Lead times in the early management of traumatic brain injury: relation to geographic conditions and clinical outcomes in a nationwide Swedish registry study
Amanda Gu, Francisco Leal-Méndez, Anders Lewén, Anders Hånell, Lina Holmberg, Per Enblad, Teodor Svedung-Wettervik, Fredrik Linder

TL;DR
This study examines how quickly traumatic brain injury patients receive care in Sweden and finds that faster treatment times are linked to better outcomes, though severity of injury is a stronger predictor.
Contribution
The study provides new insights into how geographic and hospital factors influence lead times and outcomes in traumatic brain injury management.
Findings
Larger geographic catchment areas were associated with longer prehospital lead times but shorter times to first CT scans.
Higher hospital caseloads correlated with longer times to first CT scans.
Faster lead times were linked to lower mortality in univariate analysis but not after adjusting for injury severity.
Abstract
Traumatic brain injury (TBI) patients are at risk of sudden deterioration, requiring timely diagnostics and treatment to prevent secondary cerebral injuries. This study investigated lead times in prehospital and early intrahospital TBI management, assessing their association with geographical conditions, hospital caseloads, and patient outcomes. This nationwide, observational cohort study included 5036 TBI patients (during 2018–2022) from the Swedish Trauma Registry (SweTrau). Lead times from trauma to alarm, from alarm to hospital arrival, and times to first computed tomography (CT) from alarm and hospital arrival, respectively, were calculated. These were analyzed against the geographical distribution of healthcare, hospital caseloads, and 30-day mortality. The majority of the cohort arrived in hospital within one hour and suffered a mild-to-moderate TBI. In univariate analyses,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
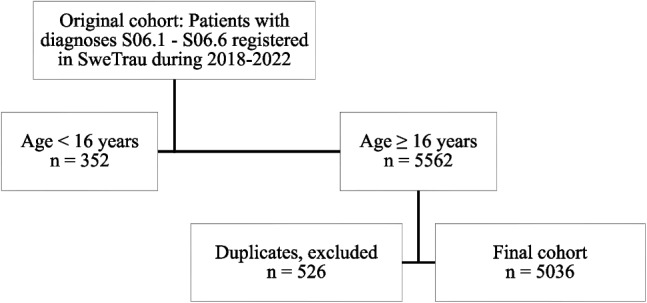 Figure 1
Figure 1- —Uppsala University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Brain Injury and Neurovascular Disturbances · Traumatic Brain Injury Research · Trauma and Emergency Care Studies
Introduction
Traumatic brain injury (TBI) affects approximately 70 million people annually and is a leading cause of mortality and morbidity worldwide [1, 8, 9]. Mild-to-moderate TBI patients typically present with symptoms such as headache, nausea, and amnesia. In some cases, there is a rapid clinical deterioration with loss of consciousness, unreactive pupils, and airway compromise, due to intracranial bleedings and elevated intracranial pressure (ICP) [8]. In addition, a subset of severe TBI cases present immediately in an unconscious state [7, 8, 8, 9]. Stable patients with mild TBI can typically be discharged from the emergency department or admitted for brief neurological monitoring without requiring further treatment [7, 8, 8, 8]. Patients with severe injuries or early deterioration are at high risk of mortality and need prompt physiological and neurosurgical management, primarily due to airway obstruction and ventilation failure caused by brain herniation following expanding intracranial hemorrhages [7, 7, 7, 9]. Additionally, patients with TBI are particularly vulnerable to secondary brain injuries resulting from hypoxia and hypotension, which may be aggravated by multi-trauma [8, 9].
Effective management of TBI requires immediate resuscitation, early diagnostics, and careful stratification to distinguish patients requiring emergent neurosurgery from those with mild injuries that can be managed conservatively. This necessitates efficient prehospital and in-hospital care pathways, which minimize delays from trauma to alarm activation, hospital arrival, imaging (trauma CT) and treatments. Prehospital care is particularly influenced by geographical variations in different hospital catchment areas, which may impact the time from injury to hospital arrival. Prehospitally, the need for immediate resuscitation must be weighed against the urgency of timely transport to a hospital capable of appropriate diagnostic imaging and advanced care [7, 7, 9]. The "Platinum Ten" principle recommends limiting on-site care to 10 min to avoid unnecessary delays while allowing sufficient time for initial stabilization [7, 8]. However, as shown in the multicenter CENTER-TBI study, prehospital practices vary considerably across Europe [9]. Subsequently, upon contact with the receiving hospital, a trauma alarm may be triggered to initiate immediate care, following local or national guidelines [8].
Evaluation and resuscitation of trauma patients follow the Advanced Trauma Life Support (ATLS) protocol prioritizing airway (A), breathing (B), circulation (C), neurological disability (D), and exposure (E) [7]. Hemodynamically unstable patients who do not respond to initial interventions may require immediate surgical interventions, while a trauma CT may be performed to evaluate potential injuries in stable patients [7, 8, 8, 9, 9]. For patients with isolated head trauma, protocols typically mandate that trained personnel assess the patient within 15 min of arrival [8]. TBI patients with mass lesions are often transferred to neurosurgical centers for hematoma evacuation and neurointensive care [7, 7, 7, 8, 8]. However, variations in hospital experience and caseload, and the distance to the nearest neurosurgical center can differ and influence the time from injury to definitive treatment [7, 9].
Sweden is a geographically large country with both densely populated urban areas and extensive sparsely populated regions, resulting in a substantial geographical variation in access to specialized neurosurgical care in terms of geographical distance and transportation time. The healthcare system is administratively divided into 20 individual health care regions, with a total of 49 local hospitals providing around the clock general trauma care, of which 7 university hospitals offer specialized neurosurgical care [1, 3, 7, 8]. The common practice is that TBI patients are stabilized initially at local hospitals, followed by secondary transfer to a neurosurgical center if needed [8, 8]. In regions maintaining a university hospital, patients may primarily be admitted to this specific neurosurgical department. Exceptionally, acute extracerebral hematomas may be evacuated in local hospitals as a life-saving procedure [8]. However, in geographically compact and densely populated regions, moderate to severe TBI patients are more often directly transported to hospitals with neurosurgical capabilities [8, 8]. Ultimately, it is evident that the geographical distribution of healthcare resources is uneven and may affect the management of TBI patients.
Many factors may influence the lapse of management of TBI patients, potentially delaying necessary diagnostics and treatments, and increasing risks of developing secondary brain injuries. There is limited evidence on how patient characteristics, geographical factors and hospital experience affect lead times in these early care pathways, and which impact delays have on clinical outcomes. Therefore, the aim of this study was to investigate variations in lead times, their explanatory variables and their effect on mortality in a Swedish nationwide cohort registry study.
Materials and methods
Study design and population
This retrospective observational study utilized data from the Swedish Trauma Registry (SweTrau), a nation-wide registry with data from hospitals in Sweden that provide care for severe traumatic injuries. The study focused on patients with TBI diagnoses and New Injury Severity Score > 15 (S06.1–S06.6), aged 16 or older, treated between January 1, 2018, and December 31, 2022. The data extracted with these inclusion criteria covered 20 Swedish health care regions and 47 hospitals. From the 5914 patients with these diagnoses during this time period, 352 were excluded due to age below 16. Furthermore, duplicate registrations were identified by person identification number or temporary identification number, age [years], date of birth, and gender. In total, 526 duplicate cases were excluded, resulting in a final cohort of 5036 individuals (Fig. 1).Fig. 1. Flow chart of patient inclusion. In this study, individuals with diagnoses S06.1 - S06.6 aged ≥ 16 years were included and duplicate case registrations were excluded.
Data collection and variable definitions
All data used in this study were acquired from the SweTrau registry [7]. Demographics (age, sex), injury mechanisms (falls, road traffic accidents etc.), injury severity (Glasgow Coma scale [GCS], abbreviated injury scale [AIS] head, injury severity score [ISS]), injury types (epidural hematoma [EDH], acute subdural hematoma [ASDH], traumatic subarachnoid hemorrhage [tSAH], contusion), interventions (craniotomy) and outcome (30-day mortality) were extracted from the registry.
Registered date and time of trauma, alarm, primary hospital arrival and first CT, respectively, were also extracted. The accuracy of these time variables in SweTrau has previously been reported to be 74% or higher when allowing a margin of error up to 10 min, with a correctness of 89.7% of the registry data overall, and a case completeness of 100% for individuals with NISS > 15 [7]. The time intervals were calculated from trauma to alarm and from alarm to arrival in the primary hospital (local hospital or university hospital), which were considered indicators of access to care. Also, time to first CT from alarm and arrival in hospital was calculated, which were considered indicators of both pre- and in-hospital trauma management. Few individuals (n = 2) exhibited lead times of negative values which were treated as missing values. Outcome was dichotomized into mortality/survival 30 days post-injury.
Statistical analysis
Statistical analyses were performed using SPSS (IBM SPSS Statistics, Version 29.0.2.0). Variables were described as medians (interquartile range (IQR)) or counts (proportions), depending on the data type. Differences in lead times for trauma management were analyzed in relation to geographical conditions (large vs. small counties), caseload (high vs. low), and clinical outcome (mortality vs. survival 30 days post-injury) using Mann–Whitney U-test. A multivariate linear regression was performed for each time interval (trauma to alarm, alarm to hospital, alarm to first CT, and hospital to first CT) as the dependent variable. The analyses were adjusted for hospital caseload (higher vs. lower), county size (larger vs. smaller), age, neurological injury severity (GCS) and type of initial hospital (university vs. local), to assess their independent associations. In addition, a multivariate logistic regression was performed with mortality as the dependent variable, to explore the independent association of the lead time variables after adjusting for demography (age and sex) and neurological injury severity (GCS). A p-value < 0.05 was considered statistically significant.
Results
Demography, management, lead times in management, injury severity, and outcome
As presented in Table 1, the median patient age was 65 years (IQR 46–78). The cohort was predominantly male (n = 3412, 68%), with a median pre-injury ASA score of 2 (IQR 1–3), and median GCS score at admission of 14 (IQR 12–15). The majority of patients were managed at university hospitals, either as primary or secondary cases (n = 3017, 59.9%). Table 1. Demography, injury mechanisms, admission status, injuries, time logistics, treatments, and outcomeVariablesEntire cohortPatients, n (%)5036 (100)Age (years), median (IQR)65 (46–78)Sex (male/female), n (%)Male 3412 (68)Female 1624 (32)Pre-injury ASA score, median (IQR)2 (1–3)Injury mechanism, n (%)Traffic accident1204 (23.9)Pedestrian accident160 (3.2)Gunshot wound21 (0.4)Penetrating trauma20 (0.4)Blunt trauma297 (5.9)Low energy fall1850 (36.7)High energy fall1268 (25.2)Injury from explosion6 (0.1)Other (eg suffocation, burns)101 (2.0)Missing109 (2.0)GCS at admission, median (IQR)14 (12–15)GCS motor at admission, median (IQR)6 (5–6)AIS head, median (IQR)2 (1–3)Epidural hematoma, n (%) (S06.4)533 (10.6)Acute subdural hematoma, n (%) (S06.5)3758 (74.6)Traumatic subarachnoid hemorrhage, n (%) (S06.6)2541 (50.5)Contusion, n (%) (S06.1)191 (3.8)Managed at university hospital alone, local hospital alone, or both,* n (%)University hospital alone1733 (37.5)Local hospital alone1608 (34.8)Both1284 (27.8)First admitting hospital, university hospital or local hospital,* n (%)University hospital2337 (46.4)Local hospital2699 (53.6)Trauma to alarm (minutes),* median (IQR)29 (2–38)Alarm to hospital (minutes),* median (IQR)45 (5–52)Alarm to first CT, * median (IQR)153 (93–474)Hospital to first CT (minutes),* median (IQR)70 (45–103)Craniotomy (yes), n (%)587 (11.7)ICP-monitoring (yes), n (%)481 (9.6)30-day mortality,* n (%)930 (19)TBI severity*Mild (GCS 13–15)3035 (60.3)Moderate (GCS 9–12)540 (10.7)Severe (GCS 3–8)548 (10.9)*Missing data: Managed at university hospital alone, local hospital alone, or both: n = 413 (8.2%); First admitting hospital: n = 2 (0.0%); Trauma to alarm: n = 848 (16.8); Alarm to hospital: n = 847 (16.8); Alarm to first CT: n = 171 (3.4); Hospital to first CT: n = 170 (3.4); 30 day mortality: n = 113 (2.2%); TBI severity: n = 802 (15.9)%
Median lead times were as follows: injury to alarm 29 min (IQR 2–38), alarm to hospital arrival 45 min (IQR 5–52), and arrival to CT 70 min (IQR 45–103). The median AIS score for head injuries was 2 (IQR 1–3). In total, 587 (11.7%) underwent craniotomy, and 481 (9.6%) received ICP monitoring. The overall 30-day mortality rate was 19% (n = 930).
Lead times of trauma management in relation to geographical factors and hospital caseload
The health care regions were dichotomized as smaller or larger based on the median geographical area per hospital (5713 km^2^), resulting in 10 smaller and 10 larger regions. As also shown in Table 2, geographically larger regions exhibited longer lead time between alarm to arrival in hospital (p < 0.05), but had no significant association to times from trauma to alarm, from alarm to first CT, or from hospital arrival to first CT. Hospitals were also dichotomized by caseload (Table 3), defined as low or high based on having a lower or higher annual volume of TBI patients than the median across all hospitals included in the registry data (46 cases in total, whereof 23 lower and 24 higher caseload hospitals, respectively). Hospital caseload was not significantly associated with any of the lead times. Table 2. Time logistics of the trauma emergency care in relation to regional geographyVariablesLarger regionsSmaller regionsp*-valueN (%) validmedian (IQR)N (%) validmedian (IQR)Trauma to alarm (minutes)8 (80.0)5 (3—8)10 (100.0)5 (5–5)0.778Alarm to hospital (minutes)10 (100.0)54 (52–64)10 (100.0)51 (48–51)0.041Alarm to first CT (minutes)10 (100.0)98 (95–120)10 (100.0)107 (95–107)0.224Hospital to first CT (minutes)10 (100.0)37 (34–47)10 (100.0)48 (39–48)0.926Average catchment area per hospital within the same region > 5713 km^2^ (median of all regions)**Average catchment area per hospital within the same region ≤ 5713 km^2^ (median of all regions)Table 3. Time logistics of the trauma emergency care in relation to caseloadVariablesHigher caseloadLower caseloadp-valueN (%) validmedian (IQR)N (%) validmedian (IQR)Trauma to alarm (minutes)21 (91.3)5 (2–45)22 (91.7)5 (1–81)0.095Alarm to hospital (minutes)22 (95.7)51 (38–69)24 (100.0)56 (39–79)0.881Alarm to first CT (minutes)21 (91.3)44 (28–108)20 (83.3)42 (30–68)0.481Hospital to first CT (minutes)21 (91.3)102 (75–149)21 (87.5)107 (81–144)0.529*Average case load per year > 67 (median of all hospitals)**Average case load per year < 67 (median of all hospitals)
In a multivariate linear regression analysis of geographical area (smaller/larger) and caseload (low/high) in relation to the lead times of TBI management, adjustments were made for age, GCS score, and first admitting hospital (university/local hospital), as presented in Table 4. Higher hospital caseload correlated independently with longer time from alarm to CT (B = 34.71, p < 0.05) and from hospital arrival to CT (B = 43.99, p < 0.05), but showed no correlation to the other lead times. Larger region size was associated with overall longer lead times (p < 0.05), except for time from alarm to first CT which was shorter (B = −10.76, p < 0.05), and did not correlate to the time from hospital arrival to CT (p > 0.05). Table 4. Multivariate linear regression analysisTrauma to alarmRegression coefficient (B)****Standardized coefficients (β)p-valueCaseload (lower/higher caseload)39.950.0130.445Size (smaller/larger regions)155.20.047 < 0.001Age (years)2.3550.0690.003Gender (male/female)−29.88−0.0130.408GCS in ED (scale)0.0990.0200.216Initial caregiver (university/local)61.180.0380.024Alarm to hospitalRegression coefficient (B)Standardized coefficients (β)p-value**Caseload (lower/higher caseload)−0.271−0.0020.899Size (smaller/larger regions)8.5350.093 < 0.001Age (years)0.1660.081** < 0.001Gender (male/female)−1.678−0.0180.253GCS in ED (scale)0.0130.065** < 0.001Initial caregiver (university/local)2.9350.0450.008Alarm to first CTRegression coefficient (B)****Standardized coefficients (β)p-valueCaseload (lower/higher caseload)34.710.108* < 0.001Size (smaller/larger regions)*−10.76−0.0470.002Age (years)0.6610.129 < 0.001Gender (male/female)1.9360.0080.569GCS in ED (scale)−0.008−0.0160.297Initial caregiver (university/local)26.330.160 < 0.001Hospital to first CTRegression coefficient (B)Standardized coefficients (β)p-valueCaseload (lower/higher caseload)*43.990.0430.006**Size (smaller/larger regions)−11.21−0.0150.294Age (years)0.2130.0130.382Gender (male/female)−3.508−0.0050.751GCS in ED (scale)0.0090.0050.725Initial caregiver (university/local)−36.85−0.070 < 0.001Regression coefficients are presented for higher hospital caseload, larger geographical region sizeCategorical variables, regression coefficients are presented for female gender and local hospital
Higher age was associated with longer time from trauma to alarm, from alarm to hospital and to CT, but not from hospital to CT (p > 0.050). Patients with lower GCS showed faster time from alarm to hospital, meanwhile, gender was not associated with any of the lead times (p > 0.05). Having been initially managed in a local hospital was associated with longer time from trauma to alarm, from alarm to hospital arrival, and from alarm to CT (all p < 0.05), but shorter time from hospital to CT (p < 0.05).
Lead times of trauma management in relation to patient outcomes.
In a univariate analysis, patients who survived presented with significantly longer time from alarm to CT, and hospital to CT, but shorter time from trauma to alarm, as seen in Table 5. Meanwhile, time from alarm to hospital was not associated with higher mortality (p > 0.05) (Table 5). Table 5. Time logistics of the trauma emergency care in relation to survival and mortalityVariablesSurvivorsDeceasedp-valueN (%) validmedian (IQR)N (%) validmedian (IQR)Trauma to alarm (minutes)3264 (81.7)5 (2–27)846 (91.2)11 (3–380)** < 0.001Alarm to hospital (minutes)3264 (81.7)52 (38–70)846 (91.2)52 (37–67)0.096Alarm to first CT (minutes)3472 (81.3)107 (77–158)660 (86.3)87 (71–119) < 0.001Hospital to first CT (minutes)3265 (81.7)48 (29–115)868 (93.5)37 (26–58) < 0.001**
In a multivariate logistic regression analysis, seen in Table 6, longer time from trauma to alarm was associated with higher mortality (OR 1.000, 95% CI (1.000–1.000), p < 0.05). Furthermore, there was no other independent association between any of the lead times and mortality, after adjustment for age, gender, GCS score, head AIS score, and pre-injury ASA score. Higher risk of mortality was associated with increasing age (OR 1.052, 95% CI (1.046–1.058), p < 0.05) and with higher pre-injury ASA score (OR 1.001, 95% CI (1.000–1.002), p < 0.05). Meanwhile, lower AIS head score showed independent association with lower mortality (OR 0.934, 95% CI (0.891–0.979), p < 0.05). Neither GCS nor gender was significantly associated with mortality. Table 6. Multivariate logistic regression analysisVariablesMortalityOR (95% CI)p-valueAge (years)1.052 (1.046–1.058)** < 0.001ASA pre-injury (score)1.001 (1.000–1.002)0.033AIS head (score)0.934 (0.891–0.979)0.005Gender (male vs female) 0.844 (0.706–1.009)0.063GCS (sum)1.000 (1.000–1.001)0.085Trauma to alarm (minutes)1.000 (1.000–1.000)* < 0.001Alarm to hospital (minutes)1.042 (0.896–1.213)1.042Alarm to first CT (minutes)0.957 (0.822–1.113)0.568Hospital to first CT (minutes)1.037 (0.891–1.207)0.638*Categorical variable, OR and 95% CI is presented for female gender
Discussion
In this large nationwide study of 5036 TBI patients, the main findings were that most patients arrived at a hospital within one hour of injury, while geographically larger regions exhibited longer prehospital management. More severe neurological and systemic injuries, indicated by lower GCS, were generally associated with shorter time to first CT. Univariate analyses showed overall longer in-hospital management among survivors, although, these relationships did not persist in multivariate regressions*.* However, the lead times also exhibited a complex interplay with other factors including injury severity, geographical conditions, and resource availability.
Our findings showed that Swedish prehospital management was generally effective, with most cases arriving at a hospital within an hour. However, there was substantial variation in pre- and in-hospital lead times. Firstly, there were several important factors related to the healthcare organization. Larger geographical county area was independently associated with longer prehospital lead times, consistent with greater transportation distances, but shorter time from arrival in hospital to first CT. The prehospital lead times were also longer at local hospitals, compared to university hospitals, while the opposite was true for in-hospital lead time from hospital arrival to first CT. One possible explanation is that university hospitals are often located in Sweden’s larger cities, where the proximity between patient and hospital and the density of prehospital resources, including helicopter emergency medical services, are generally higher. However, a potential drawback is the typically high patient load at these emergency departments, leading to increased competition for rapid assessment and imaging resources with other critically ill patients. In contrast, a major trauma case at a smaller hospital is more uncommon and may be prioritized more rapidly throughout the chain of care, leading to shorter in-hospital lead times. Consistent with this idea, higher caseload hospitals exhibited slower in-hospital lead times. While a high volume of cases could theoretically lead to greater efficiency through routine and experience [7, 7, 7–9, 9], this potential advantage was likely outweighed by the strain on resources and bottlenecks associated with managing many critically ill patients simultaneously [7, 8].
Secondly, there were also several important patient-specific factors related to the lead times in trauma management, and to mortality. Older patients consistently exhibited longer lead times. Moreover, the presence of comorbidities makes early management more complex, and older or more frail patients may require more thorough assessment and stabilization before proceeding to imaging or definitive care. Also, offering the full extent of advanced trauma care may not always be appropriate or beneficial in this patient group, and individualized decisions regarding the level of intervention are often required. As expected, patients with more severe neurological injuries exhibited shorter prehospital lead times, probably as they received high-priority to receive necessary diagnostics and possibly in-hospital emergency neurosurgery [8]. This may have contributed to the increased risk of mortality associated with shorter prehospital leadtimes, observed in univariate analysis. Furthermore, a study of more severe injuries in an older cohort by Region Stockholm showed early transfers to be associated with poorer outcomes [7]. This supports the hypothesis that patients in greatest need of acute care are likely identified and transferred promptly, even though such cases often represent a particularly vulnerable and clinically complex subgroup.
Regarding the clinical significance of lead times on outcome, univariate analyses in this study showed that patients who survived exhibited longer lead times to CT and definitive care. This was likely confounded by injury severity, as survivors tended to have milder injuries with less urgent need for intervention. Consistently, in multivariate analysis, adjusting for such clinical variables, no independent association between lead times and outcome could be demonstrated. This suggests that, at the group level, time intervals in trauma management may be of lower prognostic relevance compared to established predictors such as age and neurological injury severity as measured by GCS, and AIS head score, as major predictors of mortality in TBI [7, 7–9]. However, higher pre-injury ASA score also showed to associate independently with higher mortality, in agreement with past research [8, 9], enhancing the significance of patient-bound conditions in the outcome after TBI.
Although the concept that "time is brain" remains highly relevant in case of impending brain herniation, this represents a relatively uncommon and dynamic subset in the entire spectrum of TBI eliciting a trauma alarm, as opposed to selected severe cases admitted to neurointensive care units [9]. In the current cohort, despite triggering trauma team activation due to suspected severe trauma, many patients presented with GCS scores within the mild-to-moderate range. Moreover, even in severe TBI, the number of patients requiring immediate neurosurgery with evacuation of intracranial bleedings may be limited, as a substantial proportion is unconscious due to factors not related to mass effect such as traumatic axonal lesions. Another aspect related to early diagnostics is the risk of intracranial bleeding progression, particularly among patients on anticoagulant therapy [7]. While such data were not available in this study, due to not being presented in the SweTrau registry, previous research has shown a clear benefit of early reversal of warfarin [9] and potential effects of prothrombin complex concentrates and tranexamic acid in patients on novel oral anticoagulants [9]. Nevertheless, these nuances may not shift overall outcome patterns at the group level, not least because trauma systems continuously strive to compensate for their weakest links. Clinical deterioration is often met with prompt countermeasures, and adverse events may be mitigated by e.g., emergency neurosurgery before causing lasting harm. Additionally, high-quality trauma care encompasses more than just rapid access to emergency neurosurgery. Timely resuscitation, with attention to airway, breathing, and circulation (ABCDE), is essential to avoid secondary brain injury from hypoxia and hypotension, both of which are well-established predictors of poor outcome in TBI [9, 9]. Still, the optimal timing for intervention is not always in the emergency room: extended prehospital time may, in some cases, be justified by the need for airway protection or hemodynamic stabilization, potentially mitigating the harm of secondary insults before hospital arrival [9].
Ultimately, while specific patient subgroups such as those with herniation syndromes or anticoagulated patients with intracranial hemorrhage may benefit from faster intervention, the complex interplay between injury severity, physiological response, and care quality makes it difficult to isolate time as a primary driver of outcome. In this cohort, characterized by a predominance of mild-to-moderate TBI, the observed lack of association between time and outcome reinforces the notion that age and clinical severity, rather than lead times per se, remain the most robust predictor of prognosis in TBI.
Methodological considerations
The study has many strengths. It is based on a large national cohort of more than 5000 TBI patients with comprehensive data coverage. Missing data was relatively rare, although certain variables had lower data availability.
The extracted times of events from the registry data, used to calculate lead time intervals, may have been imprecise (± 1 h), due to registration in SweTrau being performed retrospectively. This introduces uncertainty, particularly regarding the time intervals which were less than one hour. Although this uncertainty may have contributed to incomprehensive results, as mentioned, the used variables have been shown to have a correctness of 74% or higher for this patient group when allowing a margin of error up to 10 min [7]. Moreover, previous studies on TBI [7, 7] have concluded that exact prehospital and in-hospital timings are not the primary determinants of patient outcomes, foreshadowing doubt to the significance of this uncertainty.
In this study, having a regional hospital as the first admitting hospital was associated with longer time from trauma to alarm, alarm to hospital arrival, and alarm to CT, but shorter time from trauma and from arrival to CT. This may be caused by a higher proportion of missing data for time from trauma to alarm and alarm to hospital arrival, compared to the lead times which were independent of the time of alarm. However, this higher rate of missing data may also be caused by registration of patients who suffered TBI while already inpatient.
While including a predominant share of mild TBI, and with a median cohort ASA score of 2, the mortality rate in this cohort was 18.4%. As the cause of death is not registered in SweTrau, it is possible that a proportion of these deaths were attributed to comorbidities or systemic injuries injuries. Also, given regards that the mortality was measured as of 30 days after injury, it cannot be disregarded that the patient deceased from a separate insult not related to TBI. Furthermore, the registry does not include information about the cause of death. Thus, especially in patients suffering multiple traumatic injuries, it cannot be certain that the patient deceased as a direct cause of the TBI. However, the overall mortality of all registered cases in SweTrau during the period of 2022–2024 was approximately 16% [2], and injury to the central nervous system and multi-organ failure are leading causes of death in patients suffering polytrauma [8, 9]. Nevertheless, the lack of this data is considered a limitation in evaluating patient outcome. Furthermore, the SweTrau registry does not include information on the prevalence of withholding of treatment or choosing not to escalate treatment. With regards to the median age of 65 years in the cohort of this study, accountability for such circumstances should be taken when observing the outcomes in TBI.
Conclusions
Many patients in this nationwide cohort arrived at a hospital within one hour of injury and underwent a first trauma CT within two hours. Geographically larger regions exhibited longer prehospital management, while university hospitals and higher caseload hospitals showed longer overall lead times but shorter in-hospital time to first CT. Severe neurological injuries were generally associated with more rapid trauma management, reflecting higher prioritization. Univariate analyses indicated that faster lead times were associated with higher mortality, while no such association was found in multivariate regressions. These findings suggest that lead times in TBI management interact intricately with both care-related and external factors, including injury severity, geographical challenges, system organization, and resource availability. While timely care, particularly in subgroups requiring urgent neurosurgical intervention or hemodynamic stabilization remains crucial, this study reinforces the view that clinical severity markers such as age and GCS are stronger predictors of outcome than the lead times in TBI management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Swe Trau (2022) Årsrapport 2021. https://swetrau.se/om-swetrau/arsrapporter. Accessed 4 Oct 2024
- 2Swe Trau (2025) Årsrapport 2024. https://swetrau.se/om-swetrau/arsrapporter. Accessed 9 Feb 2026
- 3Statistiska centralbyrån (SCB) (2025). Befolkningstäthet i Sverige. https://www.scb.se/hitta-statistik/sverige-i-siffror/manniskorna-i-sverige/befolkningstathet-i-sverige/. Accessed 1 May 2025
- 4Brown JB, Kheng M, Carney NA, Rubiano AM, Puyana JC (2019) Geographical disparity and traumatic brain injury in America: rural areas suffer poorer outcomes. J Neurosci Rural Pract 10:10–15. 10.4103/jnrp.jnrp_310_1810.4103/jnrp.jnrp_310_18PMC 633796130765964 · doi ↗ · pubmed ↗
- 5Bullock MR, Chesnut R, Ghajar J, Gordon D, Hartl R, Newell DW et al. (2006) Surgical management of acute epidural hematomas. Neurosurgery 58:S 7–15; discussion Si-iv 16710967 · pubmed ↗
- 6Ponsford JL, Carey M, Oliver J, Ponsfod M, Acher R, Mc Kenzie D, Downing MG (2024) Considering the importance of personal and injury factors influencing outcome after traumatic brain injury. Arch Phys Med Rehab 105(9):1666–1672. 10.1016/j.ampr.2024.03.00310.1016/j.apmr.2024.03.00338493908 · doi ↗ · pubmed ↗
- 7Bhogadi SK, Nelson A, Hosseinpour H, Anand T, Hejazi O, Colosimo C, Spencer AL, Dittilo M, Magnotta LJ, Joseph B (2024) Effect of PCC on outcomes of severe traumatic brain injury patients on preinjury anticoagulation. AM J Surg 232:138–141. 10.1016/j.amjsurg.2024.01.03510.1016/j.amjsurg.2024.01.03538309997 · doi ↗ · pubmed ↗
- 8Ginstman MF, Fredrik MN (2020) Svår traumatisk hjärnskada. Läkartidningen. https://lakartidningen.se/klinik-och-vetenskap-1/medicinens-abc/2020/06/svar-traumatisk-hjarnskada/. Accessed 22 Jan 202532542612 · pubmed ↗