A methodological framework for constructing opioid agonist therapy episodes in administrative health data
Kiana Yazdani, Cassidy Tam, Christopher C. Fisher, Scott D. Emerson, Jason Trigg, Katherine W. Kooij, Mary A. De Vera, Fidel Vila-Rodriguez, Robert S. Hogg, Julio S. G. Montaner, Viviane Dias Lima

TL;DR
This paper introduces a new framework for accurately tracking opioid treatment episodes in health data by considering medication switches and dispensing patterns.
Contribution
The novel contribution is a methodological framework combining Allen’s interval algebra, temporal margins, and drug-specific permissible gaps for OAT episode construction.
Findings
The before relation was most common for methadone dispensations.
Monotherapy episodes made up 93.53% of all identified OAT episodes.
The framework is transferable to other populations with parameter adjustments.
Abstract
Opioid Agonist Therapy (OAT) is the most effective intervention to reduce overdose risk, and administrative health data are now increasingly used to study OAT outcomes. However, current methods for constructing OAT episodes rely heavily on fixed permissible gaps and often overlook switches between medications, concurrent therapies, and the temporal complexity of dispensing patterns. We aimed to develop a robust episode-construction framework that more precisely reflects real-world OAT use within administrative health data. We analyzed OAT dispensations from people living with HIV in British Columbia (2010–2020). Episodes were constructed using three components: Allen’s interval algebra, temporal margins (\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs}…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
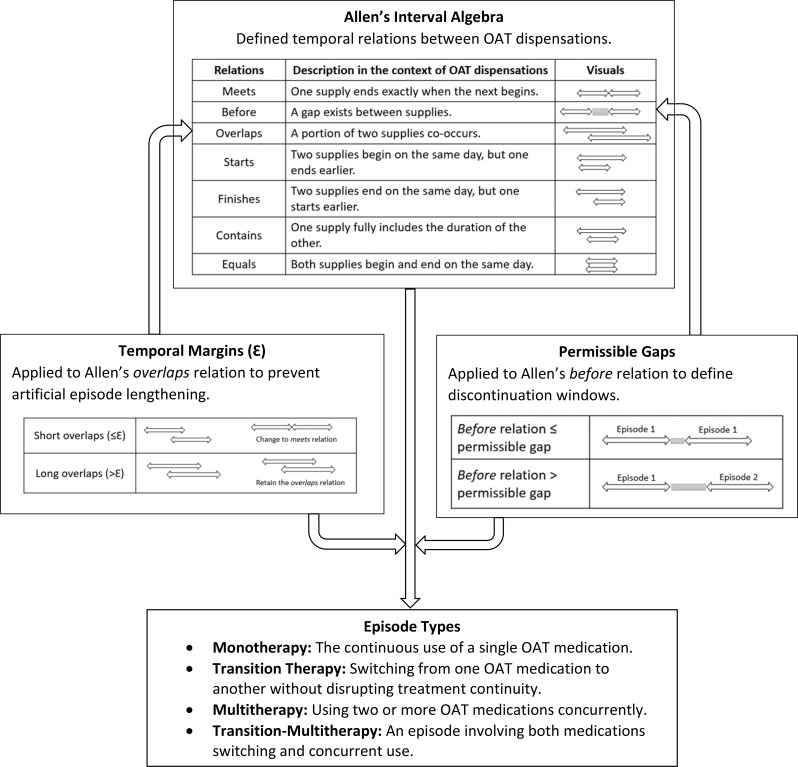 Figure 1
Figure 1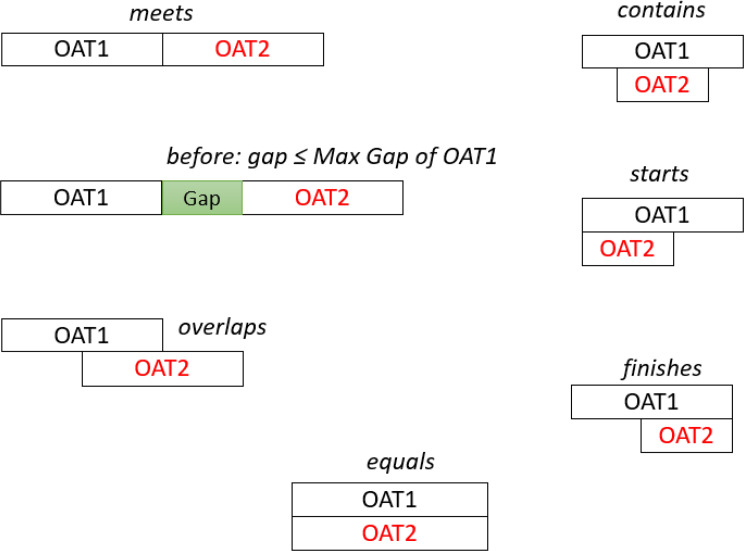 Figure 2
Figure 2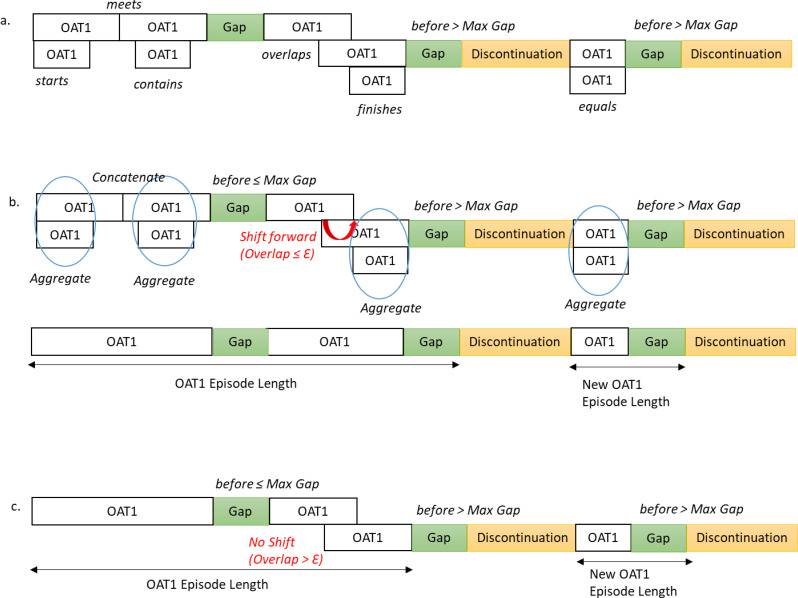 Figure 3
Figure 3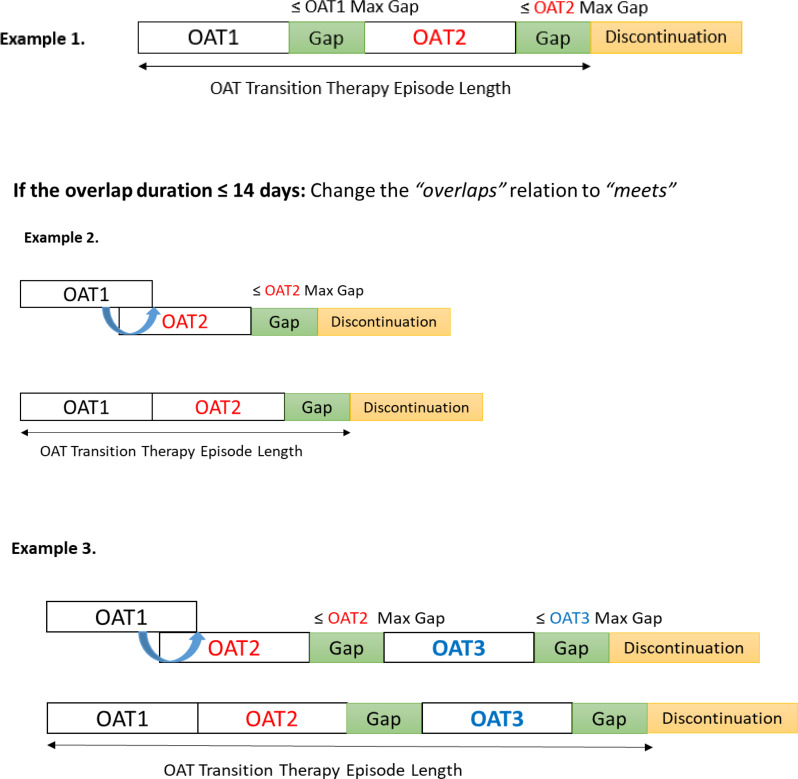 Figure 4
Figure 4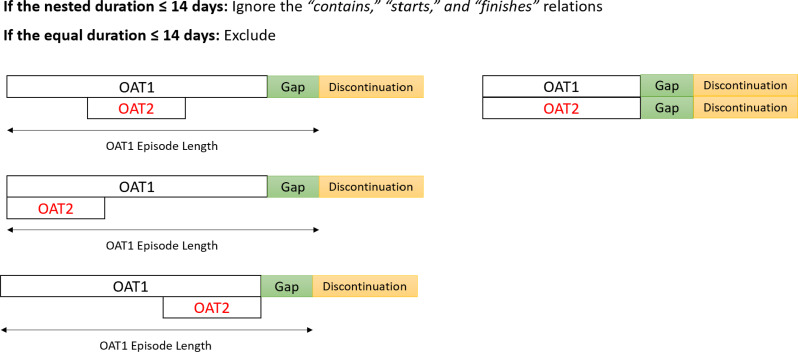 Figure 5
Figure 5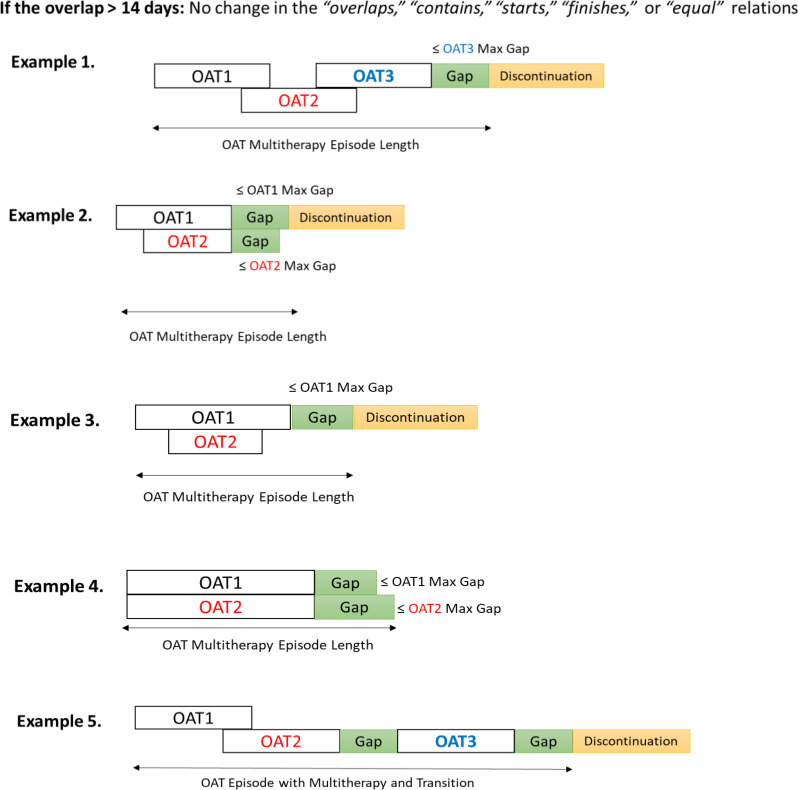 Figure 6
Figure 6- —https://doi.org/10.13039/501100000024Canadian Institutes of Health Research
- —https://doi.org/10.13039/501100004726Ministry of Health, British Columbia
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOpioid Use Disorder Treatment · Substance Abuse Treatment and Outcomes · HIV, Drug Use, Sexual Risk
Introduction
Opioid Use Disorder (OUD) is a chronic relapsing condition associated with elevated rates of morbidity and mortality [1]. In 2016, British Columbia (BC), Canada, declared a public health emergency due to the alarming increase in overdose deaths driven by a toxic drug supply (the increasingly contaminated and unpredictable unregulated drug market) [2, 3]. Opioid poisoning has since become the leading cause of unnatural death in BC, surpassing the combined number of homicides, suicides, and motor vehicle accidents [4]. Please confirm the inserted city name is correct and amend if necessary.
Despite the complexity of OUD, individuals can achieve sustained long-term recovery with appropriate treatment and support [4]. Opioid Agonist Therapy (OAT) is currently the most effective, evidence-based intervention for OUD, reducing all-cause and overdose mortality [5, 6]. Research additionally suggests that OAT prevents overdoses during the fentanyl crisis, where this potent opioid has entered the illicit drug supply and significantly increases overdose risk [6, 7].
A growing body of OAT-focused research in Canada, especially in BC, now extensively uses administrative health data [6, 8–12]. Administrative health data refer to routinely collected records generated through interactions with the healthcare system, including clinic visits, hospital encounters, laboratory testing, and pharmacy dispensations, primarily for billing, reimbursement, and system management rather than for research purposes [13]. Owing to their population coverage and real-world nature, administrative health datasets provide a powerful and cost-efficient resource for large-scale research [14, 15]. However, because they were not designed for research, they may contain diagnostic under-capture, incomplete information, or coding inconsistencies [13]. Therefore, rigorous methodological approaches are essential to ensure valid inferences and to mitigate data-related bias.
Although administrative health data offer valuable insights into OAT outcomes, current research has two important methodological limitations in constructing OAT treatment episodes. First, most studies do not fully reflect significant programmatic changes in OAT delivery introduced in response to the increasingly toxic drug supply and escalating overdose mortality [4, 9]. For example, OAT treatment options have expanded; in BC, four medications are now approved for treating OUD: methadone, buprenorphine, slow-release oral morphine (SROM), and injectable OAT (iOAT). Less restrictive prescribing practices also allow patients to switch between therapies or use multiple regimens concurrently, depending on their preferences, treatment goals, and disease severity [4, 9]. Yet, most administrative-data studies continue to construct treatment episodes for a single OAT medication, typically methadone or buprenorphine, with limited consideration of additional treatment options, switching patterns, or concurrent OAT use.
Second, episode construction has mainly relied on the permissible gap framework, which defines a continuous episode by specifying the maximum allowable gap between two consecutive dispensations [16]. While this method is practical, assuming fixed gaps oversimplifies the temporal dynamics of OAT dispensations, which may result from patient behaviour, prescriber decisions, programmatic factors, or pharmacy workflow [17]. The permissible gap framework is also limited when dealing with overlapping dispensations. Common practice is either to include the overlap periods or to omit them at the expected end time, failing to account for overlap lengths [16, 18, 19]. Improper management of these overlaps can lead to misclassification of treatment exposure and biased estimates of associations with clinical outcomes [16, 20].
To address these methodological challenges and given the critical importance of OAT outcomes amid the ongoing toxic drug supply, we developed a comprehensive framework for constructing OAT treatment episodes in administrative health data that more precisely reflects real-world OUD care and strengthens OAT-related analyses. This framework integrated three key components: (1) Allen’s interval algebra, a temporal logic system that characterizes the full range of temporal relationships between two dispensations; (2) temporal margins ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} ), which extend this algebra by differentiating short from long overlaps and enabling the identification of episodes with medication switches or concurrent therapies; and (3) the permissible gap, that determines when an episode is discontinued.
Methods
Data sources and study sample
The data were sourced from the Seek and Treat for Optimal Prevention of HIV/AIDS (STOP HIV/AIDS) study, an open, bidirectional, population-based longitudinal cohort maintained at the BC Centre for Excellence in HIV/AIDS (BC-CfE) [21]. It includes de-identified, individual-level data on adults ≥ 19 years old with HIV, covering the period from April 1, 1996, to March 31, 2020. The cohort was established by linking three provincial data sources: the BC-CFE Drug Treatment Program [22], the BC Centre for Disease Control HIV/AIDS Surveillance database [23], and administrative health datasets provided by the BC Ministry of Health. Central to our study of OAT was the PharmaNet administrative health database, which records all dispensed prescription medications from BC community and hospital outpatient pharmacies for at-home use [24]. Here, dispensation data refers to records of medications provided to patients, rather than prescriptions written and actual medication use. PharmaNet database excludes inpatient dispensations, over-the-counter medications, and antiretroviral drugs for HIV treatment provided by BC-CfE.
To study OAT using PharmaNet data, we used several core fields. The Drug/Product Identification Number (DIN/PIN) was used to identify the specific OAT medication dispensed. The Date of Service indicated when the medication was provided, while the Days supply reflected the duration for which the dispensation was intended. The Quantity Dispensed represented the total number of OAT units supplied, and the Drug Strength captured the potency of the active ingredients per unit. The daily dose was calculated by multiplying the quantity dispensed by the drug strength and dividing the result by the days supply.
This was not a prespecified secondary analysis of the STOP HIV/AIDS study, but was undertaken to address the complexity observed in OAT data from a prior project [11] and within the context of an ongoing project examining the impact of stimulant use disorder (StUD) on OAT retention, and to help bridge the gap between clinical practice and dispensation data. We analyzed a sample of people living with HIV (PLWH) from the STOP cohort diagnosed with either OUD alone or concurrent OUD and StUD, who received at least one OAT dispensation between April 1, 2010, and March 31, 2020. The case-finding algorithms for OUD and StUD are detailed in Appendix 1.
Identifying OAT dispensations
The OAT medications examined in this study were methadone, buprenorphine, SROM, and iOAT, identified using their respective DIN/PIN in PharmaNet. Methadone, a long-acting full agonist, is available in several formulations, including liquid, unflavored, and compounded preparations. Buprenorphine, a partial agonist, is available as either buprenorphine/naloxone (Suboxone) tablets or subcutaneous buprenorphine (Sublocade), administered as a monthly injection. The SROM, an intermediate-acting full agonist, is available in a 24-hour formulation. Lastly, iOAT consists of short-acting full agonists, including diacetylmorphine and hydromorphone [4]. Appendix 2 and the complementary Excel file contain the complete definitions and set of DIN/PIN codes for all OAT medications.
Initial pharmanet data cleaning
Given the variability in OAT dosing (e.g., split doses, variable quantities, multiple same-day pickups) and pharmacy-specific workflow patterns, raw dispensation records sometimes contained errors or inconsistent values requiring correction. These included days supply that were incompatible with the dispensing interval, misaligned service dates, implausible quantity-per-day (QPD) values inconsistent with adjacent records, and large outliers. To address these issues, before constructing treatment episodes, we implemented a sequence of logic-based corrections, adapted from the published methodologies of Pearce et al. [6] and from our previous analysis [11]. We first consolidated split-dose dispensations by summing the quantities for the same day. We then corrected days supply or service dates when they were inconsistent with adjacent records and had inconsistent QPD values. Large QPD deviations were addressed by recalculating the days supply when this produced a clinically plausible pattern, or by adjusting the quantity dispensed when the implied daily dose conflicted with adjacent records. Days supply values that exceeded the time to the next dispensation were reset to match that interval. Appendix 3 provides a detailed description of these cleaning procedures and contrasts them with those used in earlier research. The complementary Excel file illustrates each correction type, and all corresponding code syntax is included in the supplementary materials.
Episode-construction framework
After completing the initial PharmaNet data cleaning described above, we operationalized three integrated components to construct OAT treatment episodes: Allen’s interval algebra, temporal margins ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} ), and the permissible gaps.
To capture the complexity of OAT dispensing patterns and the full range of temporal relationships that can stem from irregular medication use, dose adjustments, medication loss, treatment switching or concurrent therapy, and pharmacy workflow inconsistencies (see Appendix 4 for examples), we incorporated Allen’s interval algebra, as adapted for multitherapy medication datasets by Khotimah et al. [19] Allen’s logic defines all possible temporal relations between two intervals, allowing us to characterize each pair of dispensations using one of seven base relations—meets, overlaps, before, starts, finishes, contains, equals—and their inverses (13 total) [25, 26]. These relations specify whether one dispensation begins exactly when another ends (meets), follows another with a non-zero gap (before), overlaps in part (overlaps), begins simultaneously but ends earlier (starts), ends simultaneously but begins later (finishes), fully contains or is fully contained within another (contains), or shares identical start and end times (equals) (Table 1).
Table 1. Allen’s interval algebraBasic RelationsDescriptionInverse RelationsVisual RepresentationTemporal OrderX meets YX ends exactly where Y startsY met by X
X_start_ < X_end_ = Y_start_ < Y_end_X overlaps YX starts before Y, and X ends during YY overlapped by X
X_start_ < Y_start_ < X_end_ < Y_end_X before YX ends before Y startsY after X
X_start_ < X_end_ < Y_start_ < Y_end_X starts YX starts at the same time as Y, but ends earlierY started by X
X_start_ = Y_start_ < X_end_ < Y_end_X finishes YX ends at the same time as Y, but starts laterY finished by X
Y_start_ < X_start_< X_end_ = Y_end_X contains YY starts after X, and ends before XY during X
X_start_ < Y_start_ < Y_end_ < X_end_X equals YX and Y start and end at the same timeX equals Y
X_start_ = Y_start_ < X_end_ = Y_end_Note: Allen’s time interval algebra describes temporal relationships between time intervals based on their chronological order. In our study, a time interval refers to the period from when an OAT is dispensed to the date it is expected to last, as determined by the days supply field in PharmaNet. Table is adapted with modifications from [Mate S, Bürkle T, Kapsner LA, et al. A method for the graphical modeling of relative temporal constraints. J Biomed Inform. 2019; 100:103314. 10.1016/j.jbi.2019.10331] [26]
Although Allen’s relations identify whether an overlap exists, they do not account for the overlap length. To address this, we incorporated temporal margins ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} ) into the overlaps relation. Short overlaps (≤ \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} ) were interpreted as continuation of therapy and recoded as meets, whereas longer overlaps (> \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} ) were retained to avoid inappropriate inflation of episode length.
The third component, the permissible gap, specifies the maximum allowable interruption between dispensations before an episode is classified as discontinued. This measure defines the discontinuation window and maps onto the before relation in Allen’s relations, which captures intervals separated by a positive gap. Establishing this window is critical for measuring OAT outcomes such as treatment retention, adherence, or care discontinuity.
Using these three components together, our framework ultimately identified four types of OAT episodes: (1) monotherapy episodes, in which a single OAT medication is dispensed continuously; (2) transition therapy episodes, where an individual switches from one OAT to another while maintaining continuity of care; (3) multitherapy episodes, reflecting concurrent use of two or more OAT medications; and (4) transition-multitherapy, where both switching and concurrent use occur within the same episode. The following sections describe in detail how each component of the framework is applied to identify these episode types. Figure 1 provides a visual schematic of the overall episode-construction framework.
Fig. 1. Integrated framework for constructing OAT treatment episodes using Allen’s interval algebra, temporal margins ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} ), and permissible gaps
Constructing monotherapy episodes
Table 2 summarises the procedures used to operationalise Allen’s relations for the construction of monotherapy episodes. Short overlaps between the same OAT dispensations, typically resulting from early refills, routine pharmacy variation, or minor supply carryover, were treated as uninterrupted treatment and recoded as meets using the temporal margin ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} ). In contrast, longer overlaps, which more often signal changes in circumstances such as dose adjustments or lost medication, were left unchanged. To select an appropriate value for \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} , we compared scenarios with no margin, a 7-day margin, and a 14-day margin by examining the difference between the original Dates of Service and the shifted dates after recoding overlaps as meets. Episode discontinuation was defined by pairing Allen’s before relation with OAT drug-specific permissible gaps, informed by BC OAT clinical guidelines, and the half-lives of OAT medications [4, 9]. Permissible gaps were set at ≤ 6 days for buprenorphine/naloxone, ≤ 5 days for methadone and SROM, and ≤ 3 days for iOAT.
Table 2A description of data manipulation techniques applied to allen’s relations to minimize discrepancies in the OAT data and support the construction of monotherapy episodesAllen’s RelationsManipulation TechniquesDescriptions
ConcatenationLinked consecutive dispensations with no gap to create a continuous single-OAT treatment.
Temporal Margin ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} )Relaxed Allen’s overlaps relation using the concept of \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} to differentiate between short and long overlaps under the following conditions:If the overlap duration was ≤ \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} days, we shifted the start date of the subsequent dispensation forward and reclassified the temporal relation from overlaps to meets. If the overlap duration was > \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} days, no adjustments were made.
PermissibleGapIntegrated Allen’s relation with OAT-specific permissible gaps to allow short interruptions within a continuous treatment. If gaps in the before relation exceeded the permissible gap, we classified the OAT as discontinued.
AggregationThe two dispensations were merged at the common start date value, and the daily dose was added for the nested period.
AggregationThe two dispensations were merged at the common end date value, and the daily dose was added for the nested period.
AggregationThe two dispensations were merged, using the start and end dates of the dispensation with the larger days supply, and the daily dose was added for the nested period.
AggregationThe two dispensations were merged, using the start and end dates from one of the two dispensations. The daily dose was added for the nested period.Note: Appendix 4, Example 5 provides an example of applying these techniques to PharmaNet dispensations for monotherapy episode construction
Constructing transition and multitherapy episodes
Transition therapy refers to a switch from one OAT medication to another while maintaining overall continuity of care. In clinical practice, transitions may occur without a washout period (for example, buprenorphine to methadone), with a brief washout (as previously required for methadone to buprenorphine), or through structured low-dose inductions that introduce short periods of overlap [4]. Within Allen’s relations, these transitions could appear as meets, before (with a washout period shorter than the drug-specific permissible gap), or as short overlaps, respectively (Fig. 2).
Fig. 2. Allen’s relations across different OAT dispensations. The meets relation could occur when switching between full agonists, with no washout period required. The before (≤ permissible gap) relation may happen when a washout period is necessary to prevent withdrawal symptoms, especially when transitioning from a full agonist to a partial agonist. The overlaps may occur during multitherapy or cross-tapering between OAT medications, particularly when moving from a full agonist to a partial agonist after the new low-dose induction protocol. The equals, contains, starts, or finishes relations could occur due to multitherapy or failed transition attempts
Multitherapy occurs when a new OAT is added to the previous one and is distinct from transition therapy. It entails the concurrent use of multiple medications, suggesting that a single treatment is insufficient to address a patient’s condition. In multitherapy, Allen’s relations could be reflected as overlaps, equals, contains, starts, or finishes (Fig. 2). These relations should remain unchanged to reflect the concurrent use of OAT medications without artificially lengthening the episode.
Therefore, as with constructing monotherapy episodes, a temporal margin ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} ) is necessary to differentiate between an overlap signifying a transition or multitherapy between different OAT dispensations. Furthermore, to classify equals, contains, starts, or finishes relations between different OAT medications as multitherapy, it was necessary to determine the minimum co-dispensation duration for two OAT types, as these relations may also arise during unsuccessful or incomplete transitions between medications.
To define this threshold, we used an approach informed by both empirical data and clinical expertise to distinguish transitions from multitherapy. We identified all periods in which two OAT medications were co-dispensed, summarized their durations using descriptive statistics, and consulted with co-author Christopher C. Fisher, a clinical pharmacist specializing in OAT, to determine the minimum duration needed to categorize an episode as multitherapy. For both transition and multitherapy episodes, discontinuation was defined using the permissible gap corresponding to the last OAT medication dispensed during that episode.
OAT episodes and hospitalizations
Our data source, PharmaNet, does not include dispensations provided during hospitalizations. Based on inpatient continuity of care guidelines, it is reasonable to assume that OAT continues in some form during patients’ hospital stays [27]. Thus, we assumed OAT continuation if a patient was admitted amid an ongoing OAT episode.
Statistical analysis
Descriptive statistics were used to characterize OAT dispensations and the constructed episodes. For continuous variables, we calculated means with standard deviations (SD), medians with first and third quartiles (Q1, Q3), and minima, maxima, and modes when relevant. Categorical variables were summarized using frequencies and percentages. All analytic procedures related to episode construction were based on the application of Allen’s interval algebra, including the identification of temporal relations, the use of temporal margins ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} ) to distinguish short from long overlaps, and the permissible gap to determine episode discontinuation. No inferential modelling was undertaken, as the primary aim was to construct and describe OAT treatment episodes. All analyses were performed using SAS version 9.4 (SAS, Cary, NC, USA).
Results
Between 2010 and 2020, out of 11,376 PLWH in the STOP cohort, we identified 1,559 (13.70%) individuals with either OUD alone (n = 396) or co-occurring OUD-StUD (n = 1,163) who were dispensed at least one OAT.
Initial pharmanet data cleaning
To contextualize the performance of our cleaning procedures, we compared error percentages with earlier PharmaNet-based work. Of 2,094,532 OAT dispensations, 21,977 (1.05%) were flagged and 8,993 (40.92%) corrected. As shown in Appendix 3, this percentage is lower than that reported in a previous BC study of PLWH receiving OAT using the same STOP data source (2.9%) [11] and lower than in a provincial OUD cohort (2.3%) [6]. This difference is expected given our population (PLWH with OUD or OUD-StUD) and refinements to our correction rules, while remaining broadly comparable to prior analyses.
Constructing monotherapy episodes
The distribution of Allen’s relations across same-type dispensations is summarized in Table 3. The before relation dominated across all OAT medications, occurring in > 90% of methadone and iOAT dispensations and 76% of buprenorphine and SROM dispensations. Equals relations were most pronounced for buprenorphine (21.46%) and SROM (20.87%), with rare occurrences of other relations (< 1%).
Table 3. Allen’s Temporal relations between same-type OAT dispensations in PLWH with OUD, or OUD-StUDMethadone(n = 1,788,395)Buprenorphine(n = 63,592)SROM(n = 207,960)iOAT(n = 34,585)Not applicable1,331 (0.07)529 (0.83)690 (0.33)175 (0.51)Meets3,752 (0.21)466 (0.73)1,677 (0.81)80 (0.23)Before1,778,136 (99.43)48,452 (76.19)159,516 (76.71)33,528 (96.94)Overlaps406 (0.02)265 (0.42)2,069 (0.99)72 (0.21)Starts26 (0.00)57 (0.09)140 (0.07)25 (0.07)Finishes113 (0.01)27 (0.04)112 (0.05)11 (0.03)Contains540 (0.03)149 (0.23)355 (0.17)34 (0.10)Equals4,091 (0.23)13,647 (21.46)43,401 (20.87)660 (1.91)Note: Data indicate n (%). Frequencies represent dispensation-level counts before episode construction and prior to applying temporal margins and permissible-gap rules. The not applicable category refers to the first record for participantsAbbreviations: OAT: Opioid Agonist Therapy; SROM: Slow-Release Oral Morphine; iOAT: Injectable Opioid Agonist therapy; PLWH: People living with HIV; OUD: Opioid Use Disorder; StUD: Stimulant Use Disorder
Without applying a temporal margin ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} ), the mode and median differences between original and shifted dates were both zero, indicating minimal shifts for most dispensations. However, large mean and maximum shifts were observed for some SROM dispensations (mean [SD]: 5.44 days [28.03]; max: 695 days), driven by accumulated overlaps. Applying \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} =7 days reduced this mean difference by approximately 98% to 0.12 days (SD:1.71) (max: 98 days), while \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} =14 days produced a mean of 0.23 days (SD:3.91) (max: 260 days) (Appendix 5). Therefore, a 7-day margin was chosen to distinguish between short and long overlaps between the same OAT dispensations. Figure 3 illustrates the framework for constructing OAT monotherapy episodes.
Fig. 3. Constructing continuous monotherapy episodes using Allen’s relation, adjusted with temporal margins and permissible gaps. The \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} was set to seven days. If the overlap duration was ≤7 days, we shifted the start date of the next dispensation forward, changing the relation from overlaps to meets (b). No adjustments were made for overlaps >7 days (c)
Constructing transition and multitherapy episodes
We identified 2,192 dispensation sequences involving more than one type of OAT, based on co-dispensation periods (Table 4). The most frequently observed pattern was a return to the initial therapy following a period of overlap, with the sequence OAT1→(OAT1 + OAT2)→OAT1 accounting for 1,800 cases (82.12%). A smaller proportion of sequences involved a transition from the initial to the second therapy, represented by OAT1→(OAT1 + OAT2)→OAT2, observed in 328 cases (14.96%). Among the former group, the most common pattern was iOAT→(iOAT+SROM)→iOAT, which occurred in 977 cases (54.28%). In the latter group, the predominant sequence was SROM→(SROM+Methadone)→Methadone, observed in 94 cases (28.66%). Other uncommon sequences with no specific pattern (n=64, 2.92%) are detailed in Appendix 6.
Table 4. All identified co-dispensation patterns with more than one OAT medicationFrequencyMedian(Q1, Q3)Mean (SD)MinMaxOAT1 → (OAT1 + OAT2) → OAT1**(**n = 1,800)iOAT → (iOAT+SROM) → iOAT9773 (1, 7)7.59 (19.58)1413SROM → (SROM + MTD) → SROM2934 (2, 9)13.15 (31.85)1277MTD → (MTD+SROM) → MTD23113 (4, 41)50.85 (110.46)1970iOAT → (iOAT + MTD) → iOAT1012 (1, 4)6.09 (14.97)1133MTD → (MTD+iOAT) → MTD922 (1, 8.5)18.91 (42.66)1217SROM → (SROM+iOAT) → SROM773 (1, 7)8.87 (22.37)1169MTD → (MTD + Bup/nal) → MTD194 (2, 8)5.05 (3.81)116SROM → (SROM + Bup/nal) → SROM77 (3, 7)8.29 (9.88)130iOAT → (iOAT + Bup/nal) → iOAT< 5Censored for privacy reasonsBup/nal → (Bup/nal+SROM) → Bup/nal< 5Censored for privacy reasonsOAT1 → (OAT1 + OAT2) → **OAT2 (**n **= 328)**SROM → (SROM + MTD) → MTD9411.5 (3,30)38.29 (98.88)1760MTD → (MTD+SROM) → SROM7711 (4, 34)75.97 (270.48)12,058SROM → (SROM+iOAT) → iOAT416 (3, 19)24.93 (50.36)1283iOAT → (iOAT+SROM) → SROM244.5 (2, 12)10 (15.84)174MTD → (MTD + Bup/nal) → Bup/nal248 (7, 12.5)9.79 (6.41)128MTD → (MTD+iOAT) → iOAT188.5 (2, 25)56.78 (149.34)1637Bup/nal → (Bup/nal + MTD) → MTD207 (2, 14)9.85 (10.60)138iOAT → (iOAT + MTD) → MTD176 (2, 15)21 (37.91)1139SROM → (SROM + Bup/nal) → Bup/nal67 (2, 7)7.67 (6.98)221Bup/nal → (Bup/nal+SROM) → SROM< 5Censored for privacy reasonsBup/nal → (Bup/nal + iOAT) → iOAT< 5Censored for privacy reasonsiOAT → (Bup/nal + iOAT) → Bup/nal< 5Censored for privacy reasonsOther Sequences with frequencies < 5 (n = 64), Appendix 6Note: The sequences were identified by analyzing the co-dispensation periods. Frequency indicates how often co-dispensations occurred. Other summary statistics provide an overview of the co-dispensation durationsAbbreviations: OAT: Opioid Agonist Therapy; MTD: Methadone; Bup/nal: Buprenorphine/naloxone; SROM: Slow-Release Oral Morphine; iOAT: Injectable Opioid Agonist Therapy; Q1: 25% interquartile; Q3: 75% interquartile; SD: Standard Deviation
The median duration of the co-dispensation periods for all identified sequences was <14 days (Table 4). However, investigating the mean and maximum values showed prolonged co-dispensation periods, suggesting multitherapy before patients either resume their initial OAT or move to an alternative OAT. We chose a 14-day margin to differentiate between transition and multitherapy. Similar to monotherapy episode construction, we applied Allen’s before relation with the permissible gap and adjusted the overlaps relations using \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} =14 days. If a new OAT dispensation occurred within the grace period of the previous OAT, we maintained the before relation and classified the episode as a transition (Fig. 4, Example 1). If Allen’s overlaps relation was ≤14 days, we adjusted it to meets to form a transition therapy episode (Fig. 4, Example 2).
Fig. 4. Constructing continuous transition therapy episodes using Allen’s relation, adjusted with temporal margins and permissible gap concepts. The \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} was set to 14 days. If Allen’s overlaps relation was ≤14 days, we adjusted it to meets to build a continuous transition therapy episode (Examples 2 and 3)
We ignored the contains, starts, and finishes relations with co-dispensation periods shorter than the 14-day margin and attributed the episode to the OAT type encompassing the others. The equals relations with durations ≤14 days were excluded (n=15) (Fig. 5). Alternatively, if the co-dispensation period in Allen’s overlaps, contains, starts, finishes, or equals relation was >14 days, we classified the episode as an OAT multitherapy episode with no adjustments made to the relations (Fig. 6).
Fig. 5. Handling contains, starts, finishes, and equals relations between OAT dispensations of multiple types with a co-dispensation period ≤14 days. The contains, starts, finishes relations with co-dispensation periods ≤14 days were ignored, and the episode was assigned to the OAT type encompassing the others. The equals relations with the co-dispensation periods ≤14 days were excluded (n=15)
Fig. 6. Constructing OAT multitherapy episode using Allen’s relations with a temporal margin of 14 days. If the co-dispensation period in Allen’s overlaps, contains, starts, finishes, or equals relation was >14 days, the relations remained unchanged, and the episode was categorized as an OAT multitherapy episode. Example 5 indicates an episode with both multitherapy and transition events
OAT episodes and hospitalizations
In Appendix 7, we explored various scenarios to more precisely define an episode’s start and end dates when OAT is initiated following hospitalization, when hospitalization occurs before the preceding OAT episode reaches its discontinuation threshold, or when OAT regimen changes occur post-hospitalization.
We identified 10,386 episodes, of which 93.53% (n=9,714) were monotherapy, 3.72% (n=386) transition therapy, and 2.27% (n=236) multitherapy. Less than 1% (n=50) involved transition and multitherapy. The median (Q1, Q3) duration of all episodes was 39 days (13, 165).
Discussion
We proposed a refined methodological framework to build OAT episodes in administrative health data by integrating Allen’s relation with the concepts of permissible gap and temporal margins ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} ). This combined methodology improves upon using the permissible gap method alone. The permissible gap provides a framework for defining discontinuation windows, which are critical components in analyzing medication outcomes. However, this approach is limited by its reliance on a fixed temporal relation, accounting only for the before relation and failing to consider the magnitude of overlaps or other temporal relations. Therefore, extending the framework with Allen’s relations and temporal margins permits a more nuanced construction of OAT treatment episodes that better reflect the complexity of real-world OAT use.
Although in our study the predominant temporal relation between same-type OAT dispensations was before, we also observed a high proportion of equals relations for buprenorphine, SROM, and iOAT that may not have been adequately captured by the permissible gap method alone. The observed relations also align with clinical practice: gaps in the data reflected as before relations could be attributed to treatment interruptions, discontinuations, or delayed refills among patients with OUD. Conversely, equals relations are likely linked to same-day supplies for witnessed ingestions, as-needed OAT medications, or split dosing [4, 27].
Incorporating a temporal margin into Allen’s relations improves the handling of overlaps and reduces misclassification of OAT exposure by preventing artificially prolonged episodes. It also allows for differentiating episodes with transition therapy and multitherapy. Although Khotimah et al. previously applied temporal margins to relax Allen’s relations in a study of diabetes medications, their method applied \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} to both overlaps and before relations [19]. This approach treats any gap shorter than \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} as meets and continuous therapy, which makes the definition of a distinct discontinuation window dependent on the choice of \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} . In contrast, our framework preserves the before relation through clinically informed permissible gaps [4], ensuring discontinuation windows remain grounded in OAT pharmacology and clinical practice.
Additionally, the temporal margin was applied in two ways in our analysis: (a) to construct monotherapy episodes, a seven-day margin was used to account for short versus long overlaps between same-type OAT dispensations, and (b) a 14-day margin was applied to differentiate transitions from multitherapy when more than one OAT was dispensed. This contrasts with the approach by Khotimah et al., in which the temporal margin was applied across diabetes medication classes to define continuous episodes, rather than distinguish transitions from multitherapy.
The selection of \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} =7 days for same-OAT dispensations and \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} =14 days for overlaps involving different OAT medications was informed by both empirical data and clinical practice. In constructing monotherapy episodes, we observed that recoding all overlaps to meets without a temporal margin ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} ) led to substantial artificial shifts in Dates of Service, producing patterns that were inconsistent with real-world dispensing behaviour. Introducing a small margin ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathcal{E}$$\end{document} =7) effectively minimized these distortions while preserving clinically appropriate continuity of therapy. For different OAT dispensations, examination of co-dispensation lengths showed that most overlaps were less than 14 days. Input from an OAT-specialized clinical pharmacist and current treatment guidelines [4] supported the use of this range to represent intentional transitions. Longer overlap periods, by contrast, more often reflected concurrent therapy rather than transitional switching. Accordingly, a 14-day margin provides a clinically appropriate threshold for distinguishing transition episodes from multitherapy.
Additional support for these parameters comes from BC’s “refilling too soon” policy, which permits refills only when 14 or fewer days of supply remain [28]. This policy reflects routine dispensing patterns that naturally allow short overlaps of this magnitude. Longer overlaps, in contrast, are unlikely to represent routine continuation and should not be appended to the end of an episode, as they likely reflect a clinically meaningful change in treatment rather than ongoing therapy. Consistent with previous OAT research, treatment duration in our cohort was short, with the median episode lasting less than two months [6, 11, 29, 30]. In such settings, shorter temporal margins are more appropriate, as they better capture the brief periods of continuity, transition, or multitherapy that characterise real-world OAT use. Similar to our findings, Khotimah et al. also observed minimal changes in episode structure when margins exceeded 14 days [19].
As in Khotimah’s study, starts, finishes, and contains relations were relatively rare, but they remain important because they represent situations in which abrupt changes in a patient’s condition occur, requiring physician management. These changes might include instances when an OAT medication is taken as needed, vomited, lost, or used subtherapeutically.
In our analysis of PharmaNet data, the most frequent co-dispensation involved SROM and methadone (n=524) (Table 4), consistent with clinical practice for patients with more severe OUD [4]. Dispensation sequences further showed that individuals receiving methadone or SROM who were initiated on buprenorphine/naloxone often reverted to their original therapy (at least 26 observed sequences) (Table 4), which could reflect the higher retention observed with methadone [31] and likely suggesting a broader preference for full-agonist therapies.
The study has limitations inherent to administrative health databases. First, PharmaNet captures medications dispensed rather than actual ingestion, and it contains no information on patient intentions, provider-directed holds, or other behavioural factors that influence treatment continuity. Nevertheless, PharmaNet remains a uniquely valuable resource, providing population-wide, event-based dispensing records within a universal health system. Moreover, combining Allen’s relations with temporal margins and drug-specific permissible gaps provides a framework that bridges temporal logic with clinical guidelines, making it well-suited to event-based datasets such as PharmaNet. Alternative approaches—such as sequence-alignment and changepoint-detection algorithms—can characterize longitudinal treatment patterns but do not represent the temporal relationships between dispensations. Sequence-alignment methods treat medication data as a sequence of discrete states and are primarily intended to measure similarity between time-indexed observations for clustering or stratification [32]. Changepoint algorithms detect abrupt or significant shifts in regularly sampled time series [33]. Therefore, these approaches cannot account for clinically meaningful overlap lengths, washout periods, drug-specific discontinuation windows, or the ordering and relational structures captured by Allen’s relations, which are required to differentiate transition and multitherapy episodes. In contrast, our interval-based framework was purposefully developed for irregularly spaced dispensing data and enables clinically meaningful reconstruction of OAT use.
Second, our findings are most directly applicable to PLWH with OUD or OUD–StUD. However, our episode-construction framework is broadly transferable because Allen’s relations, temporal margins, and drug-specific permissible gaps operate on interval timing rather than on population- or jurisdiction-specific fields. In settings without explicit days supply information, intervals can be inferred from the quantity dispensed, standard dosing schedules, or local pharmacy practices. As such, the framework can be adapted for non-HIV populations and applied in international contexts with appropriate calibration of permissible gaps and temporal margins to reflect local clinical practice.
Third, our data ended in March 2020 and therefore do not capture the substantial changes in OAT delivery that occurred during the COVID-19 pandemic. We recommend that future studies apply this methodological framework to post-2020 data to assess how shifts in prescribing practices, increased use of take-home doses [9], and evolving models of care influence OAT episode structure, continuity, transitions, and multitherapy patterns.
Fourth, although external validation through chart review or comparison with a clinical gold standard would have strengthened the framework, it would have required additional administrative approvals, ethics amendments, and chart linkages beyond the scope and timelines of this methodological study. To enhance internal validity, an OAT-specialized clinical pharmacist (Christopher C. Fisher) reviewed all data-cleaning and episode-construction steps, and the conceptual framework was vetted by three physicians with addiction expertise (Drs. Ron Joe, Michael Mulvey, and Galilee Thompson). We also benchmarked our initial cleaning error rates against two prior studies led by our group—one among PLWH receiving OAT in BC [11] and another in a provincial OUD cohort [6]—both of which showed comparable patterns. Finally, the distribution of temporal relations in our cohort closely mirrored those reported by Khotimah et al. in a different therapeutic area, supporting the consistency of our interval-based approach [19].
Conclusion
We developed a refined framework for constructing monotherapy, transition therapy, and multitherapy episodes in administrative health data by combining Allen’s relations with the permissible gap and data-driven temporal margins. Our methodology builds on previous research that either solely used the permissible gap to construct episodes for the same medication or used Allen’s relations with a temporal margin across different medication classes. By combining both techniques, we propose a more flexible and comprehensive approach that leverages the strengths of each, enabling more precise construction of medication episodes and better capture of the complexity of real-world patterns. By offering methodological tools to optimize the usability of administrative health data, this study contributes to clinical practice and policy development. It facilitates more precise assessments of OAT outcomes by properly considering overlaps, transitions, multitherapy, and temporal dynamics, which are increasingly relevant as OAT evolves to meet the complex needs of patients with OUD. Future studies could use this method to examine OUD populations and replicate its applicability using data from after 2020, a period marked by increased OAT transitions, combination therapies, and the COVID-19 pandemic.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
Supplementary Material 3
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1British Columbia’s Office of the Human Rights Commissioner. A human rights-based approach to the toxic drug crisis. Available at: https://bchumanrights.ca/resources/publications/publication/toxic-drug-crisis/.
- 2Tsang VWL, Wong JSH, Westenberg JN, et al. Systematic review on intentional non-medical fentanyl use among people who use drugs. Front Psychiatry. 2024 Feb 13;15:2024.10.3389/fpsyt.2024.1347678 PMC 1089683338414500 · doi ↗ · pubmed ↗
- 3BC Centre for Excellence in HIV/AIDS. Drug treatment and laboratory database. BC Centre for Excellence in HIV/AIDS; 2020. Available at: http://bccfe.ca/.
- 4BC Centre for Disease Control. Provincial HIV/AIDS surveillance database. BC Centre for Disease Control (BCCDC); 2020. Available at: http://www.bccdc.ca/our-services/service-areas/bccdc-public-health-laboratory.
- 5BC Ministry of Health Pharma Net. BC Ministry of Health; 2020. Available at: https://www 2.gov.bc.ca/gov/content/health/conducting-health-research-evaluation/data-access-health-data-central.
- 6Centre for Addition and Mental Health. Opioid agonist therapy: a synthesis of canadian guidelines for treating opioid use disorder. Available at: https://www.camh.ca/-/media/professionals-files/canadian-opioid-use-disorder-guideline 2021-pdf.pdf.
- 7Government of British Columbia. Pharma care. Available at: https://www 2.gov.bc.ca/gov/content/health/practitioner-professional-resources/pharmacare/pharmacies/product-identification-numbers/oat-pins-and-dins.
- 8Vanoli J, Nava CR, Airoldi C, Ucciero A, Salvi V, Barone-Adesi F. Use of state sequence analysis in pharmacoepidemiology: a tutorial. Int J Environ Res Public Health. 2021 Dec 20;18(24).10.3390/ijerph 182413398 PMC 870585034949007 · doi ↗ · pubmed ↗