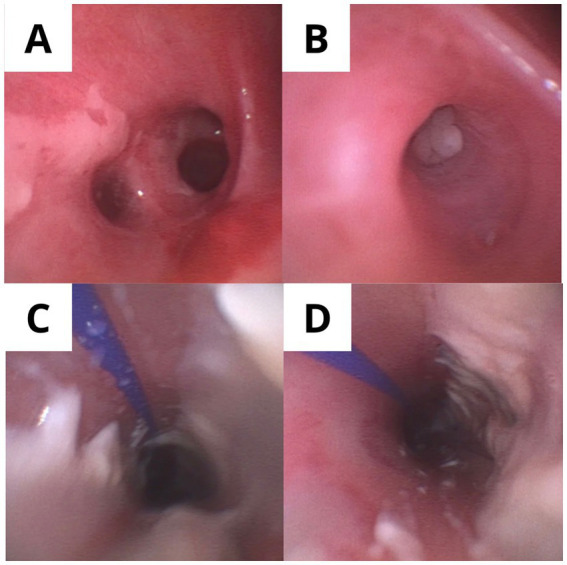 Figure 1
Figure 1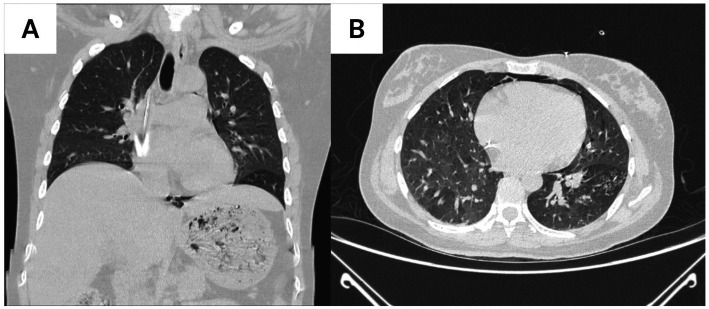 Figure 2
Figure 2| Time point | Clinical event | Key laboratory/imaging findings | Diagnostic procedures | Therapeutic interventions |
|---|---|---|---|---|
| Day 0 (Admission) | ED presentation: altered mental status, tachypnea, dehydration | pH 7.09, glucose 548 mg/dL, AG 26 mEq/L, HCO₃⁻ 6.1 mmol/L, HbA1c 9.0%, WBC 17,890/μL, CRP 25.3 mg/L, SpO₂ 89% RA | – | ICU admission; DKA protocol: 1-L 0.9% NaCl bolus, then 250–300 mL/h; IV insulin 0.1 U/kg/h; High-flow O₂ |
| Hour 6 | Progressive respiratory failure | PaO₂/FiO₂ < 200, RR 35/min, increasing work of breathing | – | Endotracheal intubation; MV (TV 6 mL/kg, PEEP 8, FiO₂ 0.6) |
| Hour 28 | Metabolic improvement | pH > 7.30 achieved, HCO₃⁻ 14.2 mmol/L | – | Continue IV insulin + dextrose-containing fluids; Transition to balanced crystalloids (Ringer’s lactate) |
| Hour 36 | Anion gap closure | AG ≤ 12 mEq/L, HCO₃⁻ 16 mmol/L, glucose 180 mg/dL | – | Plan transition to subcutaneous insulin |
| Day 2 (ICU day 2) | Bronchoscopy performed | Chest CT: multifocal consolidations, bronchiectasis, air trapping (left lower lobe) | BAL: Multiplex PCR: parainfluenza, rhinovirus, | Antibiotics: cefuroxime 750 mg IV q8h + clindamycin 600 mg IV q8h; Fluconazole 400 mg IV daily initiated |
| Day 3 | Insulin transition | Oral intake tolerated, ketones cleared, glucose 140–180 mg/dL | Diabetes autoantibodies: GAD65 (−), IA-2 (−), ZnT8 (−); C-peptide 2.1 ng/mL | Subcutaneous basal-bolus insulin (glargine 10 U qHS + lispro 4 U pre-meals) |
| Day 4 | Successful extubation | SpO₂ 96% on 2 L NC, RR 18/min, hemodynamically stable | – | Transfer to step-down unit; Continue antibiotics/fluconazole |
| Day 7 | ICU discharge | Clinically stable, afebrile, glucose 100–150 mg/dL | – | Transfer to general medical ward |
| Day 14 | Hospital discharge | Antibiotics/fluconazole completed (14 days each) | – | Discharge on insulin: glargine 8 U qHS + lispro 3 U pre-meals |
| Day 18 | – | Repeat chest CT: complete resolution of consolidations | – | – |
| 1 Month | Follow-up visit | HbA1c 7.2%; PFTs: DLCO 70%, mild restriction | Pulmonary function testing | Insulin dose reduced: glargine 6 U qHS + lispro 2 U pre-meals |
| 3 Months | Follow-up visit | HbA1c 6.1%, fasting glucose 100–110 mg/dL | – | Further insulin taper: glargine 4 U qHS + lispro 1 U pre-meals |
| 5 Months | Insulin discontinuation | HbA1c 5.6%, fasting glucose 90–100 mg/dL, PPG < 140 mg/dL on CGM | Continuous glucose monitoring | Insulin discontinued; Diet + exercise management |
| 6 Months | Follow-up visit | PFTs normalized: DLCO 99%, TLC 97%; VE/VCO₂ 30 | Pulmonary function + cardiopulmonary exercise testing | Continue lifestyle modifications |
| 8 Months | Metabolic phenotyping | HbA1c 5.4%; OGTT: fasting 92 mg/dL, 2-h 130 mg/dL (normal tolerance) | 75-g oral glucose tolerance test | Diagnosis: ketosis-prone diabetes with remission confirmed |
| Parameter | Reference range | 1 month post-discharge | 6 months post-discharge | Interpretation |
|---|---|---|---|---|
| Spirometry | ||||
| FVC (L) | 3.2–4.5 | 2.8 (78% predicted) | 3.9 (95% predicted) | Complete recovery of lung volumes |
| FEV₁ (L) | 2.8–3.9 | 2.4 (76% predicted) | 3.5 (94% predicted) | Resolution of restrictive pattern |
| FEV₁/FVC ratio | >0.70 | 0.86 | 0.90 | No obstructive component at any time point |
| Lung volumes | ||||
| TLC (L) | 4.5–6.0 | 4.2 (82% predicted) | 5.3 (97% predicted) | Normalization of total lung capacity |
| RV (L) | 1.2–1.8 | 1.4 (89% predicted) | 1.5 (94% predicted) | Normal residual volume throughout |
| Gas exchange | ||||
| DLCO (mL/min/mmHg) | 20–30 | 14.8 (70% predicted) | 21.2 (99% predicted) | Marked improvement in diffusion capacity |
| DLCO/VA | 4.0–6.0 | 3.2 | 4.8 | Resolution of alveolar-capillary impairment |
| Exercise testing | ||||
| Peak VO₂ (mL/kg/min) | >25 | 18.4 (65% predicted) | 26.8 (94% predicted) | Restoration of aerobic capacity |
| VE/VCO₂ slope | 25–35 | 35 | 30 | Improved ventilatory efficiency |
| Peak HR (bpm) | 190–195 | 168 | 188 | Normal chronotropic response at 6 months |
| SpO₂ at peak (%) | >95 | 94 | 98 | No exercise-induced desaturation at 6 months |
| Investigation category | Timing | Key findings | Clinical significance |
|---|---|---|---|
| Initial laboratory assessment | Day 0 (admission) | pH 7.09, glucose 548 mg/dL, AG 26 mEq/L, HbA1c 9.0%, WBC 17,890/μL, CRP 25.3 mg/L | Confirmed severe DKA with marked inflammatory response |
| Diabetes phenotyping | Day 3 | GAD65 (−), IA-2 (−), ZnT8 (−); C-peptide 2.1 ng/mL | Excluded autoimmune type 1 diabetes; preserved endogenous insulin secretion |
| Respiratory imaging | Day 2 | Chest CT: multifocal consolidations, cylindrical bronchiectasis, air trapping (left lower lobe) | Documented severe pneumonia as precipitant |
| Microbiologic diagnosis | Day 2 (BAL) | Multiplex PCR: parainfluenza, rhinovirus, | Confirmed polymicrobial bacterial/viral pneumonia + invasive candidiasis |
| Antimicrobial therapy | Days 2–14 | Cefuroxime + clindamycin × 14 days; Fluconazole 400 mg IV daily × 14 days | Targeted therapy based on stewardship-informed interpretation |
| DKA resolution | Hour 36 | AG ≤ 12 mEq/L, pH > 7.30, HCO₃⁻ 16 mmol/L | Met biochemical criteria for DKA resolution |
| Radiologic follow-up | Day 18 | Chest CT: complete resolution of consolidations | Confirmed radiologic recovery |
| Pulmonary function assessment | 1 month, 6 months | Month 1: DLCO 70%, mild restriction; Month 6: DLCO 99%, all parameters normalized | Documented complete pulmonary recovery |
| Long-term glycemic assessment | 8 months | HbA1c 5.4%; OGTT: fasting 92 mg/dL, 2-h 130 mg/dL (normal) | Confirmed ketosis-prone diabetes with sustained remission |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes and associated disorders · High Altitude and Hypoxia · Travel-related health issues
Introduction
Diabetic ketoacidosis (DKA) is a life-threatening hyperglycemic emergency caused by absolute or relative insulin deficiency, characterized by metabolic acidosis and ketonemia, and most commonly triggered by acute physiologic stress such as infection, dehydration, or trauma (1). DKA may be the first clinical presentation of diabetes in adults, including ketosis-prone diabetes (KPD), in which patients present with DKA but may later achieve glycemic remission as β-cell function recovers (2).
High-altitude hypoxia is associated with complex and heterogeneous changes in glucose homeostasis (3–5). Acute hypobaric hypoxia can increase sympathetic activation and counter-regulatory hormones, worsening insulin resistance and promoting lipolysis and ketogenesis; in susceptible individuals, altitude exposure may therefore unmask previously unrecognized dysglycemia (5, 6). Hypoxia-inducible signaling has also been implicated in impaired pancreatic β-cell function, providing a cellular mechanism that may lower the threshold for ketoacidosis during hypoxic stress (7).
Moreover, high-altitude environments can alter immune cell populations and host defenses, potentially increasing vulnerability to respiratory infections (8). Concomitant viral and bacterial respiratory infections are well-known precipitants of metabolic decompensation and can drive severe systemic inflammation that accelerates ketoacidosis (9, 10). Accordingly, the convergence of hypoxic exposure, dehydration, and severe infection may serve as a catalyst for DKA in individuals with underlying but previously unrecognized chronic dysglycemia (11).
This case presents a unique confluence of factors—recent high-altitude travel, polymicrobial respiratory infection, and sudden onset of DKA—as the first manifestation of a ketosis-prone diabetes phenotype suggested by an elevated admission HbA1c and subsequent remission with preserved endogenous insulin secretion (2, 11). Molecular testing via multiplex PCR supported early etiologic clarification and antimicrobial targeting, allowing for timely resolution of both metabolic and respiratory derangements (12, 13).
Case presentation
A previously healthy 28-year-old woman from Guayaquil, Ecuador (approximately 0 m altitude) presented to the emergency department with altered mental status, tachypnea, and dehydration, 7 days after returning from a five-day trip to Cusco, Peru (3,400 m). While at altitude, she experienced mild cold-like symptoms but remained physically active. Anthropometric measurements at admission revealed a BMI of 24.8 kg/m^2^ and a waist circumference of 78 cm. There was no family history of early-onset diabetes, recurrent ketosis, or other endocrinopathies across multiple generations; although MODY was considered given her age and presentation, the absence of familial clustering, lack of syndromic features, and subsequent glycemic normalization with insulin independence indicated low pre-test probability, and genetic testing was not pursued (14).
After returning to sea level, she developed cough, sore throat, and fever, which progressed over 4 days to polydipsia, polyuria, fatigue, and dyspnea. On presentation, vital signs were: heart rate 122 bpm, respiratory rate 30/min, blood pressure 145/90 mmHg, and SpO₂ 89% on room air. Glasgow Coma Scale was 13/15. Physical examination revealed dry mucosa, reduced skin turgor, and bilateral basal crackles. A systematic evaluation for immune dysfunction was performed; she denied any history of recurrent, severe, unusual, or opportunistic infections and had no known immunodeficiency, no recent corticosteroid exposure, and no immunomodulatory therapy.
Laboratory testing confirmed diabetic ketoacidosis: pH 7.09, glucose 548 mg/dL, bicarbonate 6.1 mmol/L, anion gap 26 mEq/L, and ketonuria. Inflammatory markers were elevated (WBC 17,890/μL, C-reactive protein 25.3 mg/L). HbA1c was 9.0%. Autoimmune antibodies (GAD65, IA-2, ZnT8) were negative, and C-peptide level was preserved at 2.1 ng/mL, consistent with retained endogenous insulin secretion in the setting of acute metabolic decompensation, supporting a ketosis-prone diabetes phenotype rather than autoimmune type 1 diabetes (2).
Chest X-ray was non-revealing. Chest CT on hospital day 2 revealed multifocal consolidations, cylindrical bronchiectasis, and air trapping predominantly in the left lower lobe (Figures 1A–D). She was admitted to the intensive care unit and initiated on high-flow oxygen and protocolized DKA management. DKA management was initiated with a 1-L bolus of 0.9% sodium chloride over the first hour, followed by intravenous fluids at 250–300 mL/h for ongoing volume repletion. After initial stabilization, fluids were transitioned to balanced crystalloids (Ringer’s lactate) to mitigate hyperchloremic metabolic acidosis and support more efficient correction of acid–base derangements, in line with contemporary evidence favoring balanced crystalloids over normal saline in DKA (15). Continuous intravenous insulin infusion was started at 0.1 U/kg/h without an initial bolus, with hourly point-of-care glucose monitoring. Once plasma glucose decreased below 250 mg/dL, dextrose-containing fluids were initiated to permit continued insulin administration until resolution of ketoacidosis. Serum potassium at presentation was 4.2 mmol/L; potassium supplementation (chloride and/or acetate salts) was titrated with 4–6 hourly electrolyte monitoring to maintain serum potassium between 4.0 and 5.0 mmol/L, following current inpatient diabetes care standards (16). Due to respiratory deterioration, endotracheal intubation and mechanical ventilation were required within 6 h.
Chest CT imaging. (A) Day 2: Rounded bilateral consolidations with cylindrical bronchiectasis and air trapping, predominantly in the left lower lobe. (B) Day 18: Resolution of previous findings with normal parenchymal appearance. Serial chest computed tomography demonstrating radiologic evolution. Axial chest CT images in lung window (W: 1,500, L: −600) at the level of the lower thorax. (A) Hospital day 2 (post-intubation): Multifocal rounded consolidations with air bronchograms (white arrow) are visible bilaterally, with predominant involvement of the left lower lobe. Cylindrical bronchiectasis (arrowhead) is present in the basal segments, and mosaic attenuation with air trapping (darker regions) suggests small airway obstruction. These findings, combined with multiplex PCR detection of parainfluenza virus, rhinovirus, Haemophilus influenzae, Staphylococcus aureus, and Moraxella catarrhalis from bronchoalveolar lavage performed on the same day, confirmed severe polymicrobial pneumonia as a major precipitant of diabetic ketoacidosis. (B) Hospital day 18 (pre-discharge): Complete resolution of consolidations with restoration of normal parenchymal architecture and aeration. The radiologic recovery paralleled clinical improvement, with successful extubation on day 4 and ICU discharge on day 7. This favorable evolution demonstrates the reversibility of acute lung injury in the setting of ketosis-prone diabetes with severe infection when appropriate antimicrobial therapy and supportive care are provided. Images were acquired without intravenous contrast due to acute kidney injury at presentation (creatinine 1.4 mg/dL, subsequently normalized). CT protocol: Non-contrast helical CT; slice thickness 1.25 mm; tube voltage 120 kVp; automatic tube current modulation.
Bronchoscopy with bronchoalveolar lavage (BAL) on ICU day 2 showed thick mucus, erythematous mucosa, and purulent secretions. Distinct white, curd-like plaques firmly adherent to the bronchial mucosa were observed, consistent with a pseudomembranous appearance (Figures 2A,B). Multiplex PCR (BioFire RP2plus) identified parainfluenza virus, rhinovirus/enterovirus, Haemophilus influenzae (10^6^ copies/mL), Staphylococcus aureus (>10^7^ copies/mL, high burden), and Moraxella catarrhalis. Candida albicans was cultured. Serum Candida mannan antigen was positive; serum β-D-glucan testing was not available at our institution. Fluconazole was initiated for 14 days based on the endoscopic pseudomembranous lesions and supportive serologic evidence, consistent with reported features of tracheobronchial candidiasis (17, 18).
Bronchoscopic appearance during bronchoalveolar lavage (day 2). (A) Thick purulent secretions obstructing the segmental bronchus of the left lower lobe. (B) Erythematous bronchial mucosa with mucopurulent exudate and adherent whitish, curd-like plaques consistent with a pseudomembranous appearance. Bronchoscopic documentation of severe tracheobronchial inflammation and candidiasis. Fiberoptic bronchoscopic images obtained during bronchoalveolar lavage on ICU day 2. (A) Left lower lobe segmental bronchus showing thick, yellow-green purulent secretions (asterisk) causing partial airway obstruction. The volume and tenacity of secretions necessitated frequent suctioning and contributed to ventilatory difficulty. (B) After partial clearance of secretions, the underlying bronchial mucosa is markedly erythematous and hyperemic, with prominent vascular engorgement consistent with acute inflammation. Distinct white, curd-like plaques (white arrows) are firmly adherent to the mucosa, creating a pseudomembranous appearance characteristic of tracheobronchial candidiasis. These plaques could not be easily removed with gentle suctioning, distinguishing them from superficial secretions. Bronchoalveolar lavage fluid from this segment grew Candida albicans in culture, and serum Candida mannan antigen was positive. This integrated endoscopic and microbiologic evidence supported the diagnosis of invasive Candida tracheobronchitis rather than simple colonization, justifying the initiation of fluconazole therapy (400 mg IV daily for 14 days) in accordance with clinical criteria for tracheobronchial fungal infection in critically ill patients. Bronchoscopy details: Flexible fiberoptic bronchoscopy performed via 7.5 mm endotracheal tube using Olympus BF-1 T180 bronchoscope; BAL performed with 3 × 50 mL aliquots of sterile 0.9% saline in left lower lobe basilar segment; return volume 65 mL (43%); samples sent for bacterial/fungal culture, multiplex PCR (BioFire FilmArray RP2plus Pneumonia Panel), and cytology. BAL, bronchoalveolar lavage; ICU, intensive care unit; IV, intravenous.
Empirical antibiotics were adjusted to cefuroxime and clindamycin. The patient remained on mechanical ventilation (tidal volume 6 mL/kg, PEEP 8 cm H₂O, FiO₂ 0.6) for 96 h. Biochemical resolution was defined using standard criteria (bicarbonate ≥15 mEq/L, pH > 7.30, and anion gap ≤12 mEq/L, with glucose <250 mg/dL while receiving dextrose-containing fluids) (16). The anion gap decreased from 26 mEq/L at presentation to the normal range by approximately 36 h, with pH > 7.30 achieved by hour 28. Intravenous insulin was then transitioned to a subcutaneous basal–bolus regimen after confirmation of anion-gap closure and tolerance of oral intake, using appropriate overlap to prevent rebound ketosis (16). She was extubated and discharged from the ICU on day 7.
She completed a 14-day hospital stay and was discharged on insulin therapy. At one-month follow-up, HbA1c had decreased to 7.2%. Insulin was progressively tapered and discontinued by month five, with HbA1c of 5.6%. Three months after insulin discontinuation, repeat HbA1c was 5.4%, and a 75-g oral glucose tolerance test demonstrated normal glucose tolerance (fasting 92 mg/dL; 2-h 130 mg/dL), supporting metabolic remission and aligning with current recommendations for post-DKA phenotyping with glucose-based testing (19, 20).
Pulmonary function tests at 1 month showed a mild restrictive defect and reduced diffusing capacity for carbon monoxide (DLCO 70%). At 6 months, all parameters had normalized (DLCO 99%). Cardiopulmonary exercise testing revealed a ventilatory equivalent for carbon dioxide (VE/VCO₂) of 35 at 1 month, improving to 30 at 6 months. Key investigations and therapeutic milestones are summarized in Tables 1–3.
Discussion
This case illustrates how severe polymicrobial pneumonia and recent high-altitude exposure can precipitate diabetic ketoacidosis in a patient with previously unrecognized chronic dysglycemia. The coexistence of multiple respiratory pathogens, critical illness, and stress-related metabolic decompensation aligns with the concept that polymicrobial infections in critically ill hosts amplify inflammatory responses and increase the risk of severe systemic complications (21).
High-altitude exposure likely contributed to metabolic vulnerability through multiple mechanisms. Acute hypobaric hypoxia triggers sympathetic nervous system activation and counter-regulatory hormone surges, promoting insulin resistance and enhanced lipolysis with subsequent ketogenesis (3–5). At the cellular level, hypoxia-inducible factor signaling may directly impair pancreatic β-cell function and insulin secretion (7). Additionally, altitude-associated dehydration and altered immune responses may have lowered the threshold for both respiratory infection and ketoacidosis in this patient with underlying but previously unrecognized dysglycemia (6, 8, 11). This case thus exemplifies how environmental stressors can unmask latent metabolic disease through convergent pathophysiological mechanisms.
The broad pathogen spectrum detected by multiplex molecular testing, including respiratory viruses and typical bacterial respiratory pathogens, highlights both the diagnostic power and interpretive challenges of these platforms in lower respiratory tract infections. “Real-world evaluations of the BioFire FilmArray Pneumonia Panel show that it can substantially enhance pathogen detection compared with culture and inform antimicrobial optimization but also emphasize that colonization and upper-airway carriage are frequently detected and must be distinguished from true infection (22–24). Studies of panel performance in lower respiratory tract samples confirm good sensitivity and specificity, yet stress that results require integration with clinical, radiologic, and quantitative data to support stewardship-focused decisions (23).
The persistence and kinetics of respiratory virus detection further complicate interpretation in complex cases like this one. Data on prolonged viral PCR positivity show that nucleic acid from respiratory viruses can remain detectable beyond the period of peak symptoms, particularly in hospitalized patients, meaning that a positive PCR does not always indicate active, causative infection at the time of testing (25). This reinforces the need to prioritize high-burden bacterial targets and the overall clinical syndrome when deciding which organisms to treat in polymicrobial reports (22, 23, 25).
The identification of Candida albicans in bronchoalveolar lavage in an ICU patient with DKA and mechanical ventilation raises the classic dilemma of colonization versus invasive disease. Reviews on invasive candidiasis in the ICU emphasize that Candida isolated from respiratory secretions usually reflects colonization and that antifungal therapy should be reserved for situations with supportive clinical, endoscopic, or serologic evidence of invasive tracheobronchial or parenchymal disease (17). Case series of Candida tracheobronchitis describe pseudomembranous, plaque-like lesions adherent to the bronchial mucosa, often accompanied by systemic or local indicators of fungal infection and favorable responses to antifungal therapy, providing a rationale for targeted treatment in selected patients such as the one presented (18).
Beyond the acute episode, accurate classification and long-term risk assessment are critical in patients whose first presentation of diabetes is DKA. Contemporary standards of care for diagnosis and classification of diabetes underscore that HbA1c alone may miss some forms of dysglycemia and that classification should integrate clinical phenotype, autoantibody status, and, when appropriate, additional testing (19). A systematic review and meta-analysis in stroke populations demonstrates that oral glucose tolerance testing can identify diabetes and impaired glucose regulation that are not detected by HbA1c, supporting the use of OGTT when precise characterization of glucose tolerance is needed, as in suspected ketosis-prone diabetes after metabolic remission (20).
Although the admission HbA1c of 9.0% indicates sustained hyperglycemia over the preceding 8–12 weeks, thereby excluding isolated stress-induced hyperglycemia in an otherwise metabolically normal individual, several key findings support ketosis-prone diabetes rather than autoimmune type 1 diabetes or established symptomatic type 2 diabetes. The absence of diabetes autoantibodies, preserved C-peptide secretion, and subsequent insulin independence are characteristic of ketosis-prone diabetes with remission. We interpret this presentation as diabetic ketoacidosis precipitated by acute physiological stressors—specifically high-altitude exposure and severe infection—occurring in a patient with previously unrecognized chronic dysglycemia. This clinical phenotype aligns with current descriptions of A^−^β^+^ ketosis-prone diabetes, a distinct entity in which patients present with DKA but lack islet autoimmunity and retain sufficient pancreatic β-cell reserve to achieve insulin independence following resolution of the acute metabolic crisis (2, 10, 26, 27).
The distinction between stress-induced hyperglycemia and pre-existing chronic dysglycemia unmasked by acute stress is clinically and prognostically important. True stress hyperglycemia occurs in previously normoglycemic individuals during critical illness and typically resolves once the acute stressor is removed, whereas sustained HbA1c elevation reflects months of antecedent dysglycemia and indicates underlying diabetes or prediabetes (28, 29). In this case, the admission HbA1c of 9.0%, combined with subsequent demonstration of glucose intolerance requiring insulin therapy before eventual remission, supports the interpretation that altitude exposure and infection precipitated ketoacidosis in the setting of previously unrecognized chronic hyperglycemia rather than inducing transient hyperglycemia in a metabolically normal host.
Finally, the multiplicity of pathogens observed in this case fits with broader evidence that polymicrobial infections in critically ill hosts are associated with more severe clinical courses and complex therapeutic decisions (21). The patient’s full recovery of pulmonary function and normalization of glucose tolerance after withdrawal of insulin therapy illustrates that, with timely diagnosis, judicious use of molecular diagnostics, and structured metabolic follow-up, both respiratory and metabolic derangements can be reversible even in severe presentations.
This case report has several limitations. As a single-patient observation, generalizability is limited. Pathogen quantification from multiplex PCR was semiquantitative, and absolute burden thresholds for clinical significance remain undefined, and comparative studies show variability in panel performance across different clinical settings (30). Serum β-D-glucan testing was unavailable (30) Serum β-D-glucan testing was unavailable, potentially limiting diagnostic certainty for invasive candidiasis. Although 8-month follow-up demonstrated sustained remission, longer observation is needed to confirm durability and exclude late relapse. Finally, genetic testing for monogenic diabetes was not pursued given low clinical suspicion, but cannot be definitively excluded.
Conclusion
This case of diabetic ketoacidosis precipitated by high-altitude exposure and severe polymicrobial pneumonia in a previously undiagnosed young woman highlights the interplay between environmental stressors, complex respiratory infection, and ketosis-prone diabetes. A careful, stewardship-based interpretation of multiplex pneumonia panel results was essential to distinguish likely pathogenic organisms from colonizers, thereby guiding antimicrobial and antifungal therapy while minimizing unnecessary treatment.
Structured post-discharge evaluation, including classification according to current diabetes standards and the use of oral glucose tolerance testing, confirmed metabolic remission and clarified the long-term phenotype and risk profile. This integrated respiratory, infectious, and metabolic approach can inform the management of similar patients who present with combined respiratory failure and DKA in the context of recent high-altitude exposure and polymicrobial airway infection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kitabchi AE Umpierrez GE Miles JM Fisher JN. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. (2009) 32:1335–43. doi: 10.2337/dc 09-9032, 19564476 PMC 2699725 · doi ↗ · pubmed ↗
- 2Kikani N Balasubramanyam A. Remission in ketosis-prone diabetes. Endocrinol Metab Clin N Am. (2023) 52:165–74. doi: 10.1016/j.ecl.2022.06.005, 36754492 · doi ↗ · pubmed ↗
- 3Braun B. Effects of high altitude on substrate use and metabolic economy: cause and effect? Med Sci Sports Exerc. (2008) 40:1495–500. doi: 10.1249/MSS.0b 013e 3181729 dd 3, 18614940 · doi ↗ · pubmed ↗
- 4Woolcott OO Ader M Bergman RN. Glucose homeostasis during short-term and prolonged exposure to high altitudes. Endocr Rev. (2015) 36:149–73. doi: 10.1210/er.2014-1063, 25675133 PMC 4399271 · doi ↗ · pubmed ↗
- 5Koufakis T Karras SN Mustafa OG Zebekakis P Kotsa K. The effects of high altitude on glucose homeostasis, metabolic control, and other diabetes-related parameters: from animal studies to real life. High Alt Med Biol. (2019) 20:1–11. doi: 10.1089/ham.2018.0076, 30362832 · doi ↗ · pubmed ↗
- 6Mohajeri S Balasubramanian P Burgess MI. Diabetes, trekking and high altitude: recognising and managing the risks. Diabet Med. (2015) 32:1425–37. doi: 10.1111/dme.12795, 25962798 · doi ↗ · pubmed ↗
- 7Wang N Shi XF Khan SA Wang B Semenza GL Prabhakar NR . Hypoxia-inducible factor-1 mediates pancreatic β-cell dysfunction by intermittent hypoxia. Am J Physiol Cell Physiol. (2020) 319:C 922–32. doi: 10.1152/ajpcell.00309.2020, 32936698 PMC 7789966 · doi ↗ · pubmed ↗
- 8Pham K Frost S Parikh K Pham A Pezzullo JC Morici L . Changes in immune cell populations during acclimatization to high altitude. Physiol Rep. (2024) 12:e 70024. doi: 10.14814/phy 2.7002439551933 PMC 11570420 · doi ↗ · pubmed ↗